
Abstract
Background
By explaining the development of health inequalities, eco-social theories highlight the importance of social environments that children are embedded in. The most important environment during early childhood is the family, as it profoundly influences children’s health through various characteristics. These include family processes, family structure/size, and living conditions, and are closely linked to the socioeconomic position (SEP) of the family. Although it is known that the SEP contributes to health inequalities in early childhood, the effects of family characteristics on health inequalities remain unclear. The objective of this scoping review is to synthesise existing research on the mediating and moderating effects of family characteristics on socioeconomic health inequalities (HI) during early childhood in high-income countries.
Methods
This review followed the methodology of “Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews”. To identify German and English scientific peer-reviewed literature published from January 1st, 2000, to December 19th, 2019, the following search term blocks were linked with the logical operator “AND”: (1) family structure/size, processes, living conditions, (2) inequalities, disparities, diversities, (3) income, education, occupation, (4) health and (5) young children. The search covered the electronic databases PubMed, PsycINFO, and Scopus.
Results
The search yielded 7,089 records. After title/abstract and full-text screening, only ten peer-reviewed articles were included in the synthesis, which analysed the effects of family characteristics on HI in early childhood. Family processes (i.e., rules /descriptive norms, stress, parental screen time, parent–child conflicts) are identified to have mediating or moderating effects. While families’ living conditions (i.e., TVs in children’s bedrooms) are suggested as mediating factors, family structure/size (i.e., single parenthood, number of children in the household) appear to moderate health inequalities.
Conclusion
Family characteristics contribute to health inequalities in early childhood. The results provide overall support of models of family stress and family investment. However, knowledge gaps remain regarding the role of family health literacy, regarding a wide range of children’s health outcomes (e.g., oral health, inflammation parameters, weight, and height), and the development of health inequalities over the life course starting at birth.
Similar content being viewed by others


Background
Extensive evidence demonstrates the existence of health inequalities across the entire course of life [1–5]. Early childhood, however, has been found to be particularly relevant for the development of health behaviour and for health in the long-term [2]. This life stage spans several age groups, including newborns (birth to 1 month), infants (1 month to 1 year), toddlers (1 year to 2 years), and preschoolers (2 years to 6 years) [6]. Health in early childhood depends on the families’ socioeconomic position (SEP), which is commonly operationalised by parental education, occupation and/or income. In general, socioeconomically disadvantaged children show disproportionately poorer health outcomes compared to children from families with a higher SEP. For example, children under the age of six from families with a lower SEP are more likely to have asthma, a delayed cognitive development, a higher prevalence of overweight/obesity, and lower levels of physical activity [7–11].
The circumstances and pathways by which SEP affects children’s health are complex. Over the last two decades, explanatory theories of health inequalities have increasingly considered eco-social perspectives [12, 13]. For example, Krieger’s eco-social theory (2001) posits that the human embodiment of health inequalities results from interactions between biological processes and the social environments humans inhabit [13, 14]. Individual health outcomes, therefore, cannot be understood independently from social environments. In early childhood, the characteristics of the family as the most important surrounding profoundly influences children’s health [15, 16]. For example, marital status, parenting styles and family living conditions are associated with health in this age group [17–19]. Various studies indicate that stressful parental partnerships, incoherent parenting practices, and unfavourable parental health behaviour are more frequently observed among families with lower SEP [20–23]. Following these eco-social perspectives, it can be assumed that the embodiment of health inequalities may result from a dynamic interplay between individuals and families’ characteristics such as processes (e.g., parenting, parental collaborating), structures/size (e.g., marital status), and living conditions.
To seek for explanatory mechanisms, two frequently cited models follow assumptions of social causation [24]. First, the family stress model (FSM) proposes that economic hardship (e.g., low income, job loss) aggravates parents’ psychological distress (e.g., hopelessness, hostility) which leads to inter-parental conflicts. This may, in turn, influence health outcomes in early childhood through inconsistent or harsh parenting practices [24, 25]. Second, the family investment model (FIM) focuses on the economic, educational, and occupational circumstances of a family that determine the resources parents can invest in their children. These investments contribute to children’s development and health in early childhood and later life. The dimensions of parental investment may be as manifold as follows: behaviour (e.g., parent–child time spent, promotion of extracurricular activities), nutrition (e.g., sufficiently nutritious diets), education (e.g., learning materials available at home), health behaviour and health (e.g., utilization of medical care, parental health behaviour, rules restricting of media use), and living conditions (e.g., residence) [25–28]. The FIM and FSM reflect theoretical assumptions of family’s mechanisms underlying health inequalities, which only have been studied with regard to few health conditions among children [29]. However, in line with the assumptions of social causation (e.g., FSM, FIM), family characteristics could depend on the SEP which, in turn, affects children’s health (defining mediating effects). Family characteristics might also affect the association between SEP and children’s health (defining moderating effects) [30].
Although it is known that family SEP determines differences in health outcomes and influences family characteristics, the specific pathways by which family SEP affects health behaviour and health in early childhood in high-income countries remain unclear [31]. Therefore, the objective of this scoping review was to synthesise the extent, the nature, the results, and the knowledge gaps of existing research on families’ characteristics underlying health inequalities by exploring:
-
(1)
which family characteristics mediate the association between SEP and health of young children (mediating effects), and
-
(2)
which family characteristics moderate the association between SEP and health of young children (moderating effects).
Methods
Scope of the search
This scoping review synthesised qualitative and quantitative research on the mediating and moderating effects of family characteristics (context) on health inequalities (concept) in early childhood (population) in high-income countries. The objective was conceptualised by the key elements of population, concept, and context [32]. To assess the scope of the research on the topic of interest, the methodology for this scoping review was based on the checklist outlined by Tricco et al. (2018): “Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews” (PRISMA Extension for Scoping Reviews) [33]. The review protocol was published a priori [34].
Figure 1 illustrates the key elements to conceptualise the research objectives of the scoping review that are based on the Population/Concept/Context framework. The core concept pertains to health that depends on the socioeconomic position (SEP) of the family, which is operationalised by parental education, occupation and/or income. The review considered manifold outcomes in health and development in the early childhood (0–6 years, population). The context encompasses the family as the most important surrounding of young children, which has different structures, processes and conditions.

Conceptual Framework of the Scoping Review
Identification in systematic search
As outlined in the review protocol [34], the search strategy was applied to PubMed, PsycINFO (via EBSCO), and Scopus to identify German and English scientific literature published from January 1st, 2000, to December 19th, 2019 following the PRISMA Extension for Scoping Reviews [33]. The database selection was based on the specific content coverage of peer-reviewed articles within Biomedical and Life Sciences (PubMed), Behavioural Sciences and Mental Health (PsycINFO), and Health Sciences and Education (Scopus).
Search terms were based on key elements of the review objectives that were integrated in the conceptual framework of this scoping review (Fig. 1). Search terms covered free-text words, subject classifications, such as medical subject headings (PubMed) and index terms (PsycINFO) [35]. In order to ensure quality, search terms were refined and checked in consideration of existing guidelines [36].
The following five search term blocks were designed and linked with the logical operator “AND” to explore the review objective:
-
Context: Family characteristics
-
Family structure and size, family processes, family living conditions
-
-
Concept: SEP related inequalities in health outcomes
-
Inequalities, disparities, diversities
-
Socioeconomic position, income, education, occupation
-
Health behaviour, health, development, mortality
-
-
Population: Early childhood
-
Newborn, infant, toddler, preschooler, child
-
The search strategy was first developed for PubMed and then adapted for use in PsycINFO and Scopus. An outline of the database-specific search strategy was published elsewhere [34].
Screening and eligibility criteria
The two-step data screening included content screening of titles and abstracts, followed by a full-text screening of the remaining articles. After the elimination of duplicates, two reviewers independently completed the first step (SH, MB), as well as the second step (SH, LS). In the case of contradictory decisions, agreement was reached via discussion between the two reviewers or consultation with a third researcher (JS) with sufficient expertise. To assess inter-observer bias, generalised kappa-type statistics [37] were calculated for both title/abstract screening and full-text screening. To ensure that the reviewers interpreted eligibility criteria similarly, 100 abstracts were randomly selected and jointly discussed.
Peer-reviewed journal articles were included, if they reported on key dimensions of the review objectives. Studies were included, if they described family characteristics (context), such as family structure/size, family processes, family living conditions or parental characteristics (e.g., health literacy) [19, 23, 38–40]. To identify health inequalities (concept), all articles had to consider differences in families’ education, income or occupation [41] that influence health outcomes. These were operationalised by health behaviour, utilisation of the healthcare system, health, etiology of communicable and non-communicable diseases, birth outcomes (e.g., birthweight), development, well-being, or mortality in early childhood (0 to 6 years) (population). Furthermore, studies were only included if they had been conducted in high-income countries as defined by the United Nations [31], and published between 01.01.2000 and 19.12.2019 in German or English. According to the scoping review methodology [33], studies with various designs (e.g., cross-sectional studies, longitudinal studies, qualitative studies, and reviews) were eligible for inclusion. Articles were included, if data analyses strived for exploring family characteristics underlying early health inequalities (e.g., moderator analyses, mediator analyses, qualitative analyses [30, 42]. Data analyses were also sufficient for inclusion, if they were reported descriptively (e.g., in reviews) or were represented exclusively in figures or graphs.
Articles that exclusively focused on i) older population groups (i.e., 6–18 years olds) or ii) other contexts than families (e.g., homeless children, children in foster care, institutionalised living, neighbourhood characteristics and environmental exposures) were excluded from the literature synthesis. The exclusion criteria were published a priori [34].
Data charting and data items
A data-charting form was jointly developed and independently filled in by two reviewers (SH, LS). Data from all articles/studies were extracted doubly, and inconsistencies were resolved in discussion between the two reviewers or via consultation with a third researcher (JS).
For studies that met all the eligibility criteria, data items were summarised in tabular form in accordance with the key dimensions of the review: family characteristics, inequalities in health, children´s age during outcome collection, and an open field for population characteristics. Additionally, data about the country, data collection and data analysis methods, and the main results were documented.
Synthesis of results
The findings were narratively synthesised following the PRISMA Extension for Scoping Reviews [33]. For illustrative purposes, the findings were mapped using the conceptual framework of this scoping review in Figs. 3, 4, and 5.
Results
a. Selection of sources of evidence
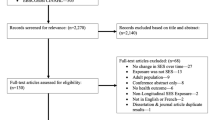
After removing duplicates, 7,089 articles were included in the screening process. Based on the title and abstracts, found articles were excluded despite matching search terms, because the terms used in the search algorithm corresponded with i) a different population (i.e., children older than 6 years), ii) contexts other than families, and iii) different concepts (i.e., spatial socioeconomic deprivation). Ensuing title/abstract screening, 417 full texts were retrieved and controlled for eligibility. A total of ten peer-reviewed studies met all inclusion criteria. Observer agreement was categorised as excellent in each data selection process (title and abstract screening: Cohen’s Kappa = 0.89; full text screening: Cohen’s Kappa = 0.92). Fig. 2 outlines the selection process.

Flowchart of Study Selection Following PRISMA Extension for Scoping Reviews
Figure 2 details database-specific results of the literature search and the numbers of articles screened at each stage in the two-step screening processes as well as reasons for exclusion at both the title/abstract-level (n = 6,672) and the full-text level (n = 407).
b. Characteristics of sources of evidence
The majority of the research included in the screening (n = 7,089) examined the impact of family characteristics on health, regardless of the SEP or vice versa. Thus, peer-reviewed articles published on socioeconomic health inequalities among young people during the past two decades did rarely consider family characteristics as mediating or moderating factors (n = 10).
The studies applied single indicators of income and education [43–49], as well as combined indices thereof [50–52]. No study considered occupation as a dimension of SEP. While one study did not report the methods of data collection [52], all other studies included self-reported information of SEP and health outcomes (n = 9). Only a few different outcomes were used, namely screen time (n = 2), behavioural difficulties (n = 2), development (n = 2), parent-rated health (n = 2), injuries (n = 1) and being breastfed (n = 1). While all outcomes in children’s development were measured [49, 52], all other outcomes were reported either by both parents (n = 7) or by the mother only [44].
Family characteristics were operationalised by four domains:
- 1.
- 2.
- 3.
-
4.
a combination thereof [49].
With the exception of parental screen time, the studies did not operationalise parental health literacy and did not consider intergenerational relations. With regard to data collection, one study applied observations and video recording [52], while the other studies were based on self-reports on family characteristics (n = 9). Although some of the studies drew their sample from a larger longitudinal study [44, 47, 48, 52], the family characteristics data of all the studies were examined cross-sectionally.
The findings mainly referred to children at the age of nine months to six years (sample sizes: 68–14,378), only one study considered newborns [43].
In terms of the geographic scope, 50% of the studies were conducted in the United States of America (n = 5). Other countries were the United Kingdom (n = 1), Canada (n = 1), Finland (n = 1), the Netherlands (n = 1), and Australia (n = 1). There was a notable absence of scientific literature from high-income European and Asian countries [31]. All the studies were published after 2010.
Figure 3 provides an overview of the number of studies that examined family characteristics and socioeconomic inequalities in health among young children (i.e., newborns, infants/toddler/preschoolers).

Overview of Studies Examining the Pathways Underlying Health Inequalities with Family Characteristics
c. Results of individual sources of evidence
Table 1 provides a detailed description of the studies included and data analyses conducted on mediating or moderating effects of family characteristics.
d. Synthesis of results
Mediating Effects (objective 1) of family processes and family living conditions
In total, seven studies conducted analyses to identify whether family characteristics have a mediating effect on health inequalities. Mediating effects were explored, if SEP was associated with family characteristics, which, in turn, affected health outcomes. To examine those effects, studies presented quantitative data analyses or only reported their findings.
The findings of the studies indicated that family processes mediate the association between family SEP and health among young people regarding the following three domains [46, 47, 50]: 1. parent-rated stress in parent–child relationship, 2. parental rules/descriptive norms, and 3. parental own health-related behaviour. Fewer economic resources were linked to higher parental stress that worsened behavioural difficulties (e.g., uncommunicative, depressed, anxious, attention problems, aggressive behaviours) [50]. Furthermore, a lower parental education was associated with fewer rules/ descriptive norms, resulting in higher daily averages in preschool children’s screen time [46]. Additionally, the parental extent of screen time [46, 47] contributed to the association of low family education and long screen time of children. In terms of family living conditions, a television set in children’s bedrooms conveyed the association between a lower educated maternal background and an extensive screen time among children [47]. Fig. 4 provides an overview of reported mediating effects and illustrates whether effects were found or not. Fig. 4 maps the findings using the conceptual framework of the scoping review by means of presenting each study in which mediating effects were examined, along with their references. The figure illustrates parameters used to operationalise socioeconomic inequalities in health in early childhood as well as the family characteristics considered.

Moderating effects (objective 2) of family processes and family structure and size
In total, five studies conducted analyses to identify whether family characteristics have a moderating effect on health inequalities. Moderating effects (P-value < 0.05) were statistically tested with interaction terms between SEP and family characteristics using logistic or linear regressions [45, 49, 51], SEP-stratified outcome measures also using either logistic or linear regression [43, 48], or graphical analyses [45, 51].
The findings of the studies indicate that family processes regarding sibling differences in parenting (i.e., differential negativity) or conflicts in parent–child relations (i.e., negativity) moderate the association between family SEP and children’s health. Children with a lower SEP (i.e., index, education) were more likely to have impairment or poor health. The effect of high negativity within families was shown to be stronger among families with a lower SEP compared to those with high SEP [45, 51]. Moreover, studies suggested moderating effects of both the structure of the family (i.e., single versus married) [43] and the number of children in the household [48, 49]. For example, the association between being breastfed and low-income households was reinforced by single-parent family structure [43]. Furthermore, among low-income compared to high-income families, a greater number of children in the household contributed to an aggravated self-regulation among preschoolers [49]. The moderating effect of having an infant in the family on the behavioural difficulties of preschool children was also shown to be stronger among children from low-income families compared to those from high-income families [48]. Fig. 5 presents all findings and the identified moderating effects.

Figure 5 maps the findings using the conceptual framework of the scoping review by means of presenting each study in which moderating effects were examined, along with their references. The figure illustrates parameters used to operationalise socioeconomic inequalities in health in early childhood as well as the family characteristics considered.
Discussion
This scoping review provides the first synthesis of scientific peer-reviewed literature addressing the extent, nature, results, and knowledge gaps concerning the impact of family characteristics on health inequalities in early childhood.
Overall, it is notable that only ten studies could be included in the review. Nevertheless, the review reveals specific mediating effects of family processes (e.g., rules/ descriptive norms, stress, and parental screen time) and families’ living conditions (e.g., TVs in bedrooms). Furthermore, negativity in families, single parenthood, and the number of children or infants living in the household emerge as moderators of health inequalities in early childhood.
Discussion of mediating effects of family characteristics (objective 1)
Parenting is the most frequently investigated family characteristic through which SEP influences preschoolers’ health. Stress in parent–child relationship [50], rules/descriptive norms [46], and parental screen time [46, 47] were found to be family processes with a mediating effect. These findings are in line with both the FSM and the FIM, as they follow the logic of social causation by assuming that differences in SEP lead to differences in parental stress and parental behaviour, resulting in health inequalities, specifically in behavioural difficulties [50] and in screen time [46, 47] among young children. Likewise, existing research examining the (isolated) impact of family characteristics or SEP on health correspond with the findings of this review. There, risk factors for behaviour problems among preschoolers or correlates of sedentary behaviour and screen-viewing among three to seven years old children are associated with both family characteristics and SEP [53–55]. Simultaneously, the systematic literature review on intervention strategies by Altenburg et al. (2016) [56] highlighted the potential impact of parental role modelling (e.g., parental own screen time) on children’s sedentary time. For instance, child-rated parental TV viewing time was found to correlate with screen time in later childhood (eighth grade) [57].
The living conditions of the family, particularly TVs in children´s bedrooms, affected socioeconomic differences in children´s TV viewing time [47]. This result corresponds with evidence on the contribution of living conditions to health-related behaviour among preschoolers. For example, health-related sleeping habits are affected by TVs in bedrooms [58]. Studies on screen time in later childhood and adolescence suggest that the number and placement of TVs are mediators of differences along parental education among adolescents [57].
Discussion of moderating effects of family characteristics (objective 2)
The studies show that differential negativity in the family (i.e., amount of negativity a child experiences relative to the others) [45] and hostile parent–child relations [51] influence the effects of lower SEP on parent-rated impairment and parent-rated general health. This finding is supported by previous research by Amato et al. (2010) [39], in which stable relationships with an adult caregiver and good parenting were associated with a better health in early life.
The presence of several children in a household was found to moderate the association of low income on lower cognitive competencies [49]. Li et al. (2017) [49] argue that children’s self-regulatory skills do not benefit from a higher number of children (i.e., opportunities for social interaction) in low-income families compared to higher-income families due to related demands on families’ resources. Similarly, Strazdins et al. (2010) [48] conclude that lower family income is associated with behavioural difficulties among preschool children, which is affected by the number of infants in the family. The extent of inequalities in cognitive and behavioural difficulties depend on family structure/size. Thereby, family characteristics contribute to inequalities in health and development in early childhood as they may intensify precarious socioeconomic circumstances.
According to the Kim and Gallien (2016), income-based disparities in breastfeeding initiation depend on single parent status [43]. Empirical literature indicates that an imbalance between work and family life affects breastfeeding initiation and duration, in particular among single mothers [59, 60]. One such study [49] indicated that low family income has an influence on development in early childhood and is affected by single parent status. This result corresponds to existing evidence gained by research on divorce. Amato et al. (2010) [39] and Fincham et al. (2010) [61] showed that marital status contributes to health.
Remaining research gaps
The effects of SEP on health considering family characteristics may not become apparent during the first years of life compared to higher age groups, because cumulative processes and effects on health throughout the course of life can be assumed [62]. This may be one potential explanation for the small number of studies identified with a special focus on the first months of life [43]. It may also be possible that previous studies applied a rather downstream approach by focusing on individual health and individual level determinants of health only, neglecting the possible impact of social environments and broader societal factors.
The extent of studies on the topic at hand is insufficient to comprehensively assess effects on health inequalities for different reasons. First, the identified literature is mainly descriptive in nature. Second, the findings are limited to a small number of considered i) family characteristics and ii) health outcomes. For example, the studies focus on conservative family structures/sizes (e.g., heteronormative parental relationships, biological parent–child relation, nuclear families). Consequently, the review unveils a number of research gaps that require further investigation in the future. Specifically, multiple levels of family transitions (e.g., parental divorce, re-partnering and remarriage, new half-siblings, and step-families), as well as interrelationships between different generations, should be taken into account [63, 64]. Additionally, this scoping review presents little research on family processes related to parental health literacy. With regard to parental role models, it would be beneficial to examine the mediating or moderating effects of parental health behaviour on the relationship between SEP and child health. Recent studies demonstrate the importance of parental role models in nutritional behaviour and physical activity that influences children’s health [26, 65, 66]. The literature also insufficiently reports on health behaviour (e.g., nutrition, physical activity), as well as health (e.g., child weight, child height, birthweight, oral/dental health) [63]. Third, the studies predominantly refer to educational disparities or families’ income differences. Perspectives on parental employment, however, may also be considered in future research on social gradients in children’s health behaviour and health [67].
Strengths and limitations
The strength of this scoping review is that it synthesised the international scientific literature on mediating and moderating effects of family characteristics on inequalities in health in early childhood in high-income countries, which, to our knowledge, has not been done before.
One limitation is that despite a large number of children attending day care facilities, this review focuses exclusively on the mediating and moderating effects of the family as the most important social environment in early childhood. The findings presented here should, therefore, be supplemented by reviews of cooperating research groups [68] on the effects of further relevant social environments, such as kindergartens [69] and schools [70], and by reviews examining late childhood and adolescence [29].
Although we have shown that families are an influential environment for young children, individual health and health behaviour are undeniably affected by factors beyond the individual and family level [5, 71, 72] often referred to as “upstream factors” or social determinants of health. These may refer, for instance, to aspects of economic stability, health care, or transport, and are often shaped by policies and contextual factors. Due to the focus of this review on family characteristics, it was not possible to study the impact of upstream factors. Furthermore, this scoping review exclusively considers individual socioeconomic differences in early health in high-income countries as defined by basic economic country conditions (e.g., gross domestic product per capita (GDP)) [31]. Therefore, the results on the mediating or moderating effects of family characteristics are restricted to higher income countries and to young individuals. According to the OECD Social Policy Division [73], there are country-specific differences in family indicators. For example, family size or household size averages vary by country. Further research should take political contexts, such as family politics and labour market policies, into account in order to understand health outcomes beyond the dimension of GDP [74].
This research reviewed correlative associations rather than causal pathways, because family characteristics were examined cross-sectionally by considering one generation of caregivers/parents only. It should be noted that recent literature on family characteristics and children’s health emphasised the impact of family transitions as described above, both in the early course of life [39, 61] and with regard to intergenerational transmission of, for example, parenting styles [75].
Due to the chosen scoping review methodology [33], various sources of research methods were eligible for inclusion. A critical appraisal (i.e., risk of bias) of the studies included was not intended [76, 77]. Rather, the scoping review resulted in a synthesis of peer-reviewed articles of the topic of interest in the last two decades.
The screening and selection process led to difficulties in the generalization of results due to a limited number of studies included. As the review is limited to peer-reviewed articles, it is possible that relevant research published in other formats, such as books, theses, and grey literature, may have remained undetected. The same is true for studies from high-income countries (e.g., France, Italy) that might have been published in other languages than English or German.
Conclusion
Families are vital social environments with regard to enabling and promoting children’s healthy development. The synthesized research provides a better understanding of the contribution of family characteristics to the association between families’ SEP and health inequalities in early childhood in higher income countries. The studies included were not enough in amount or extent to comprehensively assess the moderating and mediating effect of family processes, family structure/size and living conditions. The small body of evidence identified supports eco-social perspectives on the interacting mechanism between contextual circumstances and individual health. Thus, public health measures for reducing HI and promoting childrens’ health might be more effective when taking children’s family situation, including their resources (e.g., human capital) and environment (e.g., area deprivation), into account.
Future research in public health should (a) validate measures of family characteristics in relation to relevant indicators of children’s health inequalities in early life (e.g., obesity, inflammation parameters), (b) analyse the impact of the family environment on newborns’ and infants’ health inequalities, and (c) clarify causal pathways and mechanisms, for instance through considering parental perspectives (e.g., on practical nexuses, relevant contextual factors and needs). This may be done by combining dimensions from the FIM and the FSM.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the study.
Abbreviations
- SEP:
-
Socioeconomic Position
- FSM:
-
Family Stress Model
- FIM:
-
Family Investment Model
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
References
Ben-Shlomo Y, Cooper R, Kuh D. The last two decades of life course epidemiology, and its relevance for research on ageing. Int J Epidemiol. 2016;45(4):973–88.
Ben-Shlomo Y, Mishra G, Kuh D. Handbook of epidemiology. 2nd ed. New York: Springer Reference; 2014.
Marmot M, Allen JJ. Social determinants of health equity. Am J of Public Health. 2014;104(4):517–9.
Scambler G. Health inequalities. Sociol Health Illn. 2012;34(1):130–46.
CSDH. Closing the gap in a generation: health equity through action on the social determinants of health: Final Report of the Commission on Social Determinants of Health. Geneva: World Health Organization; 2008.
Kail RV, Cavanaugh JC. Human development: A life-span view. 7th ed. Australia, Brazil, Mexico: Cengage Learning; 2016.
Chen JH. Asthma and child behavioral skills: does family socioeconomic status matter? Soc Sci Med. 2014;115:38–48.
Bürgi F, Meyer U, Niederer I, Ebenegger V, Marques-Vidal P, Granacher U, et al. Socio-cultural determinants of adiposity and physical activity in preschool children: a cross-sectional study. BMC Public Health. 2010;10:733.
Hale L, Berger LM, LeBourgeois MK, Brooks-Gunn J. Social and demographic predictors of preschoolers’ bedtime routines. J Dev Behav Pediatr. 2009;30(5):394–402.
Iguacel I, Fernández-Alvira JM, Labayen I, Moreno LA, Samper MP, Rodríguez G. Social vulnerabilities as determinants of overweight in 2-, 4- and 6-year-old Spanish children. Eur J Public Health. 2018;28(2):289–95.
Khanam R, Nghiem S. Family Income and Child Cognitive and Noncognitive Development in Australia: Does Money Matter? Demography. 2016;53(3):597–621.
Bronfenbrenner U. The ecology of human development: Experiments by nature and design. Cambridge, Mass: Harvard University Press; 1996.
Krieger N. Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol. 2001;30(4):668–77.
Krieger N. Embodiment: a conceptual glossary for epidemiology. J Epidemiol Community Health. 2005;59(5):350–5.
Silverstein M, Giarrusso R. Aging and Family Life: A Decade Review. J Marriage Fam. 2010;72(5):1039–58.
Waite LJ, Plewes TJ, editors. New directions in the sociology of aging. Washington, D.C.: The National Academy Press; 2013.
Leventhal T, Newman S. Housing and child development. Child Youth Serv Rev. 2010;32(9):1165–74.
Neel MLM, Stark AR, Maitre NL. Parenting style impacts cognitive and behavioural outcomes of former preterm infants: A systematic review. Child Care Health Dev. 2018;44(4):507–15.
Brown SL. Marriage and Child Well-Being: Research and Policy Perspectives. J Marriage Fam. 2010;72(5):1059–77.
Ursache A, Merz EC, Melvin S, Meyer J, Noble KG. Socioeconomic status, hair cortisol and internalizing symptoms in parents and children. Psychoneuroendocrinology. 2017;78:142–50.
Kramer MR, Schneider EB, Kane JB, Margerison-Zilko C, Jones-Smith J, King K, et al. Getting Under the Skin: Children’s Health Disparities as Embodiment of Social Class. Popul Res Policy Rev. 2017;36(5):671–97.
Edin K, Kissane RJ. Poverty and the American Family: A Decade in Review. J Marriage Fam. 2010;72(3):460–79.
Conger RD, Conger KJ, Martin MJ. Socioeconomic Status, Family Processes, and Individual Development. J Marriage Fam. 2010;72(3):685–704.
Simons LG, Steele ME. The Negative Impact of Economic Hardship on Adolescent Academic Engagement: An Examination Parental Investment and Family Stress Processes. J Youth Adolesc. 2020;49(5):973–90.
Masarik AS, Conger RD. Stress and child development: a review of the Family Stress Model. Curr Opin Psychol. 2017;13:85–90.
Sosu EM, Schmidt P. Economic Deprivation and Its Effects on Childhood Conduct Problems: The Mediating Role of Family Stress and Investment Factors. Front Psychol. 2017;8:1580.
Conger RD, Donnellan MB. An interactionist perspective on the socioeconomic context of human development. Annu Rev Psychol. 2007;58:175–99.
Hearst MO, Sevcik S, Fulkerson JA, Pasch KE, Harnack LJ, Lytle LA. Stressed out and overcommitted! The relationships between time demands and family rules and parents’ and their child’s weight status. Health Educ Behav. 2012;39(4):446–54.
Blume M, Rattay P, Hoffmann S, Spallek J, Sander L, Herr R, et al. Health Inequalities in Children and Adolescents: A Scoping Review of the Mediating and Moderating Effects of Family Characteristics. IJERPH. 2021;18(15):7739.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
United Nations. World Economic Situation and Prospects.: Statistical annex.; 2019. Available from: URL: https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/wesp2019_book-annex-en.pdf.
von Elm E, Schreiber G, Haupt CC. Methodische Anleitung für Scoping Reviews (JBI-Methodologie). Z Evid Fortbild Qual Gesundhwes. 2019;143:1–7.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73.
Hoffmann S, Wachtler B, Sander L, Blume M, Hilger-Kolb J, Herke M et al. Health inequalities among infants and pre-school children: Protocol for a scoping review examining the moderating and mediating role of contextual and compositional family characteristics; 2020. Available from: https://doi.org/10.17605/OSF.IO/3U4ST
Baumann N. How to use the medical subject headings (MeSH). Int J Clin Pract. 2016;70(2):171–4.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–6.
Landis JR, Koch GG. The Measurement of Observer Agreement for Categorical Data. Biometrics. 1977;33(1):159.
White L, Rogers SJ. Economic Circumstances and Family Outcomes: A Review of the 1990s. J Marriage Fam. 2000;62(4):1035–51.
Amato PR. Research on Divorce: Continuing Trends and New Developments. J Marriage Fam. 2010;72(3):650–66.
Johnson MD, Hank K, Yurkiw J. Longitudinal Associations Between Adult Relations with Intimate Partners and Siblings. J Marriage Fam. 2021;83.2:551–62. https://doi.org/10.1111/jomf.12710.
Richter M, Hurrelmann K. Gesundheitliche Ungleichheit [Health inequalities]. Wiesbaden: VS Verlag für Sozialwissenschaften; 2009.
Abdi N, Sadeghi R, Zamani-Alavijeh F, Taghdisi MH, Shojaeezadeh D. Explaining nutritional habits and behaviors of low socioeconomic status women in Sanandaj: a qualitative content analysis. Electron Physician. 2016;8(1):1733–9.
Kim J, Gallien TL. Childcare arrangements and infant feeding practices by family structure and household income among US children aged 0 to 2 years. Matern Child Nutr. 2016;12(3):591–602.
Pearce A, Li L, Abbas J, Ferguson B, Graham H, Law C. Does the home environment influence inequalities in unintentional injury in early childhood? Findings from the UK Millennium Cohort Study. J Epidemiol Community Health. 2012;66(2):181–8.
Browne DT, Jenkins JM. Health across early childhood and socioeconomic status: examining the moderating effects of differential parenting. Soc Sci Med. 2012;74(10):1622–9.
Määttä S, Kaukonen R, Vepsäläinen H, Lehto E, Ylönen A, Ray C, et al. The mediating role of the home environment in relation to parental educational level and preschool children’s screen time: a cross-sectional study. BMC Public Health. 2017;17(1):1–11.
Wijtzes AI, Jansen W, Kamphuis CBM, Jaddoe VWV, Moll HA, Tiemeier H, et al. Increased risk of exceeding entertainment-media guidelines in preschool children from low socioeconomic background: the Generation R Study. Prev Med. 2012;55(4):325–9.
Strazdins L, Shipley M, Clements M, Obrien LV, Broom DH. Job quality and inequality: parents’ jobs and children’s emotional and behavioural difficulties. Soc Sci Med. 2010;70(12):2052–60.
Li M, Riis JL, Ghazarian SR, Johnson SB. Income, Family Context, and Self-Regulation in 5-Year-Old Children. J Dev Behav Pediatr. 2017;38(2):99–108.
Puff J, Renk K. Relationships among parents’ economic stress, parenting, and young children’s behavior problems. Child Psychiatry Hum Dev. 2014;45(6):712–27.
Hagan MJ, Roubinov DS, Adler NE, Boyce WT, Bush NR. Socioeconomic Adversity, Negativity in the Parent Child-Relationship, and Physiological Reactivity: An Examination of Pathways and Interactive Processes Affecting Young Children’s Physical Health. Psychosom Med. 2016;78(9):998–1007.
Demir ÖE, Rowe ML, Heller G, Goldin-Meadow S, Levine SC. Vocabulary, syntax, and narrative development in typically developing children and children with early unilateral brain injury: early parental talk about the “there-and-then” matters. Dev Psychol. 2015;51(2):161–75.
Wakschlag LS, Keenan K. Clinical significance and correlates of disruptive behavior in environmentally at-risk preschoolers. J Clin Child Psychol. 2001;30(2):262–75.
Hinkley T, Salmon J, Okely AD, Trost SG. Correlates of sedentary behaviours in preschool children: a review. Int J Behav Nutr Phys Act. 2010;7(1):66.
HoyosCillero I, Jago R. Systematic review of correlates of screen-viewing among young children. Prev Med. 2010;51(1):3–10.
Altenburg TM, Kist-van Holthe J, Chinapaw MJM. Effectiveness of intervention strategies exclusively targeting reductions in children’s sedentary time: a systematic review of the literature. Int J Behav Nutr Phys Act. 2016;13:65.
Gebremariam MK, Henjum S, Terragni L, Torheim LE. Correlates of screen time and mediators of differences by parental education among adolescents. BMC Pediatr. 2020;20(1):279.
Nuutinen T, Ray C, Roos E. Do computer use, TV viewing, and the presence of the media in the bedroom predict school-aged children’s sleep habits in a longitudinal study? BMC Public Health. 2013;13(1):684.
Ogbuanu C, Glover S, Probst J, Hussey J, Liu J. Balancing work and family: effect of employment characteristics on breastfeeding. J Hum Lact. 2011;27(3):225–38.
Noble S. Maternal employment and the initiation of breastfeeding. Acta Paediatr. 2001;90(4):423–8.
Fincham FD, Beach SRH. Marriage in the New Millennium: A Decade in Review. J Marriage Fam. 2010;72(3):630–49.
Gerhardstein P, Dickerson K, Miller S, Hipp D. Early operant learning is unaffected by socio-economic status and other demographic factors: a meta-analysis. Infant Behav Dev. 2012;35(3):472–8.
Umberson D, Thomeer MB. Family Matters: Research on Family Ties and Health, 2010–2020. J Marriage Fam. 2020;82(1):404–19.
Umberson D, Pudrovska T, Reczek C. Parenthood, Childlessness, and Well-Being: A Life Course Perspective. J Marriage Fam. 2010;72(3):612–29.
Scott-Andrews KQ, Wengrovius C, Robinson LE. Parents accurately perceive problematic eating behaviors but overestimate physical activity levels in preschool children. Eat Weight Disord. 2021;26(3):931–9.
Xu H, Li Wen M, Rissel C. Associations of parental influences with physical activity and screen time among young children: a systematic review. J Obes. 2015;2015:546925.
Pieters J, Rawlings S. Parental unemployment and child health in China. Rev Econ Household. 2020;18(1):207–37.
FOR. Understanding the institutional context of health inequalities among young people. 2019.
Herr RM, Diehl K, Schneider S, Osenbruegge N, Memmer N, Sachse S, et al. Which Meso-Level Characteristics of Early Childhood Education and Care Centers Are Associated with Health, Health Behavior, and Well-Being of Young Children? Findings of a Scoping Review. Int J Environ Res Public Health. 2021;18(9):4973.
Herke M, Moor I, Winter K, Hoffmann S, Spallek J, Hilger-Kolb J, et al. Role of contextual and compositional characteristics of schools for health inequalities in childhood and adolescence: protocol for a scoping review. BMJ Open. 2020;10(12):e038999.
Dahlgren G, Whitehead M. Policies and strategies to promote social equity in health: Background document to WHO – Strategy paper for Europe; 1991 [cited 2021 Oct 25]. Available from: URL: http://repositori.uji.es/xmlui/bitstream/handle/10234/187797/GoeranD_Policies_and_strategies_to_promote_social_equity_in_health.pdf?sequence=1.
Dahlgren G, Whitehead M. The Dahlgren-Whitehead model of health determinants: 30 years on and still chasing rainbows. Public Health. 2021;199:20–4.
OECD. OECD Family Database of Social Policy Division: SF1.1: Family size and household composition; 2015. Available from: URL: http://www.oecd.org/els/family/SF_1_1_Family_size_and_composition.pdf.
Clark R. World health inequality: convergence, divergence, and development. Soc Sci Med. 2011;72(4):617–24.
Jeon S, Neppl TK. Intergenerational continuity in economic hardship, parental positivity, and positive parenting: The association with child behavior. J Fam Psychol. 2016;30(1):22–32.
Sucharew H, Macaluso M. Progress Notes: Methods for Research Evidence Synthesis: The Scoping Review Approach. J Hosp Med. 2019;14(7):416–8.
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143.
Acknowledgements
The authors thank FOR 2723 for support of the SC and the possibility to discuss the work. Special thanks to Karsten Hank for his valuable advice.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by the German Research Foundation (DFG) grant number FOR2723 (project number 384210238). The individual grant number for the subproject is SP 1495/4–1.
Author information
Authors and Affiliations
Contributions
JS and TL conceived the study. JS and SH conceived the reviews research objectives. SH wrote the first draft of the manuscript. SH, LS, MB, BW, and JS conducted the review and contributed to analyses. SH, LS, MB, BW, SvS, MH, CRP, PMMF, WS, MT, and JS contributed to developing the research question and critically commented on the draft in the early stages of the paper. LS, MB, BW, SvS, MH, CRP, PMMF, WS, MT, and JS read, contributed to, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
As no primary data were collected for this scoping review and all studies were identified via literature searches in scientific databases, ethical approval and consent was not required.
Consent for Publication
Consent for publication is not applicable to this article as the manuscript does not contain any individual personal data.
Competing Interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hoffmann, S., Sander, L., Wachtler, B. et al. Moderating or mediating effects of family characteristics on socioeconomic inequalities in child health in high-income countries – a scoping review. BMC Public Health 22, 338 (2022). https://doi.org/10.1186/s12889-022-12603-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12603-4