
Abstract
Background
To assess the associations between no table salt and hypertension or stroke.
Methods
The data of 15,352 subjects were collected from National Health and Nutrition Examination Survey (NHANES) database. All subjects were divided into no hypertension or stroke group (n = 10,894), hypertension group (n = 5888), stroke group (n = 164) and hypertension and stroke group (n = 511). Univariate and multivariate logistic regression analysis was used to measure the associations of salt type used with hypertension and stroke and co-variables were respectively adjusted in different models.
Results
After adjusting age and gender, other salt intake was associated with 1.88-fold risk of hypertension (OR = 1.88, 95%CI: 1.44–2.46) and no table salt was associated with 1.30-fold risk of hypertension (OR = 1.30, 95%CI: 1.15–1.47). After adjusting age, gender, race, BMI, PIR, marital status, CVDs, whether doctors’ told them to reduce salt, and diabetes, the risk of hypertension was 1.23-fold increase in no table salt group (OR = 1.23, 95%CI: 1.04–1.46). After the adjustment of age and gender, the risk of hypertension and stroke was 3.33-fold increase (OR = 3.33, 95%CI: 2.12–5.32) in other salt intake group and 1.43-fold increase (OR = 1.43, 95%CI:1.17–1.74) in no table salt group.
Conclusion
Other salt intake or no table salt were associated with a higher risk of hypertension or hypertension and stroke.
Similar content being viewed by others


Background
Hypertension is reported to be a major cause of premature deaths and a heavy burden of cardiovascular morbidity and mortality, which resulted in approximately 7.1 million deaths and an estimated cost of $48.6 billion ever year [1]. Hypertension is widely validated to increase the risk of developing cardiovascular diseases (CVD) such as coronary heart disease (CHD) and stroke [2, 3]. Hypertension has strong associations with atherosclerosis deposits blocking and narrowing brain arteries, which has become a major risk factor for the occurrence of stroke [4, 5]. Stroke is reported to be the leading cause of death in China and the second leading cause of death all through the world [6]. Stroke is also the main reason of long-term neurological disability in adults, which leads to a substantial economic burden to the society and a decreased quality of life in patients [7]. Considering the considerable amount of economic burden to the family and society, more effective health care planning and prevention of hypertension and stroke are necessary.
Currently, some researches proposed that lifestyle changes may have significant effects on blood pressure control [8]. As high salt intake was reported to be associated with the risk of hypertension and cardiovascular events, restricting dietary salt has been proposed to be a method for hypertension prevention [9, 10]. Salt reduction was considered to be an important dietary target for 2025 to reduce the mortality of main noncommunicable diseases by the World Health Organization (WHO) [11]. In recent years, low-salt diet or event no-salt diet was advocated to improve health and prevent some diseases [12]. Previously, a study reported that about 10% of the sodium intake comes from discretionary salt use including table salt and salt added while cooking, which can be controlled by individuals [13]. For some people, to control salt use in daily life indicated low salt or no salt indicate adding low or no salt at table, and some other people added lite salt or salt substitute at table. Lite salt or salt substitute refer to sodium chloride in traditional salt is partially replaced with potassium chloride or magnesium sulfate, which are considered as a strategy under consideration by several countries for lowing blood pressure [14]. At present, various studies have explored the associations between sodium intake and the risk of hypertension or stroke [3, 15]. High sodium intake was associated with increased risk of hypertension or stroke. People was advocated to reduced salt use. But for common people, monitoring the salt contributions of specific foods and food groups, differentiating the inherent and processing-added sodium content of foods or other dietary sources were difficult [13]. It is easier for controlling the discretionary salt use including table salt and salt added while cooking to achieve the sodium intake reduction. Previous studies were focused on the volume of salt intake with the risk of hypertension and stroke, whether the different types of salt used just at table or during cooking were associated with the risk of hypertension or stroke were still unclear. Thus, the associations of doesn’t add salt product or adding different varieties of salt at the table or during cooking in hypertension or stroke still needs investigation, which might provide a guide for salt use in common people in the prevention of hypertension stroke.
In the current study, the associations of different salt types added at table or no table salt with the occurrence of hypertension and stroke were assessed based on the data from National Health and Nutrition Examination Survey (NHANES) database.
Methods
Study population
The NHANES database included a multifaceted health examination on a nationally representative sample of the civilian, non-institutionalized population in the United States based on complex multistage stratified probability sampling methods [16]. NHANES data is publicly available and the data collection and data release were approved by the National Center for Health Statistics (NCHS) Ethics Review Board [17]. The current study collected the clinical data of 22,564 participants aged > 20 years from the NHANES database from 2011 to 2018. After excluding participants without data on salt intake, and baseline characteristics including poverty income ratio (PIR), history of diabetes, body mass index (BMI), sodium and marital status, 15,352 subjects were involved in. All subjects were divided into no hypertension or stroke group (n = 9297), hypertension group (n = 4661), stroke group (n = 340) and hypertension and stroke group (n = 1054). The detailed screen process was shown in Fig. 1.

Screen process of participants in this study
Main variables and outcome variables
The data of all participants were collected and analyzed including age, gender, BMI (kg/m2, < 18.5 kg/m2, 18.5–24.9 kg/m2, 25.0–29.9 kg/m2 or ≥ 30.0 kg/m2), race (Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black or other), education level (less than 9th grade, 9-11th grade, high school graduate, some college, or college graduate), marital status (married, widowed, divorced, separated, never married and living with partner), and PIR, history of diabetes, history of cardiovascular diseases (CVDs; congestive heart failure, coronary heart disease, angina/angina pectoris and heart attack), whether the participant’s doctor told them to reduce salt intake, type of table salt used (ordinary salt, other salt or no table salt).
Data measurement and variable definition
In NHANES database, health questionnaires were collected from all subjects in their home, and physical, laboratory and anthropometric examinations were performed in Mobile Examination Centers (MEC) by well-trained health technicians following standardized procedures.
People with hypertension, stroke, or hypertension and stroke were measured as outcome variables. Hypertension was defined as self-reported physician diagnosis, mean systolic blood pressure ≥ 140 mmHg or mean diastolic blood pressure ≥ 90 mmHg or use of antihypertensive medication [18]. Data from the Medical Conditions Questionnaire (MCQ160f) were applied to identify stroke diagnosis. Participants who replied “Yes” to the question “Has a doctor or other health professional ever told you that you had stroke?” were identified as stroke survivors [19]. Those who replied to have difficulties causing by stroke problems based on the Physical Functioning Questionnaire (PFQ) (063A-063E) were also defined to have stroke [20].
Hypertension and stroke was defined according to the self-reported physician diagnosis of both hypertension and stroke.
No table salt referred to no salt used or added at the table and in food preparation in household. Ordinary salt includes regular iodized salt, sea salt and seasoning salts made with regular salt, indicating using or adding these kinds of salt at the table or while cooking. Other salt indicated the lite salt or salt substitute at the table or while cooking. Potassium intake were calculated from the in-person 24-h dietary recall interview which was administered by trained interviewers using the USDA automated multiple-pass method [21, 22].
All subjects were asked to list all food and beverages consumed in the 24-h period from midnight to midnight on the day before the interview. The NHANES calculates the nutrient intake from food and beverage data based on the USDA’s Food and Nutrient Database for Dietary Studies (FNDDS) [23]. The FNDDS uses food composition data from the USDA National Nutrient Database or Standard Reference [24]. At the end of the dietary recall, participants were asked questions about discretionary salt use. The questions are:
-
1.
What type of salt do you usually add to food at the table? Would you say ordinary salt (includes regular iodized salt, sea salt, and seasoning salts made with regular salt), lite salt, salt substitute, don’t use or add salt at the table, other, don’t know?
-
2.
How often do you add ordinary salt to food at the table? Would you say rarely, occasionally, very often, refused, don’t know?
-
3.
How often is ordinary salt or seasoned salt added in cooking or preparing foods in your household? Is it never, rarely, occasionally, very often, or you don’t know?
Another variable including the data on salt use from the NHANES was DR2SKY with the questions of salt used at table yesterday? (Did {you/SP} add any salt to {your/her/his} food at the table yesterday? Salt includes ordinary or seasoned salt, lite salt, or a salt substitute.) and what type of salt was it? (Was it ordinary or seasoned salt, lite salt, or a salt substitute?).
The BMI in all people was divided into four groups: malnutrition group (< 18.5 kg/m2), normal weight group (18.5–24.9 kg/m2), overweight group (25.0–29.9 kg/m2) or obesity group (≥ 30.0 kg/m2).
Statistical analysis
All statistical tests were conducted by two-sided test. The sample data were subjected to a weighted manner to all analyses to account for the cluster sample design, oversampling, poststratification, survey nonresponse and sampling frame, and the weights were taken from sdmvstra, sdmvpsu and wtmec2yr variables in the NHANES database [25]. The mobile examination center (MEC) exam weight (wtmec2yr variables) was applied for weighting. The variable name for the masked variance unit pseudo-stratum was sdmvstra and the variable name for the masked variance unit pseudo-primary sampling units (PSUs) was sdmvpsu. The weight of the survey enabled it to be extended to the civilian noninstitutionalized US population. Sampling errors were calculated to determining their statistical reliability [26]. The measurement data of normal distribution were described by Mean ± standard deviation (Mean ± SD), the independent sample t test was applied for comparisons between groups. The non-normal distributed data were expressed by M (Q1, Q3), and differences between groups were compared by the Mann–Whitney U rank sum test. The enumeration data were described as n (%) and comparison of different groups was performed by chi-square test. Logistic regression analysis was used to measure the associations of salt types with hypertension and stroke. The odds ratios (ORs) and confidence intervals (CIs) were employed for evaluating the reliability of an estimate. As for different types of salt intake, three models were established: Crude model: the model without adjustment; Model 1: adjusted for age and gender; Model 2: adjusted for age, gender, race, BMI and PIR. SAS 9.4 statistical analysis software was used for data analyzing. The svydesign and svyglm function in R package survey (4.02 version) was applied for logistic regression modeling and draw the forest plot. The detailed data analysis process was presented in Supplementary Fig. 1. P < 0.05 was considered as statistical difference.
Results
The characteristics of participants
In total, 22,564 subjects from NHANES between 2011 and 2018 were involved in this study. After excluding participants with incomplete data on salt intake (n = 3175) and subjects with incomplete data on PIR (n = 1740), history of diabetes (n = 5), BMI (n = 170), sodium (n = 2150) and marital status (n = 2), 15,352 subjects were finally included and were divided into no hypertension or stroke group (n = 9297), hypertension group (n = 4661), stroke group (n = 340) and hypertension and stroke group (n = 1054). Among them, 5062 people were aged 20–39 years, accounting for 32.97%, 5164 people aged 40–59 years, accounting for 33.64%; 4274 persons aged 60–79 years, accounting for 27.84% and 852 persons aged ≥ 80 years, accounting for 5.55%. There were 7302 (47.56%) males and 8050 (52.44%) females. The median PIR of all participants was 2.14. In the study population, 2144 (13.97%) people had diabetes, 12,795 (83.34%) people had no diabetes, and 413 (2.69%) people were in borderline. There were 5715 patients with hypertension, accounting for 37.23% and 1394 patients suffered from stroke, accounting for 9.08%. As for salt used, 9964 people used ordinary salt, accounting for 64.90%, 664 people used other salts (lite salt or salt substitute), accounting for 4.33% and 4724 people did not add salt at the table, accounting for 30.77% (Table 1).
Comparisons of characteristics of participants among different groups
All study population was divided into four groups, 9297 people were no hypertension or stroke, 4661 people were hypertension patients, 340 people were stroke patients, and 1054 people were hypertension and stroke patients, The results depicted that the proration of people in different age (χ2 = 3036.02, P < 0.001), race (χ2 = 354.30, P < 0.001), education level (χ2 = 361.77, P < 0.001), marital status (χ2 = 1041.96, P < 0.001), BMI (χ2 = 815.64, P < 0.001), PIR (χ2 = 260.78, P < 0.001), diabetes (χ2 = 1697.86, P < 0.001), CVDs, doctors told them to reduce salt and change type of table salt used (χ2 = 207.99, P < 0.001) groups among no hypertension or stroke, hypertension patients, hypertension and stroke patients were statistically different (Table 2).
Multivariate logistic regression analysis
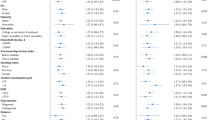
Compared with people consuming ordinary salt, the risk of hypertension was 2.09-fold increased (OR = 2.09, 95%CI: 1.61–2.71) in other salt intake group and 1.39-fold increased (OR = 1.39, 95%CI: 1.3–1.57) in no table salt group. After adjusting age and gender, other salt intake was associated with 1.88-fold risk of hypertension (OR = 1.88, 95%CI: 1.44–2.46) and no table salt was associated with 1.30-fold risk of hypertension (OR = 1.30, 95%CI: 1.15–1.47). After adjusting age, gender, race, BMI, PIR, marital status, CVDs, whether doctors’ told them to reduce salt and diabetes, the risk of hypertension was 1.23-fold increase in no table salt group (OR = 1.23, 95%CI: 1.04–1.46). Compared with those with ordinary salt at table, the risk of stroke in ordinary salt group or no table salt group was not statistically different (Fig. 2).

Forest plot of multivariable analysis of the associations between salt types and hypertension, stroke or hypertension companied with stroke
In comparison with people with ordinary salt at table, the risk of hypertension and stroke was 4.09-fold increase (OR = 4.09, 95%CI: 2.61–6.43) in other salt intake group and 1.61-fold increase (OR = 1.61, 95%CI: 1.32–1.95) in no table salt group. Post adjusting age and gender, the risk of hypertension and stroke was 3.33-fold increase (OR = 3.33, 95%CI: 2.12–5.32) in other salt intake group and 1.43-fold increase (OR = 1.43, 95%CI:1.17–1.74) in no table salt group. After adjusting age, gender, race, BMI, PIR, marital status, CVDs, whether doctors’ told them to reduce salt and diabetes, other salt intake and no table salt was not statistically associated with risk of hypertension and stroke (all P > 0.05) (Fig. 2).
Discussion
In the present study, the data of 15,352 participants were collected from the NHANES database to analyze the associations of salt types added at table with hypertension and stroke. The result delineated that other salt intake or no table salt might be associated with an increased risk of hypertension. Other salt intake or no table salt might be also associated with an increased risk of hypertension and stroke. The findings of our study might give a reference for the use of salt at table in preventing the occurrence of hypertension and stroke and improving the prognosis of patients with hypertension or hypertension and stroke.
Currently, salt substitutes are used to replace ordinary salt (100% sodium chloride) where a portion of sodium is replaced with potassium chloride (usually 25%-30%) and/or magnesium sulphate (10%-14%). Several meta-analyses involving randomized controlled trials (RCTs) revealed that salt substitutes application decreased the systolic blood pressure and diastolic blood pressure in patients with hypertension [27]. Salt substitute might be an accessible and effective method for reducing the risk of death caused by stroke in patients with hypertension [28]. In this study, patients with other salt intake (lite salt or salt substitute) were associated with a higher risk of hypertension or hypertension and stroke. Some studies have indicated that people may prefer the taste of ordinary salt to salt substitutes and some people do not accept the taste of salt substitutes, so when they use salt substitutes, they might use more amount of salt, which actually resulted in a high sodium intake [29]. In addition, we found for people with more salt substitutes at table, the potassium intake was lower than those with ordinary salt intake (Supplementary Fig. 2). Previous studies have revealed that potassium is an essential nutrient and the addition of a high potassium diet could reduce the blood pressure in people [30, 31]. Also, some randomized controlled trials indicated that higher potassium intake could lower the blood pressure in those with hypertension [32]. Therefore, adequate potassium supplement was recommended in people especially hypertension people.
As for people do not add salt product at the table, excessive low salt diet might cause salt-sensitivity hypertension, as long-term low sodium intake might result in the high sensitivity to salt in human body and increased sodium intake might stimulate the secretions of hormones such as epinephrine and angiotensin, which led to hypertension [33]. Salt-sensitivity hypertension was a potential area requiring validation for further research, as some other researchers indicated that although a high-salt diet might increase the accumulation of sodium, the expansion of volume, and the adjustment of cardiac outputs, the autoregulation might maintain the flow via increasing the systemic vascular resistance, and causing the kidneys to excrete more salt and water, and therefore reducing systems to normal and minimizing the changes in blood pressure [34]. Another study also depicted that sodium reduction only decreased the blood pressure in participants with a blood pressure in the highest 25th percentile of all population and the author also suggested to reframe the policy of lowering dietary sodium intake in the general population and hypertension patients [35]. Sodium is main extracellular cation in the body to maintain intravascular volume, which is required in human body and salt restriction in humans may cause some adverse effects [36]. A previous study also reported that salt-deficient diet promoted cystogenesis in ARPKD via epithelial sodium channel [37]. Besides, people might intake more sodium rather than eat at table. Nowadays, commercial products infiltrate sodium insensibly into our nutrition and the involuntary sodium intake was high in daily life [38]. People who used other salt or do not add salt at table might prefer other commercial products with high sodium.
The findings of our study suggested that adding ordinary salt at table with appropriate volume is recommended for the prevention of hypertension. In addition, for people with hypertension or hypertension and stroke, adding lower volume of ordinary salt at table as well as enough potassium supplement were necessary for blood pressure control. This study measured the associations of salt with hypertension and stroke based on the data of 15,352 subjects from NHANES database. Our study involved in a large sample size and subgroup analysis was conducted in different types of salt, which might increase the reliability of our results. The findings of our study might provide a reference for the salt use at table or during cooking for common people. Several limitations existed in the current study. Firstly, the participants included in NHANES database were mainly from western countries, and whether the findings were suitable for people from oriental countries still needs validation in more studies. Secondly, the sample size in other salt group was small, which might decrease the statistical power. Thirdly, all data were collected from NHANES database, and important variables such as 24-h urine sodium of participants were not evaluated; the outcome variables were self-reported, which might cause bias. Fourthly, the self-reports of prior stroke in the NHANES stroke data represents a sample of stroke survivors, and we couldn’t analyze the data on those with acute stroke die, or are disabled to the extent that they are hospitalized, home-bound or institutionalized in long term care facilities. In the future, RCTs including large scale of sample size were required to verify the results in this study.
Conclusions
This study analyzed the associations of different salt types and no table salt with hypertension and stroke based on the data of 15,352 subjects NHANES database. The results delineated that no table salt was associated with a higher risk of hypertension or hypertension and stroke. The findings suggested that salt intake is important and required in common people and in patients with hypertension or hypertension with stroke, necessary ordinary salt intake and enough potassium intake were required to control the blood pressure.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. The original data were accessed from https://www.cdc.gov/nchs/nhanes/about_nhanes.
Abbreviations
- NHANES:
-
National Health and Nutrition Examination Survey
- BMI:
-
Body mass index
- CVD:
-
Cardiovascular diseases
- CHD:
-
Coronary heart disease
- WHO:
-
World Health Organization
- PIR:
-
Poverty income ratio
- MEC:
-
Mobile Examination Centers
- Mean ± SD:
-
Mean ± standard deviation
- OR:
-
Odds ratio
- CI:
-
confidence intervals
References
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation. 2016;134(6):441–50.
Fan F, Yuan Z, Qin X, Li J, Zhang Y, Li Y, et al. Optimal Systolic Blood Pressure Levels for Primary Prevention of Stroke in General Hypertensive Adults: Findings From the CSPPT (China Stroke Primary Prevention Trial). Hypertension. 2017;69(4):697–704.
Rust P, Ekmekcioglu C. Impact of Salt Intake on the Pathogenesis and Treatment of Hypertension. Adv Exp Med Biol. 2017;956:61–84.
Chaudhary NS, Bridges SL Jr, Saag KG, Rahn EJ, Curtis JR, et al. Severity of Hypertension Mediates the Association of Hyperuricemia With Stroke in the REGARDS Case Cohort Study. Hypertension. 2020;75(1):246–56.
O’Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–75.
GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):439–58.
Aringazina A, Kuandikov T, Arkhipov V. Burden of the Cardiovascular Diseases in Central Asia. Cent Asian J Glob Health. 2018;7(1):321.
Lenfant C, Chobanian AV, Jones DW, Roccella EJ. Seventh report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7): resetting the hypertension sails. Hypertension. 2003;41(6):1178–9.
O’Donnell M, Mente A, Rangarajan S, McQueen MJ, Wang X, Liu L, et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N Engl J Med. 2014;371(7):612–23.
Strazzullo P, D’Elia L, Kandala NB, Cappuccio FP. Salt intake, stroke, and cardiovascular disease: meta-analysis of prospective studies. BMJ. 2009;339:b4567.
Beaglehole R, Bonita R, Horton R, Ezzati M, Bhala N, Amuyunzu-Nyamongo M, et al. Measuring progress on NCDs: one goal and five targets. Lancet. 2012;380(9850):1283–5.
Khan MS, Jones DW, Butler J. Salt, No Salt, or Less Salt for Patients With Heart Failure? Am J Med. 2020;133(1):32–8.
Mattes RD, Donnelly D. Relative contributions of dietary sodium sources. J Am Coll Nutr. 1991;10(4):383–93.
Zhou B, Webster J, Fu LY, Wang HL, Wu XM, Wang WL, Shi JP. Intake of low sodium salt substitute for 3years attenuates the increase in blood pressure in a rural population of North China - A randomized controlled trial. Int J Cardiol. 2016;215:377–82.
Aburto NJ, Ziolkovska A, Hooper L, Elliott P, Cappuccio FP, Meerpohl JJ. Effect of lower sodium intake on health: systematic review and meta-analyses. BMJ (Clinical research ed). 2013;346:f1326.
Gallo S, Byham-Gray L, Duffy VB, Hoffman HJ, Hayes JE, Rawal S. Associations of olfactory dysfunction with anthropometric and cardiometabolic measures: Findings from the 2013–2014 national health and nutrition examination survey (NHANES). Physiol Behav. 2020;215: 112702.
Statistics NCfHS: https://www.cdc.gov/nchs/nhanes/about_nhanes
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159–219.
Statistics NCfH: Available from: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/MCQ_G.htm.
Statistics NCfH: Available from: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/PFQ_G.htm.
Rehm CD, Peñalvo JL, Afshin A, Mozaffarian D. Dietary Intake Among US Adults, 1999–2012. JAMA. 2016;315(23):2542–53.
Services UDoAAR: Available from: http://www.ars.usda.gov/Services/docs.htm?docid= 7710 2010.
US Department of Agriculture Agricultural Research Services. USDA food and nutrient database for dietary studies, 4.1. Version current 16 February 2012. Available from: http://www.ars.usda.gov/Services/docs.htm?docid=20511 Cited 22 January 2012.
US Department of Agriculture Agricultural Research Services. USDA national nutrient database for standard reference. Version current 16 May 2012. Available from: http://www.ars.usda.gov/main/site_main.htm?modecode=12-35-45-00 Cited 16 May 2012.
Centers for Disease Control and Prevention (CDC). NCfHSN: National Health and Nutrition Examination Survey: analytic guidelines, 2011–2014 and 2015–2016. 2018.
Statistics NCfH: Available from: https://wwwn.cdc.gov/nchs/data/nhanes/analyticguidelines/11-16-analytic-guidelines.pdf.
Hernandez AV, Emonds EE, Chen BA, Zavala-Loayza AJ, Thota P, Pasupuleti V, et al. Effect of low-sodium salt substitutes on blood pressure, detected hypertension, stroke and mortality. Heart. 2019;105(12):953–60.
Sun H, Ma B, Wu X, Wang H, Zhou B. Long-Term Effect of Salt Substitute on All-Cause and Cardiovascular Disease Mortality: An Exploratory Follow-Up of a Randomized Controlled Trial. Front Cardiovasc Med. 2021;8:645902.
Li N, Prescott J, Wu Y, Barzi F, Yu X, Zhao L, Neal B. The effects of a reduced-sodium, high-potassium salt substitute on food taste and acceptability in rural northern China. Br J Nutr. 2009;101(7):1088–93.
Smiljanec K, Mbakwe A, Ramos Gonzalez M, Farquhar WB, Lennon SL. Dietary Potassium Attenuates the Effects of Dietary Sodium on Vascular Function in Salt-Resistant Adults. Nutrients. 2020;12(5):1206.
Stone MS, Martyn L, Weaver CM. Potassium Intake, Bioavailability, Hypertension, and Glucose Control. Nutrients. 2016;8(7):444.
Aburto NJ, Hanson S, Gutierrez H, Hooper L, Elliott P, Cappuccio FP. Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ (Clinical research ed). 2013;346:f1378.
Chatelanat O, Pechère-Bertschi A, Ponte B. Salt sensitivity and hypertension. Rev Med Suisse. 2019;15(662):1625–8.
Titze J, Luft FC. Speculations on salt and the genesis of arterial hypertension. Kidney Int. 2017;91(6):1324–35.
Graudal N, Hubeck-Graudal T, Jürgens G, Taylor RS. Dose-response relation between dietary sodium and blood pressure: a meta-regression analysis of 133 randomized controlled trials. Am J Clin Nutr. 2019;109(5):1273–8.
Nishimuta M, Kodama N, Yoshitake Y, Shimada M, Serizawa N. Dietary Salt (Sodium Chloride) Requirement and Adverse Effects of Salt Restriction in Humans. J Nutr Sci Vitaminol (Tokyo). 2018;64(2):83–9.
Ilatovskaya DV, Levchenko V, Pavlov TS, Isaeva E, Klemens CA, Johnson J, et al. Salt-deficient diet exacerbates cystogenesis in ARPKD via epithelial sodium channel (ENaC). EBioMedicine. 2019;40:663–74.
Goldstein P, Leshem M. Dietary sodium, added salt, and serum sodium associations with growth and depression in the U.S. general population. Appetite. 2014;79:83–90.
Acknowledgements
None.
Funding
This study was supported by Hypertension Disease (Tai Ge) Special Scientific Research Project of Sichuan Medical Association (2019TG34); Guizhou Health Committee (gzwjkj2020-1–209); Science and Technology Department of Guizhou Province (QKHJC [2020] 1Y031). The funding body played no role in this study.
Author information
Authors and Affiliations
Contributions
ZQL and YLZ designed the study. ZQL wrote the manuscript. LH, XXR, JL and XJX collected, analyzed and interpreted the data. YLZ critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure 1.
The detailed process of data analysis in this study.
Additional file 2: Supplementary Figure 2.
The potassium levels in people with different types of salt added at table.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Z., Hu, L., Rong, X. et al. Role of no table salt on hypertension and stroke based on large sample size from National Health and Nutrition Examination Survey database. BMC Public Health 22, 1292 (2022). https://doi.org/10.1186/s12889-022-13722-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13722-8