
Abstract
Background
Despite being easily corrected with eyeglasses, over two-thirds of the world’s child population presents with vision impairment (VI) due to uncorrected refractive errors. While systematic reviews have shown that VI can significantly impact children’s depression and anxiety, none have reviewed the existing literature on the association between spectacle correction and well-being. This review aims to address this knowledge gap.
Main outcome measures
The main outcome measures were i) cognitive and education well-being which included mathematics and english literacy, reading fluency, school function, academic performance and grades; ii) psychological and mental health well-being which included physical anxiety, learning anxiety and mental health test scores and iii) quality of life.
Methods
We searched eight databases for articles published between 1999 to 2021 that assessed the associations between spectacle correction and children’s (0 to 18 years) well-being. There were no restrictions on language or geographic location. Two reviewers independently screened all publications using validated quality checklists. The findings of the review were analysed using narrative synthesis. [PROSPERO CRD42020196847].
Results
Of 692 records found in the databases, six randomised control trials, one cohort, one cross-sectional and one qualitative study (N = 9, 1.3%) were eligible for analysis. Data were collected from 25 522 children, 20 parents and 25 teachers across the nine studies. Seven were rated as good quality (67 to 100% of quality criteria fulfilled), and two were satisfactory (33 to 66% of quality criteria fulfilled). Spectacle correction was found to improve children’s educational well-being (n = 4 very strong evidence; n = 2 strong evidence), quality of life (n = 1, very strong evidence) and decrease anxiety and increase mental health scores (n = 1, strong evidence).
Conclusion
Evidence suggests that spectacle correction improves children’s cognitive and educational well-being, psychological well-being, mental health, and quality of life. More research is needed, given the paucity of published literature and the focus on only three aspects of well-being.
Similar content being viewed by others
Background
It has been estimated that 19 million children have vision impairment, with uncorrected refractive error (URE) affecting 12 million children [1], making it the leading cause of childhood vision impairment worldwide [2]. Although spectacles can effectively correct refractive errors, less than one-third of children who need spectacles in low-resource settings have them [3]. Studies have found that vision impairment and ocular morbidities have increased anxiety [4], reading difficulties [5,6,7], anti-social behaviour [8], quality of life issues [9] and problems with self-esteem [10].
A meta-analysis by Mavi et al. found that children with uncorrected hyperopia had lower education performance (Standardised Mean Difference [SMD] − 0.18, 95%CI − 0.27 to − 0.09) and reading skills (SMD − 0.46, 95% CI, − 0.90 to − 0.03) compared to emmetropic children [11]. Another systematic review by Li and Chan et al. found that vision-impaired children have higher depression (SMD 0.57, 95%CI 0.26–0.89) and anxiety scores (SMD 0.61, 95% CI 0.40–0.82) than normally sighted children. The same systematic review also observed myopic children having higher depression scores than normally sighted children (SMD 0.59, 95% CI 0.36–0.81) [12]. Uncorrected myopia is also shown to impact children’s mental health negatively [13]. Furthermore, many of these studies were cross-sectional [7,8,9,10, 13,14,15,16] and could not demonstrate the causal relationship between VI due to URE and aspects of well-being due to the inherent limitations of the study design.
Studies on the impact of spectacle correction on children’s well-being are rare, with most focusing on the impact on academic performance [11, 17,18,19,20]. However, child well-being is a multi-dimensional construct that explores various domains of a child’s life, including health, education, living conditions, material well-being, and interpersonal relations [21]. The scarcity of conclusive evidence makes promoting healthy well-being in children by correcting their refractive error challenging despite having a long-term impact on their later years and into adulthood, affecting their ability to actively participate in society, their communities, and their families [22].
No systematic review of the impact of spectacle correction on the broader aspects of children’s well-being has been published or registered to date. Considering the increasing evidence on the detrimental effects of vision impairment due to URE on children, we conducted a review to systematically synthesise the findings from the existing literature on the impact of spectacle correction on various aspects of children’s well-being.
Methods
This systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO Registration number: CRD42020196847). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Systematic Review Protocols (PRISMA-P) guidelines were used to develop and report the systematic review protocol [23].
The search strategy was adapted to each electronic database, including MEDLINE, PubMed, Embase, SCOPUS, ProQuest, Weipu Database (VIP), Chinese National Knowledge Infrastructure (CNKI) and Wanfang databases using the search terms in Supplementary file 1. The inclusion criteria were as follows: studies of any language from any geographic locations, published between 1999 and 2021, qualitative, observational or interventional studies; participants were children 18 years and younger diagnosed with vision impairment due to uncorrected refractive error, without any ocular comorbidities. No grey literature was included in the review. The intervention of interest was spectacle correction. The primary outcome was well-being according to the Organisation of Economic and Co-operative Development’s [24] Measuring What Matters for Child Well-being and Policies, which includes social health, physical health, cognitive and education and material health, in addition to physiological and mental health and quality of life.
Two reviewers (PGP and ACY) independently screened all titles and abstracts against eligibility criteria. If an article’s eligibility could not be determined based on its title and abstract, its full text was retrieved and screened by the two same reviewers. A third senior reviewer (VFC) was consulted in cases of disagreement between the two reviewers. Data were then extracted into a pre-designed Microsoft Excel Spreadsheet, capturing information on the publication date, author(s), title, geographic location, study setting, study design, sample size, sampling method, outcome measure, and key findings, limitations, strengths and recommendations. Two data extractors (PGP and ACY) checked for data errors and consistencies.
Two reviewers (PGP and ACY) independently appraised the quality of each randomised control trial (RCT) and qualitative study using the Critical Appraisal Skills Programme checklists (CASP) [25]. In contrast, cohort and cross-sectional studies were appraised using the Joanna Briggs Institute’s Critical Appraisal-Checklists (JBI) [26]. Discrepancies were resolved through discussion and consensus. A third senior reviewer (VFC) was consulted in cases of disagreement between the two reviewers.
Due to the high heterogeneity nature of the studies, we performed narrative synthesis on the findings to report the wide range of study design, characteristics, and well-being outcomes. The quality of the studies was reported as per the criteria of the appraisal tools. The quality of the study evidence was rated as Good (fulfilled 67 to 100% of criteria), Satisfactory (fulfilled 33 to 66% of criteria) or Poor (fulfilled 0 to 33% of criteria) [27].
Results
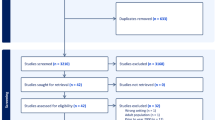
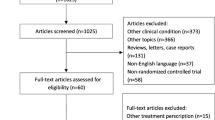
The electronic database search yielded 692 studies. After removing 174 duplicates and 416 studies due to irrelevant titles, 102 studies were included for abstract screening. Seventy-five studies were excluded. Of the 39 studies that underwent full-text screening, 30 (76.9%) were excluded because i) they did not demonstrate the impact of spectacle correction directly or as a comparison to before the spectacle correction was used (n = 17; 43.6%) [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44], ii) they did not measure the impact of spectacles on children’s well-being (n = 9; 23.1%) [45,46,47,48,49,50,51,52,53], iii) the population’s age was older than 18 years-old (n = 3; 7.7%) [54,55,56] and iv) it was not a published study (n = 1; 2.6%) [57]. Nine full-text studies were eligible for data extraction and appraisal [17, 18, 20, 58,59,60,61,62,63]. The study selection processes are outlined in the PRISMA flow depicted in Fig. 1.

Flow chart of results of the search strategy and study selection processes
Characteristics of the eligible studies
The eligible studies included six randomised control trials [20, 58, 59, 61,62,63], one cohort study [18], one cross-sectional study [60] and one qualitative study [60] published between 2012 and 2020. Five were conducted in China [20, 58, 59, 61, 63], three in the United States of America (19–21) and one in the Netherlands [62] (Table 1). Data was gathered from 25 522 children, 20 parents and 25 teachers across the nine reviewed studies.
Seven studies investigated children’s cognitive and educational well-being, where four were RCTs [20, 59, 61, 62], one cohort [18], one cross-sectional [60] and one qualitative study [17]. The remaining two studies in this review explored the impact of spectacle correction on children’s psychological and mental health well-being [58] and children’s quality of life [63]. Randomisation was adopted in six of the nine studies either by township or cluster [3, 20, 59], by study participants [62, 63] or schools [58]. Two studies used purposive sampling [18, 60], and one study used convenience sampling [17].
The studies investigating the impact of spectacle correction on cognitive and educational well-being used a range of indicators, with Ma et al. [61] using only math scores; Hannum and Zhang [59] using math scores, literacy and language achievement tests; Dudovitz et al. [18] using achievement marks in math, English language arts, work habits and behaviour; Nie et al.[20] using math scores, aspirations for further schooling and school dropout rate; the studies by van Rijn et al. [62] and Harvey et al. [60] used reading speed of words and nonwords and oral reading fluency respectively. The RCT by Guan et al. [58] was the only study that explored the impact of myopic spectacle correction on children’s mental health using the validated Mental Health Test (MHT) score and its subscales of learning and physical anxiety scores. Zhou et al. [63] investigated quality of life using the validated National Eye Institute Refractive Error Quality of Life-42 (NEI-RQL-42) questionnaire. The qualitative study by Dudovitz et al. [17] used focus group interviews to explore parent, teachers and student perspectives on how spectacle correction improves child well-being and school function.
The impact of spectacle correction on children’s cognitive and educational well-being
Trials by Ma et al. [61], Nie et al. [20], and Hannum and Zhang [59] that assessed math scores as an outcome found improvement by 0.25 standard deviations (SD) (satisfactory quality evidence), 0.14 SD (good quality evidence) and 0.26 SD (good quality evidence) in math scores post spectacle correction. Dudovitz et al. [18] found that after the provision of spectacle correction, students who performed in the bottom tercile for math rank at baseline achieved a significant immediate and sustained improvement of 10 to 24 percentile points (p < 0.001) (good quality evidence).
In addition to math scores, Hannum and Zhang’s [59] trial also found an average treatment effect of 0.34 SD on literacy assessment (good quality evidence) and a 44% reduction in the chances of failing a class (p < 0.01). Dudovits et al. [17] found 4.5 percentile points improvement (p = 0.02) for English Language Arts (good quality evidence) post-correction. Harvey et al. [60] also found a mean significant improvement in oral reading frequency of 6.05 words per minute (p = 0.001) among moderate astigmats and an improvement of 1.87 words per minute (p = 0.193) with spectacle correction (good quality evidence).
The qualitative study by Dudovitz et al. [17] found that providing corrective lenses to children improved their school function (good quality evidence), including behaviour or focus, willingness to practise academic skills, and improved academic performance. Participants reported improved reading ability due to a greater willingness to practice academic skills, more accuracy with math-related homework, effort and task persistence, improved concentration and focus in the classroom, less disruptive behaviour in the classroom, and more engagement and ability to participate in class (good quality evidence). A minor theme noted in this study was the ease with which homework was executed after receiving glasses.
The psychological and mental health impact of spectacle correction
Guan et al. [58] found a significant decline (0.08 SD; p < 0.10) in physical anxiety among children post myopic correction (good quality evidence). There was no significant impact on learning anxiety or overall mental health (good quality evidence). The study also found spectacle correction significantly improved the MHT score (0.26 SD; p < 0.05) in students studying at a high intensity (more than two hours a day), but those who studied at a moderate degree of intensity (between half an hour to two hours a day) experienced a decline in MHT score (0.13SD; p = 0.03) (good quality evidence). Students studying at a low-intensity level (studying for less than half an hour per day) experienced an increase in Learning Anxiety (0.17SD; p < 0.05) (good quality evidence). Albeit insignificant, children also experienced a decline in learning anxiety (0.25 SD, p < 0.10); a decrease in physical anxiety (0.22 SD; p < 0.10) post-correction (good quality evidence).
Quality of life impact of spectacle correction
Zhou et al. [63] found that irrespective of the method of refraction used to determine the spectacle correction, all methods showed a significant increase in quality-of-life scores with spectacle correction ranging from 2.32 [95% CI (0.37, 4.27) p = 0.020] in the group tested by an optometrist to 4.65 [95% CI (2.45, 6.86) p < 0.001] in the group receiving ready-made spectacles (good quality evidence).
Tables 1, 2 and 3 show that irrespective of the aspect of well-being investigated, spectacle correction had a positive impact, improving well-being. However, the effect of confounding factors on the study results was unclear in most cases In four out of nine studies, the type of refractive error being corrected was not specified [17, 18, 59, 61], three studies used myopic correction, [20, 58, 63] one used hyperopic correction [62], and one study used astigmatic correction [60].
Quality appraisal of studies
The results of the quality appraisal are summarised in Table 4. Seven of the nine studies (77.8%) were rated as good quality, and two (22.2%) were satisfactory [27]. All studies in the review addressed a focused issue. Among the RCTs, randomisation of the groups to either the intervention or control groups was done at the cluster or school levels to ensure that participants were blind to the interventions. However, this made blinding of investigators in these clusters or schools difficult as they could easily see which groups were provided with the interventions. Almost all RCTs (n = 4, 67.6%) did not accurately report the data; only one (16.67%) could not generalise findings beyond the study areas. In the cohort study by Dudovitz et al. [18] it was unclear if the exposure and outcomes were measured in a valid or reliable way and if the loss to follow-up was explored. It was also unclear if confounding factors were identified in the cross-sectional study to assess the impact of spectacle correction on reading fluency [60].
Discussion
This systematic review summarised the literature narratively on the impact of spectacle correction on well-being in children with VI due to uncorrected refractive error. All the eight eligible studies were of good or satisfactory quality. The limited evidence suggests that spectacle correction improves children’s cognitive and education, psychological and mental health well-being and quality of life.
Even though well-being is multi-dimensional and comprises a range of aspects, [64] the review found seven studies that focused strongly on cognitive and educational well-being, with limited studies (n = 1) on psychological and mental health and quality of life (n = 1). School is a significant part of a child’s life [65], and many learning activities are visually based [66], including reading, digital media and observation, thereby creating a dependency on optimal visual function [67]. Therefore, combining the fact that academic performance is a key predictor of lifelong health [68], and the availability of standardised testing could also lead to the focus on educational impact.
Overall, there was good quality [18, 20, 59, 60, 63] and satisfactory quality evidence [17, 61, 62] that spectacle correction can improve cognitive and educational well-being. Nie et al. [20], Ma et al. [61], and Hannum and Zhang’s [59] trials and, Dudovits et al.’ s [18] cohort study, has sufficient power to strongly suggest that spectacle correction can improve mathematic scores. Most of these studies were conducted in China and may limit the ability to apply their findings to other contexts. However, seeing almost half of the children in the world with VI due to URE live in Asia [69], with almost 80% of myopic adolescents living in East Asia having distance vision impairment, these findings are critically relevant in this geographic location. The scarcity of evidence outside of China also highlighted the opportunities for further research in other parts of the world.
Furthermore, despite Ma et al.’ s [61] argument that change in mathematics scores is a more valid and sensitive outcome for spectacle correction, other studies also suggest improvement in literacy, English, and reading tests. Wang et al. [70] suggested that poor academic performance in subjects such as math and English could be attributed to reduced capacity for children to perform optimally on visually demanding tasks in a modern classroom. The quantitative findings were also supported by the focus group findings from Dudovits et al.’ s [17] qualitative research that explained the perceived causal pathway of improving school function. Qualitative research on this topic is rare, but it allows a deeper understanding of experiences, phenomena, and context and explains the quantitative findings to understand human experience.
Children were at a higher risk of developing poor vision by spending more time on learning [70], and increased near work due to academic pressures has also been implicated in the increase in refractive error, particularly myopia [71]. Hence, it is not surprising that while our review shows that the positive impact of spectacle correction on psychological and mental health well-being was found among Chinese children, the greatest effect was found among children who studied for longer periods in the day [58]. We hypothesise that poorer vision prior to correction is likely to yield a greater perceived impact of the correction on the visually demanding tasks associated with the academic environment.
Numerous studies investigate the impact of uncorrected refractive error and vision impairment on aspects of quality of life in children, finding the decreased quality of life in individuals with vision impairment or uncorrected refractive error [9, 72,73,74,75]. Furthermore, numerous tools quantitatively assess the refractive error-related quality of life [76]. However, there is a paucity of studies investigating the impact of spectacle correction on the quality of life in children. The study by Zhou et al. [63] provides good evidence that quality-of-life scores increase with spectacle correction. The strength of this study is noted in the use of a self-reported measure of the quality of life (NEI-RQL-42) recommended over parental proxy reporting [77]. However, Kaphle emphasised that refractive correction may not address all quality of life issues related to URE.
While spectacle correction provides a convenient and, in many cases, cost-effective method of refractive correction, it is met with poor compliance, in many cases attributed to stigma and misconceptions [27]. Our review can be used to allay these misconceptions and educate spectacles users ahead of time as it clearly shows the positive impact of spectacle correction on academic performance, mental health and quality of life.
The limitations of this review must be acknowledged. One, the restriction to only published studies which have excluded unpublished reports, such as grey literature and programme evaluations, often provide a wealth of information that published studies do not capture [78]. These evaluation reports usually focus on the implementation effectiveness and provide a wealth of information on effective spectacle provision implementation strategies but often, lack methodological rigour to capture the impact of spectacle correction on children’s well-being. Future research could strive to incorporate these valuable sources of information without compromising on rigor by using an effectiveness-implementation hybrid designs in the programme evaluation. Two, due to the mutlifaceted factors contributing to uncorrected refractive error which could significantly impact the outcomes of spectacle correction, it reduces the generalizability of the results. These factors may include physical factors (inadequate access to routine eye examinations or a lack of trained eye care professionals, especially in rural or underserved areas, leading to a lack of diagnosis) and geographical, socioeconomic, and cultural factors (geographical constraints, and lack of awareness about the importance of spectacle correction can impede access to corrective measures). Consequently, future research should aim to capture these varied contexts and factors to allow comprehensive understanding of the impacts of spectacle correction, ensuring that the benefits observed can be appropriately generalised and applied to various settings and populations. Three, we also did not conduct a meta-analysis in this review due to the great variation in study methodologies and outcomes.
Conclusion
This review found that the limited studies touched the surface of the complex well-being construct regarding the impact of spectacle correction on children. The findings suggest that children have improved cognitive and educational well-being, psychological and mental health well-being and quality of life. More research is needed in different geographical locations to explore the impact of spectacle correction on the wider array of well-being constructs.
Availability of data and materials
The study protocol can be accessed on PROSPERO (42,020,196,847). Additional data not presented in the manuscript can be obtained from the authors by reasonable request.
Abbreviations
- CI:
-
Confidence interval
- RCT:
-
Randomised control trial
- VI:
-
Vision impairment
- URE:
-
Uncorrected refractive error
- SMD:
-
Standaridised mean difference
References
Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–8.
Flaxman SR, Bourne RRA, Resnikoff S, Ackland P, Braithwaite T, Cicinelli MV, Das A, Jonas JB, Keeffe J, Kempen JH, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–34.
Ma X, Zhou Z, Yi H, Pang X, Shi Y, Chen Q, Meltzer ME, le Cessie S, He M, Rozelle S, et al. Effect of providing free glasses on children’s educational outcomes in China: cluster randomized controlled trial. BMJ. 2014;349: g5740.
Lazarczyk J, Urban B, Konarzewska B, Al E. The differences in level of trait anxiety among girls and boys aged 13–17 years with myopia and emmetropia. BMC Ophthalmol. 2016;16:201.
Rosner J, Rosner J. The relationship between moderate hyperopia and academic achievement: how much plus is enough? J Am Optom Assoc. 1997;68(10):648–50.
Williams W, Latif A, Hannington L, Watkins D. Hyperopia and educational attainment in a primary school cohort. Arch Dis Child. 2005;90(2):150–3.
Dusek W, Pierscionek B, Mcclelland J. A survey of visual function in an Austrian population of school-age children with reading and writing difficulties. BMC Ophthalmol. 2010;10:16.
Johnson R, Zaba J. The visual screening of adjudicated adolescents. Journal of Behavioural Optometry. 1999;10:13–7.
Chadha RK, Subramanian A. The effect of visual impairment on quality of life of children aged 3–16 years. Br J Ophthalmol. 2011;95(5):642–5.
Dias L, Manny R, Hyman L, Fern K, Correction of Myopia Evaluation Trial Group. The relationship between self-esteem of myopic children and ocular and demographic characteristics. Optom Vis Sci. 2002;79(11):688–96.
Mavi S, Chan VF, Virgili G, Biagini I, Congdon N, et al. The Impact of Hyperopia on Academic Performance Among Children: A Systematic Review. Asia Pac J Ophthalmol. 2022;11(1):36–51.
Li D, Chan VF, Virgili G, Piyasena P, Negash H, Whitestone N, O'Connor S, Xiao B, Clarke M, Cherwek DH, et al. Impact of vision impairment and ocular morbidity and their treatment on depression and anxiety in children: a systematic review. Ophthalmology. 2022;129(10):1152–70.
Yi H, Zhang L, Ma X, Congdon N, Shi Y, Pang X, Zeng J, Wang L, Boswell M, Rozelle S. Poor vision among China’s rural primary school students: Prevalence, correlates and consequences. China Econ Rev. 2015;33:247–62.
Shankar S, Evans M, Bobier W. Hyperopia and emergent literacy of young children: Pilot study. Optom Vis Sci. 2007;84(11):1031–8.
Shashidhar S, Rao C, Hegde R. Factors affecting scholastic performances of adolescents. Indian J Pediatr. 2009;76(5):495–9.
Saw S, Cheng A, Fong A, et al. School grades and myopia. Ophthalmic Physiol Opt. 2007;27(2):126–9.
Dudovitz RN, Izadpanah N, Chung PJ, Slusser W. Parent, Teacher, and Student Perspectives on How Corrective Lenses Improve Child Wellbeing and School Function. Matern Child Health J. 2016;20(5):974–83.
Dudovitz RN, Sim MS, Elashoff D, Klarin J, Slusser W, Chung PJ. Receipt of Corrective Lenses and Academic Performance of Low-Income Students. Acad Pediatr. 2020;20(7):910–6.
Glewwe P, Park A, Zhao M. A better vision for development: Eyeglasses and academic performance in rural primary schools in China. J Dev Econ. 2016;122:170–82.
Nie J, Pang X, Wang L, Rozelle S, Sylvia S. Seeing Is Believing: Experimental Evidence on the Impact of Eyeglasses on Academic Performance, Aspirations, and Dropout among Junior High School Students in Rural China. Econ Dev Cult Change. 2019;68(2):335–55.
Uyan-Semerci P, Erdoğan E. Child Well-Being Indicators Through the Eyes of Children in Turkey. Int Soc Child Indic. 2017;10:267–95.
Promoting Positive Well-Being for Children: A Report for Decision-Makers in Parliament, Central Government and Local Areas [https://janwhitenaturalplay.files.wordpress.com/2012/01/promoting_positive_well-being_for_children_policy.pdf]
Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339: b2535.
Measuring What Matters for Child Well-being and Policies [https://www.oecd-ilibrary.org/content/publication/e82fded1-en]
CASP checklists. [https://casp-uk.net/casp-tools-checklists/]
Critical appraisal tools. [https://jbi.global/critical-appraisal-tools]
Dhirar N, Dudeja S, Duggal M, Gupta PC, Jaiswal N, Singh M, Ram J. Compliance to spectacle use in children with refractive errors- a systematic review and meta-analysis. BMC Ophthalmol. 2020;20(1):71.
Castanon Holguin AM, Congdon N, Patel N, Ratcliffe A, Esteso P, Toledo Flores S, Gilbert D, Pereyra Rito MA, Munoz B. Factors associated with spectacle-wear compliance in school-aged Mexican children. Invest Ophthalmol Vis Sci. 2006;47(3):925–8.
Dias L, Hyman L, Manny R, Fern K. The COMET Group: Evaluating the Self-esteem of Myopic Children Over a Three-Year Period: The COMET Experience. Optom Vis Sci. 2005;82(4):338–47.
Gogate P, Mukhopadhyaya D, Mahadik A, Naduvilath TJ, Sane S, Shinde A, Holden B. Spectacle compliance amongst rural secondary school children in Pune district. India Indian J Ophthalmol. 2013;61(1):8–12.
Jones-Jordan L, Wang X, Scherer RW, Mutti DO. Spectacle correction versus no spectacles for prevention of strabismus in hyperopic children. Cochrane Database Syst Rev. 2014;8(8):Cd007738.
Li Q, Yang J, He Y, Wang T, Zhong L, Zhu Z, Wang T, Ling S. Investigation of the psychological health of first-year high school students with myopia in Guangzhou. Brain Behav. 2020;10(4): e01594.
Ma X, Congdon N, Yi H, Zhou Z, Pang X, Meltzer ME, Shi Y, He M, Liu Y, Rozelle S. Safety of Spectacles for Children’s Vision: A Cluster-Randomized Controlled Trial. Am J Ophthalmol. 2015;160(5):897–904.
Monteiro GB, Temporini ER, de Carvalho KM. Use of optical aids by visually impaired students: social and cultural factors. Arq Bras Oftalmol. 2006;69(4):503–7.
Pinquart M, Pfeiffer JP. Psychological well-being in visually impaired and unimpaired individuals. Br J Vis Impair. 2011;29(1):27–45.
Odedra N, Wedner SH, Shigongo ZS, Nyalali K, Gilbert C. Barriers to spectacle use in Tanzanian secondary school students. Ophthalmic Epidemiol. 2008;15(6):410–7.
Orfield A, Basa F, Yun J. Vision problems of children in poverty in an urban school clinic: their epidemic numbers, impact on learning, and approaches to remediation. Journal of Optometry and Vision Development. 2001;32(3):114–41.
Qian DJ, Zhong H, Li J, Liu H, Pan CW. Spectacles utilization and its impact on health-related quality of life among rural Chinese adolescents. Eye (Lond). 2018;32(12):1879–85.
Robaei D, Kifley A, Rose KA, Mitchell P. Refractive error and patterns of spectacle use in 12-year-old Australian children. Ophthalmology. 2006;113(9):1567–73.
Vaughn W, Maples WC, Hoenes R. The association between vision quality of life and academics as measured by the College of Optometrists in Vision Development Quality of Life questionnaire. Optometry. 2006;77(3):116–23.
Walline JJ, Jones LA, Chitkara M, Coffey B, Jackson JM, Manny RE, Rah MJ, Prinstein MJ, Zadnik K. The Adolescent and Child Health Initiative to Encourage Vision Empowerment (ACHIEVE) study design and baseline data. Optom Vis Sci. 2006;83(1):37–45.
Wang CY, Zhang G, Tang B, Jin L, Huang W, Wang X, Chen T, Zhu W, Xiao B, Wang J, et al. A Randomized Noninferiority Trial of Wearing Adjustable Glasses versus Standard and Ready-made Spectacles among Chinese Schoolchildren: Wearability and Evaluation of Adjustable Refraction III. Ophthalmology. 2020;127(1):27–37.
Yi H, Zhang H, Ma X, Zhang L, Wang X, Jin L, Naidoo K, Minto H, Zou H, Lu L, et al. Impact of Free Glasses and a Teacher Incentive on Children’s Use of Eyeglasses: A Cluster-Randomized Controlled Trial. Am J Ophthalmol. 2015;160(5):889-896.e881.
von-Bischhoffshausen FB, Munoz B, Riquelme A, Ormeno MJ, Silva JC. Spectacle-wear compliance in school children in Concepcion Chile. Ophthalmic Epidemiol. 2014;21(6):362–9.
Black SA, McConnell EL, McKerr L, McClelland JF, Little JA, Dillenburger K, Jackson AJ, Anketell PM, Saunders KJ. In-school eyecare in special education settings has measurable benefits for children’s vision and behaviour. PLoS ONE. 2019;14(8): e0220480.
Bogdănici ST, Costin D, Bogdănici CM. Quality of life for amblyopic children and their parents. Rev Med Chir Soc Med Nat Iasi. 2015;119(1):214–20.
Esteso P, Castanon A, Toledo S, Rito MA, Ervin A, Wojciechowski R, Congdon NG. Correction of moderate myopia is associated with improvement in self-reported visual functioning among Mexican school-aged children. Invest Ophthalmol Vis Sci. 2007;48(11):4949–54.
Evans JR, Morjaria P, Powell C. Vision screening for correctable visual acuity deficits in school-age children and adolescents. Cochrane Database Syst Rev. 2018;2:CD005023.
Gogate P, Bhusan S, Ray S, Shinde A. Impact of correcting visual impairment and low vision in deaf-mute students in Pune. India Indian J Ophthalmol. 2016;64(12):898–903.
Morjaria P, Evans J, Gilbert C. Predictors of Spectacle Wear and Reasons for Nonwear in Students Randomized to Ready-made or Custom-made Spectacles: Results of Secondary Objectives From a Randomized Noninferiority Trial. JAMA Ophthalmol. 2019;137(4):408–14.
Nanthavisit U, Sornchai J, Jenchitr W. Survey of refractive errors among Buddhist scripture, Dhamma-Bali and regular school of Buddhist novices in the Bangkok metropolitan area. J Med Assoc Thai. 2008;91(Suppl 1):S24-29.
Schneider J, Leeder SR, Gopinath B, Wang JJ, Mitchell P. Frequency, course, and impact of correctable visual impairment (uncorrected refractive error). Surv Ophthalmol. 2010;55(6):539–60.
Sharma A, Congdon N, Patel M, Gilbert C. School-based approaches to the correction of refractive error in children. Surv Ophthalmol. 2012;57(3):272–83.
Gao Y, Lim EW, Yang A, Drobe B, Bullimore MA. The impact of spectacle lenses for myopia control on visual functions. Ophthalmic Physiol Opt. 2021;41(6):1320–31.
Queirós A, Villa-Collar C, Gutiérrez AR, Jorge J, González-Méijome JM. Quality of life of myopic subjects with different methods of visual correction using the NEI RQL-42 questionnaire. Eye Contact Lens. 2012;38(2):116–21.
Wills J, Gillett R, Eastwell E, Abraham R, Coffey K, Webber A, Wood J. Effect of simulated astigmatic refractive error on reading performance in the young. Optom Vis Sci. 2012;89(3):271–6.
Glewwe P, Park A, Zhao M. The Impact of Eyeglasses on the Academic Performance of Primary School Students: Evidence from a Randomized Trial in Rural China. In: 10th Joint Conference on Food, Agriculture and the Environment. Duluth: Center for International Food and Agricultural Policy; 2006. (No. 1685-2016-137082).
Guan H, Wang H, Du K, Zhao J, Boswell M, Shi Y, Qian Y. The Effect of Providing Free Eyeglasses on Children's Mental Health Outcomes in China: A Cluster-Randomized Controlled Trial. Int J Environ Res Public Health. 2018;15(12):2749
Hannum E, Zhang Y. Poverty and Proximate Barriers to Learning: Vision Deficiencies, Vision Correction and Educational Outcomes in Rural Northwest China. World Dev. 2012;40(9):1921–31.
Harvey EM, Miller JM, Twelker JD, Davis AL. Reading Fluency in School-Aged Children with Bilateral Astigmatism. Optom Vis Sci. 2016;93(2):118–25.
Ma Y, Congdon N, Shi Y, Hogg R, Medina A, Boswell M, Rozelle S, Iyer M. Effect of a Local Vision Care Center on Eyeglasses Use and School Performance in Rural China: A Cluster Randomized Clinical Trial. JAMA Ophthalmol. 2018;136(7):731–7.
van Rijn L, Krijnen J, Nefkens-Molster A, Wensing K, Gutker E, Knol D. Spectacles may improve reading speed in children with hyperopia. Optom Vis Sci. 2014;91(4):397–403.
Zhou Z, Chen T, Jin L, Zheng D, Chen S, He M, Silver J, Ellwein L, Moore B, Congdon NG. Self-refraction, ready-made glasses and quality of life among rural myopic Chinese children: a non-inferiority randomized trial. Acta Ophthalmol. 2017;95(6):567–75.
Statham J, Chase E. Childhood wellbeing: A brief overview. London: Childhood Wellbeing Research Centre; 2010.
Decarlo DK, McGwin G Jr, Bixler ML, Wallander J, Owsley C. Impact of pediatric vision impairment on daily life: results of focus groups. Optom Vis Sci. 2012;89(9):1409–16.
Narayanasamy S, Vincent S, Sampson G, Wood J. Visual demands in modern Australian primary school classrooms. Clin Exp Optom. 2016;99(3):233–40.
Falkenberg HK, Langaas T, Svarverud E. Vision status of children aged 7–15 years referred from school vision screening in Norway during 2003–2013: a retrospective study. BMC Ophthalmol. 2019;19(1):180.
Freudenberg N, Ruglis J. Reframing school dropout as a public health issue. Prev Chronic Dis. 2007;4(4):1–11.
Resnikoff S, Pascolini D, Mariotti S, Pokharel G. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008;86(1):63–70.
Wang S, Hao X, Ma X, Yu Y, Wu L, Wang Y, Li Y. Associations between Poor Vision, Vision-Related Behaviors and Mathematics Achievement in Chinese Students from the CNAEQ-PEH 2015. Int J Environ Res Public Health. 2020;17(22):8561.
Huang HM, Chang DS, Wu PC. The Association between Near Work Activities and Myopia in Children-A Systematic Review and Meta-Analysis. PLoS ONE. 2015;10(10): e0140419.
Kandel H, Khadka J, Goggin M, Pesudovs K. Impact of refractive error on quality of life: a qualitative study. Clin Exp Ophthalmol. 2017;45(7):677–88.
Kumaran SE, Balasubramaniam SM, Kumar DS, Ramani KK. Refractive Error and Vision-Related Quality of Life in South Indian Children. Optom Vis Sci. 2015;92(3):272–8.
Elsman E, Koel M, Van Nispen R, Van Rens G. Quality of Life and Participation of Children With Visual Impairment: Comparison With Population Reference Scores. Invest Ophthalmol Vis Sci. 2021;62(7):14.
Magakwe TSS, Hansraj R, Xulu-Kasaba ZNQ. The impact of uncorrected refractive error and visual impairment on the quality of life amongst school-going children in Sekhukhune district (Limpopo), South Africa. 2022;81(1):7.
Kaphle D, Kandel H, Khadka J, Mashige KP, Msosa JM, Naidoo KS. Validation and use of quality of life impact of refractive correction questionnaire in spectacle wearers in Malawi: A clinic-based study. Malawi Med J. 2020;32(2):54–63.
Robertson AO, Tadić V, Horvat-Gitsels LA, Cortina-Borja M, Rahi JS. Differences in Self-Rated Versus Parent Proxy-Rated Vision-Related Quality of Life and Functional Vision of Visually Impaired Children. Am J Ophthalmol. 2021;230:167–77.
Adams J, Hillier-Brown FC, Moore HJ, Lake AA, Araujo-Soares V, White M. Summerbell C: Searching and synthesising ‘grey literature’ and ‘grey information’ in public health: critical reflections on three case studies. Syst Rev. 2016;5(164):1–11.
Acknowledgements
None.
Funding
VFC is funded by Wellcome Trust (222490/Z/21/Z) and the Economic and Social Reseaecrh Council (R1148CPH). The funding bodies played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
VFC and PGP designed the study. PGP, ACY screened articles for inclusion, abstracted data from included studies and completed the data analysis. VFC AND PGP drafted the manuscript. VFC, PGP, ACY, KPM, and KSN edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pirindhavellie, GP., Yong, A.C., Mashige, K.P. et al. The impact of spectacle correction on the well-being of children with vision impairment due to uncorrected refractive error: a systematic review. BMC Public Health 23, 1575 (2023). https://doi.org/10.1186/s12889-023-16484-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16484-z