
Abstract
Background
Pulmonary hypertension (PH) is a serious and life-threatening disease characterized by elevated mean arterial pressure and pulmonary vascular resistance. COVID-19 may exacerbate PH, as evidenced by higher mortality rates among those with PH. The objective of this study was to understand the unique burdens that the COVID-19 pandemic has placed upon families of children living with PH.
Methods
Participants were recruited online through the “Families of children with pulmonary hypertension” Facebook group and asked to complete a survey about their experiences during the COVID-19 pandemic.
Results
A total of 139 parents/caregivers of children living with PH completed the online survey. Almost all (85.6%) of parents/caregivers had received the COVID-19 vaccine, though only 59.7% reported a willingness to vaccinate their child with PH against COVID-19. Over 75% of parents/caregivers felt that they practiced preventative measures (e.g., wearing a facemask, social distancing, and avoiding gatherings) more than those in the community where they live. They also reported several hardships related to caring for their child with PH during the pandemic such as financial duress, loss of work, and affording treatment costs.
Conclusions
These findings indicate that parents/caregivers of children at higher risk for COVID-19 complications may be more willing to act on clinical recommendations themselves as proxy for protecting those at high risk. The economic, emotional and social impacts of COVID-19 are significantly greater for high-risk individuals.
Similar content being viewed by others

Background
Pulmonary hypertension (PH) is rare but a serious and potentially life-threatening disease characterized by an elevation in mean pulmonary artery pressure and pulmonary vascular resistance [1]. In severe cases, PH leads to right heart failure, clinical worsening, and death. PH is an important cause of morbidity and mortality in children, with an estimated annual incidence rate of approximately 3 cases per million children and is most commonly idiopathic or associated with congenital heart disease [2,3,4,5,6,7,8,9]. In children, untreated PH carries a grim prognosis, with subtypes such as idiopathic PH predicting a median survival of just 10 months [10]. PH has been reported in 23 to 37% of premature infants with chronic lung disease (CLD) in multiple retrospective studies, and carries a 2-year mortality rate as high as 48% [11,12,13,14]. In addition to substantial mortality risk, PH associated with chronic lung disease is associated with increased morbidity such as prolonged mechanical ventilation, need for supplemental oxygen, and increased hospital length of stay [11,12,13,14,15,16,17,18]. PH has primarily been characterized and studied among adults and therefore the development of treatment therapies has also targeted this population. Studies evaluating therapeutic dosing, side effects, and outcome for pediatric patients are lacking, however children are benefitting from therapies used to treat adults [19].
Since the onset of the coronavirus disease-19 (COVID-19) pandemic, millions of people have been infected with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and millions have lost their lives as a result [20, 21]. Though COVID-19 incidence among those with PH appears to be similar to infection among the general population, the mortality rates for those with PH are significantly higher [22]. Children living with PH are thought to be particularly vulnerable to SAR-CoV-2 as it predominantly affects the respiratory tract, causing endothelial dysfunction, hypoxia and vasoconstriction. This further compromises the cardiopulmonary system, one that is already vulnerable due to the underlying pulmonary vascular disease [23]. A survey of 77 PH Comprehensive Care Centers estimated the incidence of COVID-19 in adults with PH to be 2.1 cases per 1000 people, though there is little data on the incidence of COVID-19 among children living with PH [24]. This is particularly concerning given the easy spread and communicability of SARS-CoV-2 [25]. Parents and caregivers of children living with PH have carried an even greater burden during this pandemic, as they not only administer detailed PH care plans, but also shoulder the responsibility of preventing SARS-CoV-2 infection in these children. In one retrospective cohort study of pediatric PH patients diagnosed with COVID-19, 35% required hospitalization due to clinical worsening or acute respiratory failure [26]. However, none of these patients required intubation. Though these patients showed excellent short-term recovery from COVID-19, the long-term consequences of long COVID on children living with PH [27] remain unknown, especially for this high-risk population of children living with PH [26].
The COVID-19 pandemic has negatively influenced infants and newborns with chronic conditions (such as PH) and their parents/caregivers, especially when clinics were temporarily closed during the pandemic leaving parents/caregivers with only telehealth/telemedicine visits to monitor their child’s condition(s) [23, 28]. Before the COVID-19 pandemic, approximately 10% of PH centers in the U.S. offered telemedicine visits, while 97% of PH centers offer virtual visits currently [23]. Since standard pediatric PH clinic visits include routine monitoring of vital signs, echocardiograms, stress tests, and laboratory evaluation, virtual appointments frequently do not meet the full needs of these patients. Thus, the crucial evaluation of the cardiopulmonary system and treatment therapy effectiveness were nonexistent, delayed or moved to irregular intervals as the healthcare system was inundated with changing guidelines, policies and recommendations to prevent the spread of COVID-19.
The goal of the current study was to understand the unique burdens that the COVID-19 pandemic has placed upon parents/caregivers of children living with PH. The focus of the study was to better understand the experiences of parents/caregivers accessing care, undertaking preventative practices against SARS-CoV-2 infection, beliefs towards COVID-19 vaccination, and disruptions such as education, doctor availability, prescription dispensing that impacted their ability to care for their child living with PH.
Methods
Facebook recruitment campaign
Participants were recruited online via Facebook™ invitations posted on the “Families of children with pulmonary hypertension” Facebook page. A random sample of group members (n = 934) also received a personal invitation via the internal Facebook messaging system (Facebook Messenger). To maximize study participation and to provide each group member an opportunity to participate, we posted the invitation on the Facebook group homepage 3 times over a 5-week period during December 2021 to January 2022. Participants who clicked on the invitation link were redirected to a secure study website and provided with study information, asked to convey consent to participate, and then immediately prompted to begin the survey using the Qualtrics™ survey platform. Eligible individuals who completed the survey were compensated for their participation and emailed a $20 gift card to Amazon.com®. The study protocol was approved by the Institutional Review Board at Brigham Young University (#IRB2021–371).
Study participants
Parents and caregivers of children living with PH were surveyed about their personal experiences, as well as those of their child living with PH. Participants were English-speaking, aged 18 years or older, members of the “Families of children with pulmonary hypertension” Facebook group, and self-identified as parents, guardians or primary caregivers of a child living with PH. This Facebook group was selected because it is the largest known gathering place for parents of children living with PH (with approximately 1500 group members), many of whom routinely (daily) interact with others to learn more about existing PH therapies, to cope, and to share experiences of caring for a child with PH.
Survey instrument
We developed a questionnaire containing questions intended to be answered by the parent of a child living with PH. The survey assessed participants’ knowledge, attitudes, perceptions, and burdens related to COVID-19 and caring for a child living with PH. Survey questions related to COVID-19 threat appraisal, vulnerability and anxiety were adapted from published studies for our study population [23, 29,30,31]. Sample survey items included “In your opinion, how effective are the following actions for keeping you safe from COVID-19”; “How often do you engage in the following practices to prevent COVID-19”; “Were you vaccinated against COVID-19”; “Will you vaccinate (or have you already vaccinated) your child who has PH against COVID-19”; and “How much do you trust the following sources to provide accurate COVID-19 information.” The majority of questions were assessed on a 5-point Likert scale ranging from 1 (strongly disagree/never) to 5 (strongly agree/always). In addition, we assessed specific familial hardships due to the COVID-19 pandemic including job loss (yes/no), loss of financial stability (yes/no), financial aid receipt to offset PH therapy costs (yes/no), and difficulty covering PH treatment costs (yes/no). Finally, we queried family sociodemographics including race (white/other), relationship to child living with PH (father, mother, guardian, primary caregiver), U.S. citizenship (yes/no), respondents’ educational attainment (high school, some college, associate’s degree, bachelor’s degree, graduate or professional degree), employment status (employed, homemaker, unemployed), household income (<$35,000, $35,000-74,999, >$75,000), health insurance status (yes/no). The average survey completion time was 19.5 minutes (range: 8 to 56 minutes).
Statistical analysis
We calculated the frequency of actions undertaken by parents/caregivers and their child living with PH to prevent SARS-CoV-2 infection, reasons for not taking actions to prevent SARS-CoV-2 infection, attitudes and perceptions regarding COVID-19 vaccination for themselves and their child living with PH, sources from which parents/caregivers would seek COVID-19-related news and information, and financial, medical, and other impacts (i.e., job or insurance loss) imposed by the COVID-19 pandemic. We report the counts and frequencies (percentages) of each of the aforementioned actions. Statistical analysis was conducted in R version 4.1.0 [32].
Results
Characteristics of the 139 parents/caregivers of children living with PH who responded to the online survey are presented in Table 1. The majority of respondents self-identified as White/Caucasian (82.0%), were mothers of the child living with PH (89.2%), had advanced educational attainment (60.5% had a college degree or higher), were U.S. residents (85.6%) and had health insurance (94.2%). Almost all parents/caregivers had received the COVID-19 vaccine (85.6%), though only 59.7% reported a willingness to vaccinate their child with PH against COVID-19. This was consistent with parent/caregivers’ attitude towards vaccinating other children in their home (57.6%). The primary reasons reported for not vaccinating their children against COVID-19 were the desire for more scientific evidence (39.5%), concerns about the safety of the vaccine (11.8%), and lack of trust in the expedited COVID-19 vaccine approval process (11.8%) (see Table 2).
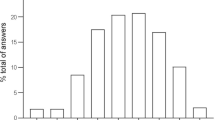
Parents/caregivers engaged in a variety of preventative practices to prevent infection with SARS-CoV-2 (see Fig. 1). For example, parents/caregivers reported that they were engaging in the following behaviors always or most of the time: avoiding international travel (89.5%), practicing social distancing where possible (81.1%), avoiding crowded places (77.6%), wearing a facemask at social events (77.0%), and avoiding physical contact and touching others (75.3%). Over 75% of parents/caregivers felt that they practiced preventative measures such as wearing a facemask, social distancing, and avoiding gatherings and events more than those in the community did where they live. Parent/caregivers were also more likely to express trust in healthcare providers (84%) and official government sources [World Health Organization (58%), the Centers for Disease Control and Prevention (61%), and government-sponsored websites (50%)] than social media (0–6%), peers (11%), or local news stations (0–17%) to receive accurate information about the COVID-19 pandemic (see Fig. 2).

Practices of parents/caregivers of children living with pulmonary hypertension to prevent COVID-19 (n = 139)

Trust of various sources for COVID-19 information reported by parents/caregivers of children living with pulmonary hypertension (n = 139)
Parents/caregivers reported several financial hardships related to caring for their child with PH during the COVID-19 pandemic (see Table 3). For example, 41.0% of parents/caregivers reported financial duress and instability during the COVID-19 pandemic, 21.0% of parents/caregivers reported having lost their job during the COVID-19 pandemic, and 8.6% reported having difficultly covering the treatment costs for their child with PH. In addition, 71.9% of parents/caregivers thought their child’s education quality had decreased due to the COVID-19 pandemic, though the manner in which children with PH received their education (e.g., in-person schooling or virtual schooling) changed in less than half (41%) of the sample.
Discussion
We sought to understand the unique burdens of the COVID-19 pandemic and preventative practices against SARS-CoV-2 infection undertaken by parents/caregivers of children living with PH using a convenience sample from an online Facebook group. We found that 85.6% of parents/caregivers of children living with PH had received the COVID-19 vaccination, which is significantly higher than the 62.8% of vaccinated individuals in United States during the same period (January 1, 2022) [33]. This finding is consistent with vaccination rates among other high-risk populations such as adults ≥65 years (80.0%) [34], dialysis patients (74.1%), and pregnant women (66.8%) on January 1, 2022 [33]. Of note, this study concluded before the surge in COVID-19 cases and subsequent vaccinations that occurred in response to the highly contagious Omicron variant in early 2022 [33, 35]. We also found that 59.7% of parents/caregivers of children living with PH were willing to vaccinate their children against COVID-19. Importantly, 41.8% of children with PH in our study sample were less than 5 years old and were not yet eligible for the vaccine at the time of the study. It is worth noting that the COVID-19 vaccination has been shown to be safe and efficacious among children since the conclusion of our study [36, 37]. However, the willingness of parents to vaccinate their children with PH was much higher than that reported vaccination rate among children in the United States (28.1%) at the time of the survey [38, 39], yet far below the parental vaccine intention attitudes (86.7% of parents reported they would definitely or probably vaccinate their children) that have been suggested elsewhere [40]. These findings indicate that parents/caregivers of children at higher risk may be more willing to act on clinical recommendations themselves as proxy for protecting their children than parents of children who do not have elevated risk from SARS-CoV-2 infection despite initial straw polls of parental attitudes towards COVID-19 vaccination.
Parents/caregivers of children living with PH were also engaged in several recommended prevention practices and at higher rates than most adults in the U.S. [41, 42]. In lieu of vaccination, these practices have been the most effective evidence-based practices to reduce the transmission of COVID-19 [43, 44]. Importantly, parents/caregivers were surveyed approximately 21 months into the pandemic, yet they reported maintaining these practices despite the fatigue, letdown and abandonment of these practices by many adults. This may be partially explained by the perceived elevated risk and/or fear of serious complications if the child with PH were to become infected with SARS-CoV-2. The longevity of practicing these behaviors has been directly linked to depression and poorer mental health outcomes [45, 46], which may be exacerbated by the financial, temporal, and emotional tolls of caring for a child with PH as has been observed in other studies [47,48,49].
The large majority (71.9%) of parents/caregivers of children living with PH reported that the quality of their child’s education has decreased due to the COVID-19 pandemic. This educational deficit is not unique to children living with PH, though this may further isolate children with PH as they are at greater risk of serious complications from SARS-CoV-2 infection. For example, since many children with PH are not able to participate in common childhood activities (i.e., running, many contact sports, riding a bike) and now must maintain social distance, they may experience disproportionate social development and educational setbacks [50]. Apart from educational impacts, parents/caregivers also reported hardships such as job loss, difficulty covering PH medications and therapies, and overall financial instability. Again, these impacts of the COVID-19 pandemic are not unique to families of children with PH, but they do highlight the extra burden shouldered by caring for a child with a chronic health condition [28, 51].
This study has some limitations. First, parents/caregivers were recruited from an online Facebook group and are a convenience sample (i.e., not representative) of all parents/caregivers of children living with PH. However, this is also a strength as this is the largest group worldwide of individuals with children living with PH. Second, survey responses were self-reported by parents/caregivers over the Internet and may be subject to under or overreporting. However, other Internet-based studies have shown increased self-disclosure and reporting with online surveys, which may reduce potential response biases (e.g., interviewer bias or social desirability) [52, 53]. Finally, the cross-sectional study design does not permit causal inference.
This study enhances our understanding of how parents/caregivers of children living with PH have responded to the COVID-19 pandemic, including preventative practices and vaccination uptake. The results demonstrate how parents/caregivers may respond differently to COVID-19 recommendations and practices in order to protect high-risk individuals under their care and supervision. Learning about the experience of these individuals living through the COVID-19 crisis can help empower public health and healthcare professionals to continue to protect the health of this population.
Availability of data and materials
We are not allowed to post the data to a repository (even de-identified) due to HIPAA concerns (potential to identify subjects). Data and materials available upon request to the corresponding author.
References
Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet. 1998;352(9129):719–25.
Berger RM, Beghetti M, Humpl T, Raskob GE, Ivy DD, Jing ZC, et al. Clinical features of paediatric pulmonary hypertension: a registry study. Lancet. 2012;379(9815):537–46.
van Loon RL, Roofthooft MT, Hillege HL, ten Harkel AD, van Osch-Gevers M, Delhaas T, et al. Pediatric pulmonary hypertension in the Netherlands: epidemiology and characterization during the period 1991 to 2005. Circulation. 2011;124(16):1755–64.
Escribano-Subias P, Blanco I, Lopez-Meseguer M, Lopez-Guarch CJ, Roman A, Morales P, et al. Survival in pulmonary hypertension in Spain: insights from the Spanish registry. Eur Respir J. 2012;40(3):596–603.
Frost AE, Badesch DB, Barst RJ, Benza RL, Elliott CG, Farber HW, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US contemporary registries. Chest. 2011;139(1):128–37.
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023–30.
Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30(1):104–9.
Jansa P, Jarkovsky J, Al-Hiti H, Popelova J, Ambroz D, Zatocil T, et al. Epidemiology and long-term survival of pulmonary arterial hypertension in the Czech Republic: a retrospective analysis of a nationwide registry. BMC Pulm Med. 2014;14:45.
Ling Y, Johnson MK, Kiely DG, Condliffe R, Elliot CA, Gibbs JS, et al. Changing demographics, epidemiology, and survival of incident pulmonary arterial hypertension: results from the pulmonary hypertension registry of the United Kingdom and Ireland. Am J Respir Crit Care Med. 2012;186(8):790–6.
D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115(5):343–9.
Ali Z, Schmidt P, Dodd J, Jeppesen DL. Predictors of bronchopulmonary dysplasia and pulmonary hypertension in newborn children. Dan Med J. 2013;60(8):A4688.
An HS, Bae EJ, Kim GB, Kwon BS, Beak JS, Kim EK, et al. Pulmonary hypertension in preterm infants with bronchopulmonary dysplasia. Korean Circ J. 2010;40(3):131–6.
Slaughter JL, Pakrashi T, Jones DE, South AP, Shah TA. Echocardiographic detection of pulmonary hypertension in extremely low birth weight infants with bronchopulmonary dysplasia requiring prolonged positive pressure ventilation. J Perinatol. 2011;31(10):635–40.
Khemani E, McElhinney DB, Rhein L, Andrade O, Lacro RV, Thomas KC, et al. Pulmonary artery hypertension in formerly premature infants with bronchopulmonary dysplasia: clinical features and outcomes in the surfactant era. Pediatrics. 2007;120(6):1260–9.
Bhat R, Salas AA, Foster C, Carlo WA, Ambalavanan N. Prospective analysis of pulmonary hypertension in extremely low birth weight infants. Pediatrics. 2012;129(3):e682–9.
Check J, Gotteiner N, Liu X, Su E, Porta N, Steinhorn R, et al. Fetal growth restriction and pulmonary hypertension in premature infants with bronchopulmonary dysplasia. J Perinatol. 2013;33(7):553–7.
Kim GB. Pulmonary hypertension in infants with bronchopulmonary dysplasia. Korean J Pediatr. 2010;53(6):688–93.
Stuart BD, Sekar P, Coulson JD, Choi SE, McGrath-Morrow SA, Collaco JM. Health-care utilization and respiratory morbidities in preterm infants with pulmonary hypertension. J Perinatol. 2013;33(7):543–7.
Barst RJ, McGoon MD, Elliott CG, Foreman AJ, Miller DP, Ivy DD. Survival in childhood pulmonary arterial hypertension: insights from the registry to evaluate early and long-term pulmonary arterial hypertension disease management. Circulation. 2012;125(1):113–22.
Johns Hopkins University of Medicine. COVID-19 Dashboard [Available from: https://coronavirus.jhu.edu/map.html.
Higgins V, Sohaei D, Diamandis EP, Prassas I. COVID-19: from an acute to chronic disease? Potential long-term health consequences. Crit Rev Clin Lab Sci. 2021;58(5):297–310.
Ryan JJ. The impact of COVID-19 on pulmonary hypertension2020 September 28, 2021. Available from: https://www.acc.org/latest-in-cardiology/articles/2020/08/13/08/35/the-impact-of-covid-19-on-pulmonary-hypertension.
Das BB. COVID-19 and pulmonary hypertension in children: what do we know so far? Medicina (Kaunas). 2020;56(12).
Farha S, Heresi GA. COVID-19 and pulmonary arterial hypertension: early data and many questions. Ann Am Thorac Soc. 2020;17(12):1528–30.
Sy KTL, White LF, Nichols BE. Population density and basic reproductive number of COVID-19 across United States counties. PLoS One. 2021;16(4):e0249271.
Morales-Demori R, Mallory GB, Chartan C, Coleman R, Ruiz F, Villafranco N, et al. Outcomes of COVID-19 infection in pediatric pulmonary hypertension: a single-center experience. Pediatr Pulmonol. 2021;56(12):3960–5.
Nabavi N. Long covid: how to define it and how to manage it. BMJ. 2020;370:m3489.
Brindisi G, Di Marino VP, Olivero F, De Canditiis D, De Castro G, Zicari AM, et al. Effects of COVID-19 lockdown on weight in a cohort of allergic children and adolescents. Ital J Pediatr. 2022;48(1):88.
Kwiatkowska J, Meyer-Szary J, Mazurek-Kula A, Zuk M, Migdal A, Kusa J, et al. The Impact of COVID-19 Pandemic on Children with Pulmonary Arterial Hypertension. Parental Anxiety and Attitudes. Follow-Up Data from the Polish Registry of Pulmonary Hypertension (BNP-PL). J Clin Med. 2021;10(8):1640.
Zhou H, Zhang G, Deng X, Jin B, Qiu Q, Yan M, et al. Understanding the current status of patients with pulmonary hypertension during COVID-19 outbreak: a small-scale national survey from China. Pulm Circ. 2020;10(2):2045894020924566.
Hanson CL, Crandall A, Barnes MD, Novilla ML. Protection motivation during COVID-19: a cross-sectional study of family health, media, and economic influences. Health Educ Behav. 2021;48(4):434–45.
R: a language and environment for statistical computing, Vienna, Austria : R Foundation for Statistical Computing; 2022.
Centers for Disease Control and Prevention. COVID Data Tracker 2022 [Available from: https://covid.cdc.gov/covid-data-tracker/#vaccination-trends_vacctrends-fully-cum.
Diesel J, Sterrett N, Dasgupta S, Kriss JL, Barry V, Vanden Esschert K, et al. COVID-19 vaccination coverage among adults - United States, December 14, 2020-may 22, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(25):922–7.
Centers for Disease Control and Prevention. Omicron Variant: What You Need to Know: Centers for Disease Control and Prevention, 2022. [Available from: https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron-variant.html.
Capponi M, Pulvirenti F, Cinicola BL, Brindisi G, Conti MG, Colaiocco G, et al. Short-term side effects and SARS-CoV-2 infection after COVID-19 Pfizer-BioNTech vaccine in children aged 5-11 years: An Italian real-world study. Vaccines (Basel). 2022;10(7).
Hause AM, Baggs J, Marquez P, Myers TR, Gee J, Su JR, et al. COVID-19 vaccine safety in children aged 5-11 years - United States, November 3-December 19, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(5152):1755–60.
Kaiser Family Foundation. Vaccinations Among Children 2022 [Available from: https://www.kff.org/coronavirus-covid-19/issue-brief/latest-data-on-covid-19-vaccinations-by-race-ethnicity/#:~:text=of%20early%202022.-,Vaccinations%20Among%20Children,-As%20of%20this.
Kates J, Tolbert J, Rouw A. Update on COVID-19 Vaccination of 5–11 Year Olds in the U.S.: Kaiser Family Foundation, 2022 [Available from: https://www.kff.org/coronavirus-covid-19/issue-brief/update-on-covid-19-vaccination-of-5-11-year-olds-in-the-u-s/.
Johns Hopkins center for communication programs. Who plans to vaccinate their children? A CCP dashboard offers clues: Johns Hopkins Bloomberg School of Public Health; 2021. [Available from: https://ccp.jhu.edu/2021/11/22/dashboard-covid-behaviors-vaccination-children/
Coroiu A, Moran C, Campbell T, Geller AC. Barriers and facilitators of adherence to social distancing recommendations during COVID-19 among a large international sample of adults. PLoS One. 2020;15(10):e0239795.
Wolff W, Martarelli CS, Schüler J, Bieleke M. High boredom proneness and low trait self-control impair adherence to social distancing guidelines during the COVID-19 pandemic. Int J Environ Res Public Health. 2020;17(15):5420.
Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–87.
Talic S, Shah S, Wild H, Gasevic D, Maharaj A, Ademi Z, et al. Effectiveness of public health measures in reducing the incidence of covid-19, SARS-CoV-2 transmission, and covid-19 mortality: systematic review and meta-analysis. Bmj. 2021;375:e068302.
Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. 2017;152:157–71.
Williams CYK, Townson AT, Kapur M, Ferreira AF, Nunn R, Galante J, et al. Interventions to reduce social isolation and loneliness during COVID-19 physical distancing measures: a rapid systematic review. PLoS One. 2021;16(2):e0247139.
Abrams HR, Leeds HS, Russell HV, Hellsten MB. Factors influencing family burden in pediatric hematology/oncology encounters. J Patient Cent Res Rev. 2019;6(4):243–51.
Bucak IH, Tumgor G, Almis H, Kose S, Dogan CN, Turgut M. Evaluation of burden and anxiety in caregivers of patients with pediatric celiac disease in the COVID-19 pandemic. Avicenna J Med. 2021;11(3):152–5.
Akkuş Y, Karacan Y, Ünlü K, Deniz M, Parlak A. The effect of anxiety and spiritual well-being on the care burden of caregivers of cancer patients during the COVID-19 pandemic. Support Care Cancer. 2022;30(2):1863–72.
U.S. Department of Education. Education in a Pandemic: The Disparate Impacts of COVID-19 on America's Students. In: Education USDo, editor. 2021.
Brindisi G, De Vittori V, De Castro G, Duse M, Zicari AM. Pills to think about in allergic rhinitis children during COVID-19 era. Acta Paediatr. 2020;109(10):2149–50.
Cantrell MA, Lupinacci P. Methodological issues in online data collection. J Adv Nurs. 2007;60(5):544–9.
Rhodes SD, Bowie DA, Hergenrather KC. Collecting behavioural data using the world wide web: considerations for researchers. J Epidemiol Community Health. 2003;57(1):68–73.
Acknowledgements
Not applicable.
Funding
Mary Lou and Ira Fulton Grant, Brigham Young University.
Author information
Authors and Affiliations
Contributions
All authors have made important and meaningful contributions to this study. MJ and EJN conceived and designed the study. EJN, EC and MJ collected the data. EJN, EC, and MP conducted the statistical analyses. All authors assisted in the preparation, review and approval of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board at Brigham Young University (#IRB2021–371) and all methods were performed in accordance with the relevant guidelines and regulations. Participants were informed about the aim of the study and the voluntariness of their participation in and withdrawal from the study, and then, they were asked to provide informed consent for participation. Consent was provided digitally by participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nelson, E.J., Cook, E., Pierce, M. et al. Preventative practices and effects of the COVID-19 pandemic on caregivers of children with pediatric pulmonary hypertension. BMC Public Health 22, 2305 (2022). https://doi.org/10.1186/s12889-022-14651-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14651-2