
Abstract
Background
Type 2 diabetes mellitus is an expanding global public health issue, especially in developing countries. This study aimed to investigate the prevalence, awareness and control rate of type 2 diabetes mellitus, and assess its risk factors in elderly Chinese individuals.
Methods
The health screening data of 376,702 individuals aged ≥ 65 years in Wuhan, China, were collected to analyse the prevalence, awareness, and control rates of diabetes. Indices, including fasting plasma glucose and other biochemical indicators, were measured for all participants using standard methods at the central laboratory. Multilevel logistic regression analysis was performed to assess the key determinants of the prevalence, awareness, and control rates of diabetes.
Results
The prevalence, awareness, and control rates of diabetes in the Chinese individuals aged ≥ 65 years were 18.80%, 77.14%, and 41.33%, respectively. There were statistically significant differences in the prevalence, awareness, and control rates by gender. Factors associated with diabetes prevalence were age, body mass index (BMI), and central obesity; while those associated with awareness and control were gender, education level, marital status, physical activity, alcohol consumption, BMI, and central obesity.
Conclusions
Diabetes is an important public health problem in the elderly in China. The awareness and control rates have improved, but overall remained poor. Therefore, effective measures to raise awareness and control the rates of diabetes should be undertaken to circumvent the growing disease burden in elderly Chinese people.
Similar content being viewed by others

Background
With a rapid economic development, dramatic changes in lifestyles, and an aging population, type 2 diabetes mellitus (T2DM) has become a leading public health problem globally, especially in developing countries [1,2,3]. According to the latest International Diabetes Federation (IDF), the global prevalence of T2DM in adults was 536.6 million people (10.5%) in 2021, and that there would be 783.2 million people (12.2%) living with diabetes worldwide by 2045 [4]. China, the largest developing country worldwide, contributes to one-fifth of the global population [5], and has shown increased prevalence of diabetes in recent years. A study by Yang et al. in 2007 identified that the prevalence rate of diabetes was 9.7% in 46,239 residents from 14 provinces in China [6]. The latest research data suggests 11% prevalence rate of diabetes in adults in China [7]. Taken together, the prevalence of diabetes is extremely high in China.
The number of individuals aged ≥ 65 years has approached 200 million in China. The results of several epidemiological surveys on prevalence of diabetes in the elderly population show that the individuals aged ≥ 65 years have a higher risk of diabetes than those in other age groups [1], and the incidence of diabetes in the elderly is increasing [8]. Therefore, it is crucial to assess epidemiological characteristics and risk factors of diabetes, and implement selective interventions and management for specific populations.
Studies suggest that severe diabetes can be alleviated with proper management and education [9,10,11]. The IDF recommends that the target for glycaemic control in patients with diabetes is fasting plasma glucose (FPG) < 7.0 mmol/L or glycosylated haemoglobin (HbA1c) < 7% [12]. However, a previous study showed that Chinese patients with diabetes have a poor blood glucose control, and only 26%–40% of patients with diabetes achieve the target [13]. A meta-analysis in mainland China indicated a mere 20.87% diabetes control rate [14]. Poor diabetes control rates impose a significant financial burden on individuals, families, healthcare systems, and countries. A study suggested that approximately $110 billion (12% of total health expenditure) was spent on the treatment and management of patients with diabetes in China in 2015 [15]. Thus, it is imperative to identify factors that affect blood glucose control to prevent and delay diabetes.
Several studies have investigated the prevalence, awareness, and control rates of diabetes in China [8, 16,17,18]. However, information on diabetes in large populations is scarce, and only few studies have assessed older adults facing a higher risk of developing diabetes. Therefore, this study aimed to assess the latest epidemiological characteristics of diabetes in Chinese individuals aged ≥ 65 years, including the prevalence and related risk factors, and to evaluate their understanding of diabetes and glycaemic control levels.
Methods
Study design and participants
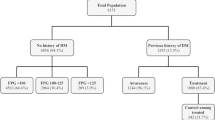
This was a population-based, cross-sectional study in individuals aged ≥ 65 years in Wuhan, China. Wuhan had 1,278,902 elderly individuals in 2018 [19]. With a scheme launched by the Wuhan Municipal Government, the Wuhan Center for Disease Control and Prevention conducted health screening of 388,403 (30.37%) elderly individuals from 11 urban districts and 6 suburban districts between January 2018 and December 2018. All participants volunteered and signed informed consent forms. The inclusion criteria were that the participants were elderly individuals aged ≥ 65 years and who were permanent residents of Wuhan. After excluding 11,701 individuals with incomplete or missing data, 376,702 participants (96.99%) finally completed the entire study.
The study was reviewed and approved by the Ethics Committee of the Wuhan Center for Disease Control and Prevention (IRB#: WHCDCIRB-K-2018023). Written informed consent was obtained from all participants prior to the data collection.
Data collection
The survey was conducted at local community health service centers in Wuhan, China. Each participant completed a health status questionnaire, and underwent body measurements and blood biochemical tests. Data were collected by trained medical staff at elementary healthcare centers.
A health status questionnaire was used to collect demographic information, including age (in years), gender (men, women), education level (elementary school and below, junior high school, technical secondary school or high school, and junior college or above), marital status (married, divorced, widowed, or single), history of diabetes (yes or no), physical activity (never, occasionally, sometimes, often, or always), smoking status (never, occasionally, often, or quit smoking), and drinking habit (never, occasionally, often, every day, or quit drinking).
Body measurements were obtained using standardised protocols. Participants’ height was measured in meters without shoes, and weight was measured in kilograms after removing heavy clothes. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2). Waist circumference (WC) was measured by placing the measuring tape over the navel and horizontally circling the waist. Blood pressure (BP) was measured by a registered nurse in a seated position using a standard mercury sphygmomanometer or automatic manometer.
Blood samples were collected from all participants after an overnight fast of at least 10 h. All blood samples were analysed at the central laboratory, which successfully completed a standardisation and certification program. Fasting plasma glucose (FPG) levels were measured using the glucose oxidase procedure.
Definitions
In this study, the diagnosis of T2DM was identified based on the Health Screening data. If one of the following three criterion was met, the subjects were regarded as T2DM: (1) FPG ≥ 7 mmol/L, (2) 2-h post-load plasma glucose ≥ 11.1 mmol/L, (3) self-reported previous diagnosis by healthcare professionals. The data were checked carefully by professionals to verify accuracy and completeness [20]. Awareness was defined as the proportion of individuals who reported a history of physician-diagnosed diabetes [15]. Control was defined as the proportion of patients with diabetes with FPG < 7.0 mmol/L, which indicated that self-reported history of diagnosed diabetes patients with FPG < 7.0 mmol/L at this physical examination were considered to have glucose control. Overweight was defined as BMI between 24.0 and 27.9, and obesity was defined as BMI ≥ 28.0. Central obesity was defined as a WC ≥ 85 cm for women and 90 cm for men according to the Healthy Adult Weight Determination in China (WS/T428–2013) [21].
Statistical analysis
Data were double entered in Epi Data 3.2 after manual checking. Double entry was used to minimise data entry errors. Participant characteristics are described as mean ± standard deviation for continuous variables and number (percentage) for categorical variables. The associated risk factors for the prevalence, awareness, and control of T2DM were analysed using multivariate logistic regression. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A P < 0.05 was considered to be statistically significant. All statistical analyses were performed using SAS version 9.4.
Results
General characteristics of participants
The socio-demographic characteristics of individuals aged ≥ 65 years in Wuhan are shown in Table 1(Additional File 1). A total of 376,702 individuals were investigated in the study, of which 167,886 (44.6%) were men and 208,816 (55.4%) were women. The average age of participants in the T2DM group tended to be higher than that of participants in non-T2DM group. BMI, systolic blood pressure (SBP), WC, and FPG levels were higher in participants in the T2DM group than those in non-T2DM group. However, participants in the non-T2DM group had a higher diastolic BP (DBP) than those in T2DM group. The differences between T2DM group and non-T2DM group were statistically significant. A majority of the participants had low education levels. A majority of the participants were married, and never smoked or consumed alcohol.
Prevalence, awareness, and control rates in different subgroups
The overall prevalence of T2DM in the Chinese individuals aged ≥ 65 years was 18.80% (Table 2, Additional File 2). There was a statistically significant difference in the prevalence of diabetes between men and women (χ2 = 208.414, P < 0.001). Of the individuals with T2DM, 77.14% were aware that they had diabetes, and 41.33% of them had their blood glucose levels under control. There were also statistically significant differences in terms of awareness and control rate by gender (χ2 = 379.454, P < 0.001; and χ2 = 95.683, P < 0.001, respectively). The results showed that individuals with a higher BMI and central obesity had a higher prevalence of T2DM than other individuals. The awareness and control rate for T2DM increased with age and education level, and was particularly high in individuals who exercised regularly. Moreover, individuals who quit smoking and drinking had the highest awareness and control rates, as opposed to those in other groups.
Analyses of risk factors for the prevalence, awareness, and control of T2DM
In the multivariate analysis, older age, higher education level, physical activity, history of higher BMI, and central obesity were risk factors for the prevalence of T2DM, while smoking and drinking were negatively related to the prevalence rate (Table 3, Additional File 3). The education level, physical activity, quite smoking, quite drinking, history of central obesity, and history of high BMI were positively related to the awareness rate. In contrast, single marital status and current drinking were negatively related to the awareness rate. Further, older age, higher education level, physical activity, quite smoking and quite drinking were positively related to the control rate; while single marital status, current drinking, history of higher BMI, and central obesity were negatively related to the control rate. Additionally, women gender showed positive correlation with awareness and control rates.
Discussion
This study investigated the prevalence, awareness, and control rates of diabetes in a large population in Wuhan, China. We found that 18.80% of the elderly residents had T2DM. In addition, 77.14% of the participants were aware that they had diabetes, and 41.33% of them had diabetes under control. These findings reveal that T2DM has been a major public health issue in China, and thus, suggests that more measures to control T2DM are needed.
The key observation from these new data was that the prevalence rates in individuals ≥ 65 in China was relatively higher than in some regional surveys in China reported in recent years (18.8% vs.16.9%) [22], and almost equaled the US population (20.4%) [23], despite the fact that overweight and obesity are far more prevalent in the United States. Basing on the fact that due to China's critical diabetes situation, T2DM is for certain to impose tremendous health care costs on elderly adults with diabetes [24], it is important to improve the awareness and control rates of diabetes in patients. In the present study, 77.14% of the participants were aware that they had diabetes, and 41.33% had controlled diabetes. According to previous studies in other regions in China, the awareness rate of diabetes was < 60%, and the control rate was approximately 30% [25, 26]. However, in some European nations and the US, which have relatively higher medical facilities, the national awareness and control rates of diabetes exceeded 70% and 50%, respectively [23, 27]. These data indicate that the awareness and control rates of diabetes in China have improved than those in the past, and diabetes health education programs have progressed. However, compared with rates in the developed countries, China would need more aggressive diabetes prevention and control.
The results of the present study showed that the prevalence of T2DM was higher in women than in men, which is consistent with results of other studies conducted in Asia [28,29,30]. Previous studies have suggested that the difference could be attributed to variability in risk factors for diabetes prevalence between men and women, or to women's longer life expectancy [31]. Women also had higher rates of diabetes awareness and control than men in the present study. This may be attributed to the fact that women use medical services more, have a higher awareness of social security, and have easier access to health services than men [32]. In addition, due to the higher prevalence of diabetes in women, those with diabetes may pay more attention to the disease, and thus, have higher awareness and control rates than men.
The present study revealed that older individuals with higher education levels had higher awareness and control rates of diabetes than those with lower education levels. This is consistent with the results of some studies [33,34,35]. Previous studies have confirmed that education level is positively correlated with the health literacy level in patients with diabetes [36]. The individuals with higher education are more self-conscious about health maintenance and know more about diabetes, and thus, consciously take steps to manage diabetes. A study based in the US has shown that obesity is associated with reduced awareness of diabetes, with obese individuals having lower blood sugar control levels than those with normal weight [37]. This finding is consistent with findings of the present study. Moreover, some observational and experimental studies suggest that unhealthy lifestyles, such as alcohol consumption, are associated with poor diabetes control [8], which is consistent with the results of the present study.
The present study found age, BMI, and central obesity to be risk factors for diabetes prevalence, which is consistent with results of previous studies on older individuals [21, 38]. With rapid development of the economy and urbanisation, the way of living has changed significantly in Chinese individuals. Chinese consumers have shown a sharp increase in consumption of meat and reduction in consumption of cereals. People are less physically active and adopt a sedentary lifestyle, which has increased the obesity rates in Chinese population and increased the risk of diabetes [39,40,41]. Previous studies have shown that smoking, drinking, and lack of physical exercise are closely associated with incidence of T2DM [42, 43]. However, these associations were not observed in the present study. This may be because we investigated participants' current behaviour rather than past behaviour, and some subjects may have changed their lifestyle after being diagnosed with T2DM, which may have affected the results.
To circumvent the high prevalence of diabetes and insufficiency of blood glucose control, the relevant government departments should continue to strengthen the prevention and management of patients with diabetes. First, to increase the early screening of patients with diabetes, early identification is crucial for the primary prevention of diabetes, especially in high-risk groups. Second, health workers should strengthen the management of patients with diabetes, regularly perform blood glucose testing, examine for complications, and impart self-management knowledge education in patients with diabetes. Finally, the government can adopt lifestyle intervention policies, lifestyle interventions can prevent or delay diabetes progress, advocating residents insist on physical exercise regularly, pay attention to weight, low salt, low fat, and low oil diet health education, which will help residents to develop a healthy lifestyle, improve lipid metabolism, maintain a healthy weight, and reduce the risk of T2DM.
This study has some limitations. First, due to the cross-sectional nature of the study, the causal relationship between T2DM and some risk factors could not be inferred; therefore, longitudinal studies are needed to verify the conclusions.Second, dietary habits, family history, and other chronic diseases associated with diabetes were not included as variables in the study.
Conclusions
The study identified high prevalence of T2DM in Chinese elderly individuals, despite improvement in awareness and control, and highlighted the demographics compared to those in developed countries. In view of the large and growing elderly population in China, diabetes may cause great harm, and thus, it is necessary to strengthen the management of senile diabetes. The relevant departments should adopt appropriate policies and interventions to implement effective education programs. Additionally, individuals should adopt a healthy lifestyle, increase physical activity, and maintain healthy weight, as these measures would help in the management of diabetes and reduce the economic burden in China.
Availability of data and materials
Data supporting the results of this study are not publicly available due to regulatory restrictions, but are available from the corresponding author on reasonable request.
Abbreviations
- T2DM:
-
Type 2 diabetes mellitus
- SD:
-
Standard deviation
- BMI:
-
Body mass index
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- WC:
-
Waist circumference
- FBG:
-
Fasting plasma glucose
- CI:
-
Confidence interval
- OR:
-
Odds ratio
References
Li MZ, Su L, Liang BY, Tan JJ, Chen Q, Long JX, Xie JJ, Wu GL, Yan Y, Guo XJ, et al. Trends in prevalence, awareness, treatment, and control of diabetes mellitus in mainland china from 1979 to 2012. Int J Endocrinol. 2013;2013:753150.
Rahman MS, Akter S, Abe SK, Islam MR, Mondal MN, Rahman JA, Rahman MM. Awareness, treatment, and control of diabetes in Bangladesh: a nationwide population-based study. PLoS One. 2015;10(2):e0118365.
Writing Group M, Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133(4):e38-360.
Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, Stein C, Basit A, Chan JCN, Mbanya JC, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119.
Zhou X, Guan H, Zheng L, Li Z, Guo X, Yang H, Yu S, Sun G, Li W, Hu W, et al. Prevalence and awareness of diabetes mellitus among a rural population in China: results from Liaoning Province. Diabet Med. 2015;32(3):332–42.
Shi ZMP, Yang SHMP, Dou KFMP, Song WJMP, Xiao JMP, Yang WM, He JMP. Prevalence of Diabetes among Men and Women in China. N Engl J Med. 2010;362(25):2425–2425 (author reply 2426).
Ma RCW. Epidemiology of diabetes and diabetic complications in China. Diabetologia. 2018;61(6):1249–60.
Liu M, Wang J, He Y, Jiang B, Wu L, Wang Y, Di Z, Zeng J. Awareness, treatment and control of type 2 diabetes among Chinese elderly and its changing trend for past decade. BMC Public Health. 2016;16:278.
Felix HC, Narcisse MR, Long CR, English E, Haggard-Duff L, Purvis RS, McElfish PA. The Effect of Family Diabetes Self-management Education on Self-care Behaviors of Marshallese Adults with Type 2 Diabetes. Am J Health Behav. 2019;43(3):490–7.
McElfish PA, Long CR, Bursac Z, Scott AJ, Felix HC, Schulz TK, Worley MA, Rowland B. Diabetes self-management education exposure and glycated haemoglobin levels among Marshallese participants in a randomized controlled study. Diabet Med. 2020;37(2):319–25.
McElfish PA, Long CR, Kohler PO, Yeary KHK, Bursac Z, Narcisse MR, Felix HC, Rowland B, Hudson JS, Goulden PA. Comparative Effectiveness and Maintenance of Diabetes Self-Management Education Interventions for Marshallese Patients With Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care. 2019;42(5):849–58.
Bi Y, Zhu D, Cheng J, Zhu Y, Xu N, Cui S, Li W, Cheng X, Wang F, Hu Y, et al. The status of glycemic control: A cross-sectional study of outpatients with type 2 diabetes mellitus across primary, secondary, and tertiary hospitals in the Jiangsu province of China. Clin Ther. 2010;32(5):973–83.
Yin J, Yeung R, Luk A, Tutino G, Zhang Y, Kong A, Chung H, Wong R, Ozaki R, Ma R, et al. Gender, diabetes education, and psychosocial factors are associated with persistent poor glycemic control in patients with type 2 diabetes in the Joint Asia Diabetes Evaluation (JADE) program. J Diabetes. 2016;8(1):109–19.
Liu M, Lv X, Li Y, Li J, He Y. Prevalence and Control Status of Diabetes and Related Risk Factors Among 4196 Chinese Male Older Elderly Aged ≥80 Years. Int J Gerontol. 2018;12(2):122–6.
Wang H, Yao J, Yin X, Guo X, Yin J, Qu H, Sun Q. Organisational and individual characteristics associated with glycaemic control among patients with type 2 diabetes: cross-sectional study in China. BMJ Open. 2020;10(4):e036331.
Xu Y, Wang L, He J, Bi Y, Li M, Wang T, Wang L, Jiang Y, Dai M, Lu J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310(9):948–59.
Irazola V, Rubinstein A, Bazzano L, Calandrelli M, Chung-Shiuan C, Elorriaga N, Gutierrez L, Lanas F, Manfredi JA, Mores N, et al. Prevalence, awareness, treatment and control of diabetes and impaired fasting glucose in the Southern Cone of Latin America. PLoS One. 2017;12(9):e0183953.
Hu D, Fu P, Xie J, Chen CS, Yu D, Whelton PK, He J, Gu D. Group MSftIC: Increasing prevalence and low awareness, treatment and control of diabetes mellitus among Chinese adults: the InterASIA study. Diabetes Res Clin Pract. 2008;81(2):250–7.
Wuhan Municipal Bureau of Statistics, Wuhan Nsoi. Wuhan Statistical Yearbook. Beijing: China Statistics Press; 2021. http://www.zgtjcbs.com.
Wang Q, Zhang X, Fang L, Guan Q, Guan L, Li Q. Prevalence, awareness, treatment and control of diabetes mellitus among middle-aged and elderly people in a rural Chinese population: a cross-sectional study. PLoS One. 2018;13(6):e0198343.
Sun Y, Ni W, Yuan X, Chi H, Xu J. Prevalence, treatment, control of type 2 diabetes and the risk factors among elderly people in Shenzhen: results from the urban Chinese population. BMC Public Health. 2020;20(1):998.
Salas A, Acosta D, Ferri CP, Guerra M, Huang Y, Jacob KS, Jimenez-Velazquez IZ, Llibre Rodriguez JJ, Sosa AL, Uwakwe R, et al. The Prevalence, Correlates, Detection and Control of Diabetes among Older People in Low and Middle Income Countries. A 10/66 Dementia Research Group Population-Based Survey. PLoS One. 2016;11(2):e0149616.
McDonald M, Hertz RP, Unger AN, Lustik MB. Prevalence, awareness, and management of hypertension, dyslipidemia, and diabetes among United States adults aged 65 and older. J Gerontol A Biol Sci Med Sci. 2009;64(2):256-263.1.
Bai A, Tao J, Tao L, Liu J. Prevalence and risk factors of diabetes among adults aged 45 years or older in China: a national cross-sectional study. Endocrinol Diabetes Metab. 2021;4(3):e00265.
Yang F, Qian D, Chen J, Hu D, Hou M, Chen S, Wang P, Group LWSP. Prevalence, awareness, treatment and control of diabetes mellitus in rural China: results from Shandong Province. Diabet Med. 2016;33(4):454–8.
Yue J, Mao X, Xu K, Lu L, Liu S, Chen F, Wang J. Prevalence, Awareness, Treatment and Control of Diabetes Mellitus in a Chinese Population. PLoS One. 2016;11(4):e0153791.
Bikbov MM, Fayzrakhmanov RR, Kazakbaeva GM, Zainullin RM, Arslangareeva II, Gilmanshin TR, Salavatova VF, Nikitin NA, Mukhamadieva SR, Yakupova DF, et al. Prevalence, awareness and control of diabetes in Russia: The Ural Eye and Medical Study on adults aged 40+ years. PLoS One. 2019;14(4):e0215636.
Sabanayagam C, Shankar A, Saw SM, Tai ES, Lim SC, Lee JJ, Wong TY. Prevalence of diabetes mellitus, glycemic control, and associated factors in a Malay population in Singapore. Asia Pac J Public Health. 2009;21(4):385–98.
Aekplakorn W, Stolk RP, Neal B, Suriyawongpaisal P, Chongsuvivatwong V, Cheepudomwit S, Woodward M, Group IC. The prevalence and management of diabetes in Thai adults: the international collaborative study of cardiovascular disease in Asia. Diabetes Care. 2003;26(10):2758–63.
Pan WH, Yeh WT, Chang HY, Hwu CM, Ho LT. Prevalence and awareness of diabetes and mean fasting glucose by age, sex, and region: results from the Nutrition and Health Survey in Taiwan, 1993–1996. Diabet Med. 2003;20(3):182–5.
King H, Aubert RE, Herman WH. Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes Care. 1998;21(9):1414–31.
Selcuk KT, Sozmen MK, Togrul BU. Diabetes prevalence and awareness in adults in the Balcova district in Turkey. Turk J Med Sci. 2015;45(6):1220–7.
Yang MH, Hall SA, Piccolo RS, Maserejian NN, McKinlay JB. Do Behavioral Risk Factors for Prediabetes and Insulin Resistance Differ across the Socioeconomic Gradient? Results from a Community-Based Epidemiologic Survey. Int J Endocrinol. 2015;2015:806257.
Redondo A, Benach J, Subirana I, Martinez JM, Munoz MA, Masia R, Ramos R, Sala J, Marrugat J, Elosua R. Trends in the prevalence, awareness, treatment, and control of cardiovascular risk factors across educational level in the 1995–2005 period. Ann Epidemiol. 2011;21(8):555–63.
Cai L, Li X, Cui W, You D, Golden AR. Trends in diabetes and pre-diabetes prevalence and diabetes awareness, treatment and control across socioeconomic gradients in rural southwest China. J Public Health (Oxf). 2018;40(2):375–80.
Hu FBMD, Manson JEMD, Stampfer MJMD, Colditz GMD, Liu SMD, Solomon CGMD, Willett WCMD. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N Engl J Med. 2001;345(11):790–7.
Okosun I, Dever GEA, Dever GEA. Abdominal Obesity and Ethnic Differences in Diabetes Awareness, Treatment, and Glycemic Control. Obes Res. 2002;10(12):1241–50.
Bi Y, Wang L, Xu Y, Jiang Y, He J, Zhang M, Zhou M, Li Y, Xu M, Lu J, et al. Diabetes-related metabolic risk factors in internal migrant workers in China: a national surveillance study. Lancet Diabetes Endocrinol. 2016;4(2):125–35.
Zhai F, Wang H, Du S, He Y, Wang Z, Ge K, Popkin BM. Prospective study on nutrition transition in China. Nutr Rev. 2009;67(Suppl 1):S56-61.
Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care. 2011;34(6):1249–57.
Ng SW, Norton EC, Popkin BM. Why have physical activity levels declined among Chinese adults? Findings from the 1991–2006 China Health and Nutrition Surveys. Soc Sci Med. 2009;68(7):1305–14.
Qiu L, Wang W, Sa R, Liu F. Prevalence and Risk Factors of Hypertension, Diabetes, and Dyslipidemia among Adults in Northwest China. Int J Hypertens. 2021;2021:5528007.
Liu X, Li Y, Li L, Zhang L, Ren Y, Zhou H, Cui L, Mao Z, Hu D, Wang C. Prevalence, awareness, treatment, control of type 2 diabetes mellitus and risk factors in Chinese rural population: the RuralDiab study. Sci Rep. 2016;6:31426.
Acknowledgements
We greatly appreciate the support of the participants and the hard work of the researchers during this study.
Funding
This study was funded by Wuhan Centers for Disease Control & Prevention (Grant No.WJ2018H242).
Author information
Authors and Affiliations
Contributions
Yaqiong Yan has made great contributions to the data analysis and manuscript writing of the paper. Tingting Wu sorted out the data and revised the manuscript. Miao Zhang participated in data cleaning, analysis and article modification. Changfeng Li participated in the data collection and collation. Qing Liu researched and designed the overall idea of the manuscript and assisted in revising the manuscript. Fang Li revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the Ethics Committee of Wuhan Center for Disease Control and Prevention (IRB#:WHCDCIRB-K-2018023), and all methods were performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants before data collection.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Sociodemographic characteristics of adults aged 65 and older in Wuhan. Notes: T2DM, type 2 diabetes mellitus; SD, standard deviation; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; WC, waist circumference; FBG, fasting plasma glucose. * P < 0.05;** P < 0.01;***P < 0.001; Categorical variables were analyzed by chi-square test.
Additional file 2: Table 2
. Prevalence, awareness, and control of T2DM among adults aged 65 and older in Wuhan. Notes: T2DM, type 2 diabetes mellitus; CI, confidence interval; BMI, body mass index. a Central obesity was defined as waist circumference 90 cm or more in men and 85 cm or more in women. * P < 0.05;** P < 0.01;***P < 0.001; Categorical variables were analyzed by chi-square test.
Additional file 3: Table 3
. Risk factors for the prevalence, awareness, and control of T2DM. Notes: T2DM, type 2 diabetes mellitus; OR, odds ratio; CI, confidence interval; BMI, body mass index. a Multivariate logistic analysis. Model fittings were conducted using stepwise method with a threshold of 0.10 for variable inclusion in the model. b Central obesity was defined as waist circumference 90 cm or more in men and 85 cm or more in women. * P < 0.05;** P < 0.01;***P < 0.001; Variables that were not included in the final logistic regression model were marked with “-”.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, Y., Wu, T., Zhang, M. et al. Prevalence, awareness and control of type 2 diabetes mellitus and risk factors in Chinese elderly population. BMC Public Health 22, 1382 (2022). https://doi.org/10.1186/s12889-022-13759-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13759-9