
Abstract
Background
No consensus has been reached on an optimal blood lactate evaluation system although several approaches have been reported in the literature in recent years. A group-based trajectory modeling (GBTM) method could better stratify patients with acute respiratory distress syndrome (ARDS) complicated with sepsis in the intensive care unit (ICU).
Patients and methods
760 patients from the comprehensive ICU of Tianjin Medical University General Hospital with ARDS complicated with sepsis were eligible for analysis. Serial serum lactate levels were measured within 48 h of admission. In addition to the GBTM lactate groups, the initial lactate, peak lactate level, the area under the curve of serial lactate (lactate AUC), and lactate clearance were also considered for comparison. The short- and long-term outcomes were the 30- and 90-day mortality, respectively.
Results
Three lactate groups were identified based on GBTM, with group 3 exhibiting the worse short- [hazard ratio (HR) for 30-day mortality: 2.96, 95% confidence interval (CI) 1.79–4.87, P < 0.001] and long term (HR for 90-day mortality: 3.49, 95% CI 2.06–5.89, P < 0.001) outcomes followed by group 2 (HR for 30-day mortality: 2.05, 95% CI 1.48–2.84, P < 0.001 and HR for 90-day mortality: 1.99, 95% CI 1.48–2.67, P < 0.001). GBTM lactate groups exhibited significantly improved diagnostic performance of initial lactate + SOFA scores/APACHE II scores models. Based on the multivariable fractional polynomial interaction (MFPI) approach, GBTM lactate groups could better differentiate high-risk patients than the initial lactate groups in short- and long-term outcomes.
Conclusions
To the best of our knowledge, this is the first report that GBTM-based serial blood lactate evaluations significantly improve the diagnostic capacity of traditional critical care evaluation systems and bring many advantages over previously documented lactate evaluation systems.
Similar content being viewed by others

Background
Elevated lactate levels are common in the setting of sepsis and usually represent an imbalance between increased production in the presence or absence of tissue hypoxia and changes in clearance [1]. Given their well-established association with multiple organ dysfunction [2], blood lactate levels and their trend over time are increasingly recognized as reliable markers of illness severity and mortality [3,4,5,6,7]. Border and Weil et al. observed that lactate levels ≥ 4 mmol/L were associated with a 50% mortality in patients with shock during a study period of 36 h [8]. An increasing body of evidence suggests that lactate measurements represent a valuable and straightforward indicator for the early identification of severe sepsis and are associated with poor outcomes [9,10,11,12,13]. Interestingly, current evidence suggests that compared with initial lactate levels at presentation or other single measured lactate values, serial blood lactate level measurements can better characterize the dynamic process of lactate production and elimination in vivo [2]. Serial lactate levels can also help define the patient's trajectory and encourage a review of the therapeutic strategy [14]. Over the years, the prognostic value of serial measurements of multiple types of lactate levels or calculations from lactate levels has been investigated, for example, the duration of hyperlactatemia [15], the area under the curve of serial lactate measurement (lactate AUC) [16], and lactate clearance [17]. Importantly, decreased lactate levels were associated with improved outcomes in almost all critically ill patients [5]. Moreover, the later the lactate level is reduced, the worse the clinical prognosis is [18].
Despite the long-standing predictive power and the prominent place of lactate levels in early goal-directed therapy for critically ill patients, there is still a lack of a dynamic and flexible method to identify high-risk patients with hyperlactatemia. Given the lag in blood lactate concentration observed during testing, it remains unclear how lactate levels affect clinical management [19]. Notwithstanding that it is well-recognized that poor outcomes in ARDS patients are often attributed to sepsis/multiple organ failure rather than respiratory failure per se [20], few studies have hitherto focused on the predictive value of lactate for the prognosis of acute respiratory distress syndrome (ARDS) patients, along with the hypoxia process [1]. Indeed, a better understanding of the association between lactate and poor prognosis in ARDS patients complicated with sepsis upon admission is required.
We validated that lactate levels are elevated in septic patients with ARDS based on cohort data, including serial measurements of blood lactate over a period. A recently developed statistical method, also known as group-based trajectory modeling (GBTM), was harnessed to identify clusters of individuals exhibiting similar progression of a specific measurement over time and to identify the association between lactate trajectory within 48 h and short- and long-term outcomes of ARDS patients complicated with sepsis. Meanwhile, although several lactate evaluation systems have been documented, including initial serum lactate levels, we sought to validate that novel subtypes of lactate based on GBTM algorithm yield better diagnostic value.
Methods
Study design, patients
This was a single-center, retrospective observational study where patients discharged from the comprehensive intensive care unit of Tianjin Medical University General Hospital from January 2019 to March 2022 were enrolled. Patients with the following conditions were excluded: (1) patients discharged within 48 h of admission; (2) patients without admission arterial blood gas analysis measurements; (3) patients not diagnosed with ARDS and sepsis; and (4) patients with repeated admissions. The diagnosis of ARDS was made according to the criteria stated by the American-European Consensus Conference (AECC) on ARDS at admission [21]. In addition, we excluded patients whose clinical entities can present with PaO2/FiO2 < 300 mmHg without being ARDS (atelectasis, volume overload, and left heart failure). The diagnosis of sepsis during ICU stay is based on the consensus Sepsis-3 definitions at admission [9], which is the SOFA score of the patient within 24 h of admission. We routinely measure the plasma lactate concentration (via long-term arterial catheterization) by a COBAS B-123 POC system (Roche Diagnostics, Rotkreuz, Switzerland) every 6 h in all patients during ICU stay. Besides the initial lactate measurement, missing values were allowed for the other time points. The patients were followed up through outpatient visits, telephone calls or hospital readmission records. This study was approved by the Ethics Committee of Tianjin Medical University General Hospital (IRB2022-YX-041-01) and conducted in accordance with the ethical standards of the Declaration of Helsinki. The need for informed consent was waived due to the retrospective nature of our study. Reporting of the study followed the guidelines from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [22]. We declare that ARDS due to coronavirus disease 2019 (COVID-19) is not involved in patients eligible for inclusion.
Study variables
The study variables used for analysis included patient demographics (age, sex), past medical history (hypertension, diabetes, coronary artery disease, stroke, renal failure, cancer), clinical characteristics upon admission [levels of systolic and diastolic blood pressure (SBP and DBP), heart rate, estimated glomerular filtration rate (eGFR), fluid intake per hour, fluid outtake per hour, red blood cell (RBC), white blood cell (WBC), platelet, hemoglobin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin, Glasgow Coma Scale (GCS) [23], Acute Physiology And Chronic Health Evaluation II (APACHE II) score [24] and Sequential Organ Failure Assessment (SOFA) score [25], PaO2/FiO2 classification, emergency surgical operation, invasive mechanical ventilation, and other inpatient treatment within 24 h of admission [antibiotics, sedative/analgesic, glucocorticoid, continuous renal replacement therapy (CRRT), low molecular weight heparin (LMWH), sodium bicarbonate, vasoactive medications, and blood component transfusion]. The eGFR was calculated according to the Chronic Kidney Disease Epidemiology Collaboration equation [26]. The definition of the above study variables is listed in Additional file 1: Table S1. Except for the APACHE II and SOFA scores, all the above parameters were included as covariables in the multivariate Cox proportional-hazards model. In addition, the initial lactate was also included during model adjustment.
In addition to the lactate groups based on the GBTM algorithm (GBTM lactate groups), the following lactate evaluation criteria were also considered in this study for comparison: (1) initial lactate level; (2) peak lactate level; (3) lactate AUC; (4) lactate clearance. The calculation of lactate AUC is shown in Additional file 1: Fig. S1.
For variables with missing values, we imputed the missing data using MissForest, a random forest imputation algorithm for missing data implemented in R (version 4.0.0) [27]. The missing rates of the study variables are shown in Additional file 1: Table S2.
Study outcomes
The study outcomes of this study were the performance of GBTM lactate groups in the prediction of the short- (30-day mortality) and long-term (90-day mortality) outcomes.
Statistical analysis
STATA 17.0 (StataCorp, College Station, TX) was used for statistical analysis. A two-tailed P-value < 0.05 was statistically significant. To capture the pattern changes of each blood lactate parameter, we used GBTM to identify distinct subgroups that shared a similar trajectory. Since the blood lactate levels were not normally distributed, the data were first logarithmically transformed. We fitted models with up to three latent classes and up to cubic polynomials. The optimal number of trajectory classes and trajectory shapes were selected based on the following criteria [28]: (1) a censored normal model for continuous tendency toward a parsimonious model, (2) the higher value of Bayesian information criterion (BIC) and Akaike information criterion (AIC), (3) each trajectory group had the odds of correct classification by weighted posterior proportions > 5, (4) each trajectory group had an average posterior probability of membership > 0.80 and (5) the expected number based on the sums of the posterior probabilities should be the same as in the proportion in each group based on the assignments for the maximum posterior probability.
To determine whether GBTM lactate groups could refine the diagnostic performance for short- and long-term outcomes, we compared the changes in AUC, net reclassification improvement (NRI) and integrated discrimination improvement (IDI) after incorporating the identified GBTM lactate groups, peak lactate value, lactate clearance and lactate AUC into the established models (initial lactate + SOFA score/APACHE II score).
The baseline characteristics between groups were reported as the means (± SD) for normally distributed data and medians with 25th and 75th percentiles for non-parametric data. Categorical variables were summarized using percentages. Differences between groups were compared using Fisher's exact test for data with a binomial distribution. The Mann–Whitney U test and unpaired t-test were used for group comparisons of continuous variables with skewed and normal distributions, respectively. The associations between GBTM lactate groups and short- and long-term risk were estimated using multivariable Cox proportional hazard analyses. Box-Whisker plots and 3D scatter plots were used to describe the GBTM lactate group characteristics by prior lactate evaluation systems.
Finally, the GBTM lactate groups and initial lactate groups were compared. The initial lactate groups were defined as group 1: ≤ 2 mmol/L; group 2: 2–4 mmol/L; and group 3: ≥ 4 mmol/L. We used the multivariable fractional polynomial interaction (MFPI) approach [29] to investigate potential interactions between group assignment (group 2 vs. 1 and group 3 vs. 1) and continuous variables such as age, eGFR, SOFA score, and APACHE II score for short- and long-term outcomes. All MFPI analyses were adjusted for covariates mentioned above. We decided to use only fractional polynomial degree 2 functions to analyze interactions. MFPI was used to estimate a fractional polynomial function for each group representing the prognostic effect of the continuous covariate of interest, optionally adjusting for other covariates. The covariables involved in adjustments are described in the section "2.2 Study Variables". A P-value < 0.05 was statistically significant for covariate selection. To quantify the magnitude of effects, we estimated hazard ratio (HR) with pointwise 95% confidence intervals (CI) as a continuous treatment effect. We adopted the 10th to the 90th quantile of distribution for the four continuous indicators.
Results
Patient characteristics
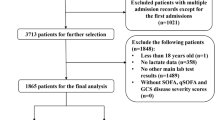
From January 2019 to March 2022, 1,548 patients were discharged from the comprehensive ICU of Tianjin Medical University General Hospital. As shown in Fig. 1, 760 patients were included in the final analysis. 255 and 302 patients experienced mortality at 30- and 90-day, respectively. There were no cases of loss to follow-up. The initial diagnosis of these eligible patients when admitted to ICU is shown in Additional file 1: Table S3. Comparisons of short- and long-term outcomes are shown in Additional file 1: Table S4. For both short- and long-term outcomes, lactate levels at all time points within 48 hours, peak lactate levels, and lactate AUC were significantly higher in the group with adverse events.

A schematic overview illustrating participant enrollment and the exclusion and inclusion criteria. ICU, intensive care unit
Trajectories of serial blood lactate within 48 h after admission to the ICU based on the GBTM algorithm
As shown in Fig. 2, based on the GBTM algorithm, after considering parsimony and assessing the relative changes in model fitting at each step, we selected a model with three latent groups and linear, quadratic, and linear polynomials (see Additional file 1: Table S5 for parameters for models fitted with different numbers of latent groups and different degrees of polynomials). GBTM lactate groups 1, 2, and 3 accounted for 53.8% (n = 409), 38.9% (n = 296) and 7.24% (n = 55) of patients, respectively. The baseline characteristics of the groups are shown in Table 1. The blood pressure, platelet count, and albumin were significantly reduced. In contrast, heart rate, fluid intake per hour, WBC, ALT, AST, APACHE II score, and SOFA scores were significantly increased from group 1 to group 3 and required more treatment, including emergency surgical operation, invasive mechanical ventilation support, sedative/analgesic, glucocorticoid, CRRT, intravenous sodium bicarbonate, vasoactive medications, and blood component transfusion.

The blood lactate trajectories based on GBTM. The data were log-transformed before modeling. The dashed lines indicate 95% confidence intervals of each trajectory
As shown in Additional file 1: Fig. S2A, compared with group 1, groups 2 and 3 were characterized by significantly increased initial lactate, peak lactate level, lactate clearance, and lactate AUC (Additional file 1: Table S6 for details). A "funnel shape" 3D scatter plot was observed when three dimensions (initial lactate, peak lactate value, and lactate AUC) were considered (Additional file 1: Fig. S2B).
Associations between GBTM lactate groups and short- and long-term outcomes
The GBTM lactate group 3 exhibited the worst (HR for 30-day mortality: 2.96, 95% CI 1.79–4.87, P < 0.001; HR for 90-day mortality: 3.49, 95% CI 2.06–5.89, P < 0.001) outcomes followed by the GBTM lactate group 2 (HR for 30-day mortality: 2.05, 95% CI 1.48–2.84, P < 0.001; HR for 90-day mortality: HR: 1.99, 95% CI 1.48–2.67, P < 0.001). The Cox hazard curves are shown in Fig. 3. When the GBTM lactate groups were added to the initial lactate models + SOFA score, there were significant increases in the established models' AUC value for short- (0.737 vs. 0.704, P = 0.009) and long-term outcomes (0.724 vs. 0.689, P = 0.004) with enhanced risk of reclassification capacity (positive and significant continuous NRI values), as well as IDI values. Furthermore, the GBTM lactate groups + initial lactate + SOFA score yielded the highest predictive performance compared with the models where the lactate AUC, lactate clearance and peak lactate level were added to the initial lactate + SOFA score (Fig. 4). These results were consistent in initial lactate + APACHE II score models (Additional file 1: Fig. S3).

Survival analysis by GBTM lactate groups. Multivariable Cox proportional hazard analyses by GBTM lactate groups with respect to 30- (left) and 90-day mortality (right). CI, confidence intervals; HR, hazard ratio

Comparison of diagnostic capacity. The AUC, IDI, and NRI for the combined assessment of diagnostic capacity when incorporating the GBTM lactate groups, peak lactate level, lactate clearance and lactate AUC into the established model (SOFA score + initial lactate). All P values represent comparisons with the established model (SOFA score + initial lactate). AUC, area under curve; IDI, integrated discrimination improvement; GBTM, group-based trajectory modeling; NRI, net reclassification improvement; SOFA score, Sequential Organ Failure Assessment score
Comparison of the nonlinearity on age, eGFR, SOFA score, and APACHE II score between GBTM lactate groups and initial lactate groups assignment with respect to short- and long-term outcomes
The baseline characteristics based on initial lactate levels are shown in Additional file 1: Table S7. The initial lactate groups 1, 2, and 3 accounted for 54.6% (n = 415), 27.2% (n = 207) and 18.2% (n = 138) of the cases, respectively. Compared with initial lactate group 1, group 2 experienced a 1.62- (HR: 1.62, 95% CI 1.19–2.22) and 1.77-fold (HR: 1.77, 95% CI 1.34–2.36) greater risk of short- and long-term mortality, respectively. The short- (HR: 1.80, 95% CI 1.25–2.59) and long-term (HR: 1.70, 95% CI 1.20–2.40) risks in group 3 were indistinguishable from those in group 2 (Additional file 1: Fig. S4).
Using the MFPI procedure, non-linearities in survival were found for the GBTM lactate groups/initial lactate groups combined with age, eGFR, SOFA score, and APACHE II score. As seen in Fig. 5, GBTM lactate group 3 experienced higher 90-day mortality than group 2 and was clearly separated and consistent across multiple continuous indicators (despite the overlap of CI). However, based on the initial lactate groups, the risk of groups 3 and 2 could not be well discriminated. GBTM lactate groups can better identify high-risk patients on four continuous scales. Compared with the GBTM lactate group 1, age, eGFR, SOFA score (8–21) and APACHE II score (11–26) were statistically significant in 100%, 100%, 72.7% (40/55), and 60.0% (33/55) of GBTM lactate group 3 patients [with the lower 95% CI above the line of equivalence (HR: 1)]. In the GBTM lactate group 2, the age, eGFR, SOFA score and APACHE II achieved statistical significance in 61.1% (181/296), 65.9% (195/296), 72.6% (215/296), and 87.8% (260/296) of the total population in group 2. In contrast, no significant difference in the four continuous parameters were found in the initial lactate groups. Hence, high-risk patients could not be identified. No significant interaction was observed across the four continuous parameters. The 30-day mortality was also roughly consistent with the above results (Additional file 1: Fig. S5).

MFPI analysis. A plot of estimated HRs of the nonlinearity on age, eGFR, SOFA score, and APACHE II score between GBTM lactate groups and initial lactate groups assignment with respect to 90-day mortality. The solid red and blue lines represent the estimated HRs of groups 3 and 2 compared to group 1. The red and blue dashed lines near them represent the CIs corresponding to the HRs, respectively. The horizontal black dashed lines denote HR of 1. A transparent blue histogram of the background represents the distribution of continuous variables. Except for SOFA scores, for the rest three continuous indicators, we adopted the 10th to the 90th quantile of distribution. APACHE II score, Acute Physiology And Chronic Health Evaluation II score; CI, confidence intervals; eGFR, estimated glomerular filtration rate; GBTM, group-based trajectory modeling; HR, hazard ratio; SOFA score, Sequential Organ Failure Assessment score
Discussion
In this retrospective cohort study of ARDS patients complicated with sepsis in the ICU, we validated the presence of elevated lactate levels in ARDS patients with sepsis. Importantly, this is the first study to document the value of GBTM-based serial blood lactate evaluations to significantly improve the diagnostic capacity of traditional critical care evaluation systems compared to previously described lactate approaches. Interestingly, we used the MFPI algorithm to demonstrate that GBTM lactate groups yield superior performance in identifying high-risk patients than initial lactate groups for both short- and long-term outcomes.
Sepsis/multiple organ failure is well-established as a common cause of mortality in ARDS patients, and improvement in clinical outcomes may depend more on the management of sepsis/multiple organ failure than on oxygenation measures alone [20]. It is widely acknowledged that blood lactate level is a useful marker of the severity of sepsis or multiple organ failure, with higher levels predictive of higher mortality [9]. The peak lactate level has been initially applied in various blood lactate evaluation systems [8]. However, it should be borne in mind that tissue hypoperfusion and hypoxia may be present with elevated lactate levels before routine hemodynamic measurements change [30]. Therefore, initial measurements of lactate levels in the ICU are valuable for early identification. Mikkelsen et al. found that the initial serum lactate was associated with mortality independent of clinically apparent organ dysfunction and shock in patients admitted to the emergency department with severe sepsis [10]. Early initial lactate-guided therapy can significantly reduce ICU mortality [11]. Overwhelming evidence substantiates that initial blood lactate levels ranging from 2.0 to 4.0 mmol/L are associated with poor outcomes [9, 10, 12, 13]. The initial lactate is simple to calculate and readily available in all institutions. However, a single measurement of the lactate concentration can be challenging to interpret, especially in patients with ARDS, since it reflects a balance between lactate production and elimination. In this study, we divided the initial lactate into three groups with 2.0 mmol/L and 4.0 mmol/L as cut-off values for comparison with the GBTM lactate groups. The high initial lactate group exhibited lower mortality rates than the corresponding GBTM-based lactate group. The initial lactate groups exhibited lower survival during survival curve analysis than the GBTM lactate groups (Additional file 1: Fig. S4). More importantly, we specifically compared GBTM lactate groups with the initial lactate groups using the MFPI algorithm. Both high (group 3) and low (group 2) initial lactate groups did not correspond well to relative high-risk and low-risk clinical outcomes on the pre-specified continuous age, eGFR, SOFA score, and APACHE II score, nor could it obtain the high-risk interval with statistical significance. Taken together, our findings substantiate that GBTM lactate groups are more advantageous than the initial lactate groups.
Since continuous blood lactate levels assessment may provide more information than individual values, serial blood lactate measurements have been proposed [31]. Subsequently, the concepts of hyperlactatemia duration [15], lactate clearance [17], and lactate AUC [16] have been recommended. In our study, GBTM-based lactate groups could roughly cover patients with high initial blood lactate, peak lactate level and lactate AUC values (Additional file 1: Fig. S2B), with group 3 more tightly associated with the three parameters than group 2 or 1. Accordingly, the GBTM groups could account for findings in the above four lactate evaluation systems. Findings in GBTM lactate groups were not driven by individual parameters such as initial lactate, peak lactate value, lactate AUC, etc., but by a combination of these. In addition, GBTM lactate groups exhibited significantly enhanced diagnostic performance of the established model of SOFA score/APACHE II score with the addition of initial lactate. Meanwhile, the AUC, NRI and IDI obtained by adding GBTM lactate groups were the largest compared with established models where lactate AUC, lactate clearance and the peak lactate values were added, suggesting better diagnostic efficacy.
Several limitations and shortcomings were present in this study. Given its retrospective design, our study may have been subject to systematic errors and biases with missing values for serial lactate measurements. Nevertheless, the random forest data interpolation method based on machine learning [27], known to outperform all other data interpolation methods [32], was used to handle the missing data. Moreover, as an observational study, we could not establish a causal relationship between lactate groups and clinical outcomes and exclude the impact of potential confounders. Indeed, we could not include these potential confounders during multivariate analysis due to the lack of data, such as body mass index. Given the strong association between lactate groups and short- or long-term outcomes and the consistency of trends for continuous indicators during MFPI, it is highly unlikely that these factors can affect the conclusions of this study. Due to a lack of information (such as bilateral infiltration on chest roentgenogram), we could not use the Berlin definition [33] to define patients with ARDS. However, we exclude patients with clinical entities can present with PaO2/FiO2 < 300 mmHg without being ARDS (atelectasis, volume overload, left heart failure) based on the initial diagnosis at ICU admission. Moreover, due to the study's retrospective nature, we could not determine the causal relationship between ARDS and sepsis. Given that the sample size in the study was small, our findings may have been biased in favor of effect size inflation, and the statistical ability may be insufficient to detect the correct number of tracks when using GBTM. Hence, future GBTM-based prospective studies with larger sample sizes are required to validate our findings.
Conclusions
The GBTM-based serial lactate evaluation method significantly improved the diagnostic capacity of traditional critical care evaluation systems and possessed many advantages over previously described lactate evaluation systems, especially over groups based on initial lactate levels. Importantly, GBTM-based serial lactate evaluation improved the identification of individuals at high risk of short- and long-term mortality in our retrospective cohort study of ARDS patients complicated with sepsis in the ICU.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIC:
-
Akaike information criterion
- ALT:
-
Alanine aminotransferase
- APACHE II:
-
Acute Physiology And Chronic Health Evaluation II
- ARDS:
-
Acute respiratory distress syndrome
- AST:
-
Aspartate aminotransferase
- AUC:
-
Area under the curve
- BIC:
-
Bayesian information criterion
- CI:
-
Confidence interval
- CRRT:
-
Continuous renal replacement therapy
- DBP:
-
Diastolic blood pressure
- eGFR:
-
Estimated glomerular filtration rate
- GBTM:
-
Group-based trajectory modeling
- GCS:
-
Glasgow Coma Scale
- HR:
-
Hazard ratio
- ICU:
-
Intensive care units
- IDI:
-
Integrated discrimination improvement
- MFPI:
-
Multivariable fractional polynomial interaction
- NRI:
-
Net reclassification improvement
- RBC:
-
Red blood cell
- SBP:
-
Systolic blood pressure
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
- SOFA:
-
Sequential Organ Failure Assessment
- WBC:
-
White blood cell
References
Bakker J, Nijsten MW, Jansen TC. Clinical use of lactate monitoring in critically ill patients. Ann Intensive Care. 2013;3:12.
Bakker J, Gris P, Coffernils M, Kahn RJ, Vincent JL. Serial blood lactate levels can predict the development of multiple organ failure following septic shock. Am J Surg. 1996;171:221–6.
Weil MH, Afifi AA. Experimental and clinical studies on lactate and pyruvate as indicators of the severity of acute circulatory failure (shock). Circulation. 1970;41:989–1001.
Bakker J, Coffernils M, Leon M, Gris P, Vincent JL. Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock. Chest. 1991;99:956–62.
Vincent JL, Quintairos ESA, Couto L Jr, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20:257.
Shapiro NI, Howell MD, Talmor D, Nathanson LA, Lisbon A, Wolfe RE, et al. Serum lactate as a predictor of mortality in emergency department patients with infection. Ann Emerg Med. 2005;45:524–8.
Nichol A, Bailey M, Egi M, Pettila V, French C, Stachowski E, et al. Dynamic lactate indices as predictors of outcome in critically ill patients. Crit Care. 2011;15:R242.
Broder G, Weil MH. Excess lactate: an index of reversibility of shock in human patients. Science. 1964;143:1457–9.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315:801–10.
Mikkelsen ME, Miltiades AN, Gaieski DF, Goyal M, Fuchs BD, Shah CV, et al. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock. Crit Care Med. 2009;37:1670–7.
Jansen TC, Van Bommel J, Schoonderbeek FJ, Sleeswijk Visser SJ, Van Der Klooster JM, Lima AP, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752–61.
Howell MD, Donnino M, Clardy P, Talmor D, Shapiro NI. Occult hypoperfusion and mortality in patients with suspected infection. Intensive Care Med. 2007;33:1892–9.
Wacharasint P, Nakada TA, Boyd JH, Russell JA, Walley KR. Normal-range blood lactate concentration in septic shock is prognostic and predictive. Shock. 2012;38:4–10.
Vincent JL, Bakker J. Blood lactate levels in sepsis: in 8 questions. Curr Opin Crit Care. 2021;27:298–302.
Jansen TC, Van Bommel J, Woodward R, Mulder PG, Bakker J. Association between blood lactate levels, Sequential Organ Failure Assessment subscores, and 28-day mortality during early and late intensive care unit stay: a retrospective observational study. Crit Care Med. 2009;37:2369–74.
Van Beest PA, Brander L, Jansen SP, Rommes JH, Kuiper MA, Spronk PE. Cumulative lactate and hospital mortality in ICU patients. Ann Intensive Care. 2013;3:6.
Zhang Z, Xu X. Lactate clearance is a useful biomarker for the prediction of all-cause mortality in critically ill patients: a systematic review and meta-analysis*. Crit Care Med. 2014;42:2118–25.
Kliegel A, Losert H, Sterz F, Holzer M, Zeiner A, Havel C, et al. Serial lactate determinations for prediction of outcome after cardiac arrest. Medicine (Baltimore). 2004;83:274–9.
Vink EE, Bakker J. Practical use of lactate levels in the intensive care. J Intensive Care Med. 2018;33:159–65.
Ferring M, Vincent JL. Is outcome from ARDS related to the severity of respiratory failure? Eur Respir J. 1997;10:1297–300.
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–24.
Vandenbroucke JP, Von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Ann Intern Med. 2007;147:W163–94.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–4.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
Moreno R, Vincent JL, Matos R, Mendonça A, Cantraine F, Thijs L, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM. Intensive Care Med. 1999;25:686–96.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12.
Stekhoven DJ, Bühlmann P. MissForest–non-parametric missing value imputation for mixed-type data. Bioinformatics. 2012;28:112–8.
Anderson-Cook C. Group-based modeling of development. J Am Stat Assoc. 2006. https://doi.org/10.5860/choice.43-1258.
Royston P, Sauerbrei W. A new approach to modelling interactions between treatment and continuous covariates in clinical trials by using fractional polynomials. Stat Med. 2004;23:2509–25.
Rady MY, Rivers EP, Nowak RM. Resuscitation of the critically ill in the ED: responses of blood pressure, heart rate, shock index, central venous oxygen saturation, and lactate. Am J Emerg Med. 1996;14:218–25.
Vincent JL, Dufaye P, Berré J, Leeman M, Degaute JP, Kahn RJ. Serial lactate determinations during circulatory shock. Crit Care Med. 1983;11:449–51.
Waljee AK, Mukherjee A, Singal AG, Zhang Y, Warren J, Balis U, et al. Comparison of imputation methods for missing laboratory data in medicine. BMJ Open. 2013;3:e002847.
Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–33.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
KX and YY conceived and designed the study, supervised the analysis process, interpreted the data, and revised the manuscript. HZ, ZL and LZ analyzed the data and drafted the manuscript. WZ and TY helped to analyze the data and generate the tables and figures. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethical Committee of Tianjin Medical University General Hospital (IRB2022-YX-041-01) in accordance with the Declaration of Helsinki, with a waiver for informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
. Definition of study variables. Table S2. Missing rates of study variables. Table S3. Initial ICU admission diagnosis of eligible patients. Table S4. Baseline characteristics by study outcomes. Table S5. The parameter for fitted models with different numbers of latent groups and different degrees of polynomials. Table S6. Baseline lactate characteristics between GBTM lactate groups. Table S7. Baseline characteristics by initial lactate. Figure S1. Calculation of lactate AUC. Figure S2. Comparisons and descriptions of GBTM lactate groups by initial lactate, peak lactate level, lactate clearance and lactate AUC. Figure S3. The ROC with associated AUC, IDI, and NRI, for the combined assessment of diagnostic capacity when incorporating the GBTM lactate groups, peak lactate level, lactate clearance and lactate AUC respectively into the established model (APACHE II score + initial lactate). Figure S4. Multivariable Cox proportional hazard analyses by initial lactate groups with respect to 30- (left) and 90-day mortality (right). Figure S5. A plot of estimated HRs of the nonlinearity on continuous age, eGFR, SOFA score, and APACHE II score between GBTM lactate groups and initial lactate groups assignment with respect to 30-day mortality.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, H., Li, Z., Zheng, W. et al. Risk stratification of patients with acute respiratory distress syndrome complicated with sepsis using lactate trajectories. BMC Pulm Med 22, 339 (2022). https://doi.org/10.1186/s12890-022-02132-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-02132-6