
Abstract
Purpose
As the detection of non-alcoholic fatty liver disease (NAFLD) is imperative for the prevention of its complications, we aimed to explore the predictive value of platelet to lymphocyte count ratio (PLR) and white blood cell count to mean platelet volume ratio (WBC/MPV) in relation to the occurrence of NAFLD among patients with obstructive sleep apnea–hypopnea syndrome (OSAHS).
Methods
This was a cross-sectional study consisting of 351 patients with OSAHS (279 with and 72 without NAFLD). The logistic regression analysis was performed to estimate associations between PLR, WBC/MPV, and NAFLD. Finally, the receiver operating characteristic curve (ROC curve) was used to analyze the efficacy of PLR and WBC/MPV in NAFLD prediction.
Results
Compared to the OSAHS-only group, there was a rising trend in AHI and TS90% in the OSAHS + NAFLD group. And the logistic regression analysis identified average oxygen saturation (MaSO2), WBC/MPV and PLR as predicted factors (odds ratio [OR] = 1.134, P = 0.031; OR = 7.559, P = 0.018, OR = 0.980, P < 0.001, respectively) for NAFLD in OSAHS patients. Moreover, compared with WBC/MPV, PLR, FLI, and APRI, a combination of WBC/MPV and PLR presented the largest AUC for the detection of NAFLD in BMI < 28 kg/m2 (0.753, 95% CI 0.684–0.822), and in age ≥ 60 years subgroup (0.786, 95% CI 0.692–0.880) in ROC analysis. Meanwhile, a combination of WBC/MPV and PLR presented the second largest AUC for the detection of NAFLD in all subjects (0.743, 95% CI 0.708–0.831), as well as in the age < 60 years subgroup (0.729, 95% CI 0.652–0.806), only ranked after FLI, suggesting the combination of WBC/MPV and PLR has a good predictive value for NAFLD in OSAHS patients.
Conclusion
We confirmed that the levels of WBC/MPV, PLR, and MaSO2 were closely related to the occurrence of NAFLD among OSAHS patients. Furthermore, our results highlighted the clinical combination of WBC/MPV and PLR levels could act as a simple and effective biomarker for screening NAFLD in patients with OSAHS.
Similar content being viewed by others

Introduction
Non-alcoholic fatty liver disease (NAFLD) is a spectrum ranging from non-alcoholic fatty liver (NAFL), to non-alcoholic steatohepatitis (NASH), to cirrhosis [1]. NAFLD has become the most common chronic liver disorder, with a global prevalence of 25.24% of the adult population, and the incidence is rapidly increasing year by year [2]. It was supposed that NAFLD would become the primary indication for liver transplantation in the future [3].
There is a growing body of evidence demonstrating a positive correlation between NAFLD and obstructive sleep apnea–hypopnea syndrome (OSAHS) [4, 5]. Of note, NAFLD is typically asymptomatic until the advanced stages, and the routine detection of NAFLD based on liver biopsy, sonography, liver/spleen CT (liver/spleen computed tomography), and magnetic resonance imaging (MRI) may not be feasible with respect to health care expenditures and biopsy-related risks [6], highlighting the importance of exploring accurate non-invasive tools for prediction and early diagnosis of fatty liver, particularly in high-risk groups including those with OSAHS.
A series of studies have shown that NAFLD was closely linked to subclinical inflammation [7, 8], and routine blood cells, including platelet and white blood cell, have proven to be good biomarkers for systemic inflammation [9, 10]. Thus, we tested the performance of the platelet-related parameters in the prediction of NAFLD.
Platelet to lymphocyte count ratio (PLR) is a novel biomarker that has been initially proposed as an ideal indicator of systemic inflammation [11,12,13]. Recently, emerging evidence indicated strong link in between OSAHS, liver diseases (including HBV/HCV and HCC), and PLR [14,15,16,17]. However, there was a lack of data regarding the association between PLR and NAFLD. White blood cell count to mean platelet volume ratio (WBC/MPV) was previously used as a predictor of thrombosis in cardiovascular and cerebrovascular illnesses [18,19,20]. However, there has been no study on the relationship between WBC/MPV, OSAHS, and NAFLD. Since OSAHS and NAFLD might both create pathological changes in the blood system, there was a possibility that WBC/MPV had a relationship with OSAHS and/or NAFLD. Furthermore, previous studies have confirmed non-invasive scores, such as the aspartate aminotransferase to platelet ratio index (APRI), and the fatty liver index (FLI) had good performance in assessing NAFLD [21, 22]. Accordingly, the present study aimed to evaluate the predictive power of platelet-related parameters (PLR and WBC/MPV) for detecting NAFLD in individuals with OSAHS compared with APRI and FLI.
Material and methods
Participants
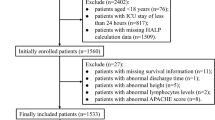
The study cohort comprised individuals who attended our sleep center because of snoring, excessive daytime sleepiness, or other related symptoms, and were finally diagnosed with OSAHS by polysomnography between January 2016 and December 2020. The exclusion criteria included the following: (1) chronic obstructive pulmonary disease, bronchial asthma, interstitial lung disease, and other chronic lung diseases; and (2) severe heart failure, stroke, and other severe cardiovascular and cerebrovascular diseases; and (3) malignant tumor or major physical or mental illness; and (4) hepatic diseases such as viral hepatitis, autoimmune liver disease, and drug-induced liver disease; and (5) immune or hematological diseases such as rheumatoid arthritis; (6) acute and chronic infections; and (7) anti-platelet drugs used in the last month; and (8) excessive drinking (the amount of alcohol consumed in men is equivalent to > 30 g of ethanol per day, and is > 20 g/d in women); and (9) other sleep disorders, such as narcolepsy and restless leg syndrome, etc.; and (10) sleep apnea attributable to other causes, such as hypothyroidism and central and mixed sleep apnea; and (11) history of previous CPAP treatment; and (12) history of previous splenectomy. The study was approved by the First Affiliated Hospital of Fujian Medical University (Fuzhou, China) and all participants gave their written informed consent after a full explanation.
Clinical data collection
All participants completed a detailed questionnaire on history of smoking and alcohol consumption, medical history (hypertension, diabetes mellitus, hyperlipidemia etc.), and medications, and physical examination. Anthropometric measurements including height and body weight were obtained with the participants wearing light clothing. The body mass index (BMI) was calculated as body weight/ height squared (kg/m2). Waist circumference (midway between the lower costal margin and iliac crest) and neck circumference (at the level of the laryngeal prominence) were measured with a tape. In addition, every subject completed an Epworth sleepiness scale (ESS) using a well-validated Chinese version with the score ranging from 0 to 24, and it was considered daytime sleepiness when ESS score was ≥ 10 [23].
Laboratory measurements
Venous blood was taken the morning after polysomnographic evaluation. Blood routine, liver function, triglyceride (TG), total cholesterol (TC), and fasting glucose were tested in all patients. Blood routine was detected by Hitachi H-7600 autoanalyzer produced by Japan Co., Ltd., and blood biochemistry was performed using a Modular P800 autoanalyzer (Roche, Tokyo, Japan). PLR measured platelet count to lymphocyte count, and WBC/MPV measured white blood cell count to mean platelet volume. Platelet-related parameters including platelet count (PC), mean platelet volume (MPV), platelet distribution width (PDW), plateletcrit (PCT), average concentration of platelet contents (MPC) were also assessed. FLI and APRI were calculated using the following formulas [21, 22]: FLI = (e0.953×ln(triglycerides)+0.139×BMI+0.718×ln(GGT)+0.053×waistcircumference−15.745)/(1 + e0.953×ln(triglycerides)+0.139×BMI+0.718×ln(GGT)+0.053×waistcircumference−15.745) × 100 (with TG measured in mmol/l, GGT in U/l, and waist circumference in cm), APRI = (AST/upper limit of normal)/platelets (109/L) × 100.
Polysomnographic evaluation
Overnight polysomnography (P Series Sleep System, Compumedics, Melbourne, Australia) was conducted to diagnose OSAHS. Electroencephalography, electrooculography, electromyography, and electrocardiography were performed during polysomnography, and the variables assessed being as follows: oronasal airflow, thoracic and abdominal respiratory efforts, and pulse oxygen saturation. AHI was defined as the number of episodes of apnea and hypopnea per hour of sleep. ODI was defined as number of episodes of oxyhemoglobin desaturation ≥ 3% from the immediate baseline per hour of total sleep time. Other variables, including LaSO2, MaSO2, and TS90%, were also assessed. All PSG studies were scored according to the criteria of the American Academy of Sleep Medicine published in 2012 [24]. The severity of OSAHS was classified based on AHI status as follows: no OSAHS, < 5 events/h; mild OSAHS, 5 to < 15 events/h; moderate OSAHS, 15 to < 30 events/h; and severe OSAHS, ≥ 30 events/h.
Assessment of NAFLD
Abdominal ultrasonography was performed by the trained sonographers using a Toshiba SSA-660A instrument (Toshiba, Tokyo, Japan) with a 2–5 MHz curved array probe. According to the revised 2018 NAFLD definition and treatment guidelines[25], diagnosis of fatty liver disease required the presence of at least two of the following three abnormal findings: diffusely increased liver near field ultrasound echo (‘bright liver’) and increased liver echotexture when compared to the kidneys, vascular blurring and deep attenuation of ultrasound signal. Participants were categorized into having NAFLD if they were diagnosed with fatty liver through ultrasonography and the weekly alcohol intake of < 210 g in men and < 140 g in women. In addition, other liver diseases (including chronic hepatitis B or C, operations on the liver, autoimmune liver diseases, cirrhotic or liver cancer, etc.) were identified by the results of their annual medical examinations (e.g., positive hepatitis B or C serology) and/or the self‐reported history of liver diseases.
Statistical analysis
All statistical analyses were carried out with IBM SPSS Statistics for windows (Version 25.0 IBM Corp. Released 2017). Armonk, NY). Normally distributed data were expressed as means ± standard deviations, while skewed data were expressed as medians with interquartile range (IQR). Categorical data were expressed as proportions (percentage). Using the χ2 test for categorical data, the independent t-test for normally distributed data, and the Mann–Whitney U test for skewed data, the differences between groups with and without NAFLD were analyzed. Using Spearman's rank correlation coefficients, the relationships between platelet-related parameters and relevant factors were evaluated. An examination of the association between platelet-related characteristics and NAFLD, which served as the dependent variable, was accomplished by means of a binary logistic regression analysis. Through the use of receiver operating characteristic curve (ROC) analysis, the predictive value of PLR, WBC/MPV, and the combination of the two indices was investigated. P < 0.05 was deemed statistically significant for all two-tailed tests.
Results
Demographic data, anthropometric and polysomnographic variables in all participants
Our study comprised 351 OSAHS patients including 283 males and 68 females, with a mean age of 51.32 ± 13.65 years and a mean BMI of 28.2 ± 11.1 kg/m2. According to the ultrasound diagnosis of NAFLD, participants were allocated to OSAHS-only group (n = 72) and OSAHS + NAFLD group (n = 279). The anthropometric and polysomnographic characteristics of the patients were summarized in Table 1. We found that age, history of smoking, neck circumference (NC), waist circumference (WC) and BMI differed significantly between the groups (all P < 0.05), whereas gender, ESS score,and medical history, such as hypertension and diabetes did not. Furthermore, no significant differences were observed in polysomnographic parameters, including AHI, LaSO2, MaSO2, TS90% and ODI. However, the OSAHS + NAFLD group tended to have a higher AHI and a longer TS90% than the OSAHS-only group, suggesting that apnea and intermittent hypoxia were more severe in the OSAHS + NAFLD group.
Normally distributed data were expressed as mean ± SD, skewed data (including NC, WC, BMI, ESS score, AHI, LaSO2, MaSO2, TS90%, and ODI) were presented as median (interquartile range). Categorical variables were expressed as number (percentage). NC neck circumference, WC waist circumference, BMI Body mass index, ESS score Epworth Sleepiness Scale score, AHI apnea–hypopnea index, LaSO2 lowest O2 saturation, MaSO2 average O2 saturation, TS90% the percentage of total sleep time spent with SpO2 < 90%, ODI oxygen desaturation index.
Biochemical and hematological parameters in all participants
Biochemical and hematological parameters were reported in Table 2. There were no significant differences between two groups in terms of TC, TBIL, ALP or fasting glucose. However, OSAHS patients with NAFLD had significantly higher TG, ALT, AST, LDL-C, GGT, FLI and APRI than those without NAFLD (all P < 0.001), while had lower HDL-C levels than the OSAHS-only group (all P < 0.001). WBC/MPV, lymphocyte count, and white blood cell count were significant higher, while PLR was lower in OSAHS + NAFLD group. Nevertheless, there was a remarkable fact that no significant differences were observed in absolute value, such as PC, MPV, PDW, PCT and MPC (all P > 0.05). And the percentage of patients with upper limit of normal lymphocyte and white blood cell count was significant higher in OSAHS + NAFLD group than in OSAHS-only group (both P < 0.05), whereas there was no significant difference in the percentage of patients with upper limit of PC and MPV (both P > 0.05).
Correlation analysis of platelet-related parameters with NAFLD in OSAHS patients
Table 3 revealed the correlations between PC, MPV, PLR, WBC/MPV, and other variables. PLR was negatively correlated with NAFLD (r = −0.250, P < 0.001), whereas WBC/MPV was positively correlated with NAFLD (r = 0.241, P < 0.001). In addition, PLR was positively correlated with MaSO2 (r = 0.115, P = 0.035), and WBC/MPV was positively correlated with ALT (r = 0.163, P = 0.006). Furthermore, platelet count, as expressions of platelet activation, had a negative correlation with LaSO2 (r = -0.107, P = 0.045), while MPV had a positive correlation with TS90% (r = 0.126, P = 0.019), suggesting sleep apnea and intermittent hypoxia played important roles in platelet activation.
Predictors of NAFLD in OSAHS patients according to logistic regression analysis
Logistic regression analysis highlighted WBC/MPV as a significant predictor of NAFLD in OSAHS populations with the highest odds ratio (OR) after adjustment, reaching 7.559 (95% CI: 1.411–40.486, P = 0.018), followed by gender (OR: 3.672; 95% CI: 1.231–10.954, P = 0.020), BMI (OR: 1.191; 95% CI: 1.028–1.380, P = 0.020), MaSO2 (OR: 1.134; 95% CI: 1.011–1.272, P = 0.031), ALT (OR: 1.049; 95% CI: 1.017–1.083, P = 0.003), HDL-C (OR: 0.070; 95% CI: 0.013–0.396, P = 0.0003), and PLR (OR: 0.980; 95% CI:0.970–0.991, P < 0.001)(Table 4).
Comparison of the parameters in the predictive power of NAFLD in OSAHS
The results of the ROC curve analysis of the WBC/MPV, PLR, the combination of WBC/MPV and PLR, FLI, and APRI corresponding to 95% CI were shown in Table 5 and Figs. 1, 2, 3, 4 and 5. The AUC of NAFLD was the highest for FLI at 0.742 (95% CI 0.708–0.831), followed by the combination of WBC/MPV and PLR (0.743, 95% CI 0.684–0.801), PLR (0.679, 95% CI 0.618–0.740), WBC/MPV (0.664, 95% CI 0.602–0.741), and APRI (0.632, 95% CI 0.563–0.700) in all subjects. In the BMI subgroup analysis, the AUCs for the combination of WBC/MPV and PLR was 0.753 (95% CI 0.684–0.822), the highest in subjects with BMI < 28 kg/m2. In BMI ≥ 28 kg/m2 subjects, the AUC for the combination of WBC/MPV and PLR with NAFLD was 0.674 (95% CI 0.536–0.812), ranked only after FLI (0.764, 95% CI 0.636–0.892) and APRI (0.688, 95% CI 0.562–0.814). In the age subgroup analysis, the AUCs for the combination of WBC/MPV and PLR of age < 60 years old and age ≥ 60 years old with NAFLD were 0.729 (95% CI 0.652–0.806) and 0.786 (95% CI 0.692–0.880), which were the highest in age ≥ 60 years subgroup and the second highest in age < 60 years subgroup, respectively. Compared with the other four parameters, the most sensitive parameter for predicting NAFLD was the combination of WBC/MPV and PLR in BMI < 28 kg/m2 subgroup, BMI ≥ 28 kg/m2 subgroup, age < 60 years subgroup, and in all subjects.

ROC curves and relat ed AUCs for WBC/MPV, PLR, FLI, APRI, and the combination of WBC/MPV and PLR in predicting the occurrence of NAFLD in all subjects. AUC area under curve, BMI body mass index, PLR platelet to lymphocyte ratio, WBC/MPV white blood cell count to mean platelet volume ratio, FLI fatty liver index, APRI AST platelet ratio index, ROC receiver operating characteristic

ROC curves and related AUCs for WBC/MPV, PLR, FLI, APRI, and the combination of WBC/MPV and PLR in predicting the occurrence of NAFLD in BMI < 28 kg/m2 subgroup. AUC area under curve, BMI body mass index, PLR platelet to lymphocyte ratio, WBC/MPV white blood cell count to mean platelet volume ratio, FLI fatty liver index, APRI AST platelet ratio index, ROC receiver operating characteristic

ROC curves and related AUCs for WBC/MPV, PLR, FLI, APRI, and the combination of WBC/MPV and PLR in predicting the occurrence of NAFLD in BMI ≥ 28 kg/m2 subgroup. AUC area under curve, BMI body mass index, PLR platelet to lymphocyte ratio, WBC/MPV white blood cell count to mean platelet volume ratio, FLI fatty liver index, APRI AST platelet ratio index, ROC receiver operating characteristic

ROC curves and related AUCs for WBC/MPV, PLR, FLI, APRI, and the combination of WBC/MPV and PLR in predicting the occurrence of NAFLD in age < 60 years subgroup. AUC area under curve, BMI body mass index, PLR platelet to lymphocyte ratio, WBC/MPV white blood cell count to mean platelet volume ratio, FLI fatty liver index, APRI AST platelet ratio index, ROC receiver operating characteristic

ROC curves and related AUCs for WBC/MPV, PLR, FLI, APRI, and the combination of WBC/MPV and PLR in predicting the occurrence of NAFLD in age ≥ 60 years subgroup. AUC area under curve, BMI body mass index, PLR platelet to lymphocyte ratio, WBC/MPV white blood cell count to mean platelet volume ratio, FLI fatty liver index, APRI AST platelet ratio index, ROC receiver operating characteristic
Discussion
In this study, we evaluated platelet-related biomarkers as potential predictors of NAFLD among OSAHS participants. Logistic regression analysis identified WBC/MPV and MaSO2 as risk factors, while PLR as a protective factor for NAFLD in OSAHS populations. In addition, a combination of PLR and WBC/MPV showed a good prediction capacity regarding NAFLD compared with WBC/MPV, PLR, FLI, and APRI. Further subgroup ROC analysis indicated a combination of PLR and WBC/MPV presented the largest AUC for the detection of NAFLD in BMI < 28 kg/m2 subgroup (0.753, 95% CI 0.684–0.822), and in the age ≥ 60 years subgroup (0.786, 95% CI 0.692–0.880).
NAFLD has become more and more common worldwide, especially in the OSAHS populations, and it can result in a range of serious complications, including liver failure and even death [26], so if we can identify NAFLD as early as possible, and then carry out the preventive intervention, the mortality can be significantly reduced. Clinically, liver biopsy is the gold standard for screening NAFLD [27]. However, the invasiveness and high cost of liver biopsy have limited its application [28, 29]. In recent years, the relation between platelet-related parameters and liver diseases has caught the interest of many scientists since platelet-related parameters can represent the inflammatory state of the body and even provide the advantages of simplicity, cost-effectiveness, non-invasiveness, etc. [11,12,13].
Our study showed that AHI and TS90% were higher in the OSAHS + NAFLD group. Subsequent binary logistic regression analysis found that MaSO2 was an independent risk factor for NAFLD, suggesting that nocturnal hypoxia played an important role in the development of NAFLD in OSAHS participants. According to previous studies, nocturnal hypoxia was linked with systemic inflammation. He et al. [30] developed an IH 3T3-L1 adipocyte and rat model respectively, recapitulating the nocturnal oxygen profile in OSAHS. The findings demonstrated that NF-κB DNA binding activities were positively correlated with the severity of OSAHS in cellular models. Additionally, the mRNA and protein levels of TNF- and IL-6 increased with the severity of OSAHS in both cellular and animal models. Many researchers have demonstrated that the activation of inflammatory and apoptotic factors caused by nocturnal hypoxia contributes to the pathogenesis and progression of NAFLD in OSAHS individuals [31]. Polotsky et al. [32] studied 90 consecutive bariatric patients who underwent PSG, and reported that nocturnal oxygen desaturation might predispose them to hepatic inflammation, hepatocyte ballooning, and liver fibrosis. A series of researches have reported that liver injuries are initiated by histology-derived oxidative stress, with the initial inflammatory signaling cascade culminating in a positive feedback loop for oxidative stress and the activation of various inflammatory mediators, such as NF-κB, TNF-α, HIF-1a, etc., causing liver tissue microcirculation dysfunction and systemic inflammatory responses [33,34,35].
Platelets play a crucial role in liver injury and liver fibrosis. Ghafoory et al. [36] demonstrated that activated platelets were found during acute liver injury (6 h) in mice exposed to CCl4, and mice with temporary platelet depletion were partially protected against CCl4-induced fibrosis, indicating a link between platelet activation and fibrosis. Notably, platelets can cause sinusoidal endothelial cells to emit a significant number of chemokines and increase the migration of neutrophils and lymphocytes [37], which ultimately induces liver injury and fibrosis, indicating that an index representing platelets and inflammation may play a role in predicting NAFLD.
PLR, a newly discovered sensitive index of the inflammation system in the body, is able to reflect the state of inflammation [38]. PLR seemed to be mostly explored in chronic HBV/HCV and HCC patients, and prior research revealed that PLR levels were higher in those with more advanced HCC and a higher recurrence risk [14], while low levels of PLR were observed in chronic HBV/HCV patients [15]. To the best of our knowledge, this is the first study that presented the association between PLR and the occurrence of NAFLD in OSASH patients, even after adjusted for well-known risk factor for NAFLD in logistic regression analysis. In this study, PLR levels of OSAHS complicated in NAFLD group were lower than those of the OSAHS-only group, and PLR seemed to be a reliable predictor of NAFLD in the OSAHS population. Given that PLR is a composite indicator that comprises both platelets and lymphocytes, the activation and aggregation of platelets, as well as inflammation and immune responses in the body, may all play a part in the development of NAFLD in OSAHS patients. In addition, PLR was shown to be positively connected with MaSO2, implying that PLR is linked to hypoxia in this research. Prior studies have shown that oxyhemoglobin desaturation is associated with platelet activation [39,40,41], and that the severity of desaturation in OSAHS patients is positively associated with excess catecholamine levels [42]. Furthermore, it is known that increased shear stress owing to sympathetic nervous system activation and high blood pressure activates platelets, hence boosting inflammatory responses in numerous target organs, including the liver [42].
WBC/MPV is usually used to predict thrombosis-related events, particularly in cardiovascular, cerebrovascular, and peripheral vascular diseases. There hasn't been any research done on the link between WBC/MPV, OSAHS, and NAFLD. We used WBC/MPV to predict NAFLD in OSAHS patients in a novel way since both OSAHS and NAFLD can lead to pathological changes in the blood system. Our research indicated that WBC/MPV ratio was greater in the OSAHS + NAFLD group, and the WBC/MPV ratio was an independent risk factor for OSAHS complicated with NAFLD. According to previous studies, patients with NAFLD exhibited higher white blood cell and platelet counts. The increased expression of inflammatory markers in NAFLD patients may promote thrombopoietin development, resulting in larger platelets in the bone marrow and platelet activation, which in turn causes liver damage, and creates a vicious cycle. In our research, we found that a combination of WBC/MPV and PLR can better predict the occurrence of NAFLD compared to PLR or WBC/MPV alone.
In this study, we also compared the efficacy of PLR, WBC/MPV, FLI, APRI, and the combination of WBC/MPV and PLR to predict the occurrence of NAFLD in patients with OSAHS. FLI and APRI were non-invasive scores widely used in the prediction of NAFLD [21, 22]. And our study revealed that the combination of WBC/MPV and PLR had a good prediction capacity in NAFLD, only ranked after FLI in all subjects. Further subgroup analysis presented a fact that the combination of WBC/MPV and PLR had an even better performance in NAFLD prediction in BMI < 28 kg/m2, and in the age ≥ 60 years subgroup. To be emphasized, there was no significant differences in the absolute value of platelet count and MPV. However, PLR and WBC/MPV, the composite indicator, have better performances in predicting NAFLD. We hypothesized that stress, changes in blood volume in vivo, and changes in specimen fluid volume during testing operations may affect absolute values of platelet count, lymphocyte count, white blood cell, and MPV, resulting in improved sensitivity and resistance to interference when using composite indicators for disease prediction.
There are a few problems with this study. As a matter of fact, our study only included a limited number of patients, and each of those patients was only evaluated at a single location. Therefore, we were unable to avoid selection bias when gathering data. Second, the PLR and WBC/MPV ratios were evaluated using a single measurement at the time of admission for the preliminary diagnosis. In order to avoid interference brought on by measurement mistakes in the subsequent study, further blood procedures will be needed to carry out multiple times at a variety of time points. Third, because a liver biopsy was not possible, a diagnosis of fatty liver was made using liver ultrasonography rather than a biopsy of the liver. Despite the fact that a previous study found that ultrasonography had a sensitivity of 89% and a specificity of 93% for NAFLD, and that it was widely used in population-based studies because of its non-invasiveness and accessibility, ultrasound has limited sensitivity in individuals with an elevated BMI, and it does not reliably detect mild steatosis [43]. Future investigations utilizing more precise methods, such as liver biopsy, would be required to confirm the findings of this study. Even with the aforementioned limitations, our study is the first cohort study to explore the diagnostic value of PLR and WBC/MPV in NAFLD among OSAHS patients, providing a non-invasive, cost-efficient and convenient method in the early-detection of NAFLD.
Conclusion
PLR and WBC/MPV are closely related to liver inflammation in patients with OSAHS. PLR and WBC/MPC are potential risk factors for NAFLD. Furthermore, our findings highlighted the combination of PLR and WBC/MPV as an effective indicator of NAFLD in patients with OSAHS. Given the accessibility and simplicity of calculation, these indices could be widely used for screening NAFLD in individuals with OSAHS in clinical settings.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NAFLD:
-
Non-alcoholic fatty liver disease
- PLR:
-
Platelet to lymphocyte count ratio
- WBC/MPV:
-
White blood cell count to mean platelet volume ratio
- OSAHS:
-
Obstructive sleep apnea–hypopnea syndrome
- ROC curve:
-
The receiver operating characteristic curve
- MaSO2 :
-
Average oxygen saturation
- NAFL:
-
Non-alcoholic fatty liver
- NASH:
-
Non-alcoholic steatohepatitis
- Liver/spleen CT:
-
Liver/spleen computed tomography
- MRI:
-
Magnetic resonance imaging
- ESS:
-
Epworth sleepiness scale
- TG:
-
Triglyceride
- TC:
-
Total cholesterol
- PC:
-
Platelet count
- MPV:
-
Mean platelet volume
- PDW:
-
Platelet distribution width
- PCT:
-
Plateletcrit
- MPC:
-
Average concentration of platelet contents
- IQR:
-
Interquartile range
- NC:
-
Neck circumference
- WC:
-
Waist circumference
- BMI:
-
Body mass index
- AHI:
-
Apnea–hypopnea index
- LaSO2 :
-
Lowest O2 saturation
- MaSO2 :
-
Average O2 saturation
- TS90%:
-
The percentage of total sleep time spent with SpO2 < 90%,
- ODI:
-
Oxygen desaturation index
- AST:
-
Aspartate transaminase
- LDL-C:
-
Low-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- TBIL:
-
Total bilirubin
- ALP:
-
Alkaline phosphatase
- GGT:
-
Gamma-glutamyl transferase
- OR:
-
Odds ratio
- AUC:
-
Area under the ROC curve
- FLI:
-
Fatty liver index
- APRI:
-
Aspartate aminotransferase to platelet ratio index
References
Sun X, Seidman JS, Zhao P, Troutman TD, Spann NJ, Que X, Zhou F, Liao Z, Pasillas M, Yang X, et al. Neutralization of oxidized phospholipids ameliorates non-alcoholic steatohepatitis. Cell Metab. 2020;31(1):189-206.e188.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incid ence, and outcomes. Hepatology. 2016;64(1):73–84.
Wong RJ, Aguilar M, Cheung R, Perumpail RB, Harrison SA, Younossi ZM, Ahmed A. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting li ver transplantation in the United States. Gastroenterology. 2015;148(3):547–55.
Arısoy A, Sertoğullarından B, Ekin S, Özgökçe M, Bulut MD, Huyut MT, Ölmez Ş, Turan M. Sleep apnea and fatty liver are coupled via energy metabolism. Med Sci Monit. 2016;22:908–13.
Umbro I, Fabiani V, Fabiani M, Angelico F, Del Ben M. Association between non-alcoholic fatty liver disease and obstructive sleep apnea. World J Gastroentero. 2020;26(20):2669–81.
Chalasani N. Nonalcoholic fatty liver disease liver fat score and fat equation to predict and quantitate hepatic steatosis: promising but not prime time! Gastroenterology. 2009;137(3):772–5.
Duseja A, Chalasani N. Epidemiology and risk factors of nonalcoholic fatty liver disease (NAFLD). Hepatol Int. 2013;7(Suppl 2):755–64.
Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastro Hepat. 2013;10(11):686–90.
Nena E, Papanas N, Steiropoulos P, Zikidou P, Zarogoulidis P, Pita E, Constantinidis TC, Maltezos E, Mikhailidis DP, Bouros D. Mean platelet volume and platelet distribution Width in non-diabetic subjects with obstructive sleep apnoea syndrome: new indices of severity? Platelets. 2012;23(6):447–54.
de Jager CP, van Wijk PT, Mathoera RB, de Jongh-Leuvenink J, van der Poll T, Wever PC. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 2010;14(5):R192.
García-Núñez A, Jiménez-Gómez G, Hidalgo-Molina A, Córdoba-Doña JA, León-Jiménez A, Campos-Caro A. Inflammatory indices obtained from routine blood tests show an inflammatory state associated with disease progression in engineered stone silicosis patients. Sci Rep. 2022;12(1):8211.
Gasparyan AY, Ayvazyan L, Mukanova U, Yessirkepov M, Kitas GD. The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann Lab Med. 2019;39(4):345–57.
Pravisani R, Mocchegiani F, Isola M, Lorenzin D, Adani GL, Cherchi V, De Martino M, Risaliti A, Lai Q, Vivarelli M, et al. Postoperative trends and prognostic values of inflammatory and nutritional biomarkers after liver transplantation for hepatocellular carcinoma. Cancers (Basel). 2021;13(3):513.
Koseoglu S, Ozcan KM, Ikinciogullari A, Cetin MA, Yildirim E, Dere H. Relationship between neutrophil to lymphocyte ratio, platelet to lymphocyte ratio and obstructive sleep apnea syndrome. Adv Clin Exp Med. 2015;24(4):623–7.
Michalak A, Cichoż-Lach H, Guz M, Kozicka J, Cybulski M, Jeleniewicz W, Stepulak A. Towards an evaluation of alcoholic liver cirrhosis and nonalcoholic fatty liver disease patients with hematological scales. World J Gastroentero. 2020;26(47):7538–49.
Kosekli MA. Mean platelet volume and platelet to lymphocyte count ratio are associated with hepatitis B-related liver fibrosis. Eur J Gastroen Hepat. 2022;34(3):324–7.
Bae BK, Park HC, Yoo GS, Choi MS, Oh JH, Yu JI. The significance of systemic inflammation markers in intrahepatic recurrence of early-stage hepatocellular carcinoma after curative treatment. Cancers (Basel). 2022;14(9):2081.
Çiçek G, Açıkgöz SK, Yayla Ç, Kundi H, İleri M. White blood cell count to mean platelet volume ratio: a novel and promising prognostic marker for ST-segment elevation myocardial infarction. Cardiol J. 2016;23(3):225–35.
Emre AR, Yasar KA, Atakan Y, Orhan C, Murathan K. Relationship between white blood count to mean platelet volume ratio and clinical outcomes and severity of coronary artery disease in patients undergoing primary percutaneous coronary intervention. Cardiovasc Ther. 2020;2020:9625181.
Guetl K, Raggam RB, Muster V, Gressenberger P, Vujic J, Avian A, Hafner F, Wehrschuetz M, Brodmann M, Gary T. The White blood cell count to mean platelet volume ratio for the prediction of chronic limb-threatening ischemia in lower extremity artery disease. J Clin Med. 2019;8(10):1593.
Bedogni G, Bellentani S, Miglioli L, Masutti F, Passalacqua M, Castiglione A, Tiribelli C. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6:33.
Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, Lok AS. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–26.
Chen NH, Johns MW, Li HY, Chu CC, Liang SC, Shu YH, Chuang ML, Wang PC. Validation of a Chinese version of the Epworth sleepiness scale. Qual life res. 2002;11(8):817–21.
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events Deliberations of the Sleep Apnea. Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619.
National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association; Fatty Liver Expert Committee, Chinese Medical Doctor Association. Guidelines of prevention and treatment for nonalcoholic fatty liver disease: a 2018 update. Chin J Hepatol. 2018;26(3):195–203.
Loomba R, Friedman SL, Shulman GI. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell. 2021;184(10):2537–64.
Bedossa P, Patel K. Biopsy and noninvasive methods to assess progression of nonalcoholic fatty liver disease. Gastroenterology. 2016;150(8):1811-1822.e1814.
Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021;397(10290):2212–24.
Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, Sanyal AJ. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. 2012;142(7):1592–609.
He Q, Yang QC, Zhou Q, Zhu H, Niu WY, Feng J, Wang Y, Cao J, Chen BY. Effects of varying degrees of intermittent hypoxia on proinflammatory cytokines and adipokines in rat s and 3T3-L1 adipocytes. PLoS ONE. 2014;9(1): e86326.
Ye J, Gao Z, Yin J, He Q. Hypoxia is a potential risk factor for chronic inflammation and adiponectin reduction in adipose tissue of ob/ob and dietary obese mice. Am J Physiol Endocrinol Metab. 2007;293(4):E1118–28.
Polotsky VY, Patil SP, Savransky V, Laffan A, Fonti S, Frame LA, Steele KE, Schweizter MA, Clark JM, Torbenson MS, et al. Obstructive sleep apnea, insulin resistance, and steatohepatitis in severe obesity. Am J Resp Crit Care. 2009;179(3):228–34.
da Rosa DP, Forgiarini LF, e Silva MB, Fiori CZ, Andrade CF, Martinez D, Marroni NP. Antioxidants inhibit the inflammatory and apoptotic processes in an intermittent hypoxia model of sleep apnea. Inflamm Res. 2015;64(1):21–9.
Ryan S. Adipose tissue inflammation by intermittent hypoxia: mechanistic link between obstructive sleep apnoea and metabolic dysfunction. J Physiol-London. 2017;595(8):2423–30.
Liu Y, Dang W, Zhang S, Wang L, Zhang X. Artesunate attenuates inflammatory injury and inhibits the NF-κB pathway in a mouse model of cerebral ischemia. J Int Med Res. 2021;49(11):3000605211053549.
Ghafoory S, Varshney R, Robison T, Kouzbari K, Woolington S, Murphy B, Xia L, Ahamed J. Platelet TGF-¦Â1 deficiency decreases liver fibrosis in a mouse model of liver injury. Blood Adv. 2018;2(5):470–80.
Lurie A. Endothelial dysfunction in adults with obstructive sleep apnea. In: Lurie A, editors. Obstructive sleep apnea in adults. Adv Cardiol, vol 46. Basel: Karger; 2011. p.139–70.
Yang C, Wen HB, Zhao YH, Huang WH, Wang ZF, Li ZQ. Systemic inflammatory indicators as prognosticators in glioblastoma patients: a comprehensive meta-analysis. Front Neurol. 2020;11:580101.
Oga T, Chin K, Tabuchi A, Kawato M, Morimoto T, Takahashi K, Handa T, Takahashi K, Taniguchi R, Kondo H, et al. Effects of obstructive sleep apnea with intermittent hypoxia on platelet aggregability. J Atheroscler Thromb. 2009;16(6):862–9.
Minoguchi K, Yokoe T, Tazaki T, Minoguchi H, Oda N, Tanaka A, Yamamoto M, Ohta S, O’Donnell CP, Adachi M. Silent brain infarction and platelet activation in obstructive sleep apnea. Am J Resp Crit Care. 2007;175(6):612–7.
Rahangdale S, Yeh SY, Novack V, Stevenson K, Barnard MR, Furman MI, Frelinger AL, Michelson AD, Malhotra A. The influence of intermittent hypoxemia on platelet activation in obese patients with obstructive sleep apnea. J Clin Sleep Med. 2011;7(2):172–8.
Kaditis AG, Alexopoulos EI, Damani E, Hatzi F, Chaidas K, Kostopoulou T, Tzigeroglou A, Gourgoulianis K. Urine levels of catecholamines in Greek children with obstructive sleep-disordered breathing. Pediatr Pulm. 2009;44(1):38–45.
Joseph AE, Saverymuttu SH. al-Sam S, Cook MG, Maxwell JD: comparison of liver histology with ultrasonography in assessing diffuse parenchymal liver disease. Clin Radiol. 1991;43(1):26–31.
Acknowledgements
Not applicable.
Funding
This work was supported by National Natural Science Foundation (No. 82070088), and Fujian Provincial Health Technology Project (No. 2020GGA044). The funding bodies played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
MLC and JFH sequence data analysis and preparation of the manuscript; BYW, study design, experiments and manuscript preparation; GPC, contributed in experimental design; JMZ, analyzed data; JC, collected data; MLC and BYW contributed equally to this work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research was approved by institutional review board in the First Affiliated Hospital of Fujian Medical University. The study was conducted in accordance with the Declaration of Helsinki. All procedures were performed in accordance with the relevant guidelines and regulations. Written informed consent were obtained from all subjects prior to participation in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, M., Wang, B., Huang, J. et al. The role of platelet-related parameters for the prediction of NAFLD in OSAHS patients. BMC Pulm Med 22, 487 (2022). https://doi.org/10.1186/s12890-022-02291-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-02291-6