
Abstract
Background
The aim of this ecological study was to assess the area-level relationship between cumulative death rate for COVID-19 and historic influenza vaccination uptake in the New York City population.
Methods
Predictors of COVID-19 death included self-reported influenza vaccination in 2017, as well as four CDC-defined risk factors of severe COVID-19 infection available at the ecological level, which were diabetes, asthma, BMI 30–100 (2 kg/m2) and hypertension, in addition to race and age (65 + years).
Results
After adjusting for potential confounders, for every one-unit increase in influenza vaccination uptake for each zip code area, the rate of COVID-19 deaths decreased by 5.17 per 100,000 residents (p < 0.0001).
Conclusions
Zip codes with a higher prevalence of influenza vaccination had lower rates of COVID-19 mortality, inciting the need to further explore the relationship between influenza vaccination uptake and COVID-19 mortality at the individual level.
Similar content being viewed by others


Background
New York City was an early and prominent epicenter of the coronavirus (COVID-19) pandemic in the United States, with over 360,000 cases and 24,000 deaths [1] as of December 2, 2020. Even though COVID-19 vaccinations are widely available, demand has tapered [2], and many Americans are still hesitant to get vaccinated [3]. As such, it is necessary to understand why some people had worse or better outcomes by assessing similarities in how people respond to different respiratory viruses.
Influenza vaccination has been postulated to mitigate COVID-19 severity [4], particularly in elderly populations [5, 6]. However, there are racial and socio-economic factors associated with both COVID-19 severity [7] and the likelihood of getting an influenza vaccine [7] that could act as confounders. Although previous studies have been conducted in Italy [5, 6] and two non-peer reviewed articles in the United States and Brazil, none include these possible confounders. For the first time, we assessed the area-level relationship between cumulative death rate for COVID-19 and historic influenza vaccination uptake in New York City and adjusted for possible confounders, including racial factors and COVID-19 severity, as defined by the Centers for Disease Control and Prevention (CDC) [8].
Methods
An ecological analysis was conducted at the modified zip code tabulation area (MODZCTA) level; there are 178 MODZCTAs in New York City. Cumulative COVID-19 death rates through December 2, 2020 were extracted by MODZCTA from the New York City (NYC) Department of Health (DOH) Coronavirus repository. Age-adjusted prevalence (%) of self-reported influenza vaccination in the previous year, diabetes, asthma, BMI ≥ 30 kg/m2, and hypertension by United Hospital Fund (UHF) neighborhood were sourced from the 2017 Community Health Survey (CHS) via the Department of Health and Mental Hygiene’s EpiQuery tool [9]. Inclusion of diabetes, asthma, BMI ≥ 30 kg/m2, and hypertension was based on CDC-defined risk factors of severe COVID-19 infection [8]. Other covariates of interest, including the percent of residents who were white, Hispanic, and ≥ 65 years old in each ZCTA, were extracted from the American Community Survey (ACS) 2018 5-year estimates [10]. Data for CHS and ACS indicators were converted to MODZCTA using crosswalks provided by the NYC DOH [11, 12]. This study is exempt from IRB approval as data used is de-identified and publicly available. We conducted a multivariable linear regression analysis to assess the MODZCTA level association of COVID-19 death rates with prevalence of influenza vaccination in 2017, adjusting for possible confounders. All methods were carried out in accordance with relevant guidelines and regulations' or the 'Declaration of Helsinki'.
Results
Overall, in NYC in 2017, 44% of residents reported receiving an influenza vaccine in the previous year, 13% reported having asthma, 25% reported having a BMI ≥ 30 kg/m2, and 28% reported having hypertension. The overall population of NYC was 43% white, 29% Hispanic, and 15% 65 years or older (Table 1).
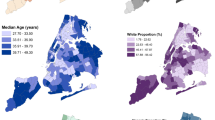
After adjusting for potential confounders, predictors accounted for 49% of the variability in the COVID-19 death rate (p < 0.0001), and for every one-unit increase in influenza vaccination uptake for each zip code area, the rate of COVID-19 deaths decreased by 5.17 per 100,000 residents (p < 0.0001) (Fig. 1). The proportion of white residents (Badj = -1.710, p < 0.0001) was also significantly inversely associated with mortality. Older age (Badj = 11.980, p < 0.0001) and the proportion of Hispanic residents were positively associated with COVID-19 mortality (Badj = 1.580, p = 0.0002).

Distribution of the COVID-19 cumulative death rate per 100,000 residents February 29-December 2, 2020 (top) and age-adjusted prevalence (%) of self-reported influenza vaccination (bottom) from UHF 2017 CHS across 178 NYC Modified Zip Code Tabulation Areas
Discussion
We show here for the first time, to our knowledge, that New York City neighborhoods with a higher prevalence of influenza vaccination had lower rates of COVID-19 mortality, even after adjustment for racial and ethnic makeup, and distribution of age and health risk factors for severe COVID-19. While the association with risk factors for severe COVID-19 was tempered after adjustment, our results still reveal some racial/ethnic disparities in the COVID-19 death rate, which may be indicative of reduced health care accessibility among minority populations [13] and increased risk for community spread [14]. However, a major limitation of this analysis is that the neighborhood-level study design hinders our ability to come to individual-level conclusions. Additionally, influenza vaccination uptake may indirectly indicate better access to healthcare in general, which may contribute to reduced COVID-19 severity. Further, it is also possible that people who get an influenza vaccine may have better health knowledge, and may have been more likely to engage in health behaviors that would reduce the risk of infection, such as masking and social distancing. Influenza vaccine data are from 2017, as the CHS does not report more recent data, and the duration of the heterologous or non-specific effects of vaccines is unknown.
This analysis is the first to consider these confounders in a US based database and contribute this information to the current literature on COVID-19. These findings suggest that influenza vaccination may have contributed to lower COVID-19 mortality. Further examining this relationship may help elucidate our understanding of population wide prevention and mitigation measures for other respiratory viruses. We suggest that future research should explore the relationship between influenza vaccination uptake and COVID-19 mortality at the individual level.
Conclusion
In light of this study, influenza vaccination should be actively promoted, in addition to the COVID-19 vaccine, as it may bolster public health, particularly for those not yet eligible for a COVID-19 vaccine.
Availability of data and materials
The data that support the findings of this study are openly.
Abbreviations
- COVID-19:
-
Coronavirus disease of 2019
- CDC:
-
Centers for Disease Control and Prevention
- MODZCTA:
-
Modified Zip Code Tabulation Area
- NYC:
-
New York City
- DOH:
-
Department of Health
- UHF:
-
United Hospital Fund
- CHS:
-
Community Health Survey
- ACS:
-
American Community Survey
References
NYC Department of Health. COVID-19: Totals Data. https://www1.nyc.gov/site/doh/covid/covid-19-data-totals.page Accessed 2 Dec 2020.
Wright, W and McDonnell Nieto del Rio, G. https://www.nytimes.com/2021/05/09/us/covid-vaccine-surplus.html New York Times.
Sgaier, SK. Meet the Four Kinds of People Holding Us Back From Full Vaccination. https://www.nytimes.com/interactive/2021/05/18/opinion/covid-19-vaccine-hesitancy.html New York Times.
Debisarun PA, Gössling KL, Bulut O, et al. Induction of trained immunity by influenza vaccination - impact on COVID-19. PLoS Pathog. 2021;17(10):e1009928. https://doi.org/10.1371/journal.ppat.1009928 (Published 2021 Oct 25).
Amato M, Werba JP, Frigerio B, et al. Relationship between Influenza vaccination coverage rate and COVID-19 outbreak: an Italian ecological study. Vaccines. 2020;8(3):535.
Marín‐Hernández D, Schwartz RE, Nixon DF. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID‐19 deaths in Italy. J Med Virol. 2020.
Grohskopf LA, Liburd LC, Redfield RR. Addressing Influenza Vaccination Disparities During the COVID-19 Pandemic. JAMA. 2020;324(11):1029.
Centers for Disease Control and Prevention. People at Increased Risk for COVID-19 (Coronavirus Disease). https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fneed-extra-precautions%2Fpeople-at-increased-risk.html
Department of Health and Mental Hygiene NYCDoHaMH EpiQuery. https://nyc.gov/health/epiquery Accessed 12 Nov 2020.
US Census Bureau. American Community Survey. 2018 American Community Survey 5-Year estimates. https://data.census.gov/cedsci/ Accessed 28 Apr 2020.
NYC Department of Health. ZCTA to MODZCTA Crosswalk. https://github.com/nychealth/coronavirus-data/blob/master/Geography-resources/ZCTA-to-MODZCTA.csv
New York City United Hospital Fund Codes. https://www1.nyc.gov/assets/doh/downloads/pdf/ah/zipcodetable.pdf
Dorn AV, Cooney RE, Sabin ML. COVID-19 exacerbating inequalities in the US. Lancet. 2020;395(10232):1243–4.
Carrión D, Colicino E, Pedretti NF, et al. Assessing capacity to social distance and neighborhood-level health disparities during the COVID-19 pandemic. In: Cold Spring Harbor Laboratory. 2020.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
AM: Conceptualization, methodology, data curation, writing- original draft preparation, visualization, investigation, software, validation. CG: conceptualization, investigation, writing- reviewing and editing, software, validation, data curation; AE: data curation. NA: conceptualization, investigation, writing- reviewing and editing, software, validation. ET: conceptualization, investigation, writing- reviewing and editing. All authors have approved the submitted version of this study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
available at the following:
1. New York City Department of Health and Mental Hygiene’s COVID-19 data repository at https://github.com/nychealth/coronavirus-data
2. New York City Department of Health and Mental Hygiene’s EpiQuery tool at https://nyc.gov/health/epiquery
3. US Census Bureau’s American Community Survey 5-year estimates at https://data.census.gov/cedsci/
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Moreland, A., Gillezeau, C., Eugene, A. et al. Ecologic study of influenza vaccination uptake and COVID-19 death rate in New York City. BMC Public Health 22, 1089 (2022). https://doi.org/10.1186/s12889-022-13515-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13515-z