
Abstract
Background
Self-rated health status can be considered a good predictor of morbidity and mortality and has been used due to its easy assessment and applicability. The instrument is efficient for understanding sociodemographic, environmental and clinical conditions that may be related to the self-rated health status. Thus, this study aims to analyze the self-assessment of health status in rural workers and its association with socioeconomic characteristics, lifestyle, clinical condition and work characteristics.
Methods
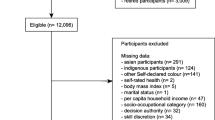
This is a cross-sectional study carried out with 787 male and female rural reporting agriculture as their main source of income in the municipality of Santa Maria de Jetibá. A simple and direct question was used “In general, compared to people your age, how do you rate your own state of health?” to see how rural workers rate their current health status. The independent variables analyzed were socioeconomic, clinical, health and work conditions. The magnitude of the associations was evaluated by means of hierarchical logistic regression.
Results
It was found that 42.1% of rural workers self-rated their health status as regular or poor. Belonging to socioeconomic classes C (OR = 1.937; 95% CI = 1.009–3.720) or D/E (OR = 2.280; 95% CI = 1.178–4.415), being overweight (or having excess weight) (OR = 1.477; 95% CI = 1.086–2.008), multimorbidity (OR = 1.715; 95% CI = 1.201–2.447) and complex multimorbidity (OR = 1.738; 95% CI = 1.097–2.751) were risk factors for worse self-rated health.
Conclusion
It was concluded that chronic diseases, socioeconomic status and overweight are risk factors for negative self-rated health. The identification of these determinants through self-rated status can support the planning of actions aimed at improving the health of the rural population.
Trial registration
This study was approved by the Research Ethics Committee of the Health Sciences Center of the Federal University of Espírito Santo (Protocol No. 2091172; CAAE No. 52839116.3.0000.5060). All research participants gave their informed consent.
Similar content being viewed by others

Background
The health of workers is conditioned by socioeconomic, lifestyle, medical condition and occupational factors [1]. The distinction between the characteristics of rural work and other activities is very particular, and among such differences we highlight the exhaustive working day, worker exposure to different weather conditions, contact with potentially harmful animals and plants, indiscriminate use of agricultural products, poor hygiene conditions, difficult access to health and education services, and low remuneration [2, 3].
A considerable portion of rural workers, especially those who handle pesticides without the correct use of individual protective equipment (IPE), can suffer impacts on their quality of life and consequently increased morbidity and mortality, which directly affect rural work [4,5,6]. Added to this is the difficult access to health services, especially in primary care [7], and as a result there is a combination of risk factors inherent to working in the field that demand special attention for this population.
It is noteworthy that the share of the agricultural sector in Brazil's gross domestic product (GDP) is 27.4%, the highest rate in the last 20 years [8]. However, the success of economic indicators does not reflect on social indicators and reflects even less on the working conditions and health of rural workers [1].
Self-rated health, a construct that involves physical, mental and social aspects of life through the individual's general perception of his/her health [9], has been widely used in epidemiological studies because it is a simple, subjective, easy-to-evaluate and applicable measure [10, 11]. It is also used for comparing health services and resource needs according to geographic areas and to calculate morbidity and mortality indicators [12,13,14] and functional decline [15].
In rural areas, the evidence on morbidity and actual health conditions is limited and inconsistent [16, 17]. Use of the self-rated health indicator can be a powerful tool to elucidate the determinants and conditions of health manifested in the rural environment and to support the planning of health care for this population. Thus, this study aims to analyze the self-rated health status in rural workers and its association with socioeconomic characteristics, lifestyle, clinical condition and work characteristics.
Methods
Study design, setting and participants
This is a cross-sectional study derived from a larger study entitled “Health condition and associated factors: A study of rural workers in Espírito Santo—AgroSaúdES”, funded by the Espírito Santo Research Support Foundation (FAPES; Grant FAPES/CNPq/Decit-SCTIE-MS/SESA-PPSUS No. 05/2015).
The study was carried out in the city of Santa Maria de Jetibá,located in the state of Espírito Santo, southeastern Brazil, and had the participation of male and female rural workers registered in the Family Health Strategy (FHS) whose main source of income was agriculture. More information about data collection and other research details can be found in a previous study [18].
The inclusion criteria considered were: age 18–59 years, not being pregnant, having agriculture as the main source of income and being in full employment for at least six months.
Data collection
Data collection took place between December 2016 and April 2017 on the premises of the health units of the studied municipality. A semi-structured questionnaire was administered with questions about socioeconomic, demographic and occupational characteristics, occupational contact with pesticides, lifestyle, eating habits, health status and self-rated health. In addition, anthropometric data were collected.
Measurements
Self-rated health status was assessed through the question: “In general, compared to people your age, how do you rate your own state of health?”. Possible answers were “very good”, “good”, “regular” and “bad”. For analysis, the variable was recategorized as “good/very good” and “fair/poor”.
Independent variables related to socioeconomic characteristics, lifestyle, health and work conditions were self-reported by the research participants. Sociodemographic variables included gender, age group, schooling, ethnicity, marital status, economic class and ties to the land.
Socioeconomic class was defined according to the Brazilian Economic Classification Criteria [19], where A and B are considered the highest economic levels, C as the intermediate level and D and E as low economic levels. Age group was categorized as “up to 29 years old”, “30–39 years old”, “40–49 years old” and “over 50 years old”, while schooling was established according to the number of years of study reported by the participant.
In relation to lifestyle, rural workers who reported smoking or not smoking but had smoked in the past were considered as a “current/previous smokers” and those who reported never having smoked as “non-smokers”. Alcohol intake was assessed by asking "How often do you drink alcohol?" and categorized as “never”, “less than once a month” and “more than once a month”. The rural workers were also asked if they performed any other physical activity besides those related to agricultural work. Individuals who accumulated at least 30 min of physical activity per day, at least 5 days a week, of moderate intensity were classified as physically active and the others were classified as physically inactive [20].
Body mass index (BMI) was defined from weight (kg) and height (m) data using the formula: BMI = Weight/(Height)2. World Health Organization (WHO) cut-off points were used for the classification of individuals as low weight (BMI < 18), normal (≥ 18.5 to < 25), overweight (≥ 25 to < 30) or obese (≥ 30) [21]. Subsequently, for a better analysis, the data were categorized into eutrophic/underweight and overweight/obesity. Waist circumference was also classified according to the WHO, considering values of ≤ 94 cm for men and ≤ 80 cm for women as “adequate” and values above these as “high/very high” [21].
To assess multimorbidity the presence of two or more chronic diseases was considered [22] and for complex multimorbidity the occurrence of three or more chronic conditions that affect three or more different body systems or domains was considered [23]. To determine the affected systems according to each disease, we used the 11th revision of the International Classification of Diseases (ICD-11): circulatory system (hypertension, stroke, heart attack, cardiac arrhythmia); endocrine, nutritional or metabolic disorders (diabetes, dyslipidemia, thyroid disorders); musculoskeletal or connective tissue system (arrhythmia); mental, behavioral or neurodevelopmental disorders (Alzheimer's, depression); genitourinary system (infertility, kidney disease); digestive system (liver cirrhosis); pulmonary system (bronchitis, asthma, pulmonary emphysema); and neoplasms (cancer) [18].
With regard to occupational characteristics, the following were evaluated: workload in hours per working week (time as a rural worker was categorized as “less than 10 years”, “10–29 years” and “over 30 years”); type of production; number of crops worked; contact and frequency of contact with pesticides, in addition to the amount of pesticides frequently in contact with; time of exposure to pesticides; and the use of IPE.
Statistical methods
Absolute and relative frequencies of the independent variables were calculated, according to the categories of the rural workers’ self-assessment of health status. A chi-square test was performed to verify the association between the independent variables and the outcome. Variables with p < 0.20 were included in the multivariate analysis.
Binary logistic regression was performed with five models according to previous studies [24, 25]. For the first four models, the Enter method was used to collect socioeconomic, behavioral, anthropometric, work and health variables, respectively. For the fifth model the Forward method was used to enter the predictor variables one by one according to their contribution to the model, leaving only statistically significant variables at the end. Adjusted odds ratios (OR), 95% confidence intervals (CI) and a significance level of 5% were presented.
Ethical aspects
This study followed all the ethical precepts of the Declaration of Helsinki and was approved by the Research Ethics Committee of the Health Sciences Center of the Federal University of Espírito Santo (Protocol No. 2091172; CAAE no. 52839116.3.0000.5060). All research participants gave their informed consent for study participation.
Results
Of the total 787 rural workers eligible for this study, 57.9% (N = 456) self-rated their health status as good or very good and 42.1% (N = 331) as fair or poor. Gender (p = 0.01) and socioeconomic class (p = 0.004) showed a statistical difference between the proportions of the categories (Table 1).
Table 2 shows the proportional differences in behavioral, anthropometric and health condition variables according to the self-assessment of health status. There is a statistical difference in BMI, waist circumference, multimorbidity and complex multimorbidity (overall p = <0.001).
The bivariate analysis between self-assessment of health status and work characteristics is described in Table 3. It is observed that, in this case, only the time working as a farmer showed a statistical difference (p = 0.047).
Table 4 shows the logistic regression models for the variables that showed p < 0.20 in the bivariate analysis. Gender, socioeconomic class, BMI, multimorbidity and complex multimorbidity were associated with the self-rated health. It was observed that males showed a reduction of 30% (p = 0.022; OR = 0.705; 95% CI = 0.522–0.951) in the chance of individuals negatively self-evaluating their own health. In addition, being in socioeconomic classes C (p = 0.047; OR = 1.937; 95% CI = 1.009–3.720) and D/E (p = 0.014; OR = 2.280; 95% CI = 1.178–4.415) almost doubled the chance of individuals negatively self-evaluating their own health. Being overweight was also shown to be a risk for negative self-rated health (p = 0.013; OR = 1.477; 95% CI = 1.086–2.008). Finally, the conditions of multimorbidity (p = 0.003; OR = 1.715; 95% CI = 1.201–2.447) and complex multimorbidity (p = 0.018; OR=1.738; 95% CI = 1.097–2.751) almost doubled the chance of individuals perceiving their health status as fair or poor. It is interesting to note that the same variables showed statistical significance independent of the model, as they were added to the analysis. This means that, in the case of the self-rated health status of rural workers, the socioeconomic, anthropometric, work and health condition variables did not influence each other but acted as a set of risk factors for the health of this population.
Discussion
This study showed a high prevalence of rural workers who self-rated their health as fair or poor, which was mainly associated with socioeconomic class, BMI and multimorbidity conditions, given that self-rated health status is an easily applicable indicator that considers biological, psychological, social, demographic and cultural factors, along with factors related to the living and working environment [24]. It is extremely important to understand how these factors affect rural populations so that the proper measures can be taken to prevent and protect the health of these individuals. The scarcity of studies on the health of rural populations in Brazil, the unique aspects associated with this population and the close relationship between self-rated health and morbidity/mortality [26] highlight the relevance and urgency of studying this topic for improving public health.
Self-assessment of health is widely used in Brazilian and international epidemiological studies because it has a strong predictive power for morbidity and mortality and the use of health services, in addition to its overall assessment of symptoms, illness and an individual's general well-being [27,28,29,30,31].
In the present study, the number of individuals who self-rated their health as fair or poor was greater than that observed in similar studies involving rural workers [17] and agricultural areas [16]. Recent population data from the Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Survey (VIGITEL) pointed out that 4.7% of the individuals evaluated their health status negatively, with this proportion being higher in women (5.5%) than in men (3.7%). In the capital of the state of Espírito Santo, this percentage was even lower, with a negative self-assessment of health by only 3.5% of the population [32]. Despite the methodological differences between VIGITEL and the present study, which limit comparison, the discrepancy between the prevalences found demonstrates the urgency of practical actions aimed at the health of individuals living in rural areas, where the prevalence of negative self-rated health is much higher and access to health services is difficult.
In accordance with what is established in the scientific literature [17, 33, 34], the present study found that women have a greater negative perception of their health status. One of the justifications for this fact may lie in the feeling of denial of weakness and rejection of help regarding health-care among men [35]. In this context, it may be that women are more attentive than men when faced with health problems and are more attentive to minor problems in their subjective assessment of health [36].
In the rural setting, it is worth noting that women have both limited access and accessibility to health services. Although used as synonyms, these terms have complementary meanings. Access concerns the provision of health services, which allows timely use to achieve the best possible results, that is, the way in which the person experiences the available service. Accessibility means the possibility that people have or do not have access to services [37]. The rural environment still has strong gender constructions that value male hegemony and female submission in decisions and opportunities, preventing the socio-institutional support [38].
The sociodemographic conditions should also be highlighted in the rural context. In the present study, there was a risk gradient for negative self-assessment of health status as socioeconomic class decreased. This finding has already been well established in the scientific literature, indicating that a higher socioeconomic level is associated with better self-rated health [24, 39, 40].
Favorable socioeconomic conditions directly influence a good assessment of health status [41]. This relationship can be explained by the greater purchasing power of materials and structural conditions in the higher classes, which have the potential to shape psychosocial factors and health behavior, favorably influencing the perception of health [39, 42].
In the specific case of rural workers, it is important to draw a historical parallel and mention the strong changes that took place after the Green Revolution, which aimed to maximize crop yields in different ecological situations [43] through genetic improvements in plants and the evolution of production apparatus [44, 45]. Such changes, marked by the mechanization of rural work, directly affected family-based agriculture, increasing inequality in the distribution of land and causing family agriculture to occupy a secondary and subordinate place in society, marked by struggles to gain space. itself in the economy [46,47,48].
Currently, according to data from the Food and Agriculture Organization of the United Nations [49], about 80% of world food production comes from family farming, occupying 18% of cultivated land in South America. In Brazil, more than 80% of agricultural exports are of the family type, which is why the country stands out as the eighth largest food producer in the world in this segment [50]. However, studies indicate that the gross monthly production value per family property is around 0.46 minimum wage, which represents a large part of the producers in extreme poverty. This reality reflects a risk to the sustainability of family farms [51] and partly explains the vulnerability that rural workers find themselves in when it comes to health.
In the present study, an association was found between excess weight, assessed through the BMI, and a negative self-assessment of health status, consistent with the scientific literature [52, 53]. This relationship has also been shown to be mediated by obesity-related comorbidities [54], such as cardiovascular disease and cancer [55, 56]. Furthermore, obesity is associated with reduced physical activity and lower exercise capacity, both conditions associated with low self-rated health [54].
In a longitudinal study, high BMI was associated with negative self-rated health, regardless of comorbidities. However, during the years of follow-up of the study, individuals who lost weight changed their perception of health previously evaluated as poor [52], showing that the BMI is an important predictor of how the individual evaluates his/her own health.
Conceptually, obesity is the result of several factors, and in this context the "environment" stands out, capable of directly affecting the individual's eating behavior and physical activity, and consequently, the energy balance [57]. For the authors, one of the environments is the "perceived environment", which highlights the individual's perception of the spaces in which he is inserted, such as the distance to leisure and food facilities [58] and consequently also to health services.
Agriculture is often described as a healthy occupation, associated with an image of a favorable lifestyle, with exposure to nature, outdoors, physical exertion and a diet based on natural foods [59]. However, this has not been the reality found in agricultural work. In addition to work-related injuries, such as physical trauma/injury and respiratory diseases, an increase in the prevalence of chronic diseases, such as arterial hypertension, dyslipidemia, diabetes and metabolic syndrome, is observed in the countryside [60,61,62,63,64,65]. Furthermore, morbidity and mortality rates from chronic health conditions are higher among rural populations compared to urban populations [66].
In this scenario enter the concepts of multimorbidity and complex multimorbidity. According to the WHO [67], multimorbidity is defined by the presence of two or more chronic diseases in the same individual. Complex multimorbidity is defined as the occurrence of three or more chronic conditions that affect three or more different body systems or domains [23].
In this study, individuals with multimorbidity and complex multimorbidity were more likely to perceive their health status as fair or poor. Petarli et al. [5], analyzing the same group of rural workers, showed the prevalence of multimorbidity and complex multimorbidity to be 41.5% and 16.7%, respectively. The most prevalent conditions were arterial hypertension, dyslipidemia and depression. Corroborating our findings, a controlled study in a rural population in China found that the presence of chronic diseases impacted changes in self-rated health status scores [67].
Agricultural work, added to sociodemographic characteristics and the reduced availability of health services, makes rural workers vulnerable to the implications and consequences of multimorbidity. The occurrence of multiple chronic conditions increases the demand for more complex care, creating a paradox between the need and the difficulty of reaching health services. This situation causes direct impacts for the patient, professionals and the health system, among which we can mention: complex health treatments, with potentially competing priorities and therapeutic goals [68]; a higher number of outpatient consultations and hospital admissions [69]; polypharmacy [70] and the higher cost of medicines and treatments [71]; and negative labor impacts, such as lower productivity and higher risk of unemployment [72].
Finally, considering that about 15 million people are currently engaged in agricultural activities in Brazil, the implications of reduced productivity associated with multimorbidity would be quite serious. Not only would the farmer be financially harmed, but this situation could compromise the food security of the population that consumes the food produced, and more broadly the country's GDP, since a large portion is dependent on agricultural activity [71].
The results of this study must be interpreted within the context of its limitations. Among them, the methodological design stands out, which does not allow for causal or temporal inferences about the associations found. In addition, some measures were based on self-report and therefore may be subject to recall bias, diagnostic suspicion and socially desirable responses. However, it is noteworthy that this is a population-based study with the assessment of aspects related to health having an unprecedented character in relation to the target population involved.
Conclusion
Gender, socioeconomic class, BMI and the conditions of multimorbidity and complex multimorbidity of rural workers were associated with the self-perception of health status. The results show that it is necessary to reassess the access and focus of the health system in rural areas, in addition to strengthening general primary care, with an appropriately qualified multidisciplinary team, so that holistic and continuous care is promoted in these populations.
Availability of data and materials
Dataset used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Dias, EC. 2006 "Condições de vida, trabalho, saúde e doença dos trabalhadores rurais no Brasil." Pinheiro TMM, organizador. Saúde do trabalhador rural–RENAST. Brasília. 1–27.
Brew B, Inder K, Allen J, Thomas M, Kelly B. The health and wellbeing of Australian farmers: a longitudinal cohort study. BMC Public Health. 2016;16:988. Published 2016 Sep 15. https://doi.org/10.1186/s12889-016-3664-y
Chengane S, Beseler CL, Duysen EG, Rautiainen RH. Occupational stress among farm and ranch operators in the midwestern United States. BMC Public Health. 2021;21(1):2076. https://doi.org/10.1186/s12889-021-12053-4.
Buralli RJ, Ribeiro H, Iglesias V, Muñoz-Quezada MT, Leão RS, Marques RC, Almeida MMC, Guimarães JRD. Occupational exposure to pesticides and health symptoms among family farmers in Brazil. Rev Saude Publica. 2020;54:133. https://doi.org/10.11606/s1518-8787.2020054002263.
Petarli GB, Cattafesta M, Luz TC, Zandonade E, Bezerra OM, Salaroli L. Exposição ocupacional a agrotóxicos, riscos e práticas de segurança na agricultura familiar em município do estado do Espírito Santo, Brasil. Rev. bras. saúde ocup. 44, 2019. https://doi.org/10.1590/2317-6369000030418
Tudi M, Li H, Li H, Wang L, Lyu J, Yang L, et al. Exposure Routes and Health Risks Associated with Pesticide Application. Toxics. 2022;10(6):335. https://doi.org/10.3390/toxics10060335.
International Labour Organization (ILO); 2021. [cited 2022 jun 20]. Available from: https://www.ilo.org/global/statistics-and-databases/publications/lang--en/index.html.
Instituto Brasileiro de Geografia e Estatística (IBGE). [cited 2022 jun 20]. Available from: https://www.ibge.gov.br/estatisticas/economicas/agricultura-e-pecuaria.html.
Doornenbal BM, Bakx R. Self-rated health trajectories: A dynamic time warp analysis. Prev Med Rep. 2021;24:101510. https://doi.org/10.1016/j.pmedr.2021.101510.
Pavão ALB, Werneck GL, Campos MR. Autoavaliação do estado de saúde e a associação com fatores sociodemográficos, hábitos de vida e morbidade na população: um inquérito nacional. Cadernos de Saúde Pública. 2013;29(4):723–34. https://doi.org/10.1590/S0102-311X2013000400010.
Lang T, Delpierre C. ‘How are you?’: what do you mean? Eur J Public Health. 2009;19:353. https://doi.org/10.1093/eurpub/ckp083.
Meng Q, Xie Z, Zhang T. A single-item self-rated health measure correlates with objective health status in the elderly: A survey in suburban Beijing. Front Public Health. 2014;214(2):27. https://doi.org/10.3389/fpubh.2014.00027.
Pagotto V, Bachion MM, Silveira EA. Autoavaliação da saúde por idosos brasileiros: revisão sistemática da literatura. Rev Panam Salud Publica. 2013;33(4):302–10.
Dong W, Pan X, Yu C, Lv J, Guo Y, Bian Z, et al. Self rated health status and risk of ischemic heart disease in the China Kadoorie Biobank study: a population based cohort study. J Am Heart Assoc. 2017;6:e006595. https://doi.org/10.1161/JAHA.117.006595.
DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question: a metaanalysis. J Gen Intern Med. 2006;21:267–75. https://doi.org/10.1111/j.1525-1497.2005.00291.x.
Moreira JP, Oliveira BL, Muzi CD, Cunha CL, Brito AS, Luiz RR. A saúde dos trabalhadores da atividade rural no Brasil. Cad Saúde Pública. 2015;31(8):1698–708. https://doi.org/10.1590/0102-311X00105114.
Martins-Silva T, Hirschmann R, Bortolotto CC, Fernandes MP, Ruivo A, Tovo-Rodrigues L. Health self-perception and morbidities, and their relation with rural work in southern Brazil. Rural and Remote Health. 2020;20:5424. https://doi.org/10.22605/RRH5424.
Petarli GB, Cattafesta M, Sant’Anna MM, de Paula Alves Bezerra OM, Zandonade E, Salaroli LB. Multimorbidity and complex multimorbidity in Brazilian rural workers. PLoS One. 2019;14(11):e0225416. https://doi.org/10.1371/journal.pone.0225416.
Associação Brasileira de Empresas de Pesquisa. Critérios de Classificação Econômica Brasileira 2014 [cited 2022 jun 20]. Available from: https://www.abep.org/criterio-brasil.
Waxman A. WHO global strategy on diet, physical activity and health. Food Nutr Bull. 2004;25(3):292–302. https://doi.org/10.1177/156482650402500310.
World Health Organization. Obesity: preventing and managing the global epidemic: report of a WHO consultation. Geneva: WHO Consultation on Obesity; 2000. p. 252p.
World Health Organization. Primary health care: now more than ever. Geneva: World Health Organization; 2008. p. 119.
Harrison C, Britt H, Miller G, Henderson J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ Open. 2014;4(7):e004694. https://doi.org/10.1136/bmjopen-2013-004694.
Petarli GB, Salaroli LB, Bissoli NS, Zandonade E. Autoavaliação do estado de saúde e fatores associados: um estudo em trabalhadores bancários. Cad Saude Publica. 2015;31:787–99. https://doi.org/10.1590/0102-311X00083114.
Silva LS, Barreto SM. Stressful working conditions and poor self-rated health among financial services employees. Rev Saude Publica. 2012;46(3):407–16. https://doi.org/10.1590/S0034-89102012005000023.
Guimarães JMN, Chor D, Werneck GL, Carvalho MS, Coeli CM, Lopes CS, et al. Association between self-rated health and mortality: 10 years follow-up to the Pró-Saúde cohort study. BMC Public Health. 2012;12:676. https://doi.org/10.1186/1471-2458-12-676.
DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. A meta-analysis J Gen Intern Med. 2006;21(3):267–75. https://doi.org/10.1111/j.1525-1497.2005.00291.x.
DeSalvo KB, Jones TM, Peabody J, McDonald J, Fihn S, Fan V, et al. Health care expenditure prediction with a single item, self-rated health measure. Med Care. 2009;47(4):440–7. https://doi.org/10.1097/MLR.0b013e318190b716.
Mavaddat N, Valderas JM, van der Linde R, Khaw KT, Kinmonth AL. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: a cross-sectional study. BMC Fam Pract. 2014;15:185. https://doi.org/10.1186/s12875-014-0185-6.
Mavaddat N, Parker RA, Sanderson S, Mant J, Kinmonth AL. Relationship of self-rated health with fatal and non-fatal outcomes in cardiovascular disease: a systematic review and meta-analysis. PLoS One. 2014;9(7):103509. https://doi.org/10.1371/journal.pone.0103509.
Santos TAP, Guimarães RA, Pagotto V, Aredes NDA, Siqueira ISL, Rocha SD, Carrijo CIS, Rosso CFW. Negative Self-Assessment of Health in Women: Association with Sociodemographic Characteristics, Physical Inactivity and Multimorbidity. Int J Environ Res Public Health. 2022;19(5):2666. https://doi.org/10.3390/ijerph19052666.
Vigitel Brasil 2021: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados brasileiros e no Distrito Federal em 2021 [cited 2022 jun 20]. Available from: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes-svs/vigitel/vigitel-brasil-2021-estimativas-sobre-frequencia-e-distribuicao-sociodemografica-de-fatores-de-risco-e-protecao-para-doencas-cronicas/@@download/file/vigitel-brasil-2021.pdf.
Castro BN, Staduto JAR. Percepção de saúde no Brasil: uma análise das diferenças por sexo dos trabalhadores. Econ soc. 2019;28(3):855–84. https://doi.org/10.1590/1982-3533.2019v28n3art10.
Malacoski FCF, Staduto JAR, Castro BNC. Saúde nas áreas rurais do nordeste e sul do Brasil: uma análise socioeconômica para homens e mulheres. Rev Econ NE. 2020;51(1):127–40.
Fernandes AA, Burnay R, Gomes I, Gil AP, Marques AM, Botelho AM. Envelhecimento e saúde: uma análise de gênero. Lisboa: Faculdade de Ciências Sociais e Humanas, 2012. p. 86
Spiers N, Jagger C, Clarke M, Arthur A. Are gender differences in the relationship between self-rated health and mortality enduring? Results from three birth cohorts in Melton Mowbray United Kingdom. Gerontologist. 2003;43(3):406–11. https://doi.org/10.1093/geront/43.3.406.
Starfield, B. Ministério da Saúde. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília: UNESCO, Ministério da Saúde; 2004.
Sehnem GD, Monteiro AS, Scopel MF, de Paula FM, Ianzer FR, Barbosa SC, et al. Acesso à atenção primária em saúde por mulheres residentes na zona rural: revisão integrativa. Res., Soc. Dev. 2020; 9(8):e50985338. https://doi.org/10.33448/rsd-v9i8.5338
Peres MA, Masiero AV, Longo GZ, Rocha GC, Matos IB, Najnie K, et al. Auto-avaliação da saúde em adultos no Sul do Brasil. Rev Saúde Pública. 2010;44(5):901–11. https://doi.org/10.1590/S0034-89102010000500016.
Hamplová D, Klusáček J, Mráček T. Assessment of self-rated health: The relative importance of physiological, mental, and socioeconomic factors. PLoS One. 2022;17(4):e0267115. https://doi.org/10.1371/journal.pone.0267115.
Alvarez-Galvez J, Rodero-Cosano ML, Motrico E, Salinas-Perez JA, Garcia-Alonso C, Salvador-Carulla L. The impact of socio-economic status on self-rated health: study of 29 countries using European social surveys (2002–2008). Int J Environ Res Public Health. 2013;10(3):747–61. https://doi.org/10.3390/ijerph10030747.
Moor I, Spallek J, Richter M. Explaining socioeconomic inequalities in self-rated health: a systematic review of the relative contribution of material, psychosocial and behavioural factors. J Epidemiol Community Health. 2017;71(6):565–75. https://doi.org/10.1136/jech-2016-207589.
Matos AK. Revolução verde, biotecnologia e tecnologias alternativas. Cadernos da FUCAMP. 2011;10(12):1–7. Available from: https://revistas.fucamp.edu.br/index.php/cadernos/article/view/134#:~:text=Resumo,cultivos%20em%20distintas%20situa%C3%A7%C3%B5es%20ecol%C3%B3gicas.
Miller GT. Ciência Ambiental. São Paulo: Thomson Learning; 2007. 123p.
Silva Santos AB, Veloso SL, de Oliveira HA. A modernização da agricultura e os impactos ambientais: da primeira revolução agrícola dos tempos modernos até os dias atuais. Anais SNCMA. 2017;13;8(1):1-9.
Blum R. Agricultura familiar: estudo preliminar da definição, classificação e problemática. Agric Fam. 2001;3:57–106. https://doi.org/10.5327/rcaa.v14i1.1415.
Wanderley MD. Raízes históricas do campesinato brasileiro. Agric Fam. 1999;3:21–55.
Altafin I. Reflexões sobre o conceito de agricultura familiar. Brasília: CDS/UnB. 2007. 1–23.
FAO. Food and Agricultural Organization. El trabajo de la FAO en la Agricultura Familiar: Prepararse para el Decenio Internacional de Agricultura Familiar (2019- 2028) para alcanzar los ODS. Nova York, Estados Unidos: FAO, 2018. [cited 2022 jun 20]. Available from: http://www.fao.org/3/ca1465es/CA1465ES.pdf.
Secretaria Especial de Agricultura Familiar e do Desenvolvimento Agrário (SEAD). [cited 2022 jun 18]. Available from: http://www.mda.gov.br/sitemda/secretaria/saf-creditorural/sobre-o-programa.
Bittencourt DD. Agricultura familiar, desafios e oportunidades rumo à inovação. Embrapa Recursos Genéticos e Biotecnologia-Capítulo em livro científico (ALICE). 2020. 15p.
Hellgren MI, Kitsche E, Groot-Zevert M, Lindblad U, Daka B. Association between body mass index and self-rated health: a Swedish population-based longitudinal study. Scand J Pub Health. 2021;49(4):369–76. https://doi.org/10.1177/1403494819875012.
Hulman A, Ibsen DB, Laursen ASD, Dahm CC. Body mass index trajectories preceding first report of poor self-rated health: A longitudinal case-control analysis of the English Longitudinal Study of Ageing. PLoS One. 2019;14(2):e0212862. https://doi.org/10.1371/journal.pone.0212862.
Sung ES, Choi CK, Jeong JA, Shin MH. The relationship between body mass index and poor self-rated health in the South Korean population. Plos one. 2020;15(8):e0219647. https://doi.org/10.1371/journal.pone.0219647.
Piché ME, Poirier P, Lemieux I, Després JP. Overview of epidemiology and contribution of obesity and body fat distribution to cardiovascular disease: an update. Prog Cardiovasc Dis. 2018;61(2):103–13. https://doi.org/10.1016/j.pcad.2018.06.004.
Swinburn B, Egger G, Raza F. Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev Med. 1999;29(6):563–70. https://doi.org/10.1006/pmed.1999.0585.
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N Engl J Med. 2003;348(17):1625–38. https://doi.org/10.1056/nejmoa021423.
Devlin N, Hansen P, Herbison P. Variations in selfreported health status: results from a New Zealand survey. N Z Med J. 2000;113:517–20.
Monteiro CA, et al. Monitoramento de fatores de risco para doenças crônicas por entrevistas telefônicas. Revista de Saúde Pública. 2005;39:47–5.
Pickett KE, Wilkinson RG. Income inequality and health: a causal review. Soc Sci Med. 2015;128:316–26. https://doi.org/10.1016/j.socscimed.2014.12.031.
Donham KJ, Meppelink SM, Kelly KM, Rohlman DS. Health indicators of a cohort of midwest farmers: health outcomes of participants in the certified safe farm program. J Agromedicine. 2019;24(3):228–38. https://doi.org/10.1080/1059924x.2019.1591316.
Abeywickrama HM, Wimalasiri KS, Koyama Y, Uchiyama M, Shimizu U, Chandrajith R, Nanayakkara N. Assessment of nutritional status and dietary pattern of a rural adult population in dry zone, Sri Lanka. Int J Environ Res Public Health. 2020;17(1):150. https://doi.org/10.3390/ijerph17010150.
van Doorn D, Richardson N, Osborne A. Farmers have hearts: the prevalence of risk factors for cardiovascular disease among a subgroup of irish livestock farmers. J Agromedicine. 2017;22(3):264–74. https://doi.org/10.1080/1059924x.2017.1318728.
Isara AR, Okundia PO. The burden of hypertension and diabetes mellitus in rural communities in southern Nigeria. The Pan African medical journal. 2015;20. https://doi.org/10.11604/pamj.2015.20.103.5619
Kapelios CJ, Kyriazis I, Ioannidis I, Dimosthenopoulos C, Hatziagelaki E, Liatis S. Diet, life-style and cardiovascular morbidity in the rural, free living population of Elafonisos island. BMC Public Health. 2017;17(1):1–1. https://doi.org/10.1186/s12889-017-4053-x.
Luz TC, Cattafesta M, Petarli GB, Meneghetti JP, Zandonade E, Bezerra OM, Salaroli LB. Cardiovascular risk factors in a Brazilian rural population. Cien Saude Colet. 2020;25:3921–32. https://doi.org/10.1590/1413-812320202510.36022018.
Wang L, Dong W, Ou Y, Chen S, Chen J, Jiang Q. Regional differences and determinants of self-rated health in a lower middle income rural Society of China. Int J Equity Health. 2018;17(1):162. https://doi.org/10.1186/s12939-018-0875-0.
Petarli GB, Salaroli LB, Cattafesta M. SAUDE, TRABALHO E AMBIENTE: um olhar interprofissional para a saude de populacoes rurais. Curitiba: Editora Appris, 2021.
Nunes BP, Soares MU, Wachs LS, Volz PM, Saes MD, Duro SM, Thumé E, Facchini LA. Hospitalization in older adults: association with multimorbidity, primary health care and private health plan. Revista de Saude Publica. 2017; 51. https://doi.org/10.1590/s1518-8787.2017051006646
Sum G, Hone T, Atun R, Millett C, Suhrcke M, Mahal A, Koh GC, Lee JT. Multimorbidity and out-of-pocket expenditure on medicines: a systematic review. BMJ global health. 2018;3(1):e000505. https://doi.org/10.1136/bmjgh-2017-000505.
Cabral GG, de Souza AC, Barbosa IR, Jerez-Roig J, Souza DL. Multimorbidity and its impact on workers: a review of longitudinal studies. Saf Health Work. 2019;10(4):393–9. https://doi.org/10.1016/j.shaw.2019.08.004.
Centro de Estudos Avançados em Economia Aplicada - CEPEA. Série histórica do PIB do agronegócio brasileiro. 2020. [cited 2022 jun 18]. Available from: https://www.cepea.esalq.usp.br/br/pib-do-agronegocio-brasileiro.aspx.
Acknowledgements
Our thanks go to the researchers and Research and Innovation Support Foundation of Espírito Santo (FAPES).
Funding
This work was supported by the Research and Innovation Support Foundation of Espírito Santo (FAPES; Grant FAPES/CNPq/Decit-SCTIE-MS/SESA-PPSUS-No. 05/2015]. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
C.A.M., C.B.P., J.R.S.F.: analysis and interpretation of data, article writing, relevant critical review of intellectual content and approval of the final version; E.Z., O.M.P.A.B.: conception, design, analysis and interpretation of data; and L.B.S.: conception, design, analysis and interpretation of data, article writing, relevant critical review of intellectual content and approval of the final version. All authors are responsible for all aspects of the research to ensure the accuracy and integrity of the study. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study followed all the ethical precepts of the Declaration of Helsinki and was approved by the Research Ethics Committee of the Health Sciences Center of the Federal University of Espírito Santo (Protocol no. 2091172; CAAE no. 52839116.3.0000.5060). All research participants gave their informed consent for study participation.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Martins, C.A., do Prado, C.B., Ferreira, J.R.S. et al. Self-rated health status and associated factors in rural workers. BMC Public Health 23, 680 (2023). https://doi.org/10.1186/s12889-023-15548-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15548-4