
Abstract
Background
Having an unhealthy lifestyle is associated with a higher risk of developing lifestyle-related diseases. Current evidence suggests that interventions targeting health-risk behaviors can help people improve their lifestyles and prevent lifestyle-related diseases. However, preventive programs are often challenged by low participation rates. Reasons for non-participation include lack of time and/or interest, and/or no perceived need for lifestyle intervention. This study explores causes for non-participation in a sample of people who chose not to take up a targeted preventive program (TOF pilot2 study). Patient-reported reasons as well as sociodemographic characteristics and lifestyle factors are in focus.
Methods
A total of 4633 patients from four Danish GP clinics received an invitation to take part in the TOF pilot2 study. Patients who chose not to participate in the TOF pilot2 study were asked to fill in a questionnaire concerning reasons for non-participation, lifestyle, BMI and self-rated health. Descriptive analyses were used to summarize the results.
Results
A total of 2462 patients (53.1%) chose not to participate in the TOF pilot2 study. Among these, 84 (3.4%) answered the full questionnaire on reasons for not participating, lifestyle, BMI and self-rated health. The most common reasons for non-participation were lack of time, having an already healthy lifestyle, and feeling healthy. Based on their self-reported lifestyle 45 (53.6%) of the non-participants had one or more health-risk behaviors including smoking, unhealthy diet, BMI ≥ 35 and/or sedentary lifestyle and were therefore eligible to receive the targeted intervention at the GP or the MHC in the original TOF pilot2 study.
Conclusion
When planning future preventive programs it is important to know the main reasons for patients to not participate. This study provides rare insight into why people opt out of health interventions and advances the evidence base in this area. Our results may inform efforts to better involve these patients in preventive health programs.
Trial registration
Trial registration number: NCT02797392.
Similar content being viewed by others

Background
Health-risk behaviors such as smoking, alcohol consumption, sedentary behavior, and unhealthy diet are associated with increased risk of a range of lifestyle-related diseases, including type 2 diabetes (T2DM), cardiovascular disease (CVD), and chronic obstructive pulmonary disease (COPD) [1,2,3,4]. These diseases have high mortality rates and are especially prevalent in upper middle- and high-income countries [5]. Studies suggest that preventive lifestyle programs that target the at-risk population can help mitigate the development of lifestyle-related diseases [6, 7]. In Denmark primary disease prevention falls under the responsibility of the municipalities. General practitioners (GP) have a key role in preventive programs against lifestyle-related diseases as they are generally familiar with their patients and their social circumstances [8]. Nonetheless, preventive programs are often hampered by low participation rates and disproportionately high uptake among women, the elderly, as well as people with better health and higher socioeconomic status [9]. At a population level, this signifies important shortcomings in intervention design and reach. It also highlights the need for insight into why people who might benefit from preventive health programs decline invitations to participate [10].
Information about non-participating populations is important for the design of targeted and tailored interventions. However, only few studies report information about non-participants and their reasons for not participating [9, 11]. This study focuses on patient-reported reasons for non-participation, sociodemographic characteristics and self-reported lifestyle among non-participants in a targeted preventive health check intervention (TOF pilot2).
Methods
Setting and study design
The TOF pilot study 2 (TOF is a Danish acronym for Early Detection and Prevention) was conducted in the Region of Southern Denmark in collaboration with four GP clinics and two municipalities, Middelfart and Haderslev. In Denmark, primary disease prevention falls under municipal purview. Municipalities thus offer courses in smoking cessation and physical activity, dietary advice and treatment of alcohol addiction. Secondary disease prevention, such as preventive medical treatment and chronic disease management, is mainly undertaken by GPs. This study was conducted as a non-randomized feasibility study and included all eligible patients from the four GP clinics.
The intervention comprised a general intervention offered to all participants and a targeted intervention for those participants at high risk of lifestyle-related disease. As part of the general intervention, a personal digital health profile was created for each participant. The digital health profile was based on participant survey responses and information from the electronic patient records at the GP and offered information about risk of disease and advice for lifestyle changes. In addition to the health profile, the targeted intervention included a health assessment at the GP for high-risk patients and follow-up with treatment intervention at the GP, tailored health services at a municipal health center (MHC), or both. Or the offer of tailored health services at a MHC for patients with health-risk behavior [12, 13].
In October 2018, a total of 4633 patients from the four GP clinics received an invitation to take part in the study. Patients were eligible to participate if they were born between 1959–1988, lived in the municipalities of Haderslev or Middelfart, had a digital mailbox, and had not been invited to the first TOF pilot study (TOF pilot1). The invitation was sent on behalf of the GP and the MHC to patients’ digital mailboxes (e-Boks). A digital mailbox is a public Danish system for secure electronic communication between residents in Denmark and public authorities and other trusted organizations (e.g., banks) [14].
The invitation contained a link to a password-protected personal website with information about the study and a consent form. Non-response triggered up to two reminders with two interval. The initial invitation as well as the reminders contained a link to a questionnaire for those patients who chose not to take part in the study (non-participation questionnaire). Participation was voluntary and patients were informed that non-participation had no influence on their treatment options.
Development of the non-participation questionnaire
Question on reasons for non-participation
Initially, 17 reasons for non-participation were formulated by the research group. The items were based on current evidence about patient-reported factors for attendance and non-attendance at preventive health checks [15,16,17,18]. The items covered project-related as well as personal and practical factors.
Patient and public involvement
The questions were tested for comprehensibility, relevance, and coverage by target group representatives. Men and people with low educational level were purposely sampled as these subgroups of the general population are particularly likely to decline preventive interventions [9, 11, 13, 19]. The recruitment strategy centered on Facebook and Instagram ads. In addition, attendees at a Meeting Place for Men (a social connectedness initiative for men) in the town of Sønderborg were contacted directly. Ultimately, 10 citizens aged 34–57 (three women, seven men) were recruited. Eight participants had no formal education beyond elementary school, one was a primary school teacher, and one was a printmaker [13].
An invitation to the TOF pilot study 2 and the questionnaire draft were sent by mail to the target group representatives. Group members were instructed to imagine that they received the invitation to participate in TOF Pilot2 study and decided not to participate. They were then instructed to access the non-response questionnaire by clicking a link in the invitation, “If you do not want to participate, please click here and let us know why”. Group members were asked to indicate if any of the questions overlapped and invited to suggest inclusion of additional questions. The questions were adjusted accordingly, and one option on reasons for non-participation were added which was “I am already in treatment for a lifestyle-related disease”.
Beyond reasons for non-participation, the questionnaire contained items on lifestyle, BMI and self-rated health. Questions on physical activity were adapted from the Danish Diabetes Risk model [20]. Questions on smoking status were derived from the COPD-PS screener [21] and the Heartscore BMI score [22]. Diet was assessed with the Swedish National Guidelines on Disease Prevention [23], and alcohol consumption was gauged according to official Danish recommendations for low-risk alcohol consumption [24].
Hence the final questionnaire contained 11 questions all of which made use of non-forced answers. (for resulting questionnaire see additional file 1).
Analysis
Information on health-risk behavior (smoking status, alcohol consumption, physical activity, diet and BMI) were dichotomized. Smoking status was defined in terms of current smoking status (yes/no). ‘Current smoker’ included daily and occasional smokers while ‘non-smoker’ referred to people who had quit smoking or never smoked [12]. Alcohol consumption was divided into low-risk or high-risk alcohol consumption (> 14 and 21 units/week for women and men, respectively [24]). Level of physical activity was dichotomized into ‘sedentary’ and ‘physically active activities during leisure time’. Activity during leisure time was defined as four hours or more of low- to high-intensity leisure-time activity (gardening, walking the dog, cycling, etc.) a week. Sedentary leisure time was defined as reading, watching television or other sedentary activities. Diet was dichotomized as unhealthy diet or otherwise. Unhealthy diet was measured as a score of four or lower on a 12-point dietary scale [23]. The respondents were asked to type in their height and weight. Respondent BMI was then calculated and categorized as either BMI < 35 or BMI ≥ 35. Self-rated health was assessed by the following question “In general, would you say your health is”: Excellent (1), Very good (2), Good (3), Fair (4) or Poor (5). This was dichotomized into “Excellent, Very good or Good self-rated health” and “Fair or Poor self-rated health”.
Register information
Patient demographic information on sex, age, country of origin, educational level, occupational status, and family income was retrieved from the Danish National Bureau of Statistics (Statistics Denmark) for the entire study population and linked at the individual level.
Age was determined at the time of invitation and categorized in 10-year age brackets (29–39, 40–49, 50–60). Country of origin was retrieved for the year 2018 and categorized as Danish, Western, or Non-western origin. Highest attained educational level was retrieved for October 2018 and categorized into five groups: Secondary school, High school, Vocational education, Higher education, and Higher education – master’s level. Educational level was then dichotomized into ‘highest educational level: “secondary school”, or “High school, vocational education, higher education and higher education – master level”. Employment status was retrieved for November 2018 and categorized according to the equivalence scales into five categories: Employed, Self-employed, Unemployed/on benefits, social welfare recipients, and other. The category “other” represents, for instance, unemployed persons from a family that relies on one income only [13]. Employment status was dichotomized as “unemployed/on benefits, social welfare recipients or other”, and “employed or self-employed”. Family income was retrieved for 2013–2018, defined by the mean annual net income of the household, and categorized into quartiles. Subsequently, family income was dichotomized (Low income: 1 = lowest quartile, 0 = above lowest quartile) [12, 13].
Statistical analyses
Descriptive analysis was used to summarize the patient’s demographic characteristics, their reasons for non-participation, smoking, alcohol consumption, diet, physical activity, BMI and their self-rated health. To examine the differences in demographic characteristics between non-participants who answered the non-participation questionnaire and those who did not, univariate and multivariate logistic regression analyses were performed. In the multivariate logistic regression analyses the demographic characteristics were adjusted for gender and age. Missing values were excluded in the analyses. Odds Ratios (crude and adjusted), p-values with a 0.05 significance level and 95% confidence intervals were reported. Stata version 16.0 was used for the analyses.
Results
Of the 4633 patients who were invited to the TOF pilot2 study, 2462 (53.1%) chose not to participate [13]. Of these, 93 (3.8%) answered some or all of the questions in the non-participation questionnaire. Eighty-four (3.4%) (men = 37 and women = 47) answered the questions on reasons for non-participation as well as questions on lifestyle, BMI and self-rated health (Fig. 1).

Flowchart of the TOF pilot2 study population
Characteristics of non-participants compared to participants
The proportion of men was higher among non-participants than participants. Further non-participants were younger, more likely to be of Western or Non-Western origin, and more likely to have secondary school as their highest educational attainment. In terms of SES, non-participants were more likely than participants to be in the lowest income quartile and more likely to be unemployed/on benefits/social welfare recipients than their participating counterparts (additional file 2).
Characteristics of responders and non-responders to the non-participation questionnaire
Table 1 shows the demographic characteristics of non-participants who answered the non-participation questionnaire (responders) and non-participants who did not (non-responders). Responders were older and more likely to be women but did not differ significantly from non-responders with regard to country of origin, level of education, occupational status, or family income (Table 1).
Reasons for non-participation
Reported reasons for non-participation
The reported reasons for not participating in the TOF pilot study 2 are shown in Table 2 and divided into the following overarching categories (bold in the table): Time constraints; No perceived need for a health check; Unclarity of the program; Privacy concerns; Do not want to know results/fear of bad results; Do not want to participate because of the program/parts of the program; and Already in treatment. The most common specific reasons for not participating were lack of time (n = 25 (29.8%)), having a healthy lifestyle (n = 24 (28.6%)), and feeling healthy (n = 20 (23.8%)). For men, the most frequently reported reason was lack of time (n = 13 (35.1%)), whereas for women it was having a healthy lifestyle (n = 17 (36.2%)). Only very few (< 5) respondents cited fear of a negative health check result as a reason for not participating. No patients reported that they were either too young or too old to benefit from a health check.
The respondents were also given the opportunity to report their own reason for not participating Twenty-eight patients used this option and the reasons reported were grouped into broader categories: “Already diagnosed with a chronic disease” (n = 5), “Does not want to participate” (n = 5), “Does not have the energy to participate (n = 4), Receives regular health checks at GP” (n = 3), “Technical difficulties with questionnaire (n = 2), Geographical reasons (n = 2), “Does not perceive themselves as in need for a health check” (n = 2), “Not satisfied with GP´s in general” (n = 2), “Fear of being stigmatized” (n = 1), “Cannot participate because of poor mobility” (n = 1) and “Privacy concerns” (n = 1).
Perceived need for health check, health behavior, and BMI
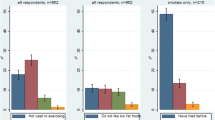
Of the responders who answered the questions on lifestyle (n = 91), 21 (23.1%) were current smokers, 14 (15.4%) had an unhealthy diet, 17 (18.7%) had a sedentary lifestyle, and none had high-risk alcohol intake. Among the participants who answered the questions on BMI and self-rated health (n = 89), 10 (11.2%) had a BMI ≥ 35 and 16 (18%) had fair or poor self-rated health.
Table 3 shows the proportion of patients with health-risk behaviors and fair or poor self-rated health among the non-participant respondents with no perceived need for a health check (n = 46) compared to respondents reporting other reasons for non-participation (n = 38)(See Table 2). We include this information to provide a sense of those responders who chose not to participate because they perceived no need to do so, but who nonetheless represent the target group for the intervention by virtue of their health-risk behaviors.
The number of patients with one or more health risk behaviors were slightly lower among patients with no perceived need for at health check (45.7%), than among patients reporting other reasons for non-participation (63.2%). In total, 45 (53.6%) of the respondents had one or more health-risk behaviors and were therefore eligible to receive the targeted intervention at the GP or the MHC.
Discussion
The aim of this study was to examine patient-reported reasons for non-participation as well as sociodemographic characteristics and self-reported lifestyle among non-participants in the TOF pilot 2 study.
Of the patients invited to take part in the study, about half declined. Consistent with many other studies focusing on health-check interventions [9, 11, 19, 25,26,27], non-participants differed from the participants by being disproportionately male, younger, and with lower SES.
Responders (i.e., non-participants who answered the questions on reasons for non-participation) were comparable to non-participants on all sociodemographic characteristics except gender and age. The main findings of the study are discussed below.
Time constraints
The most common reason cited for non-participation was a lack of time (29.8%). This resonates with previous findings [15, 16, 18]. People in the work force have previously reported lack of time because of a busy work schedule as a barrier to exercise [28] and maintaining a healthy diet [29]. Therefore, as the target group of the present study comprised working-age patients (29–60 years), time constraints related to a busy work schedule most likely also influenced the likelihood of intervention uptake. A possible solution to reach people in the work force could be to implement preventive programs at workplaces. Indeed, recent workplace interventions have shown promising results in terms of physical activity, dietary behavior, healthy weight [30], smoking cessation [31], and cardiovascular-disease-risk reduction [32].
A notable finding from our study concerns the fact that almost 30% of non-participants were unemployed/on benefits. The existing literature concerning time constraints as a reason for non-participation has not included a specific focus on the unemployed. But a study that investigated reasons for non-participation in a health promotion program targeting low-income households, including unemployed, reports circumstances such as family illness as a barrier for participation [33].
Mismatch between perceived and actual risk
The reasons “I already have a healthy lifestyle” and “I feel healthy” are the second and third most frequent reasons provided by non-participants. Indeed, 40.5% of the patients reported one or both, which makes this the most cited reason for non-participation. Consistent with these results, other studies have reported the feeling of healthiness as a factor in non-participation [9, 18]. To have a healthy lifestyle or to feel healthy is a subjective assessment and it is possible that their risk perception of developing a lifestyle-related disease is inaccurate. Previous studies have shown a mismatch between actual risk and risk perception of developing lifestyle-related diseases where participants’ perceived risk was lower than the actual risk [8, 34, 35]. The results of present study indicate that 21 (45.7%) non-participants perceived no need for a health check, but nonetheless had one or more health-risk behaviors. In the TOF pilot study 2 these patients would have received an offer of a targeted intervention at the GP or the MHC. Though it is challenging to reach out to patients who already feel healthy, even though they show health-risk behavior, it is important as such patients might not engage in the necessary lifestyle changes. A possible solution could be for health professionals to educate their patients about actual and perceived risk of health behaviors [36]. It may be challenging to get patients who believe that they are healthy to seek out and engage in such education. However, previous studies have indicated that completing an online risk calculator with a health care professional, who can help interpret the results in the context of patient preferences, needs and expectations, is preferable among patients [36,37,38].
Unclarity of the program
Confusion about the aim and content of the intervention was reported by 20.2% of the non-participants. This aligns with another study in which lengthy and ambiguous information about the intervention represented a key barrier for uptake and participation [39]. That study recommended shortening participant information as much as possible, but recognized that this might be difficult as ethics committees generally require specific and wordy details to be incorporated into participant information [39].
Privacy concerns
The reasons “I do not want my medical records to be shared with the research team” and “I am concerned that others will get access to the results e.g., insurance companies” were reported as reasons for non-participation by 14.3% and 10.7%, respectively. Patient medical records are generally perceived as more private than other types of personal information, and patients may therefore be less likely to disclose this information [40, 41]. Patients may worry their information could end up in the wrong hands, such as insurance companies [41, 42]. One study indicated that participants were willing to disclose health information in their physicians office [41] and even though it could also be a possibility in this program it would be a lot more time consuming and resource demanding compared to the current set up.
Do not want to know results/Fear of bad results
Both of the reasons “Participation in this intervention will make me unnecessarily nervous” and “I do not want to know my risk of developing a lifestyle disease” were reported as reasons for non-participation by 13.1% of respondents. Similar results are evident in other studies regarding attendance at GP health checks [43,44,45]. More direct and clear communication from the GP concerning risk behavior and the importance of health checks may mitigate this level of willful ignorance and galvanize the patient into preventive action. Indeed, previous studies show that non-responders seems to value a personal approach about their own risk perception from the GP [46].
Do not want to participate because of the program/parts of the program
Reasons as “I do not believe the intervention can help me get a healthier lifestyle” and “I do not like others interfering with my lifestyle” were reported as reasons for non-participation by 11.9% and 10.7%, respectively. Several factors could underly these reasons for non-participation, including for example, dissatisfaction with the specific program design or operation – an issue seen in a previous study [9]. However, given the fundamental nature of these two reasons for non-participation – that is, disbelief in the efficacy of the intervention, and a more general rejection of outside interference with one’s lifestyle – persuading this subgroup to participate would presumably always be a hard sell. Still, as mentioned earlier a personal approach from the GP should be explored further as a possible solution to increase participation within this group [46].
Strengths and limitations
A strength of this study is the involvement and response from a group that is usually hard to reach (i.e., non-participants). The reasons for not participating in a preventive program targeting lifestyle-related diseases is a key factor in the implementation of current and future preventive programs.
While the low response rate of 3.8% is a clear limitation to the external validity of the present study, we emphasize the fact that non-responders and responders to the non-participation questionnaire were comparable on most of the measured demographic parameters including country of origin, level of education, occupational status and family income. This suggests that despite the low response rate, responders are at least somewhat representative of the population of interest. Nonetheless, there is a possibility that this study could be subject to selection bias as responders to the non-participation questionnaire may differ systematically from the other non-responders on other factors than demographic ones. For instance, the digital nature of the non-response questionnaire might represent a barrier for people who lack the necessary IT skills and literacy. This was also considered a limiting factor of the TOF pilot1 study [47]. Further, questionnaire respondents may have had a more positive attitude towards participation in the TOF pilot study 2 than other non-participants. This could influence the results concerning reasons for non-participation and maybe over -or underestimate some of the reasons. This factor and the low response rate was also reported in a recent similar study [46]. Furthermore, the questionnaire was self-reported which could cause recall bias and/or information bias as there is a possibility that the patients do not remember or misunderstand some of the questions.
Another limitation relates to the fact that this study did not measure non-participants willingness to participate in future preventive programs against lifestyle-related diseases. Therefore, we cannot know if the reservations described only pertained to the current set up or point in time.
Implications
Although the GPs were very much involved in the design and planning of the TOF intervention the results in this study could indicate that there is still room for improvement. The existing literature indicate that participation rates may increase if the GP plays a bigger role in the intervention. Both regarding the invitation process as non-responders seems to value a personal approach from the GP but also to establish a dialogue on actual risk and risk perception of health behavior with the patients as there seems to be mismatch [8]. By doing this, patients might be better suited to assess the actual health risks associated with their behavior. In turn, this might encourage them to change their lifestyle – for example by participating in a preventive program.
As the most common reason for non-participation relates to time constraints, a program that could be implemented at workplaces might increase participation rates. Regarding the current set up it should be a possibility for people to receive offers of a targeted intervention at the GP or the MHC out of office hours. Furthermore, given the large proportion of unemployed non-participants, a program targeting the unemployed could be a solution for reaching this group more effectively. In terms of future similar health promotion programs our results, regarding time constraints being the most common reason, suggests that it is important to remove structural barriers and create an environment in which it becomes possible or easier for the individual to participate.
Finally, to better understand the reasons for non-participation, a qualitative study would conceivably provide a wider and richer perspective on the underlying reasons for non-participation. Knowledge about the reasons for non-participation is not exhaustive and warrants further evidence in order to target the population who may benefit from preventive interventions.
Conclusion
In the present study, the most common reasons for non-participation in a targeted preventive health check intervention were “time-constraints” and “already feels healthy”. However, regarding the reason “already feels healthy”, results on the patients lifestyle indicates that patients at risk for lifestyle diseases do not perceive themselves as being at risk so there might be an incongruence between perceived risk and actual risk.
Our results extends existing knowledge on reasons for non-participation and highlights future areas of research.
Availability of data and materials
The data that support the findings of this study are not publicly available. Data will however be available from the authors upon reasonable request and with permission from the Danish Data Protection Agency. If data from this study is requested please contact Christian Leick.
Abbreviations
- BMI:
-
Body mass Index
- COPD:
-
Chronic obstructive pulmonary disease
- CVD:
-
Cardiovascular disease
- GP:
-
General practitioner
- MHC:
-
Municipal health center
- T2DM:
-
Type 2 diabetes
- TOF:
-
TOF is a Danish acronym for Early Detection and Prevention (in Danish: Tidlig Opsporing og Forebyggelse)
References
Klatsky A. Alcohol and cardiovascular diseases: where do we stand today? J Intern Med. 2015;278(3):238–50.
Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2011;2(2):1143–211.
Sami W, Ansari T, Butt NS, Ab Hamid MR. Effect of diet on type 2 diabetes mellitus: A review. Int J Health Sci. 2017;11(2):65.
US Department of Health, Human Services. The health consequences of smoking—50 years of progress: a report of the Surgeon General. Atlanta GA: US Department of Health and Human Services, Centers for Disease; 2014.
Mathers C, Stevens G, Hogan D, Mahanani WR, Ho J. Global and regional causes of death: patterns and trends, 2000–15. 2017.
Ambrosino N, Bertella E. Lifestyle interventions in prevention and comprehensive management of COPD. Breathe. 2018;14(3):186–94.
Schellenberg ES, Dryden DM, Vandermeer B, Ha C, Korownyk C. Lifestyle interventions for patients with and at risk for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2013;159(8):543–51.
Badenbroek IF, Nielen MM, Hollander M, Stol DM, de Wit NJ, Schellevis FG. Characteristics and motives of non-responders in a stepwise cardiometabolic disease prevention program in primary care. Eur J Public Health. 2021;31(5):991–96.
Groeneveld IF, Proper KI, van der Beek AJ, Hildebrandt VH, van Mechelen W. Factors associated with non-participation and drop-out in a lifestyle intervention for workers with an elevated risk of cardiovascular disease. Int J Behav Nutr Phys Act. 2009;6(1):80.
Cheung KL, Peter M, Smit C, de Vries H, Pieterse ME. The impact of non-response bias due to sampling in public health studies: a comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health. 2017;17(1):1–10.
Lakerveld J, IJzelenberg W, Van Tulder MW, Hellemans IM, Rauwerda JA, Van Rossum AC, et al. Motives for (not) participating in a lifestyle intervention trial. BMC Med Res Methodol. 2008;8(1):17.
Larsen LB, Sonderlund AL, Sondergaard J, Thomsen JL, Halling A, Hvidt NC, et al. Targeted prevention in primary care aimed at lifestyle-related diseases: a study protocol for a non-randomised pilot study. BMC Fam Pract. 2018;19(1):124.
Thilsing T, Larsen LB, Sonderlund AL, Andreassen SS, Christensen JR, Svensson NH, et al. Effects of a Co-Design-Based Invitation Strategy on Participation in a Preventive Health Check Program: Randomized Controlled Trial. JMIR Public Health Surveill. 2021;7(3):e25617.
Agency for Digitisation. MoF. https://digst.dk/it-loesninger/digital-post/om-loesningen/2021 04/03/2021. Available from: https://digst.dk/it-loesninger/digital-post/om-loesningen/.
Murray J, Craigs CL, Hill KM, Honey S, House A. A systematic review of patient reported factors associated with uptake and completion of cardiovascular lifestyle behaviour change. BMC Cardiovasc Disord. 2012;12(1):120.
Harte E, MacLure C, Martin A, Saunders CL, Meads C, Walter FM, et al. Reasons why people do not attend NHS Health Checks: a systematic review and qualitative synthesis. Br J Gen Pract. 2018;68(666):e28–35.
Toft UN, Kristoffersen LH, Aadahl M, von Huth SL, Pisinger C, Jørgensen T. Diet and exercise intervention in a general population—mediators of participation and adherence: the Inter99 study. Eur J Pub Health. 2007;17(5):455–63.
Petter J, Reitsma-van Rooijen MM, Korevaar JC, Nielen MM. Willingness to participate in prevention programs for cardiometabolic diseases. BMC Public Health. 2015;15(1):44.
Chien S-Y, Chuang M-C, Chen I. Why people do not attend health screenings: Factors that influence willingness to participate in health screenings for chronic diseases. Int J Environ Res Public Health. 2020;17(10):3495.
Christensen J, Sandbæk A, Lauritzen T, Borch-Johnsen K. Population-based stepwise screening for unrecognised Type 2 diabetes is ineffective in general practice despite reliable algorithms. Diabetologia. 2004;47(9):1566–73.
Martinez FJ, Raczek AE, Seifer FD, Conoscenti CS, Curtice TG, D’Eletto T, et al. Development and initial validation of a self-scored COPD Population Screener Questionnaire (COPD-PS). J Chron Obstruct Pulmon Dis. 2008;5(2):85–95.
European Society of Cardiology. Heartscore webpage [Available from: http://www.heartscore.org/en_GB/.
Socialstyrelsen S. Sjukdomsförebyggande metoder Vetenskabeligt underlag för nationella riktlinjer Svenska Socialstyrelsen. 2011.
Danish Health Authority. Sundhedsstyrelsens udmeldinger om alkohol 2019 [cited 2020 Nov 24.]. Available from: https://www.sst.dk/da/viden/alkohol/alkoholforebyggelse/sundhedsstyrelsens-udmeldinger-om-alkohol.
Wigertz A, Lönn S, Hall P, Feychting M. Non-participant characteristics and the association between socioeconomic factors and brain tumour risk. J Epidemiol Community Health. 2010;64(8):736–43.
Hertzum-Larsen R, Kjær SK, Frederiksen K, Thomsen LT. Participation in cervical cancer screening among immigrants and Danish-born women in Denmark. Prev Med. 2019;123:55–64.
Schinkel S, Schouten BC, Kerpiclik F, Van Den Putte B, Van Weert JC. Perceptions of barriers to patient participation: Are they due to language, culture, or discrimination? Health communication. 2018.
Nielsen JB, Leppin A, e Gyrd-Hansen D, Jarbøl DE, Søndergaard J, Larsen PV. Barriers to lifestyle changes for prevention of cardiovascular disease–a survey among 40–60-year old Danes. BMC Cardiovasc Disord. 2017;17(1):245.
Seguin R, Connor L, Nelson M, LaCroix A, Eldridge G. Understanding barriers and facilitators to healthy eating and active living in rural communities. J Nutr Metab. 2014;2014:146502.
Schröer S, Haupt J, Pieper C. Evidence-based lifestyle interventions in the workplace—an overview. Occup Med. 2014;64(1):8–12.
Cahill K, Lancaster T. Workplace interventions for smoking cessation. Cochrane Database Syst Rev. 2014;(2):CD003440.
Groeneveld IF, Proper KI, van der Beek AJ, Hildebrandt VH, van Mechelen W. Lifestyle-focused interventions at the workplace to reduce the risk of cardiovascular disease-a systematic review. Scand J Work Environ Health. 2010;36(3):202–15.
Nagelhout GE, Abidi L, de Vries H. Reasons for (not) participating in a community-based health promotion program for low-income multi-problem households in the Netherlands: A qualitative study. Health Soc Care Community. 2021;29(1):241–9.
Homko CJ, Santamore WP, Zamora L, Shirk G, Gaughan J, Cross R, et al. Cardiovascular disease knowledge and risk perception among underserved individuals at increased risk of cardiovascular disease. J Cardiovasc Nurs. 2008;23(4):332–7.
Azahar N, Ismail Z, Hassan R, Yusoff K. PS 15–01 Mismatch between actual risk and perceived risk for cardiovascular disease among elderly in a rural population of Malaysia. J Hypertens. 2016;34: e459.
Stol DM, Hollander M, Damman OC, Nielen MM, Badenbroek IF, Schellevis FG, et al. Mismatch between self-perceived and calculated cardiometabolic disease risk among participants in a prevention program for cardiometabolic disease: a cross-sectional study. BMC Public Health. 2020;20:1–9.
Nolan T, Dack C, Pal K, Ross J, Stevenson FA, Peacock R, et al. Patient reactions to a web-based cardiovascular risk calculator in type 2 diabetes: a qualitative study in primary care. Br J Gen Pract. 2015;65(632):e152–60.
Damman O, van der Beek A, Timmermans D. Employees are ambivalent about health checks in the occupational setting. Occup Med. 2015;65(6):451–8.
Attwood S, Morton K, Mitchell J, Van Emmenis M, Sutton S. Reasons for non-participation in a primary care-based physical activity trial: a qualitative study. BMJ Open. 2016;6(5):e011577.
Metzger MJ. Privacy, trust, and disclosure: Exploring barriers to electronic commerce. J Computer-Mediated Commun. 2004;9(4):JCMC942.
Caine KE, Burnham KE, Fisk AD, Rogers WA, editors. Privacy concerns and disclosure behavior in a health setting. Proceedings of the Human Factors and Ergonomics Society Annual Meeting; 2008: SAGE Publications Sage CA: Los Angeles, CA.
Westin AF. The Dimensions of Privacy: A National Opinion Research Survey of Attitudes Toward Privacy. 1979.
Jenkinson CE, Asprey A, Clark CE, Richards SH. Patients’ willingness to attend the NHS cardiovascular health checks in primary care: a qualitative interview study. BMC Fam Pract. 2015;16(1):1–10.
Burgess C, Wright AJ, Forster AS, Dodhia H, Miller J, Fuller F, et al. Influences on individuals’ decisions to take up the offer of a health check: a qualitative study. Health Expect. 2015;18(6):2437–48.
Engebretson J, Mahoney JS, Walker G. Participation in community health screenings: a qualitative evaluation. J Community Health Nurs. 2005;22(2):77–92.
Badenbroek IF, Nielen MM, Hollander M, Stol DM, Drijkoningen AE, Kraaijenhagen RA, et al. Mapping non-response in a prevention program for cardiometabolic diseases in primary care: How to improve participation? Preventive Medicine Reports. 2020:101092.
Larsen LB, Sondergaard J, Thomsen JL, Halling A, Sønderlund AL, Christensen JR, et al. Step-wise approach to prevention of chronic diseases in the Danish primary care sector with the use of a personal digital health profile and targeted follow-up–an assessment of attendance. BMC Public Health. 2019;19(1):1–14.
Acknowledgements
The authors wish to thank the patients, GPs, and municipal health professionals who took part in the study.
Funding
The study received funding from Trygfonden (grant no 125508), The Committee of Quality and Education in General Practice in the Region of Southern Denmark (grant no 18/527), The Region of Southern Denmark (grant no 11/13244) and The Fund for General Practice (grant no A2804). The sponsors had no involvement in the review or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
LBL, ALS, NHS, JS and TT participated in the design of the study. CL and TT interpreted the data and CL was the main contributor to the manuscript. LBL, ALS, NHS and JS contributed to the interpretation of the data and LBL, ALS, NHS, JS and TT contributed to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Research & Innovation Organisation (RIO) at the University of Southern Denmark (18/32742), and the TOF pilot study 2 was registered at ClinicalTrial.gov (NCT03913585) (13). According to Danish regulations (Act on Research Ethics Review of Health Research Projects [Sect. 14.2]), this study did not need approval from a health research ethics committee as no research on human tissue or other biological material was performed. This was confirmed in writing by the Regional Committee on Health Research Ethics for Southern Denmark (J.nr. S-20152000–28).
The study complies with the Helsinki declaration with informed written consent to study participation and to disclosure of data from the GPs EPR from all participants before enrolment. Participants were asked to read the information and electronically sign the consent form. Written information was supplemented with short videos describing the purpose of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Questionnaire.
Additional file 2.
Characteristics of non-participants compared to participants.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Leick, C., Larsen, L.B., Larrabee Sonderlund, A. et al. Non-participation in a targeted prevention program aimed at lifestyle-related diseases: a questionnaire-based assessment of patient-reported reasons. BMC Public Health 22, 970 (2022). https://doi.org/10.1186/s12889-022-13382-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13382-8