
Abstract
Background
Failure to use antenatal care (ANC) and inadequate receipt of components of ANC pose a significant risk for the pregnant woman and the baby. This study aimed to examine a regional analysis of factors associated with receiving no ANC and inadequate receipt of components of ANC services among Indian women.
Method
Information from 173,970 women of reproductive age 15–49 years from the 2019–21 India National Family Health Survey (NFSH-5) was analysed. Logistic regression analyses that adjusted for cluster and survey weights were conducted to assess the socio-demographic and other factors associated with receiving non-use of ANC and inadequate receipt of components of ANC, respectively, in the six regions and 28 states, and 8 union territories in India.
Results
Across regions in India, 7% of women reported no ANC, and the prevalence of inadequate and adequate receipt of components of ANC in all six regions ranged from 67 to 89% and 8% to 24%, respectively. Of all the 36 federated entities, the prevalence of inadequate receipt of ANC components was less than two-thirds in Tamil Nadu, Puducherry, Andaman and the Nicobar Islands, Odisha, and Gujarat. Our analyses revealed that associated factors vary by region, state, and union territories. Women from poor households reported increased odds of receiving no ANC in North, East and North-eastern regions. Women who reported no schooling in South, East and Central regions were associated with increased odds of receiving no ANC. Women from poor households in Himachal Pradesh, Bihar, Uttar Pradesh, Nagaland, Manipur, Uttar Pradesh, and Madhya Pradesh states reported significantly higher odds of inadequate components ANC than women from rich households. The receipt of inadequate components of ANC was significantly higher among women who never read magazines in Delhi, Ladakh, Karnataka, Telangana, Jharkhand, Maharashtra, Uttar Pradesh, Chhattisgarh, Arunachal Pradesh, Manipur, and Mizoram states in India.
Conclusion
A better understanding of the factors associated with and incorporating them into the short- and long-term intervention strategies, including free financial support from the Indian government to encourage pregnant women from lower socioeconomic groups to use health services across all regions, states and union territories.
Similar content being viewed by others


Background
Globally, 830 women die daily due to pregnancy- and/or childbirth-related complications [1]. Evidence from the Global Burden of Disease, Injuries and Risk Factors (GBD) study in 2015 revealed that 75% of these maternal deaths could be attributed to inadequate use of antenatal care (ANC) services which may lead to pregnancy or childbirth complications, particularly in low- and middle-income countries (LMICs), including South Asian countries [2]. According to the World Health Organization (WHO), adequate receipt of ANC consists of 4 or more ANC visits and the receipt of 7 or more ANC service components [3]. The components of adequate ANC include: confirming the pregnancy date and expected time of delivery; obstetric examination and blood pressure check; urine and blood test; treatment of diseases as required; tetanus toxoid vaccination; iron and folate acid (IFA) supplementation; and health education on self-care, nutrition and sleeping under insecticide-treated bed-nets [3,4,5].
The global burden of maternal and child morbidity and mortality due to inadequate receipt of ANC services could be reduced with the effective implementation of health education and health promotion strategies in routine ANC visits [3]. India has one of the highest maternal deaths in South Asia, and it lies between 214 and 300 maternal deaths per 100,000 live births. This estimate shows that the country lags well behind the Sustainable Development Goal (SDG-3) of reducing maternal deaths to less than 70 maternal deaths per 100,000 live births by 2030 [1, 6]. In a recent study conducted in South Asian countries, lower maternal education and household wealth index, a lack of family support for women to access ANC services, a lack of quality ANC counselling and an inadequate supply of required nutritional supplements were barriers to adequate receipt of ANC services [7].
In India, few discrete subnational studies have described relevant factors associated with the non-use or limited use of ANC services as well as the non-receipt of adequate ANC services. A study conducted in the eastern region, Bihar showed that only some 40% of pregnant women attended 4 or more ANC visits and received IFA supplements [8]. A separate study conducted in the northern region of Uttar Pradesh indicated that higher-caste women were significantly more likely to utilise ANC services compared to women belonging to the lower castes [9]. Another study conducted in the same region affirmed that higher socioeconomic status was associated with an increased likelihood of receiving most ANC service components [10]. The findings concurred with a study conducted in the four southern Indian states, women from disadvantaged socioeconomic households were significantly less likely to receive quality ANC compared to their counterparts [11]. Using national-level data, studies have elucidated other determinants of ANC service [12,13,14]; however, the use of national data can mask subnational differences, particularly given the significant disparities in socioeconomic and health service indicators across India [15].
A recent population-based study on utilisation, equity and determinants of full antenatal care in India found that mothers with low education and low income were associated with full ANC utilization [16]. However, this study only adjusted for a few confounding factors because they used the concentration index method, and the examination of receipt of ANC components was not examined by combining both frequency and receipts of ANC. Hence, investigating both the receipt of ANC and the receipt of components of ANC are important factors for reducing maternal and neonatal mortality, particularly in regions, states and Union territories in India.
Therefore, understanding regions, states and union territories factors associated with inadequate receipt of ANC components and non-use of ANC in India is needed to guide initiatives that can give greater priority to improving maternal and child health services in the country. Hence, this study aimed to investigate the factors associated with inadequate receipt of components and non-use of ANC services in India using HFSH-5. The findings from this study will be relevant to policymakers, health practitioners and women’s health advocates in informing policies and programs to improve ANC and to design initiatives to provide appropriate ANC services to Nigerian women.
Methods
Data source
The study used the National Family Health Survey (NFSH-5, also called the 2019–21 India Demographic Health Surveys (DHS) dataset. The NFHS-5 is a population-based survey collected by the Indian Ministry of Health, with technical assistance provided by the Inner-City Fund (ICF) International, Maryland, USA. The NFHS-4 collects data on women’s health (e.g., ANC, births, postnatal care and domestic violence information), infant and young children’s health (e.g., feeding practices), as well as socioeconomic characteristics, encompasses a nationwide sample of women between aged 15 and 49 years from 724,115 interviewed, yielding a response rate of 96.9%.
The overall sample was obtained using a two-stage sampling design for rural and urban areas in India. Villages and census enumeration blocks were the primary sampling units (PSU). In the first stage of the sampling, approximately 300 households were selected from the initial rural and urban PSU, these were further divided into segments of 100–150 households. In the NFHS-5, two out of the selected segments were randomly selected for the NFHS-5 survey, using systematic sampling with probability proportional to segment size, where a cluster was either a PSU or a segment of a PSU. In the second stage, 22 households were randomly selected from each rural and urban cluster using a systematic sampling approach [15]. The response rates were over 95% in every Indian state and territory except 94.0% in Madhya Pradesh [15, 17] and 81% in Chandigarh [15]. Detailed information on the survey methodology is noted in the NFHS-5 reports [15].
In our study, we restricted the analyses to the most recent singleton live birth within the five years preceding the NHHS-5 survey to reduce the potential effect of recall bias, and this approach is consistent with past studies [13]. This approach yielded a weighted total of 173,370 samples.
Outcome variables
This study considered two outcome variables: The frequency of ANC visits, and the second outcome relates to receiving the recommended essential receipts of ANC components during pregnancy. In the second outcome variable, we created a composite score of receipts of ANC components which comprises a simple count of the receipts of ANC components a pregnant mother received in her most recent birth within the five years prior to the survey. The second outcome variable had a minimum value of zero, indicating that a pregnant mother did not receive any ANC service and a maximum value of nine, indicating that the women received services for all the nine receipts of ANC components. The outcome variables for this study were divided into 3 categories: 1) adequate receipt of ANC components, 2) inadequate receipt of ANC components, and, 3) no ANC visit. In our analysis of regions, states and union territories, adequate receipt of ANC components was assigned ‘0’, inadequate receipt of ANC components was categorised as ‘1’, and adequate receipt of ANC components was assigned ‘0’ no ANC was assigned ‘1’. No ANC visit category included infants whose women never attended any ANC visits during pregnancy. Inadequate receipt of ANC components are infants whose women reported less than four ANC visits during pregnancy and used less than nine receipts of ANC components, and adequate receipt of ANC components are infants whose women attended four or more ANC visits during pregnancy and used all the nine receipts of ANC components.
According to the WHO, appropriate components of ANC include: confirming the pregnancy date and expected time of delivery; obstetric examination and blood pressure check; urine and blood test; treatment of diseases if required; tetanus toxoid vaccination; iron and folate supplementation; and health education on self-care, nutrition and sleeping under insecticide-treated bed-nets [3]. In the present study, the nine components of ANC were based on the NFSH-5 surveyed items. These components included: a) told about pregnancy complications, b) had abdomen examined, c) weight measured during pregnancy, d) given IFA supplementation, e) given the drug for intestinal parasites, f) had tetanus injection before birth, g) blood pressure check, h) urine and i) blood test during pregnancy.
Study variables
We used the modified Anderson’s behavioural model framework [18] to group the factors potentially associated with inadequate receipt of ANC components (Fig. 1). Twenty-five potential risk factors were identified and categorised into four main groups: 1) community-level factors, 2) predisposing (socio-demographic and health knowledge), 3) enabling including health services and 4) need factors.

Conceptual framework adapted from Anderson behavioural model
The study factors selected were based on Fig. 1 and evidence from previous studies on ANC [14, 19, 20]. The study factors included community and socioeconomic, health knowledge, enabling and need factors. Community factors include the place of residence, and socio-demographic include maternal age at delivery, household wealth index; maternal education; place of delivery; maternal marital status; maternal working status, combined birth rank and interval. The health knowledge factors are frequency of listening to the radio, watching television and reading newspapers, knowledge of delivery complications and knowledge of post-delivery complications. Enabling factors were permission to visit health services, distance to health services, not wanting to go alone to health care, getting money to pay for health services, postnatal checkups and women’s autonomy factors (power over earning, power over household decision-making, wife beaten for refusing sex, attitude to domestic violence). A detailed description of all these study factors is provided in Supplementary Table 1 and the NFHS-5 report [15].
The household wealth index was obtained from a principal components statistical method conducted by the International Institute for Population Sciences (IIPS) and ICF International and was calculated as a score of ownership of about 22 household assets such as transportation devices, and ownership of durable goods and household facilities. The IIPS and ICF International classified the household wealth index into five categories. Each household was assigned to one of these categories: poorest, poorer, middle, rich and richest. These data were re-categorised, where the bottom 40% were referred to as poor households, the next 40% classified as the middle households and the top 20% as rich households to ensure an adequate sample in each category [21, 22] and detailed information regarding the definition and categorisation of potential variables used in the study are provided in Supplementary Table 1.
Statistical analysis
Data analysis was performed using the survey "svy" commands of Stata version 13.1 (Stata Corp, College Station, TX, USA), which allowed for adjustments for sampling weights. The Taylor series linearization method was used to estimate confidence intervals (CIs) around prevalence estimates in the surveys. First, regional frequency tabulations were conducted to describe the data used in this study, followed by the Taylor series linearization method in the surveys when estimating 95% CIs around the regional prevalence of no ANC, inadequate and adequate receipt of components of ANC. Two logistic regression analyses models that adjusted for clustering and sampling weights were used to identify factors with non-ANC or inadequate receipt of components of ANC for each region, 28 states and 8 union territories, respectively, and detailed information on how the regions were classified has been reported elsewhere [23].
As part of the multivariable logistic analyses, a five-stage model was performed by following a similar conceptual model approach to Andersen’s [24]. In the first modelling stage, community and socioeconomic factors were first entered into the model to assess their associations with the study outcomes. A manually executed backward elimination method was conducted to select factors significantly associated with the outcomes. In the second model, the significant factors in the first stage were added to health knowledge factors, and a manually executed backward elimination procedure followed this. A similar approach was used for enabling health services and need factors in the third, fourth and fifth stages, respectively. To avoid any statistical bias, we double-checked we manually executed the backwards elimination method by using the following procedures: (1) we entered only potential risk factors with P-value < 0.20 in the backward elimination process, (2) we tested the backward elimination by also including all variables (all potential risk factors); and (3) we tested and reported any collinearity in the final model. The odds ratio (OR) with 95% CIs were calculated to assess the adjusted risk of independent variables, and those with P < 0.05 were retained in the final model.
Results
Regional characteristics of the study participants
Table 1 reported the regional characteristics of the study population across all regions in India. More than two-thirds of the women surveyed were aged between 20 and 29 years. As summarised in Table 1, over 50% of the women surveyed who resided in India’s Northern, Southern and Western regions were classified as rich, whilst above 50% of women from the Eastern, Central and North-Eastern regions were poor. Across all the six regions, less than 2% of women were either divorced, separated, or widowed. More than 83% of the women delivered their babies in a health facility, with the highest percentage in the Southern region (98.4%) and the lowest in the North-Eastern region (83.3%). Across all six regions, more than 80% of women reported that their husbands have power over money earned and authority over household purchasing decision-making.
Regional prevalence of receipt of components of ANC visits
Table 2 revealed the regional prevalence receipt of components of ANC visits received by Indian women during their last pregnancy. Over 90% of women who lived in the Northern, Southern, North-Eastern and Western regions had their abdomen examined, weight measured, blood pressure checked, and urine and blood test during pregnancy. Over 85% of women received IFA supplementation across all the regions in India.
The proportion of pregnant women who received intestinal parasites drugs as part of ANC varied from 14% to 45.5%, with the highest rate in the Southern region (45.5% of the study sample) and the North-Eastern region having the lowest reported rate (14%). Nationally, about half of the components of ANC were suboptimal (< 90%) and these included, told about pregnancy complications, IFA and intestinal parasites drugs (see Table 2 for details).
Regional prevalence of no, inadequate and adequate receipts of components of ANC
Figure 2 shows the regional prevalence and 95% CIs of no ANC, inadequate receipts, and adequate receipts of ANC components by regions in India. The prevalence of no ANC ranged between 5 and 9% in North-Eastern, Central and Eastern regions, with the overall national prevalence of 6.8% (95%CI: 6.6–7.0). The prevalence of no ANC was significantly higher in the Eastern and Central regions and was lower in the West and Eastern regions. Inadequate receipt of ANC components lies between 72 and 89%, the lowest prevalence is in the North-Eastern region, and the highest prevalence is in the Western region, with an overall prevalence of 80.4% (95%CI: 80.1–80.7) across India.

Regional prevalence and 95%CI of no, inadequate and adequate receipt of the components of ANC visits by Regions in India, NFSH-5
The Central region had a significantly lower prevalence of inadequate receipt of ANC components. In contrast, the prevalence of inadequate receipt of ANC components did not differ statistically in the Eastern and South regions. The Eastern and Western regions reported the highest prevalence of adequate receipt of ANC components, while the Central region reported the lowest (see Fig. 2).
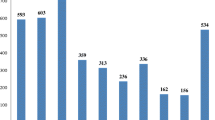
The prevalence of receipt of ANC by the 28 states and 8 Union territories in India was presented in supplementary Fig. 1. The prevalence of no ANC visits was over 1.0% in Nagaland, Manipur, Odisha, Gujarat, Maharashtra, Karnataka, Goa, and Lakshadweep and less than 5.0% in Rajasthan, Uttar Pradesh and Bihar. Of all the 36 federated entities, the prevalence of inadequate receipt of ANC components was less than 7.0% in 5 entities: Tamil Nadu, Puducherry, Andaman and the Nicobar Islands, Odisha and Gujarat. The prevalence of adequate receipt of ANC components was over 30% in Tamil Nadu, Puducherry, Andaman and Nicobar Islands and Odisha (see Supplementary Fig. 1 states for details).
Factors associated with no ANC
The odds of no ANC visit were significantly higher among women who reported no postnatal checkup after delivery in all five regions except the North-eastern region of India. No ANC visit was significantly higher among women with no education in South, East and Central regions, and no ANC visit was significantly higher among women with limited knowledge of delivery complications in all regions except in the North-eastern region. Women from poor households in in North, East and North-eastern regions significantly reported higher odds of no ANC visit (Table 3).
In all regions, the odds of no ANC visit were higher among first time mothers. Women who did not use contraceptives reported higher odds of no ANC in all regions except in the South and North-eastern regions. Similarly, the odds of no ANC visit were significantly higher among women who reported that distance to health facilities was not a big problem in the South and North-Eastern regions. Women who had no intention to become pregnant were significantly more likely to make no ANC visits in the East, West and Central regions.
Women who had never listened to the radio significantly reported higher odds of no ANC visit in the Northern (AOR = 1.99; 95%CI: 1.42 to 2.79) and Southern regions (AOR = 1.41; 95%CI: 1.17 to 1.68) and women who never watched television reported increased odds of receiving no ANC visit in the South (AOR = 1.29; 95%CI: 1.10 to 2.52), East (AOR = 1.50; 95%CI: 1.30 to 1.74) and Central regions (AOR = 1.35; 95%CI: 1.20 to 1.51). Women who lived in rural areas in North and South regions, and their first child reported higher odds of receiving no ANC in all regions except Central and North-eastern regions.
In the state analysis for no ANC, older women (30 +) and women with limited post-delivery complication in Delhi. Women who never watched television and had no PNC in Jammu Kashmir reported higher odds of no ANC visit. Women who delivered their babies in Uttar Pradesh state and women who never watched television in Kerala states in South India were significantly more likely to make no ANC visits. Women from Mizoram in India who did not use contraceptives reported higher odds of No ANC and women from poor households in Arunachal Pradesh state (AOR = 2.75; 95%CI: 1.82 to 4.16) and women from Tripura state with limited knowledge of delivery complication AOR = 1.49; 95%CI: 1.00 to 2.65) were significantly more likely make no ANC visits (see, Tables 1–6 in Supplementary Table 2 for details).
Factors associated with inadequate receipt of ANC components
As shown in Table 4, the receipt of inadequate components of ANC was significantly lower among women with no schooling in all regions except the West region, and the receipt of inadequate components of ANC was significantly lower among women from poor and middle-income households in the East, West and North-eastern regions. The receipt of inadequate components of ANC was low among women who listened to the radio at least once a week.
Women with limited knowledge of delivery complications reported significantly higher odds of inadequate components ANC in the North (AOR = 1.18; 95%CI: 1.01 to 1.38) and East (AOR = 1.24; 95%CI: 1.08 to 1.41) regions. The odds of inadequate components of ANC in the Eastern and Central were significantly higher in women who intended not to become pregnant than in women who intended to become pregnant now by 26% and 34%, respectively. Older women (aged 30 plus) were significantly higher odds of inadequate components ANC in South and East regions. Place of delivery by inadequate components ANC varies lower odds in North region and higher odds in Central and North-eastern regions.
Women who had 2nd or 3rd birth rank infants and a short birth interval of less than or equal to two years reported higher odds of inadequate components of ANC in all regions except North and West regions. The odds of receiving inadequate components of ANC were significantly higher among women in Central (AOR = 1.62; 95%CI: 1.26 to 2.08) region who reported that distance to health services was a big problem. Participants who reported joint decision-making in the household were more likely to report inadequate components of ANC in the East region (AOR = 1.21; 95%CI: 1.00 to 1.45).
The odds of inadequate components of ANC in were significantly higher among women with no schooling in Jammu Kashmir. Women from poor households in Himachal Pradesh, Bihar, Uttar Pradesh, Nagaland, Manipur, Uttar Pradesh, and Madhya Pradesh states in India reported higher odds of inadequate components ANC than women from rich households. Women with limited knowledge of delivery complications reported significantly higher odds of inadequate components ANC in Himachal Pradesh, Punjab, Haryana, Delhi, Andhra Pradesh, Karnataka, Kerala, Tamil Nadu, Puducherry, Andaman Nicobar, Uttar Pradesh, Chhattisgarh, Madhya Pradesh, Sikkim, Nagaland, and Assam states in India. The receipt of inadequate components of ANC was significantly higher among women who never read magazines in Delhi, Ladakh, Karnataka, Telangana, Jharkhand, Maharashtra, Uttar Pradesh, Chhattisgarh, Arunachal Pradesh, Manipur and Mizoram states in India (see, Tables 1–6 in Supplementary Table 3 for details).
Discussion
Main findings
The components of ANC received by Indian women varied in the present study. Approximately seven percent (6.8%) of Indian women reported no ANC visit during pregnancy, and over three-quarters (80%) of Indian women reported inadequate receipts of ANC components, with varied subnational prevalence estimates. Several factors have emerged in this regional analysis that explain the inadequate receipt of ANC components and no ANC across India, and these associated factors vary by region, state, and Union territories; these factors are discussed below.
A recent study revealed that pregnant women in low and middle-income countries do not have access to all ANC components recommended by WHO [25]. This study found that the prevalence of inadequate receipt of ANC components and no ANC were lower (< 5.0%) in the Western and Eastern regions than the Indian national average. We reported that blood pressure check, weight check during pregnancy, and having blood and urine sample collected for investigation was relatively high (> 80%) in all regions of India. However, the prevalence of drugs for intestinal parasites during pregnancy was low in all six Indian regions. These findings are consistent with a district-level study conducted in India for ANC visits, Tetanus Toxoid vaccination (TT) and IFA, where the results showed that more emphasis needs to be given to the comprehensive provision of ANC components [10].
Factors associated with inadequate receipt of ANC components
Our study found that residing in rural areas was associated with inadequate ANC components in the Central, Eastern regions and Lakshadweep states in India. This result was consistent with other studies conducted in developing countries [18,19,20]. A possible cause of inadequate receipt of ANC components in the rural Central, Eastern region and Lakshadweep states in India could be attributed to little or no access to media, low level of education, less availability of health facilities and skilled health personnel and cultural methods adopted in pregnancy [10]. This finding could also relate to the fact that major health centres and hospitals in India are located in urban areas, making rural pregnant women prefer receiving ANC components at home [26]. In addition, various programs, such as the free distribution of IFA supplements and drugs for intestinal parasites, should be integrated with ANC to improve the quality of ANC components provided at the rural level [19].
We found that women who reported limited knowledge about delivery complications had higher odds of inadequate receipt of ANC components including 16 states and union territories in India. These findings are consistent with a cross-sectional study conducted in Indonesia which found that women with inadequate receipt of ANC had higher odds of labour complications [22]. Similarly, a cross-sectional study conducted in Assem, India, found that women who received inadequate receipt of ANC were more likely to report delivery complications and post-delivery complications than those who received adequate ANC receipts [22]. These findings mirrored a recent study from India, which indicated that less than half of the pregnant women did not receive the minimum recommended 4 ANC visits [12]. A possible reason for the higher odds could be the distance to health facilities and limited knowledge about delivery and post-delivery complications [27]. Women may prefer not to deliver at the hospital due to the low-quality health facilities and distance to health facilities [28].
This study noted that women who delivered their babies at home reported higher odds of inadequate receipt of ANC than those who delivered their babies at the health facility in northern region and Gujarat state in West India; but the opposite finding was noted in central, north-eastern regions and Jammu Kashmir and Bihar state in India. The preference for home delivery among pregnant Indian women could be due to traditional cultural beliefs, the family’s financial ability to pay for health services, transport and access to the health facility, previous uncomplicated home deliveries, and fear of medical procedures, including obstetric examination [19, 25]. Women who had never listened to the radio and watched television reported mixed results across the six Indian regions. A cross-sectional study in India supported these findings and revealed a strong relationship between media exposure and at least eight ANC visits [29]. Also, insufficient access to media such as radio, magazines, and television could be linked to poor maternal awareness about ANC services [30]. Overcoming these barriers to inadequate receipt of ANC components by taking considerate actions at individual and community levels would enable the Indian government to achieve the SDG-3 of ensuring good health and promoting well-being.
Bruce et al. [19] women who reported later or had no intention to become pregnant had higher odds of inadequate receipt of ANC components in the North and Eastern regions. These findings agreed with a systematic review that examined the effect of ANC in developing countries which found that higher-order births were associated with increased odds of inadequate use of ANC [31].
In this study, we observed that women with no schooling and/or those from poorer households reported a higher likelihood of inadequate receipt of ANC components compared to their counterparts in almost all Indian regions, including 9 states. As previously suggested, women from low socioeconomic groups have limited knowledge about ANC visits and ANC components, delivery and post-delivery complications, and postnatal checkups or family planning [12, 27]. These findings are also consistent with other studies from low-and middle-income countries such as Nepal [32], Pakistan [33, 34] and Nigeria [18], which highlighted that low maternal education levels and poorest households are associated with inadequate receipt of ANC components. However, there is a need for the Indian government to educate women on how ways to improve their health outcomes, especially during pregnancy and by providing free ANC services, including ANC components for pregnant women from low socioeconomic groups, especially those rural women.
Factors associated with no ANC
We found that women with no Schooling and/or those from poorer households were more likely to not utilise ANC services in many Indian regions, including 7 states. This finding is similar to other studies conducted in developing countries where low maternal education was one of the factors for no ANC visits [18, 33, 35]. A recent population-based study conducted in India in 2019 examining the enablers and barriers of ANC services revealed that maternal education was associated with several ANC visits [13].
Our study showed that women who delivered their babies at home were less likely not to use ANC services in the central, eastern, and western regions compared to their counterparts. However, the opposite result was noted in the northeastern region, where women who delivered their babies at the health facility were less likely not to use ANC services compared to women who delivered their babies at home. Part of the study finding supported research conducted in South Asia which showed that women who had more than three ANC visits reported a 7% higher probability of using a health facility for birthing compared to their counterparts who delivered at home with limited ANC visits [36]. Empowering Indian women through education would promote a better understanding of health messages, including enabling pregnant women to choose institutional delivery, better decision-making capacity in the household and knowledge about delivery and post-delivery complications [27].
The study showed that higher birth rank and long birth intervals reported higher odds of no ANC in all regions. These findings were supported by a cross-sectional study conducted in 12 East African countries which revealed that birth rank significantly affected ANC visits with decreased odds of birth rank among women who had four or more ANC visits [37]. A study conducted in regional Ethiopia found that birth interval was significantly higher among women who did not attend ANC [38]. The problem with distance to health facilities was related to limited ANC visits to southern India. This finding was consistent with research conducted in Nepal [32], Pakistan [33, 34] and Nigeria [25], which found that long distances to health facilities and access to ANC services were associated with No ANC visits.
Women who did not use a contraceptive and from socioeconomically disadvantaged groups reported higher odds of no ANC in all regions except the Southern regions. This is consistent with a community-based study conducted in Northeast Ethiopia which revealed that women from low socioeconomic status were less likely to use ANC [39], and a study that examined ways to improve the updated postpartum family planning in northern Tanzania found that counselling women during ANC did not improve contraceptive use [40].
Study limitation and strengths
Limitations of this study were due to the cross-sectional design, which does not allow causal association between the study factors and outcome variables. Also, as ANC components were self-reported by pregnant women, recall bias, misclassification, and measurement of factors associated with no or inadequate receipt of ANC components. However, the major strengths of this study are that it utilised the most recent DHS, which provides a population-based, nationally representative sample and covers large sample sizes with a 98% response rate. The study has good internal validity as the questionnaire was validated by trained health personnel.
This study highlights the factors associated with no or inadequate receipt of ANC components at the regional level, states and union territories in India. Poor households, knowledge about delivery complications and post-delivery complications were significant factors associated with increased odds of receiving no or inadequate quality ANC in India, and these associated factors vary across all six regions. Home delivery reported higher odds of no ANC or inadequate quality ANC in all six regions except the East region. Women who had no postnatal checkups after delivery, low mother education level and a big problem with paying for health services reported higher odds of no ANC or inadequate quality ANC in all the various regions in India To improve women’s access to ANC services across all regions in India, it is prudent to consider the factors mentioned above to monitor and improve the maternal health programme in India, including media campaigns for creating awareness about ANC services, especially among pregnant women from lower socioeconomic groups.
Availability of data and materials
The dataset analysed during the current study are available in the DHS Program repository, https://dhsprogram.com/.
Abbreviations
- ANC:
-
Antenatal care
- NDHS:
-
Nigeria Demographic and Health Survey
- WHO:
-
World Health Organization
- NFHS:
-
National Family Health Survey
- GBD:
-
Global Burden of Disease
- TT:
-
Tetanus Toxoid vaccination
- IFA:
-
Iron-folic acid
- SDGs:
-
Sustainable Development Goals
- LMIC:
-
Low and middle-income countries
- AOR:
-
Adjusted Odds ratio
- CI:
-
Confidence interval
References
Kassebaum NJ, Barber RM, Bhutta ZA, Dandona L, Gething PW, Hay SI, et al. Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1775–812.
World Health Organization. World health statistics 2010 2010. Available from: https://apps.who.int/iris/handle/10665/44292. cited 2021 2/12/2021
World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience 2016. Available from: https://www.who.int/publications/i/item/9789241549912. cited 2021 3/12/2021
World Health Organization. Women and health : today’s evidence tomorrow’s agenda 2009. Available from: https://apps.who.int/iris/handle/10665/44168. cited 2021 2/12/2021
World Health Organization. Maternal mortality 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality. cited 2021 2/12/2021
Coffey D. Costs and consequences of a cash transfer for hospital births in a rural district of Uttar Pradesh, India. Soc Sci Med. 2014;114:89–96.
Goudet S, Murira Z, Torlesse H, Hatchard J, Busch-Hallen J. Effectiveness of programme approaches to improve the coverage of maternal nutrition interventions in South Asia. Matern Child Nutr. 2018;14:e12699.
Wendt A, Stephenson R, Young M, Webb-Girard A, Hogue C, Ramakrishnan U, et al. Individual and facility-level determinants of iron and folic acid receipt and adequate consumption among pregnant women in rural Bihar, India. PLoS ONE. 2015;10(3):e0120404.
Saroha E, Altarac M, Sibley LM. Caste and maternal health care service use among rural Hindu women in Maitha, Uttar Pradesh, India. J Midwifery Womens Health. 2008;53(5):e41–7.
Pallikadavath S, Foss M, Stones RW. Antenatal care: provision and inequality in rural north India. Soc Sci Med. 2004;59(6):1147–58.
Rani M, Bonu S, Harvey S. Differentials in the quality of antenatal care in India. Int J Qual Health Care. 2008;20(1):62–71.
Kumar G, Choudhary TS, Srivastava A, Upadhyay RP, Taneja S, Bahl R, et al. Utilisation, equity and determinants of full antenatal care in India: analysis from the National Family Health Survey 4. BMC Pregnancy Childbirth. 2019;19(1):1–9.
Ogbo FA, Dhami MV, Ude EM, Senanayake P, Osuagwu UL, Awosemo AO, et al. Enablers and barriers to the utilization of antenatal care services in India. Int J Environ Res Public Health. 2019;16(17):3152.
Singh L, Dubey R, Singh S, Goel R, Nair S, Singh P. Measuring quality of antenatal care: a secondary analysis of national survey data from India. BJOG Int J ObstetGynaecol. 2019;126:7–13.
International Institute for Population Sciences (IIPS), ICF. National Family Health Survey (NFHS-5). Andhra Pradesh. Mumbai, India IIPS,2022 Available from: http://rchiips.org/nfhs/factsheet_NFHS-5.shtml 2022.
Kumar G, Choudhary TS, Srivastava A, Upadhyay RP, Taneja S, Bahl R, et al. Utilisation, equity and determinants of full antenatal care in India: analysis from the National Family Health Survey 4. BMC Pregnancy Childbirth. 2019;19(1):327. https://doi.org/10.1186/s12884-019-2473-6.
Agha S, Tappis H. The timing of antenatal care initiation and the content of care in Sindh. Pakistan BMC pregnancy and childbirth. 2016;16(1):1–9.
Agho KE, Ezeh OK, Ogbo FA, Enoma AI, Raynes-Greenow C. Factors associated with inadequate receipt of components and use of antenatal care services in Nigeria: a population-based study. Int Health. 2018;10(3):172–81.
Bruce SG, Blanchard AK, Gurav K, Roy A, Jayanna K, Mohan HL, et al. Preferences for infant delivery site among pregnant women and new mothers in Northern Karnataka. India BMC Pregnancy Childbirth. 2015;15(1):1–10.
Nguyen PH, Sanghvi T, Kim SS, Tran LM, Afsana K, Mahmud Z, et al. Factors influencing maternal nutrition practices in a large scale maternal, newborn and child health program in Bangladesh. PLoS ONE. 2017;12(7):e0179873.
Bantas K, Aryastuti N, Gayatri D. The relationship between antenatal care with childbirth complication in Indonesian’s mothers (data analysis of the Indonesia Demographic and Health Survey 2012). J Epidemiol Kesehat Indones. 2019;2(2).
Gogoi M, Unisa S, Prusty RK. Utilization of maternal health care services and reproductive health complications in Assam. India J Public Health. 2014;22(4):351–9.
Dhami MV, Ogbo FA, Diallo TM, Agho KE, Maternal G, Collaboration CHR. Regional analysis of associations between infant and young child feeding practices and Diarrhoea in Indian children. Int J Environ Res Public Health. 2020;17(13):4740.
Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995:1–10.
Iyengar SD, Iyengar K, Suhalka V, Agarwal K. Comparison of domiciliary and institutional delivery-care practices in rural Rajasthan, India. J Health Popul Nutr. 2009;27(2):303.
Gorain A, Barik A, Chowdhury A, Rai RK. Preference in place of delivery among rural Indian women. PLoS ONE. 2017;12(12):e0190117.
Patel R, Marbaniang SP, Srivastava S, Kumar P, Chauhan S. Why Women Choose to Delivery at Home in India: A Study of Prevalence, Factors, and Socio-Economic Inequality. 2021.
Das J, Hammer J. Are institutional births institutionalizing deaths 2014. Available from: https://www.worldbank.org/en/webarchives/archive?url=https%3A%2F%2Fweb.worldbank.org%2Farchive%2Fwebsite01605%2FWEB%2FARE_INST.HTM&mdk=384273014. cited 2021 3/12/2021
Dhawan D, Pinnamaneni R, Bekalu M, Viswanath K. Association between different types of mass media and antenatal care visits in India: a cross-sectional study from the National Family Health Survey (2015–2016). BMJ Open. 2020;10(12):e042839.
Paul P, Chouhan P. Socio-demographic factors influencing utilization of maternal health care services in India. Clin Epidemiol Global Health. 2020;8(3):666–70.
Simkhada B, Teijlingen ERv, Porter M, Simkhada P. Factors affecting the utilization of antenatal care in developing countries: systematic review of the literature. J Adv Nurs. 2008;61(3):244–60.
Joshi C, Torvaldsen S, Hodgson R, Hayen A. Factors associated with the use and quality of antenatal care in Nepal: a population-based study using the demographic and health survey data. BMC Pregnancy Childbirth. 2014;14(1):1–11.
Nisar YB, Dibley MJ, Mir AM. Factors associated with non-use of antenatal iron and folic acid supplements among Pakistani women: a cross sectional household survey. BMC Pregnancy Childbirth. 2014;14(1):1–12.
Noh J-W, Kim Y-M, Lee LJ, Akram N, Shahid F, Kwon YD, et al. Factors associated with the use of antenatal care in Sindh province, Pakistan: A population-based study. PloS one. 2019;14(4):e0213987.
Shahjahan M, Chowdhury HA, Akter J, Afroz A, Rahman MM, Hafez M. Factors associated with use of antenatal care services in a rural area of Bangladesh. South East Asia Journal of Public Health. 2012;2(2):61–6.
Dixit P, Khan J, Dwivedi LK, Gupta A. Dimensions of antenatal care service and the alacrity of mothers towards institutional delivery in South and South East Asia. PLoS ONE. 2017;12(7):e0181793.
Tessema ZT, Minyihun A. Utilization and determinants of antenatal care visits in east African countries: a multicountry analysis of demographic and health Surveys. Adv Public Health. 2021;2021.
Hailu D, Gulte T. Determinants of short Interbirth interval among reproductive age mothers in Arba Minch District. Ethiopia Int J Reprod Med. 2016;2016:6072437.
Shibre G, Mekonnen W. Socio-economic inequalities in ANC attendance among mothers who gave birth in the past 12 months in Debre Brehan town and surrounding rural areas, North East Ethiopia: a community-based survey. Reprod Health. 2019;16(1):1–14.
Keogh SC, Urassa M, Kumogola Y, Kalongoji S, Kimaro D, Zaba B. Postpartum contraception in northern Tanzania: patterns of use, relationship to antenatal intentions, and impact of antenatal counseling. Stud Fam Plann. 2015;46(4):405–22.
Acknowledgements
This study is part of the first author Master of Public Health dissertation with the School of Health Sciences at Western Sydney University, Australia. We are grateful to Measure DHS, ORC Macro, Calverton, MD, USA for providing the 2017 National Family Health Survey (HFHS- 4) data for this analysis.
The Global Maternal and Child Health Research Collaboration (GloMACH)
Nilu Nagdev1, Osita Ezeh Ezeh1, Daarwin Subramanee1, Kingsley E. Agho1,2,7, Osuagwu Levi Uchechukwu2, Kedir Yimam Ahmed2, Felix Akpojene Ogbo2,3,4, Mansi Vijaybhai Dhami2,5, Thierno Diallo6, Abukari Ibrahim Issaka8, Pramesh R. Ghimire9, Blessing Jaka Akombi-Inyang10, Pascal Ogeleka11, Tanvir Abir12, Rose Victor13, Deborah Charwe13, Abdon Gregory Rwabilimbo14
1School of Health Sciences, Western Sydney University, Campbelltown Campus, Locked Bag 1797, Penrith NSW 2571, Australia
2Translational Health Research Institute, School of Medicine, Western Sydney University, Campbelltown Campus, NSW 2560, Australia
3General Practice Unit, Prescot Specialist Medical Centre Makurdi, Benue State, Nigeria
4Barmera Medical Clinic [Lake Bonney Private Medical Clinic], 24 Hawdon Street, Barmera, SA 5345, Australia
5Belmont Hospital, 16 Croudace Bay Road, Belmont NSW 2280, Australia
6Humanitarian & Development Studies, School of Social Sciences, Western Sydney University, Locked Bag 1797, Penrith NSW 2751, Australia
7African Vision Research Institute (AVRI), University of KwaZulu-Natal, Westville Campus, Durban, 3629, South Africa
8School of Sciences, Western Sydney University, Campbelltown Campus, Locked Bag 1797, Penrith NSW 2751, Australia
9Southern New South Wales Local Health District, Queanbeyan, NSW 2620, Australia
10The University of New South Wales, Kensington, NSW 2033, Australia
11La Trobe University, Bundoora, VIC 3086, Australia
12Daffodil International University, Dhaka, Bangladesh
13Tanzania Food and Nutrition Centre, Dar-es-Salaam, Tanzania
14Chato District Council, Geita Region, Northwestern Tanzania
Pre-publication history
The pre-publication history for this paper can be accessed.
here: https://www.researchsquare.com/article/rs-1138036/latest.pdf
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Consortia
Contributions
NN and KEA were involved in the conception and design of this study. NN carried out the analysis and drafted the manuscript. KEA, FAO, MD, DL and TD gave advice on interpretation and revised and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research design, including the content of all the survey questionnaires of the NFHS-4, was reviewed by the United States Centers for Disease Control and Prevention (CDC) and approved by both the ICF Institutional Review Board and the IIPS Institutional Review Board. We obtained approval from Measure DHS to download and use the data for this study. All methods (use of data) were performed in compliance with the Declarations of Helsinki. The data used in our study, all identifier information removed, and no personal identity was compromised.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary Table 1. Definition and categorisation of potential variables used in the study.
Additional file 2: Table S1.
Factors associated with no ANC in North India states. Table S2. Factors associated with no ANC in South India states. Table S3. Factors associated with no ANC in East India states. Table S4. Factors associated with no ANC in West India states. Table S5. Factors associated with no ANC in Central India states. Table S6. Factors associated with no ANC in Northeast India states.
Additional file 3: Table S1.
Factors associated with inadequate ANC in North India states. Table S2. Factors associated with inadequate ANC in South Indian states. Table S3. Factors associated with inadequate ANC in East India states. Table S4. Factors associated with inadequate ANC in West Indiana states. Table S5. Factors associated with inadequate ANC in Central India states. Table S6. Factors associated with inadequate ANC in Northeast Indian states.
Additional file 4.
Prevalence of receipt of ANC by States and Union territories in India, 2019-21.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nagdev, N., Ogbo, F.A., Dhami, M.V. et al. Factors associated with inadequate receipt of components and non-use of antenatal care services in India: a regional analysis. BMC Public Health 23, 6 (2023). https://doi.org/10.1186/s12889-022-14812-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14812-3