
Abstract
Background
Quantitative evidence on the impact of meteorological factors on influenza transmissibility across different virus types/subtypes is scarce, and no previous studies have reported the effect of hourly temperature variability (HTV) on influenza transmissibility. Herein, we explored the associations between meteorological factors and influenza transmissibility according to the influenza type and subtype in Guangzhou, a subtropical city in China.
Methods
We collected influenza surveillance and meteorological data of Guangzhou between October 2010 and December 2019. Influenza transmissibility was measured using the instantaneous effective reproductive number (Rt). A gamma regression with a log link combined with a distributed lag non-linear model was used to assess the associations of daily meteorological factors with Rt by influenza types/subtypes.
Results
The exposure-response relationship between ambient temperature and Rt was non-linear, with elevated transmissibility at low and high temperatures. Influenza transmissibility increased as HTV increased when HTV < around 4.5 °C. A non-linear association was observed between absolute humidity and Rt, with increased transmissibility at low absolute humidity and at around 19 g/m3. Relative humidity had a U-shaped association with influenza transmissibility. The associations between meteorological factors and influenza transmissibility varied according to the influenza type and subtype: elevated transmissibility was observed at high ambient temperatures for influenza A(H3N2), but not for influenza A(H1N1)pdm09; transmissibility of influenza A(H1N1)pdm09 increased as HTV increased when HTV < around 4.5 °C, but the transmissibility decreased with HTV when HTV < 2.5 °C and 3.0 °C for influenza A(H3N2) and B, respectively; positive association of Rt with absolute humidity was witnessed for influenza A(H3N2) even when absolute humidity was larger than 19 g/m3, which was different from that for influenza A(H1N1)pdm09 and influenza B.
Conclusions
Temperature variability has an impact on influenza transmissibility. Ambient temperature, temperature variability, and humidity influence the transmissibility of different influenza types/subtypes discrepantly. Our findings have important implications for improving preparedness for influenza epidemics, especially under climate change conditions.
Similar content being viewed by others


Introduction
Influenza is a significant threat to public health worldwide. Each year, seasonal influenza causes approximately three to 5 million cases of severe illness and 290,000–650,000 respiratory deaths globally [1]. Influenza seasonality varies across climatic zones. Specifically, influenza commonly peaks during winter in temperate zones [2], whereas its seasonality is more complicated and difficult to predict in subtropical and tropical regions with semi-annual peaks or year-round activity [3].
Understanding the drivers of influenza transmission will inform preventive and control measures. Previous studies have attempted to reveal the potential role of meteorological factors (e.g., ambient temperature and humidity) and school closure in modulating influenza transmission [4,5,6,7,8]. However, different findings on the association between meteorological variables and influenza transmissibility have been reported in previous studies [5,6,7,8]. For example, Zhang et al. detected increased influenza transmissibility at both low and high ambient temperatures in China [7], whereas Zhang et al. did not observe increased transmissibility at high temperature in Guangzhou, China [8]. Regarding the association between outdoor absolute humidity and influenza transmissibility, U-shaped [5], non-linear inverse [8], and statistically non-significant associations [6] have been reported previously. Different study locations and study periods are likely to contribute to the inconclusive findings. Differential influenza types/subtypes predominate at different locations and time periods of diverse meteorological characteristics and have discrepant transmissibility. Therefore, the influence of meteorological factors on influenza transmissibility is expected to vary according to the influenza type and subtype. Further determination of the meteorological drivers of influenza transmission by type/subtype would have important implications for precise interventions against influenza. Nevertheless, only one study has reported the type/subtype-specific impact of meteorological factors on influenza transmissibility [7].
Under climate change, extreme weather events will occur more frequently in the future, and temperatures are likely to become more unstable. It has been projected that each degree of global warming will result in a 10% increase in temperature variability in the subtropical hotspots of the Northern Hemisphere in the future [9]. Exposure to temperature variability is inevitable. It is hypothesized that large temperature variability is likely to facilitate the transmission of influenza. However, only one study has investigated the impact of short-term temperature variability on influenza transmission: Zhang et al. has reported a U-shaped association between the diurnal temperature range (DTR) and influenza transmissibility [8]. DTR is an index that only accounts for the variation in extreme temperatures within a day and does not consider the inter-day variation in temperatures. Further efforts are warranted to investigate the impact of temperature variability on influenza transmissibility using an index that accounts for both intra- and inter-day variations. This includes the hourly temperature variability (HTV; the standard deviation of hourly temperatures), which has been commonly used to assess the impact of temperature variability on health outcomes, such as hospital admissions and mortality [10,11,12].
Guangzhou is the largest city in the south of China (latitude: 23°07′N; longitude 113°15′E) and has a population density of 2059 per km2 in 2019. Meanwhile, Guangzhou is a transportation hub, the risk of influenza transmission is high. In this study, we explored the effects of meteorological factors (i.e., ambient mean temperature, HTV, absolute humidity, and relative humidity) on influenza transmissibility by type/subtype in Guangzhou, China.
Methods
Data collection
Influenza surveillance data were obtained from the Guangzhou Center for Disease Control and Prevention (CDC). The week in which the first Monday of January lied was defined as the start week of a specific year. We extracted the weekly fraction of consultations for influenza-like illness (ILI: body temperature ≥ 38 °C with cough or sore throat) among outpatient visits at sentinel hospitals in Guangzhou between October 4, 2010 (the first Monday of October 2010) and January 5, 2020 (the end of the last week of 2019). In addition, virological data, that is, weekly percentages of specimens that tested positive for influenza A(H1N1)pdm09, A(H3N2), and B, were also compiled.
We obtained hourly data on temperature recorded at two meters above the land surface from the fifth generation of European Reanalysis Land (ERA5-Land) dataset at a spatial resolution of 0.1° × 0.1° (~ 9 km × 9 km) [13]. The hourly relative humidity (for 06:00, 09:00, 12:00, 15:00, and 18:00) at a height of two meters above the surface were collected from Agrometeorological ERA5 with a spatial resolution of 0.1° × 0.1° as well [14]. We averaged data points of all of the 89 grids to obtain the hour data for the subsequent analysis. And the daily mean temperature and relative humidity were obtained by averaging the hourly data. Information on holiday-related school closures, including public holidays, weekends, winter holidays, and summer holidays, were also collected. The Public Security Bureau of Guangzhou Municipality provided data on annual population size.
Calculation of influenza virus activity proxy
To determine influenza virus activity, the weekly ILI+ was calculated by multiplying the ILI consultation rate (ILI%, the proportion of patients with ILI among the outpatients) by the rate of specimens positive for influenza (lab%) [5, 7, 15]. ILI+ would be an ideal measure of the incidence of influenza infection under some conditions, e.g. (1) the proportion of ILIs that seek medical consultations is stable over time; (2) the sample from sentinel hospitals for ILI% estimation is representative of the study population; (3) the sample of viral testing for lab% estimation is representative of the medical consultations for ILI; (4) the performance of diagnosis method for influenza virus does not change over time [16].
Estimation of the daily instantaneous effective reproductive number
The weekly number of influenza infections was estimated as ILI+ multiplied by the population size and a conversion rate (γ = 1) [17]. The daily number of influenza infections was interpolated using the spline function [4]. Influenza transmissibility was measured using the instantaneous effective reproductive number (Rt), defined as the average number of secondary infections resulting from an infectious individual at time t. We estimated Rt as the number of new infections at time t (i.e. It) divided by the total infectiousness of infected individual at time t [18]:
where ws is the current infectiousness of individuals which were infected s days ago, based on the distribution of serial interval. We assumed that the serial intervals followed gamma distributions with means ± standard deviations of 3.3 ± 1.7, 3.08 ± 1.39, 3.48 ± 1.88, and 3.72 ± 1.95 for influenza, A(H1N1)pdm09, A(H3N2), and B, respectively [19]. The estimates of Rt can be highly fluctuating due to small time step of data. To address this issue, we estimated the Rt over a 7-day time window, assuming that the daily Rt did not change over this time window [8].
Assessment of the associations between meteorological factors and R t
Our preliminary analysis suggested that Rt fitted the gamma distribution better than the lognormal distribution in terms of Akaike’s Information Criteria. Therefore, a gamma regression with a log link combined with a distributed lag non-linear model was used to assess the potentially non-linear effects of meteorological factors on influenza transmissibility [20], after adjusting for inter-epidemic effects and the effects of depletion of susceptibility over time and holidays. The analysis was restricted to the data from maximum of 9 weeks either side of the peak of influenza epidemic (Additional file 1) to prevent the potential impact of the low and irregular reporting at the very start and end of each epidemic. HTV was not included in the regression model when the effect of temperature was assessed as it may mediate the effect of temperature on influenza transmissibility. Temperature and absolute humidity were commonly highly correlated; therefore, these two variables were not included in the same model when analyzing the effect of each of these variables on influenza transmissibility. Absolute humidity and relative humidity were not included in the same model. Details of the models fitted are provided in Additional file 1. Wald test was applied to assess the statistical significance of each meteorological factor.
Sensitivity analyses were conducted to assess the robustness of results by (1) setting γ = 0.5, γ = 0.05, γ = 0.005; (2) changing the mean ± standard deviation of serial interval for influenza and different influenza types/subtypes to 3.3 ± 1.7 and 2.6 ± 1.5 [21]; (3) considering data from maximum 8–10 weeks either side of each epidemic peak. All statistical analyses were performed using the R software (version 4.1.1; R Foundation for Statistical Computing).
Results
A total of 11 influenza epidemics were detected during the study period (Fig. 1). Influenza epidemics varied by influenza type/subtype. Specifically, there were seven, seven, and six influenza A(H1N1)pdm09, A(H3N2), and B epidemics, respectively, with different lengths and peaks. Influenza A(H1N1)pdm09 and A(H3N2) co-circulated in 6/200 epidemic weeks (200 epidemic weeks were considered in the regression analysis of the associations between meteorological factors and Rt), influenza A(H3N2) and B co-circulated in 14/200 epidemic weeks, and influenza A(H1N1)pdm09 and B co-circulated in 35/200 epidemic weeks. We estimated that an infected individual could cause a median of 1.007 secondary cases (Table 1 and Additional file 1). The median Rt of influenza A(H3N2) (1.049) was higher than that of influenza A(H1N1)pdm09 (1.009) and influenza B (1.004) (Table 1 and Additional file 1).

Weekly influenza infection rates in Guangzhou, China from October 2010 to December 2019. Lines indicate the influenza infection rate; colored areas, influenza epidemics used in the gamma regression analysis
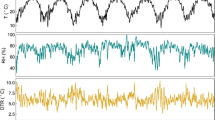
During the influenza epidemics, the mean daily temperature, HTV over 0–14 days, daily absolute humidity, and relative humidity were 20.74 °C, 3.34 °C, 14.78 g/m3, and 76.06%, respectively (Table 2 and Fig. 2). On average, temperature and absolute humidity were higher during influenza A(H3N2) epidemics than during other epidemics, whereas the mean HTV was lower during influenza A(H3N2) epidemics than during other influenza epidemics.

Time-series of daily meteorological factors in Guangzhou, China from October 4, 2010 to December 30, 2019. Lines indicate the time-series of daily meteorological factors and colored areas, influenza epidemics used in the gamma regression analysis. Abbreviation: HTV, hourly temperature variability
Figure 3 shows the exposure-response associations between meteorological factors and Rt. And Additional file 1 present the results of Wald tests of the statistical significance of each meteorological factor. It was apparent that the association between ambient temperature and Rt was non-linear, with elevated transmissibility at low and high temperatures. Influenza transmissibility increased as HTV increased when HTV < around 4.5 °C. A non-linear association was observed between absolute humidity and Rt, with increased transmissibility at low absolute humidity and at around 19 g/m3. Relative humidity had a U-shaped association with influenza transmissibility.

Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various meteorological variables. Curves and colored areas represent the point estimates of Rt ratios and the corresponding confidence intervals, respectively. The ticks along the x-axis are observed meteorological data. Horizontal lines indicating Rt ratio = 1 were also plotted. The Rt ratios are the ratio of predicted Rt with respect to reference values for the meteorological factors of mean temperature, hourly temperature variability (HTV), absolute humidity, and relative humidity set to 18.12 °C, 3.25 °C, 10.88 g/m3, and 66.99%, respectively. Reference values for the mean temperature, absolute humidity, and relative humidity corresponded to the lowest transmission risk of influenza, and the median is used as the reference value for HTV. We depicted the associations excluding the 10 lowest and the 10 largest values of meteorological factors, avoiding the potentially unrobust estimates due to small sample size
As expected, the associations between meteorological factors and influenza transmissibility varied according to the influenza type and subtype (Fig. 3 and Additional file 1). Regarding the association with ambient temperature, the Rt ratio for influenza A(H1N1)pdm09 in large decreased with temperature and the Rt ratio for influenza B declined with temperature when it was colder than around 19 °C, whereas, the lowest Rt ratio for influenza A(H3N2) was witnessed at around 21 °C, higher than which, the Rt ratio increased with temperature. As for the relationship with HTV, the Rt ratio for influenza A(H1N1)pdm09 increased with HTV when HTV < around 4.5 °C, while the lowest Rt ratio for influenza A(H3N2) was observed at 2.5 °C and the transmissibility of influenza B decreased with HTV when HTV < 3.0 °C. An initially decreasing, then increasing, and finally declining trend was observed in the associations between absolute humidity and transmissibility of influenza A(H1N1)pdm09 and influenza B. For influenza A(H3N2), the Rt ratio increased with absolute humidity.
Point estimates of Rt were robust to the change in the conversion rate, although the 95% credible intervals of Rt were wider when lower conversion rates were used to estimate the number of influenza infections (Additional file 1). Rt estimates were similar to the results of main analysis when assuming that mean ± standard deviation of serial interval was 3.3 ± 1.7 (Additional file 1). Both of mean and standard deviation of Rt estimates decreased when assuming that mean ± standard deviation of serial interval was 2.6 ± 1.5 (Additional file 1). The estimated associations of Rt with ambient temperature, HTV, absolute humidity, and relative humidity were in large robust to the conversation rate and to the mean and standard deviation of the serial interval (Additional file 1). Overall, the estimates of the associations between meteorological factors and Rt did not vary substantially when altering the maximum weeks either side of the epidemic peak, although the association between HTV and transmissibility for influenza A(H3N2) was inconclusive (Additional file 1).
Discussion
This study explored the associations between influenza transmissibility and meteorological variables by influenza type/subtype in Guangzhou, a subtropical city in China. The results showed that influenza transmissibility had a non-liner relationship with ambient temperature, HTV, absolute humidity, and relative humidity, and this relationship differed according to influenza type and subtype.
Ambient temperature and humidity play potential roles in the influenza transmission [22, 23]. We observed that influenza transmissibility increased at both low and high temperatures, consistent with a previous study in China based on the data of 30 provincial-level administrative divisions (PLADs) during 2010–2017 [7]. However, Zhang et al. reported an elevated influenza transmissibility at low temperatures but not at high temperatures in Guangzhou, China during 2005–2021 [8]. We found that relative humidity had a U-shaped association with influenza transmissibility, in accordance with a previous report [8]. In this study, the effect of absolute humidity on influenza transmissibility was relatively complicated, with a high transmission risk occurring at low absolute humidity and at approximately 19 g/m3. Zhang et al. reported a similar result in China [7], while Ali et al. identified a U-shaped association in China based on data from nine PLADs [5]. Zhang et al. found that influenza transmissibility decreased with absolute humidity in Guangzhou, China [8]. Lei et al. showed that the association was statistically non-significant in temperate and subtropical regions in China based on data from five PLADs during 2013–2019 [6]. Different study locations, study periods (with differentially predominant circulating influenza types/subtypes and epidemic intensities), and influenza incidences used to estimate Rt (reported number of symptomatic influenza cases or the one estimated based on ILI+) may have contributed to the differential findings on the associations between meteorological variables and influenza transmissibility (Additional file 1).
To the best of our knowledge, this is the first study to reveal the association between HTV and influenza transmissibility. We found that the HTV was positively associated with Rt ratio for influenza when HTV < around 4.5 °C. Similarly, previous studies reported a positive association between DTR and influenza incidence [24] and respiratory infections [25, 26]. Zhang et al. showed a U-shaped curve for the association between DTR and influenza transmissibility [8]. DTR only reflects intra-day variations based on extreme temperatures, whereas HTV reflects both intra- and inter-day variations, not merely based on extreme temperatures. Thus, it is possible that the association between HTV and influenza transmissibility was different from that between DTR and influenza transmissibility, in addition to the reasons mentioned above for the different findings regarding the associations of Rt with ambient temperature and humidity.
The potential impact of meteorological factors on influenza transmissibility can be explained by (1) virus stability and shedding, (2) adaptive immune responses, and (3) changes in human behavior (e.g., spending more time indoors) in response to meteorological factors. Several plausible reasons have been proposed for the high transmissibility at low and high temperatures. First, cold air weakens the nasal mucociliary clearance, facilitates the ordering of lipids on the viral membrane, and strengthens viral stability and viral shedding, thus reinforcing viral amplification and transmission [27, 28]. Second, adaptive immune responses are hindered at low and high temperatures [29, 30], making people more susceptible to influenza infection. Third, people tend to spend more time indoor at low and high temperatures (cooling with air conditioner), leading to more human-to-human contact and increased transmissibility [31]. Regarding the mechanisms of the association between absolute humidity and influenza transmissibility, at low humidity, there could be serious impairments in mucociliary clearance and airway tissue repair mechanisms. Further, global type I interferon-stimulated gene expression could be inhibited following intranasal influenza virus infection [32]. Increased absolute humidity in summer may also result in elevated influenza transmissibility through human behavioral changes. Large temperature variations often occur with sudden changes in temperature. Our findings regarding the positive association between HTV and influenza transmissibility when HTV < around 4.5 °C can be explained by the following possible mechanisms. First, sudden temperature changes cause a more significant inflammatory nasal response, resulting in decreased ability of the nasal cavity to clear the respiratory virus [33]. Second, large temperature variations can affect humoral and cellular immunity [34]. A previous study related sudden temperature changes with an increase in the release of inflammatory mediators associated with mast cells [35]. Increased HTV may have led to a decline in immunity to influenza and influenza transmissibility. Influenza is often transmitted indoors, and there are discrepancies between indoor and outdoor environmental factors such as temperature and humidity [6]. Therefore, indoor-outdoor differences should be considered when interpreting the effects of meteorological factors on influenza transmissibility.
Interestingly, we observed subtype-dependence effects of meteorological factors on influenza transmissibility: high ambient temperatures were associated with elevated transmissibility for influenza A(H3N2), but not for influenza A(H1N1)pdm09; when absolute humidity was larger than around 19 g/m3, absolute humidity was still positively associated with transmissibility for influenza A(H3N2), but not for other influenza type/subtype (Fig. 3). The differences in the effects of meteorological factors on influenza transmissibility across influenza types/subtypes may be attributed to disparities in viral properties and efficiency in response to environmental factors [36,37,38]. Viral inactivation depends on the thermal denaturation of proteins and nucleic acids [39]. The environment may influence the stability of influenza viruses by inducing conformational changes in surface glycoproteins or increasing the ordering of lipids in the viral envelope [28, 40]. Disparities in envelope proteins may be responsible for the differential environmental dependence among influenza types/subtypes [7]. An experimental study also reported strain-dependent variations in the longevity of influenza A(H1N1)pdm09, A(H3N2), and B lineages in droplets [37]. In addition, different influenza types/subtypes predominated in distinct time periods and influenza activity of a specific type/subtype was low in some meteorological conditions, probably resulting in insufficient sample size for the inference of the association between a specific meteorological factor and Rt in these conditions. Further studies are warranted to reveal the mechanisms underlying the different effects of meteorological factors on influenza transmissibility according to influenza type and subtype.
This study has some limitations. First, we did not have data on “true” influenza incidence because a certain proportion of influenza infections did not seek hospital consultation. Therefore, the number of influenza cases reported in surveillance systems is an underestimate of influenza infection. Here, we estimated influenza incidence based on ILI+, as previous studies have suggested that ILI+ may be a better proxy than ILI and virological data for assessing influenza virus activity [16, 41]. We did not consider the delays from infection to case report when inferring the influenza incidence. Further studies are warranted to deal with this issue with an appropriate approach which is robust even when the distribution of the delay from infection to case report is uncertain. Second, we did not examine the associations between meteorological factors and influenza transmissibility by different age groups because the surveillance was designed to delineate the pattern for the whole population and not for different age groups. Third, we focused only on the impact of meteorological factors on influenza transmissibility in a subtropical city. Such efforts would provide invaluable data on the mechanisms of influenza seasonality in subtropical cities, which are not fully understood. More efforts are needed to reveal the mechanisms of influenza seasonality using data from more cities across different climatic zones.
Conclusions
Temperature variability has an impact on influenza transmissibility. Ambient temperature, temperature variability, and humidity influence the transmissibility of different influenza types/subtypes discrepantly. Our findings have important implications for improving preparedness for influenza epidemics, especially under climate change conditions.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Abbreviations
- CDC:
-
Guangzhou Center for Disease Control and Prevention
- DTR:
-
Diurnal temperature range
- ERA5-Land:
-
The fifth generation of European Reanalysis Land
- HTV:
-
Hourly temperature variability
- ILI:
-
Influenza-like illness
- PLADs:
-
Provincial-level administrative divisions
- R t :
-
Effective reproductive number
References
World Health Organization. Influenza (Seasonal). Geneva: World Health Organization. 2023. https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal). Accessed 20 Aug 2023 .
Tamerius J, Nelson MI, Zhou SZ, Viboud C, Miller MA, Alonso WJ. Global influenza seasonality: reconciling patterns across temperate and tropical regions. Environ Health Perspect. 2011;119(4):439–45.
Newman LP, Bhat N, Fleming JA, Neuzil KM. Global influenza seasonality to inform country-level vaccine programs: an analysis of WHO FluNet influenza surveillance data between 2011 and 2016. PLoS One. 2018;13(2):e0193263.
Ali ST, Cowling BJ, Lau EHY, Fang VJ, Leung GM. Mitigation of influenza B epidemic with school closures, Hong Kong, 2018. Emerg Infect Dis. 2018;24(11):2071–3.
Ali ST, Cowling BJ, Wong JY, Chen D, Shan S, Lau EHY, et al. Influenza seasonality and its environmental driving factors in mainland China and Hong Kong. Sci Total Environ. 2022;818:151724.
Lei H, Yang M, Dong Z, Hu K, Chen T, Yang L, et al. Indoor relative humidity shapes influenza seasonality in temperate and subtropical climates in China. Int J Infect Dis. 2023;126:54–63.
Zhang B, Chen T, Liang S, Shen W, Sun Q, Wang D, Wang G, et al. Subtypes specified environmental dependence of seasonal influenza virus. Sci Total Environ. 2022;852:158525.
Zhang R, Lai KY, Liu W, Liu Y, Cai W, Webster C, et al. Association of climatic variables with risk of transmission of influenza in Guangzhou, China, 2005–2021. Int J Hyg Environ Health. 2023;252:114217.
Bathiany S, Dakos V, Scheffer M, Lenton TM. Climate models predict increasing temperature variability in poor countries. Sci Adv. 2018;4(5):eaar5809.
Guo Y, Gasparrini A, Armstrong BG, Tawatsupa B, Tobias A, Lavigne E, et al. Temperature variability and mortality: a multi-country study. Environ Health Perspect. 2016;124(10):1554–9.
Yang Z, Yang J, Zhou M, Yin P, Chen Z, Zhao Q, et al. Hourly temperature variability and mortality in 31 major Chinese cities: effect modification by individual characteristics, season and temperature zone. Environ Int. 2021;156:106746.
Zhan ZY, Tian Q, Chen TT, Ye Y, Lin Q, Han D, et al. Temperature variability and hospital admissions for chronic obstructive pulmonary disease: analysis of attributable disease burden and vulnerable subpopulation. Int J Chron Obstruct Pulmon Dis. 2020;15:2225–35.
Muñoz SJ. ERA5-Land hourly data from 1950 to present. Copernicus Climate Change Service (C3S) Climate Data Store (CDS); 2019. https://doi.org/10.24381/cds.e2161bac.
Boogaard H, Schubert J, De Wit A, Lazebnik J, Hutjes R, Van der Grijn G, et al. Agrometeorological indicators from 1979 to present derived from reanalysis. Copernicus Climate Change Service (C3S) Climate Data Store (CDS); 2020. https://doi.org/10.24381/cds.6c68c9bb.
Hansen CL, Chaves SS, Demont C, Viboud C. Mortality associated with influenza and respiratory syncytial virus in the US, 1999-2018. JAMA Netw Open. 2022;5(2):e220527.
Goldstein E, Cobey S, Takahashi S, Miller JC, Lipsitch M. Predicting the epidemic sizes of influenza a/H1N1, a/H3N2, and B: a statistical method. PLoS Med. 2011;8(7):e1001051.
Yang W, Lau EHY, Cowling BJ. Dynamic interactions of influenza viruses in Hong Kong during 1998-2018. PLoS Comput Biol. 2020;16(6):e1007989.
Cori A, Ferguson NM, Fraser C, Cauchemez S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am J Epidemiol. 2013;178(9):1505–12.
Levy JW, Cowling BJ, Simmerman JM, Olsen SJ, Fang VJ, Suntarattiwong P, et al. The serial intervals of seasonal and pandemic influenza viruses in households in Bangkok. Thailand Am J Epidemiol. 2013;177(12):1443–51.
Johnson KD, Beiglböck M, Eder M, Grass A, Hermisson J, Pammer G, et al. Disease momentum: estimating the reproduction number in the presence of superspreading. Infect Dis Model. 2021;6:706–28.
Cauchemez S, Donnelly CA, Reed C, Ghani AC, Fraser C, Kent CK, et al. Household transmission of 2009 pandemic influenza a (H1N1) virus in the United States. N Engl J Med. 2009;361(27):2619–27.
Shaman J, Kohn M. Absolute humidity modulates influenza survival, transmission, and seasonality. Proc Natl Acad Sci U S A. 2009;106(9):3243–8.
Lowen CA, Steel J. Roles of humidity and temperature in shaping influenza seasonality. J Virol. 2014;88(14):7692–5.
Lao J, Liu Z, Liu Y, Zhang J, Jiang B. Influence of diurnal temperature range on influenza incidence in the elderly. Zhonghua Liu Xing Bing Xue Za Zhi. 2018;39(11):1454–8.
Ge WZ, Xu F, Zhao ZH, Zhao JZ, Kan HD. Association between diurnal temperature range and respiratory tract infections. Biomed Environ Sci. 2013;26(3):222–5.
Onozuka D. The influence of diurnal temperature range on the incidence of respiratory syncytial virus in Japan. Epidemiol Infect. 2014;143(4):813–20.
Eccles R. An explanation for the seasonality of acute upper respiratory tract viral infections. Acta Otolaryngol. 2002;122(2):183–91.
Polozov IV, Bezrukov L, Gawrisch K, Zimmerberg J. Progressive ordering with decreasing temperature of the phospholipids of influenza virus. Nat Chem Biol. 2008;4(4):248–55.
Abram QH, Dixon B, Katzenback BA. Impacts of low temperature on the teleost immune system. Biology (Basel). 2017;6(4):39.
Moriyama M, Ichinohe T. High ambient temperature dampens adaptive immune responses to influenza a virus infection. Proc Natl Acad Sci. 2019;116(8):3118–25.
Lofgren E, Fefferman NH, Naumov YN, Gorski J, Naumova EN. Influenza seasonality: underlying causes and modeling theories. J Virol. 2007;81(11):5429–36.
Kudo E, Song E, Yockey LJ, Rakib T, Wong PW, Homer RJ, et al. Low ambient humidity impairs barrier function and innate resistance against influenza infection. Proc Natl Acad Sci. 2019;116(22):10905–10.
Graudenz GS, Landgraf RG, Jancar S, Tribess A, Fonseca SG, Faé KC, et al. The role of allergic rhinitis in nasal responses to sudden temperature changes. J Allergy Clin Immunol. 2006;118(5):1126–32.
Bull GM. The weather and deaths from pneumonia. Lancet. 1980;1(8183):1405–8.
Togias AG, Naclerio RM, Proud D, Fish JE, Adkinson NFJ, Kagey-Sobotka A, et al. Nasal challenge with cold, dry air results in release of inflammatory mediators. Possible mast cell involvement. J Clin Invest. 1985;76(4):1375–81.
Jin H, Lu B, Zhou H, Ma C, Zhao J, Yang C-f, et al. Multiple amino acid residues confer temperature sensitivity to human influenza virus vaccine strains (flumist) derived from cold-adapted a/Ann Arbor/6/60. Virology. 2003;306(1):18–24.
Kormuth KA, Lin K, Qian Z, Myerburg MM, Marr LC, Lakdawala SS. Environmental persistence of influenza viruses is dependent upon virus type and host origin. mSphere. 2019;4(4):e00552–e00519.
Medcalf L, Poole E, Elton D, Digard P. Temperature-sensitive lesions in two influenza a viruses defective for replicative transcription disrupt RNA binding by the nucleoprotein. J Virol. 1999;73(9):7349–7256.
Woese C. Thermal inactivation of animal viruses. Ann N Y Acad Sci. 1960;83:741–51.
Marr LC, Tang JW, Mullekom JV, Lakdawala SS. Mechanistic insights into the effect of humidity on airborne influenza virus survival, transmission and incidence. J R Soc Interface. 2019;16(150):20180298.
Wong JY, Wu P, Nishiura H, Goldstein E, Lau EHY, Yang L, et al. Infection fatality risk of the pandemic a(H1N1)2009 virus in Hong Kong. Am J Epidemiol. 2013;177(8):834–40.
Acknowledgements
We thank staff members of Guangzhou CDC and Pan-Pan Zhu for administrative work and data collection.
Funding
This work was supported by National Nature Science Foundation of China [82003555] and Science and Technology Plan Project of Guangzhou [SL2023A04J02137].
Author information
Authors and Affiliations
Contributions
Ze-Lin Yan: writing-original draft, formal analysis, software; Wen-Hui Liu: writing-original draft, data curation; Yu-Xiang Long: writing-review, formal analysis, editing; Bo-Wen Ming: writing-review & editing; Zhou Yang: writing-review & editing; Peng-Zhe Qin: conceptualization, resources, supervision; Chun-Quan Ou: conceptualization, methodology, supervision; Li Li: conceptualization, methodology, funding acquisition. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee of Southern Medical University (NFYKDX-ER2022012). The need for informed consent was waived because the data were deidentified and aggregated.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Definition of influenza epidemics. Models. Fig. S1. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza epidemic used in the gamma regression analysis. Fig. S2. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H1N1)pdm09 epidemic used in the gamma regression analysis. Fig. S3. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H3N2) epidemic used in the gamma regression analysis. Fig. S4. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza B epidemic used in the gamma regression analysis. Table S1. Results of Wald tests of the statistical significance of each meteorological factor. Table S2. Summary statistics of the estimates of daily instantaneous effective reproductive number when using different conversion rates to calculate influenza incidence. Fig. S5. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza epidemic when setting the conversion rate to 0.5. Fig. S6. Estimates of daily instantaneous effective reproductive reproduction number (Rt) for each influenza A(H1N1)pdm09 epidemic when setting the conversion rate to 0.5. Fig. S7. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H3N2) epidemic when setting the conversion rate to 0.5. Fig. S8. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza B epidemic when setting the conversion rate to 0.5. Fig. S9. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza epidemic when setting the conversion rate to 0.05. Fig. S10. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H1N1)pdm09 epidemic when setting the conversion rate to 0.05. Fig. S11. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H3N2) epidemic when setting the conversion rate to 0.05. Fig. S12. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza B epidemic when setting the conversion rate to 0.05. Fig. S13. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza epidemic when setting the conversion rate to 0.005. Fig. S14. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H1N1)pdm09 epidemic when setting the conversion rate to 0.005. Fig. S15. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H3N2) epidemic when setting the conversion rate to 0.005. Fig. S16. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza B epidemic when setting the conversion rate to 0.005. Table S3. Summary statistics of the estimates of daily instantaneous effective reproductive number when assuming different means and standard deviations of the serial interval. Fig. S17. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H1N1)pdm09 epidemic when assuming the mean and standard deviation of serial interval were 3.3 and 1.7, respectively. Fig. S18. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H3N2) epidemic when assuming the mean and standard deviation of serial interval were 3.3 and 1.7, respectively. Fig. S19. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza B epidemic when assuming the mean and standard deviation of serial interval were 3.3 and 1.7, respectively. Fig. S20. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza epidemic when assuming the mean and standard deviation of serial interval were 2.6 and 1.5, respectively. Fig. S21. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H1N1)pdm09 epidemic when assuming the mean and standard deviation of serial interval were 2.6 and 1.5, respectively. Fig. S22. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza A(H3N2) epidemic when assuming the mean and standard deviation of serial interval were 2.6 and 1.5, respectively. Fig. S23. Estimates of daily instantaneous effective reproductive number (Rt) for each influenza B epidemic when assuming the mean and standard deviation of serial interval were 2.6 and 1.5, respectively. Fig. S24. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when setting the conversion rate to 0.5. Fig. S25. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when setting the conversion rate to 0.05. Fig. S26. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when setting the conversion rate to 0.005. Fig. S27. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when setting the mean and standard deviation of serial interval for influenza to 3.3 and 1.7, respectively. Fig. S28. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when setting the mean and standard deviation of serial interval for influenza to 2.6 and 1.5, respectively. Fig. S29. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when considering data from maximum 8 weeks either side of each epidemic peak. Fig. S30. Exposure-response curves of the associations of daily instantaneous effective reproductive number (Rt) with various climatic variables when considering data from maximum 10 weeks either side of each epidemic peak. Table S4. Comparisons of studies which assessed the association between meteorological factors and influenza transmissibility.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, ZL., Liu, WH., Long, YX. et al. Effects of meteorological factors on influenza transmissibility by virus type/subtype. BMC Public Health 24, 494 (2024). https://doi.org/10.1186/s12889-024-17961-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17961-9