
Abstract
Background
Secondary organizing pneumonia (SOP) is difficult to distinguish from cryptogenic organizing pneumonia (COP) considering various clinical situations. SOP caused by Mycobacterium tuberculosis is rare; indeed, it has not been reported as a sequela of disseminated tuberculosis.
Methods
From January 2016 to December 2018, we identified six cases of tuberculosis-associated SOP in which Mycobacterium tuberculosis was revealed by microbiological examination; one of the cases was miliary tuberculosis.
Results
Of the six cases, 17% were positive for acid fast bacillus (AFB) stain, but 100% were positive for M. tuberculosis polymerase chain reaction (MTB PCR) and AFB culture. In all cases, transbronchial lung biopsy was performed and organizing pneumonia was confirmed pathologically. All survived after treatment with anti-tuberculosis therapy.
Conclusions
Pulmonary tuberculosis, which shows OP in lung biopsy, is diagnosed through MTB PCR and AFB culture, and the prognosis is thought to be good.
Similar content being viewed by others


Background
Organizing pneumonia (OP) is pathologically defined as the presence of organized polypoid granulation tissue in alveolar ducts and alveoli bronchioles, with or without bronchiolar organization [1, 2]. OP is classified as cryptogenic (idiopathic) OP (COP) or secondary OP (SOP). SOP refers to OP caused by a known cause, and representative examples include infection, connective tissue disease, drugs, inflammatory bowel disease, hematologic malignancies, organ transplantations and radiation therapy [2, 3]. Post-respiratory infection SOP occurs after an infectious pneumonia, such as viruses, bacteria, fungi, or parasites [4, 5]. It can also be caused by Mycobacterium tuberculosis, although rarely [6,7,8,9]; to date, disseminated tuberculosis has not been reported as SOP. According to statistics in 2017, Korea is a country with a prevalence of tuberculosis in 70 people per 100,000 population, but so far there has been only one case report on tuberculosis-related OP. Here, we report six cases of SOP that occurred after M. tuberculosis infection, including disseminated tuberculosis, and review the current literature.
Methods
This retrospective study is based on a review of medical records of patients that underwent lung biopsy at the Department of Respiratory Medicine at Daegu Catholic University Medical Center between January 2016 and December 2018 to confirm OP. In total, 85 OP cases were identified pathologically, and microbiological data obtained during the same period was collected to confirm SOP. SOP was 66 (77.6%) out of 85 cases, with infection-related SOP (54 cases) including pulmonary tuberculosis, followed by cancer, radiation therapy, connective tissue disease, and drugs. The study was approved by the local institutional review board (No. CR-19-069). The requirement for informed consent was waived.
Microbial information was confirmed by acid fast bacillus (AFB) smear, AFB culture, and M. tuberculosis polymerase chain reaction (MTB PCR) of sputum, bronchial wash fluid, and tissue (if necessary) to prove the presence of M. tuberculosis. Pulmonary tuberculosis was diagnosed by MTB PCR of bronchial wash fluid or sputum; false-positives were eliminated by cross referencing the PCR results with clinical, AFB smear, and culture results. In addition, even if the AFB smear was positive, samples were further tested using MTB PCR or AFB culture prior to a final diagnosis of pulmonary tuberculosis.
Lung biopsy was performed when the pneumonia was in the form of a mass, there was no improvement in treatment, or the pneumonia pattern needed to be differentiated from other diseases.
The lung biopsy results revealed six SOP cases with proven pulmonary tuberculosis. Patient characteristics, symptoms, smoking history, underlying disease, medication history, laboratory test results, chest radiographs, treatments, response to treatment, drug sensitivity test using absolute concentration method, and death were investigated retrospectively. All patients were followed up for 12 months. In addition, we reviewed all articles reporting SOP related to pulmonary tuberculosis.
Results
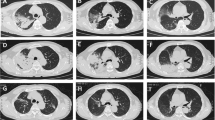
The case series are summarized in Table 1. The Fig. 1 shows the radiologic features, and the Fig. 2 shows the pathologic features of these cases. The Fig. 3 shows the chest X ray (CXR) and computed tomography (CT) before and after treatment.

Chest computed tomography (CT) scan features of all six cases. a Case 1. Consolidation in both upper lobes and pleural effusion. Transbronchial lung biopsy (TBLB) was performed in the left upper lobe. b Case 2. Consolidation in the left lower lobe, which was subjected to TBLB. c Case 3. A thick-walled cavity is present in the right upper lobe, which was subjected to TBLB. d Case 4. Consolidation in the right lower and left lower lobes. TBLB was performed in the right lower lobe. e Case 5. Multiple nodules with patchy consolidation in both lungs. TBLB was performed in the right middle lobe. f Case 6. A solitary pulmonary nodule in the right upper lobe, which was subjected to TBLB

Lung pathologic features of all six cases. There were organizing polypoid granulation tissue plugs within alveolar ducts and terminal bronchioles. a Case 1, b Case 2, c Case 3, d Case 4, f Case 6. H & E stain, X 100. e Case 5. X200

Pre-treatment and post-treatment chest images of all six cases. a Case 1, b Case 2, c Case 3, d Case 4, e Case 5, f Case 6. In each case, ‘-Pre’ means before treatment and ‘-Post’ means after treatment. ‘E-2mo Tx’ means chest X ray at 2mo of treatment in case 5
Case 1
An 81-year-old male visited hospital with a 3-day history of anorexia, fever, cough, and phlegm. Examination at the time of the visit revealed the following: blood pressure (BP), 137/62 mmHg; pulse rate (PR), 103 beats/min; respiratory rate (RR), 20 breaths/min; body temperature (BT), 37.7 °C, and peripheral saturation, 95% on room air. CXR (Fig. 3a-Pre) and CT (Fig. 1a) revealed lobar consolidation in both upper lung fields, focal consolidation in right middle and right lower lobes, and bilateral pleural effusion. A complete blood count revealed the leukocyte number to be 7400/uL (neutrophils, 81.9%). Other laboratory values were as follows: hemoglobin (Hb), 9.8 g/dL; erythrocyte sedimentation rate (ESR), 20 mm/hr. (normal range, 0–10 mm/hr); C-reactive protein (CRP), 45.5 mg/L (normal, < 5 mg/L); procalcitonin, 0.14 ng/mL (normal < 0.5 ng/mL); pro-B-type natriuretic peptide (pro-BNP), 1271 pg/mL (normal range, 17.5–158.2 pg/mL); Na, 130 mEq/L; blood urea nitrogen (BUN), 5.9 mg/dL; creatinine (Cr), 0.7 mg/dL; and albumin, 1.6 g/dL. An anti-HIV antibody screening test was negative. After starting antibiotic treatment for community acquired pneumonia, a sputum AFB smear was negative, but the sputum MTB PCR was positive. Therefore, he received a diagnosis of pulmonary tuberculosis and was treated with isoniazid, rifampin, ethambutol, and pyrazinamide. After 2 weeks, CXR was unable to rule out malignancy and did not improve, so CT was taken. We performed transbronchial lung biopsy (TBLB) and bronchial washing under radial probe endobronchial ultrasonography (R-EBUS). The biopsy revealed OP with small granuloma (Fig. 2a). Anti-tuberculosis treatment was continued due to a positive AFB stain and MTB PCR of the bronchial wash fluid. Subsequent AFB culture confirmed M. tuberculosis, which was sensitive to all anti-tuberculosis drugs. No steroid was used. A further follow-up CXR (Fig. 3a-Post) showed an improvement in his condition.
Case 2
A 72-year-old male visited the hospital with a recent history of cough, phlegm and increased focal opacity in of left lower lung field (LLLF) on CXR (Fig. 3b-Pre). On admission, BP was 120/70 mmHg, PR was 90/min, RR was 20/min, and BT was 36.6 °C. Chest CT showed consolidation in the LLLF (Fig. 1b). The leukocyte count was 4700/uL (neutrophils, 58%), Hb was 12.6 g/dL, ESR was 26 mm/hr., CRP was 5.3 mg/L, procalcitonin was 0.03 ng/mL, Na was 139 mEq/L, BUN was 15.1 mg/dL, Cr was 0.8 mg/dL, and albumin was 2.8 g/dL. An anti-HIV antibody screening test was negative. To confirm the cause of pneumonia, TBLB and bronchoalveolar lavage (BAL) were performed under R-EBUS. The lung biopsy results suggested OP (Fig. 2b). AFB stain of bronchial wash fluid was negative, but the MTB PCR was positive. Since the biopsy and radiologic examination results did not show findings appropriate for TB, the MTB PCR result was determined to be a false-positive. Therefore, he received corticosteroid treatment while maintaining antibiotic treatment. CXR showed that LLLF infiltration improved after steroids, but 3 weeks later M. tuberculosis was confirmed on AFB culture of BAL fluid. Therefore, the steroid was discontinued and anti-tuberculosis treatment was started. The microbe was sensitive to all anti-tuberculosis drugs and CXR revealed that all lesions improved thereafter (Fig. 3b-Post).
Case 3
A 54-year-old female patient was transferred to the clinic due to identification of a speculated mass measuring 3.2 × 2.8 cm in right upper lobe (RUL) on CXR and chest CT (Fig. 1c), accompanied by a fever lasting 4 days. Upon hospitalization, BP was 120/70 mmHg, PR was 78/min, RR was 20 /min, and BT was 36.9 °C. The leukocyte count was 7500/uL (neutrophils, 51.9%), Hb was 15.3 g/dL, ESR was 6 mm/hr., CRP was 1.4 mg/L, Na was 142 mEq/L, BUN was 16 mg/dL, Cr was 0.6 mg/dL, and albumin was 4.7 g/dL. No anti-HIV antibody screening test was performed. Antibiotic treatment was based on a diagnosis of pneumonia, and TBLB and bronchial washing were performed under R-EBUS to exclude malignancy. The biopsy results revealed OP (Fig. 2c). AFB stain of the bronchial wash fluid was negative, but MTB PCR was positive. Therefore, we made a diagnosis of pulmonary tuberculosis and began anti-tuberculosis treatment. An AFB culture test confirmed M. tuberculosis, which was sensitive to all drugs. No steroids were used. After 6 months of anti-tuberculosis treatment, chest CT revealed that the mass lesions on the RUL had improved (Fig. 3c-Post).
Case 4
A 57-year-old male patient visited the emergency room with a 3-week history of generalized weakness and dyspnea. At the time of the visit his BP was 134/72 mmHg, his PR was 118/min, his RR was 20/min, his BT was 36.1 °C, and room air oxygen saturation was 90%. CXR (Fig. 3d-Pre) and Chest CT revealed multiple micronodules distributed randomly in both lungs, accompanied by cavitary nodules, irregular linear opacity, and patchy consolidation in both apices. He was diagnosed with miliary tuberculosis with active pulmonary tuberculosis. The leukocyte count was 4500/uL (neutrophils, 93.2%), Hb was 14.5 g/dL, ESR was 8 mm/hr., CRP was 213 mg/L, procalcitonin was 17.65 ng/mL, Na was 114 mEq/L, BUN was 81.2 mg/dL, Cr was 2 mg/dL, and albumin was 2.9 g/dL. An anti-HIV antibody screening test was negative. Sputum AFB stain was negative, but MTB PCR was positive; therefore, he received anti-tuberculosis drugs (isoniazid, rifampin, ethambutol and pyrazinamide). Follow-up chest CT revealed increased diffuse consolidation and ground glass opacity (GGO) in both lungs (Fig. 1d). Mechanical ventilator treatment began on the 22nd day of hospitalization due to hypoxia. To confirm the cause of the exacerbation we performed a blind TBLB and BAL. The BAL AFB stain was negative, and the MTB PCR results were positive. The biopsy results confirmed OP (Fig. 2d) and so he received corticosteroids while continuing anti-tuberculosis treatment. Subsequently, as hypoxia and CXR improved, the patient was extubated on the 12th day of ventilator treatment. M. tuberculosis was cultured in sputum and was confirmed to be sensitive to all drugs. The steroid was tapered for a total of 6 months and although anti-tuberculosis drug treatment continued, rifampin was stopped due to leukopenia and ethambutol was stopped due to impaired vision. The patient received anti-tuberculosis treatment (isoniazid, pyrazinamide, and levofloxacin) for 18 months. After treatment was completed, CXR showed that all lesions had improved (Fig. 3d-Post).
Case 5
A 78-year-old male was admitted to the emergency room due to fainting and near drowning while sitting in a bathtub. At the time of the visit, his BP was 100/60 mmHg, his PR was 126/min, his RR was 23/min, his BT was 37.8 °C, and his peripheral saturation was 83% on nasal O2 (4 L/min). Chest CT revealed suspected pulmonary edema with diffuse patchy consolidations and GGO with a crazy paving pattern in both lungs. The leukocyte count was 5400/uL (neutrophils, 61.3%), Hb was 11.3 g/dL, ESR was 6 mm/hr., CRP was 0.6 mg/L, procalcitonin was 13.16 ng/mL, BNP was 253 pg/mL, Na was 131 mEq/L, BUN was 13.1 mg/dL, and Cr was 0.9 mg/dL. The anti-HIV antibody screening test was negative. The patient’s medical history and imaging findings suggested a high probability of pulmonary edema, but procalcitonin was high and a mild fever of > 37.8 °C persisted. Therefore, antibiotic treatment was started for suspected pneumonia, along with diuretics. CXR (Fig. 3e-Pre) showed new infiltration in both lungs, so Chest CT (Fig. 1e) was followed up on the 10th day of hospitalization. In chest CT, new diffuse centrilobular nodules with multifocal conglomerated nodules were observed in both lungs. TBLB and BAL were performed under R-EBUS to identify the cause. AFB stain of the BAL fluid was negative, but the MTB PCR was positive; therefore, anti-tuberculosis drugs were started. The biopsy confirmed OP (Fig. 2e), but no steroids were given. M. tuberculosis was identified on BAL AFB culture, which was sensitive to all drugs. Anti-tuberculosis drugs were used for 2 months. CXR tracking confirmed that the lesions improved (Fig. 3e-2mo Tx). However, side effects occurred and, despite providing medical care about side effects, he stopped all medications on his own after 2 months. The patient is just being followed as he wanted.
Case 6
A 70-year-old male visited the clinic due to identification of a 2.7 cm solitary pulmonary nodule on CXR (Fig. 3f-Pre) and CT (Fig. 1f). At the time of the visit, his BP was 121/74 mmHg, his PR was 62/min, his RR was 20/min, and his BT was 36.4 °C. The leukocyte count was 6200/uL (neutrophils, 57.8%), Hb was 12.1 g/dL, Na was 134 mEq/L, BUN was 9.7 mg/dL, Cr was 0.8 mg/dL, and albumin was 4.4 g/dL. No anti-HIV antibody screening test was performed. No antibiotics were used. TBLB and bronchial washing were performed under R-EBUS; the biopsy confirmed OP (Fig. 2e). AFB staining of the bronchial washing fluid was negative, but the MTB PCR was positive, so anti-tuberculosis treatment was started due to a diagnosis of pulmonary tuberculosis. M. tuberculosis was confirmed by AFB culture and was sensitive to all drugs. Steroids were not used. After 6 months of anti-tuberculosis treatment, CXR revealed that the RUL nodular lesion had improved (Fig. 3f-Post).
Discussion
OP is triggered by lung injury. The alveolar epithelium reacts to lung damage and produces granulation tissue. Inflammatory debris fills the alveoli, alveolar ducts, and terminal bronchioles, with characteristic endoluminal buds of granulation tissue known as the Masson body [10]. SOP is caused by infection-induced lung injury, drug toxicity, inhalation of a pathogen (e.g., cocaine), inhalation of toxic gas, gastroesophageal reflux, connective tissue disorders, organ transplantation, or radiation [3, 11, 12], but SOP caused by tuberculosis is rare. Here, we describe six cases (Table 1) of tuberculosis-related SOP and conducted a literature review (Table 2).
Symptoms and microbial test results
COP has an acute and subacute course. Symptoms include coughing, dyspnea, and fever, meaning that it can easily be mistaken for infectious pneumonia and treated initially with antibiotics for several weeks [13, 14]. However, even if OP is diagnosed by performing a biopsy after a patient exhibits slow clinical improvement, efforts should be made to differentiate the cause, bearing in mind the possibility of SOP. Cases 1–3 and case 5 reported herein were treated initially with antibiotics due to suspected pneumonia. Although the biopsy results of all four patients confirmed OP, and all AFB stains of the initial respiratory samples were negative, it was possible to initiate anti-tuberculosis treatment relatively early because the MTB PCR was positive [15]. It should be borne in mind that tuberculosis is a possible cause of OP in regions such as Korea, which have a relatively high prevalence of tuberculosis. Therefore, when performing a bronchoscopy to obtain a biopsy, a tuberculosis test such as MTB PCR will help to confirm whether SOP is present.
Our literature review to collect articles reporting OP associated with M. tuberculosis infection identified five cases published worldwide (Table 2) [6,7,8,9]. The AFB smear of bronchial washing fluid was positive in only one case, reported by Yoon et al. [8]; it was negative in bronchial washing fluid or sputum in the other four cases [6,7,8,9]. MTB PCR of bronchial washing fluid was positive in one case because MTB PCR was performed in only two cases [8]. All lung tissue had OP histologically, but in only two cases was the AFB smear positive in lung tissue [6, 9]. Eventually, all cases were AFB culture-positive in bronchial washing fluid or sputum, confirming a diagnosis of tuberculosis.
Taking the six cases reported herein along with the other five reported worldwide, only 18% showed a positive result (i.e., OP associated with M. tuberculosis infection) for the AFB smear of respiratory samples. MTB PCR of respiratory specimens was positive in seven out of eight cases (87.5%). AFB culture was positive for all respiratory specimens. In areas in which the prevalence of tuberculosis is high, confirming MTB PCR with a respiratory sample is likely to make the diagnosis faster even if the biopsy revealed OP.
Biopsy methods
In our study, case 4 underwent blind TBLB because the lesion was diffuse; the other five cases had localized lesions and, after confirming the lesion with R-EBUS without fluoroscopy, TBLB was performed. It was possible to obtain an appropriate sample without pneumothorax by performing R-EBUS [16]. Ma et al. [17] reported that R-EBUS increases the accuracy of OP diagnosis, with fewer side effects. OP is best diagnosed from a surgical lung biopsy, but this is associated with an increased risk of morbidity and mortality. Many studies reported improvements in treatment decision making after diagnosis of OP with TBLB [4, 18, 19]. OP is more likely to appear as GGO or consolidation on the chest CT than as a nodule or mass [10, 20]. Often, tissue biopsy via bronchoscopy is often performed blind; in such cases it is difficult to obtain tissue from an accurate location. In our study, an exact histological diagnosis of OP was possible in the five patients who underwent R-EBUS-guided TBLB due to accurate localization of the lesion.
Treatments
In our study, all six cases received anti-tuberculosis treatment, which improved the lung lesions. However, in case 2, the lung lesions improved after administration of steroids prior to anti-tuberculosis treatment. In case 4, the condition progressed to acute respiratory distress syndrome (ARDS) during anti-tuberculosis treatment; the cause was confirmed to be OP, so pulmonary lesions improved after administration of steroids together with anti-tuberculosis treatment. Among the articles identified in the literature review (Table 2), we found two cases that improved after anti-tuberculosis treatment without steroid treatment [8]. However, there was one case in which the pulmonary lesion was improved after administration of steroids before tuberculosis was diagnosed [7]; this is similar to case 2 in our study. Lawn et al. [6] reported a case of ARDS similar to case 4 in our study; OP and tuberculosis were demonstrated at postmortem biopsy. In this case, steroid use may have helped improve the prognosis. In case 4, despite the use of anti-tuberculosis drugs after a diagnosis of military tuberculosis, ARDS developed and the improved after steroid administration.
The occurrence of pathological reactions in tuberculosis is inextricably linked with the host’s response to the invading M. tuberculosis. The immunologic response to M. tuberculosis is likely responsible for the characteristic presentation of tuberculosis [21]. As in case 4, in the case of a patient with insufficient Immune response, it would have been expressed in the form of a disseminated infection, although not human immunodeficiency virus (HIV). In this case, it is thought that the pulmonary inflammation worsened after using tuberculosis drugs, such as immune reconstitution inflammatory syndrome (IRIS).
The use of corticosteroids in pulmonary tuberculosis has been and remains controversial. A controlled trial reported by Johnson et al. [22] demonstrated that corticosteroid treatment most benefited the seriously ill patient (defined by low serum albumin concentration, low body weight, and severe weight loss) who had extensive tuberculosis. This benefit was evidenced mainly by an increase in the rate of radiographic clearing; there was no adverse effect on the bacteriologic response. Similar results can be found in a systemic review [23]. And steroids may also be of benefit in patients with marked abnormalities of gas exchange and respiratory failure [24, 25]. But, in less severely ill patients, methylprednisolone was either of no benefit or actually decreased the speed of sputum conversion [25]. The fact that steroids can be helpful when ARDS worsen despite anti-tuberculosis treatment is probably due to the lung pathology as OP.
All cases in our study were sensitive to antibiotics used to treat tuberculosis and all survived. Therefore, tuberculosis-associated SOP has a good prognosis.
All the patients were told about their disease and received anti-tuberculosis treatment (isoniazid, rifampin, ethambutol, pyrazinamide). However, a case 5 patient refused to treat anti-tuberculosis medication due to his side effects (neuralgia and anorexia), which did not finish the entire drug duration despite the side effects treatment.
Biopsy features
If AFBs is transported to and reached the lungs, but the host’s defense system fails to clear the infection, the AFB proliferates inside the alveolar macrophages and kills the cells. Infected macrophages produce cytokines that attract other phagocytes, eventually forming nodular granulomas. Histologically, tuberculosis is characterized by granuloma, which is a cellular aggregate; macrophages and lymphocytes are important for formation of granulomas [26, 27]. Granulomas have been traditionally considered to be host-protective structures, thought to “wall off” bacteria and keep them from disseminating. Whereas this view may apply in later stages of fibrotic and calcified granulomas, early granuloma formation actually promotes infection by facilitating cell-to-cell spread within the macrophage aggregates, thus optimizing expansion of the bacterial population [25]. However, OP is characterized histologically by fibrosis and organized granulation tissue in the alveoli; fibroblasts play an important role and are recruited in response to alveolar epithelial cell injury [4]. In case 1, OP and granuloma were present; according to Huo et al. [28], the presence of epithelioid cell granulomas or giant multinucleated cells in OP is associated with an infectious etiology [7]. In this case, it is predicted that, in some areas, an immune response to typical tuberculosis occurs and, in some areas, fibroblasts are activated due to alveolar epithelial cell injury, thus showing up as OP. In cases 2–6, we could not confirm granuloma histologically; since we cannot biopsy all the lungs, we believe that the area with OP is biopsied. Granulomatous formation caused by a cellular immune response may be in the lungs that are not biopsied. Further research is needed.
Since this case series showed small numbers of cases, it may be limited in general application.
Conclusions
Pulmonary tuberculosis can be a cause of SOP. In areas with high tuberculosis prevalence, we suggest that performing tuberculosis-related tests, especially MTB PCR, is useful for early diagnosis and treatment of tuberculosis related OP, even if the lung biopsy results show OP. The prognosis of tuberculosis related OP is thought to be good.
Availability of data and materials
All authors had access to data and material and vouch for its complete accuracy. Literature review can be accessed through Pubmed and Google Scholar. Data and materials can be accessed through the medical records at Daegu Catholic University Medical Center. All images are available through PACS imaging system storage at Daegu Catholic University Medical Center.
Change history
14 April 2022
Following the original publication of this article, the authors flagged that a required funding statement was missing from the Funding declaration; please see the linked correction for further details.
28 April 2022
A Correction to this paper has been published: https://doi.org/10.1186/s12890-022-01938-8
Abbreviations
- OP:
-
Organizing pneumonia
- COP:
-
Cryptogenic organizing pneumonia
- SOP:
-
Secondary organizing pneumonia
- AFB:
-
Acid fast bacillus
- MTB PCR:
-
Mycobacterium tuberculosis polymerase chain reaction
- BP:
-
Blood pressure
- PR:
-
Pulse rate
- RR:
-
Respiration rate
- BT:
-
Body temperature
- CXR:
-
Chest X ray
- CT:
-
Computed tomography
- Hb:
-
Hemoglobin
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- Pro-BNP:
-
Pro-B-type natriuretic peptide
- Na:
-
Sodium
- BUN:
-
Blood urea nitrogen
- Cr:
-
Creatinine
- TBLB:
-
Transbronchial lung biopsy
- R-EBUS:
-
Radial probe endobronchial ultrasound
- LLLF:
-
Left lower lung field
- BAL:
-
Bronchoalveolar lavage
- RUL:
-
Right upper lobe
References
European RS, Society AT. American Thoracic Society/European Respiratory Society international multidisciplinary consensus classification of the idiopathic interstitial pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS executive committee, June 2001. Am J Respir Crit Care Med. 2002;165(2):277.
Epler GR, Colby TV, McLoud TC, Carrington CB, Gaensler EA. Bronchiolitis obliterans organizing pneumonia. N Engl J Med. 1985;312(3):152–8.
Epler GR. Bronchiolitis obliterans organizing pneumonia, 25 years: a variety of causes, but what are the treatment options? Expert Rev Respir Med. 2011;5(3):353–61.
Cordier J. Cryptogenic organising pneumonia. Eur Respir J. 2006;28(2):422.
Drakopanagiotakis F, Polychronopoulos V, Judson MA. Organizing pneumonia. Am J Med Sci. 2008;335(1):34–9.
Lawn SD, Wainwright H, Orrell C. Fatal unmasking tuberculosis immune reconstitution disease with bronchiolitis obliterans organizing pneumonia: the role of macrophages. AIDS. 2009;23(1):143–5.
Sander R, Gómez C, Borderías L. Organizing pneumonia and pulmonary tuberculosis: coexistent or associated diseases. Archivos Bronconeumol (English Edition). 2016;52(11):570–1.
Yoon HS, Lee EJ, Lee JY, Chon GR, Lee SH, Kim SJ. Organizing pneumonia associated with M ycobacterium tuberculosis infection. Respirol Case Rep. 2015;3(4):128–31.
Hsieh M-H, Lin C-Y. Pulmonary tuberculosis presenting as organizing pneumonia. Am J Respir Crit Care Med. 2014;189(9):e63.
Baque-Juston M, Pellegrin A, Leroy S, Marquette CH, Padovani B. Organizing pneumonia: what is it? A conceptual approach and pictorial review. Diagn Interv Imaging. 2014;95(9):771–7.
Gómez-Gómez A, Martínez-Martínez R, Gotway MB. Organizing pneumonia associated with swine-origin influenza a H1N1 2009 viral infection. Am J Roentgenol. 2011;196(1):W103–4.
Roberton BJ, Hansell DM. Organizing pneumonia: a kaleidoscope of concepts and morphologies. Eur Radiol. 2011;21(11):2244.
Alasaly K, Muller N, Ostrow DN, Champion P, Fitz Gerald JM. Cryptogenic organizing pneumonia. A report of 25 cases and a review of the literature. Medicine (Baltimore). 1995;74(4):201–11.
Sen T, Udwadia ZF. Cryptogenic organizing pneumonia: clinical profile in a series of 34 admitted patients in a hospital in India. J Assoc Physicians India. 2008;56:229–32.
Kim EJ. A tuberculosis-associated Endobronchial polyp that was negative for acid-fast Bacillus. Intern Med. 2018;57(18):2701–4.
Kim EJ, Kim KC. Utility of radial probe Endobronchial ultrasound-guided Transbronchial lung biopsy in diffuse lung lesions. Tuberc Respir Dis. 2019;82(3):201–10.
Ma M, Li Y, Cai H-R, Ding J-J, Wang Y-S, Gao Y-J, Dai J-H, Zhao Q, Xiao Y-L, Meng F-Q. Radial probe Endobronchial ultrasound-guided lung biopsy for Histopathological diagnosis of cryptogenic organizing pneumonia. Chin Med J. 2017;130(2):236.
Lazor R, Vandevenne A, Pelletier A, Leclerc P, Court-Fortune I, Cordier JF. Cryptogenic organizing pneumonia. Characteristics of relapses in a series of 48 patients. The Groupe d’Etudes et de Recherche sur les Maladles “Orphelines” Pulmonaires (GERM“O”P). Am J Respir Crit Care Med. 2000;162(2 Pt 1):571–7.
Li Y, Li Y, Han F, Yu H, Yang T, Li H, Guan W, Guo X. Case report cryptogenic organising pneumonia: clinical, pathological, and prognostic analysis of 27 cases. Int J Clin Exp Med. 2016;9(3):6911–9.
Lee JW, Lee KS, Lee HY, Chung MP, Yi CA, Kim TS, Chung MJ. Cryptogenic organizing pneumonia: serial high-resolution CT findings in 22 patients. Am J Roentgenol. 2010;195(4):916–22.
Ernst JD. The immunological life cycle of tuberculosis. Nat Rev Immunol. 2012;12(8):581–91.
Johnson J, Turk T, MacDonald F. Corticosteroids in pulmonary tuberculosis: II. Importance of background factors. Am Rev Respir Dis. 1967;96(1):43–61.
Smego R, Ahmed N. A systematic review of the adjunctive use of systemic corticosteroids for pulmonary tuberculosis. Int J Tuberc Lung Dis. 2003;7(3):208–13.
Huseby JS, Hudson LD. Miliary tuberculosis and adult respiratory distress syndrome. Ann Intern Med. 1976;85(5):609–11.
Murray and Nadel’s Textbook of Respiratory Medicine, 20ed. 2016, 35:593–628.
Flynn J, Chan J, Lin P. Macrophages and control of granulomatous inflammation in tuberculosis. Mucosal Immunol. 2011;4(3):271.
Rubin EJ. The granuloma in tuberculosis—friend or foe? N Engl J Med. 2009;360(23):2471–3.
Huo Z, Feng R, Tian X, Zhang H, Huo L, Liu H. Clinicopathological findings of focal organizing pneumonia: a retrospective study of 37 cases. Int J Clin Exp Pathol. 2015;8(1):511–6.
Acknowledgements
Not Applicable.
Funding
This work was supported by research grants from Daegu Catholic University in 2019.
Author information
Authors and Affiliations
Contributions
EJK contributed with literature review, drafting and revising the final draft. KCK helped with reviewing, formatting, and revising the final draft of the manuscript. All authors listed above read and approved this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This case series was approved by the institutional review board of Daegu Catholic University Medical Center (No. CR-19-069). The requirement for informed consent was waived. Patients in these cases and the information department of this hospital allowed access and use of medical records.
Consent for publication
Written informed consent was obtained from patients for publication of this report and identifying images or other personal or clinical details.
Competing interests
All authors listed above have no conflicts of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Article corrected in 2022.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kim, E.J., Kim, K.C. Pulmonary tuberculosis presenting secondary organizing pneumonia with organized polypoid granulation tissue: case series and review of the literature. BMC Pulm Med 20, 252 (2020). https://doi.org/10.1186/s12890-020-01292-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-020-01292-7