
Abstract
Background
In general during pregnancy, women are aware of the importance of good diet quality, interested in nutrition, and receptive to changing dietary intake. However, adherence to dietary guidelines is sub-optimal. A pregnant woman’s first information source regarding nutrition information is her midwife. Healthy nutrition promotion by midwives may therefore be very promising, but midwives face multiple barriers in providing nutritional support. Empowering pregnant women to improve their diet quality is expected to improve their health. Therefore an empowerment intervention has been developed to improve diet quality among pregnant women. The objective of this study is to evaluate the effectiveness and feasibility of Power 4 a Healthy Pregnancy (P4HP). P4HP aims to empower pregnant women to have a healthier diet quality.
Methods/design
This study applies a mixed methodology consisting of a non-blinded cluster randomized trial with an intervention (P4HP) group and a control group and a process evaluation. Midwifery practices, the clusters, will be randomly allocated to the intervention arm (n = 7) and control arm (n = 7). Participating women are placed in intervention or control conditions based on their midwifery practice. Each midwifery practice includes 25 pregnant women, making 350 participants in total. Health related outcomes, diet quality, empowerment, Sense of Coherence, Quality of Life, and Self-Rated Health of participants will be assessed before (T0) and after (T1) the intervention. The process evaluation focuses on multidisciplinary collaboration, facilitators, and barriers, and consists of in-depth interviews with midwives, dieticians and pregnant women.
Discussion
This study is the first to evaluate an empowerment intervention to improve diet quality in this target population. This mixed method evaluation will contribute to knowledge about the effectiveness and feasibility regarding diet quality, empowerment, health-related outcomes, multidisciplinary collaboration, facilitators and barriers of the empowerment intervention P4HP. Results will help inform how to empower pregnant women to achieve improved diet quality by midwives and dieticians. If proven effective, P4HP has the potential to be implemented nationally and scaled up to a long-term trajectory from preconception to the postnatal phase.
Trial registration
The trial is prospectively registered at the Netherlands Trial Register (NL9551). Date registered: 19/05/2021.
Similar content being viewed by others

Background
A healthy diet is important for everyone, but crucial during pregnancy for the health of both mother and child [1,2,3,4,5]. During pregnancy, women are aware of the importance of a good diet quality and are interested in nutrition [6, 7]. However, adherence to dietary guidelines and recommendations is sub-optimal, especially among pregnant women with lower socioeconomic status (SES) [8,9,10], and specifically for the intake of fruit, vegetables, grains, folate, and iron [11,12,13,14,15]. Poor diet quality by the mother is associated with adverse health outcomes, including increased risk of pre-eclampsia, gestational diabetes, and excessive gestational weight gain. For the unborn, a poor diet of the mother is related to adverse birth outcomes, including premature birth and low birth weight, as well as disadvantageous health outcomes later in life, such as the increased risk of developing chronic diseases [1,2,3]. However, due to several challenges, such as nausea, cravings, and ingrained habits, pregnant women experience difficulties with the implementation of dietary changes and sustaining these changes during their pregnancy [8, 16]. On top of that, the diet quality of pregnant women is challenged by aspects such as the costs of living and their physical and social environments.
Pregnancy is often regarded as a critical transition, a teachable moment, in which women are more receptive to changing dietary patterns than in other phases in life [6, 7, 17,18,19]. Pregnancy might increase awareness regarding diet since women generally feel that one of the few things to positively impact the health of their child is to make dietary improvements [20]. A pregnant woman’s first, most important, and most trusted information source regarding nutrition information is their midwife [6, 7, 21,22,23,24,25]. Also, midwives feel responsible to inform pregnant women about a healthy diet [25]. Compared to other countries, midwives in the Netherlands play a relatively large and central role in maternity care. Healthy nutrition promotion by midwives is therefore promising to make use of this window of opportunity where women are increasingly aware of their behaviours for their health and their child’s health [21, 23, 25, 26]. However, although midwives feel the responsibility to provide nutritional advice, they do not consider themselves nutritional experts and encounter structural barriers in providing nutrition communication [5, 25, 27,28,29]. Some of the main barriers for midwives are time constraints and unsupportive health systems (e.g. a lack of cooperation with other health professionals) [5, 29,30,31,32], as well as limited relevant and reliable resources and training [5, 29, 33,34,35]. As a result, nutrition communication in antenatal care generally remains suboptimal. Currently, only Dutch women with pregnancy complications, overweight/obesity, or excessive gestational weight gain, or those who asked for it themselves receive comprehensive guidance regarding their nutrition during pregnancy [25, 36, 37].
The modern concept of empowerment is increasingly defined as strengthening the capabilities and the self-reliance of individuals [38]. We use Aubel’s definition, who describes empowerment as ‘the ability of individuals or groups to improve capacities, to critically analyse situations and to take actions to improve those situations’ [39]. This definition applies bottom-up thinking to drive behaviour change [40,41,42], requiring an environment in which pregnant women can engage in open communication [40]. The process of empowering pregnant women is expected to improve their health, as they are supported to make healthier choices, for example in terms of nutrition [6, 21]. This can therefore result in improved child health and providing children with a healthy and successful start of life [2, 3].
P4HP has been developed in the past years together with stakeholders, aiming to empower pregnant women to have a healthier diet quality [42,43,44,45]. This intervention may contribute to enduring new-borns with a healthy, successful start of life [2, 3] and has the potential to improve health across generations. P4HP uses a women-centered empowerment approach, to prioritize the woman’s individual needs, as defined by the woman herself, assigning to the woman’s choice, control, and continuity of care. P4HP allows women to be empowered, gaining control over their lives and learning how to achieve goals that are meaningful to them. Individuals are most likely to change their behaviour to make healthier choices when they are educated and motivated to do so, in addition to environments and policies supporting these decisions [46].
A similar intervention in which empowerment and diet quality among pregnant women is central has not been implemented before to our best knowledge. The research will contribute to theoretical development by providing practice-based evidence [47, 48]. This mixed methods study aims to 1) evaluate the effectiveness of P4HP regarding diet quality, empowerment, Sense of Coherence (SOC), Quality of Life (QoL), and Self-Rated Health (SRH) using a cluster randomized controlled trial (C-RCT), and 2) evaluate P4HP in terms of multidisciplinary collaboration, facilitators and barriers using a process evaluation. This way, as we retrieve both information about what is needed to achieve an effect and about what is needed in the implementation and in the multisectoral collaboration, we gain insight in both the effectiveness as well as the feasibility of P4HP.
Research in the area of empowerment towards dietary intake in pregnancy is sparse [24, 49]. Still, empowerment has been linked to diet quality, although mostly in global south [50,51,52,53]. Additional to empowerment and diet quality, health outcomes are included, as empowerment has been previously linked to the concepts QoL [54, 55], SOC [56, 57], and SRH [58, 59]. Also diet quality has been linked to the concepts QoL [60, 61], SOC [62, 63], and SRH [64, 65]. We hypothesize that empowerment, improved diet quality, and the health outcomes QoL, SOC and SRH will have a mutually reinforcing, invigorative effect on each other (Fig. 1).

Overview of hypothesis P4HP
Methods
Study design
This mixed methods study consists of a non-blinded C-RCT with an intervention (P4HP) group and a control group and a process evaluation. A qualitative process evaluation will take place to evaluate P4HP by midwives and dieticians in terms of multidisciplinary collaboration, facilitators, and barriers.
A pilot study has launched on October 1st, 2021, with the aim to reach a total of 10 participants from two midwifery practices within 2 months. In this pilot study we pre-test the questionnaires, the perceptions of the P4HP intervention, and the practical and technical matters regarding implementation, including the organization of multidisciplinary collaboration. Any suggestions by the midwives, dieticians, and pregnant women will be duly accommodated to improve the feasibility.
Non-blinded C-RCT
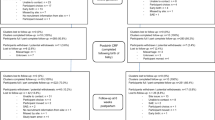
The non-blinded C-RCT will evaluate the effectiveness of P4HP on pregnant women’s empowerment, diet quality, and health outcomes between intervention and control practices. Figure 2 details the flow of participants from recruitment of midwifery practices until the last follow-up contact for intervention and control participants. The clusters are midwifery practices in the Netherlands and the participants are Dutch-speaking pregnant women visiting the practice. Cluster randomization is applied to eliminate the risk of cross-contamination between the two study arms. Thus, whether pregnant women are placed in the intervention or the control group is based on whether receiving care from intervention or control midwifery practices. Due to the nature of the intervention, it is not possible to blind the professionals, participants, or investigators to the study conditions. This protocol has been written according to the recommendations of the Standard Protocol Items Recommendations for Interventional Trials (SPIRIT) 2013 statement [66, 67] (Additional file 1). SPIRIT guides key content to facilitating the drafting of high-quality protocols, including recommendations for intervention trials.

Flow diagram of the participants through the trial
Cluster and participant recruitment
Midwifery practices in the Netherlands will be recruited by using existing connections, snowballing, social media, and presentations of the study at local collaborations of midwifery practices. Midwifery practices are randomized as clusters to either an intervention arm or standard birth care. Clusters will be randomized by a researcher, who is unfamiliar with the midwifery practices, using a randomization scheme in Excel.
Eligible pregnant women will be recruited in randomized midwifery practices (clusters) in the Netherlands using a purposive sampling technique. Midwives will be informed by the research team about the in- and exclusion criteria. Midwives will explore whether or not the pregnant women meet the inclusion criteria and explain to them the purpose of the study. The women will be invited to participate voluntarily. To be eligible to participate in this study, a participant must meet all of the following criteria: being in the first trimester of pregnancy; > 18 years of age; understanding and speaking Dutch; consuming a Dutch diet pattern i.e. a diet with a maximum of one hot meal per day. A potential participant who meets any of the following criteria will be excluded from participation: not willing to provide informed consent; having a severe chronic illness/condition (for example cancer); having conditions that may affect diet quality. The recruitment of participants will begin on 01-01-2022 and will end when all 14 midwifery practices have met their target of 25 women. Alternatively, the recruitment will end on 31-12-2022.
Sample size estimation
The sample size estimation is based on the design of a C-RCT [68] using the Group-or Cluster-Randomized Trials sample size calculator from the National Institutes of Health [69], where each cluster represents a midwifery practice. The results indicate that to detect an effect size of 0.4 (small to medium) [70] with a power of 80%, an alpha of 0.05, and an intra-cluster correlation coefficient of 0.02, each arm should include 7 clusters of 25 participants each. The assumption of an intra-cluster correlation coefficient of 0.02 is based on our experience with the SLIMMER project, a cluster randomized trial of a combined lifestyle intervention including behaviour change in diet and physical activity on overweight and risk of diabetes [71]. We strive to keep the number of participating pregnant women per cluster as similar as possible. Based on the sensitivity analysis for this sample size estimation [69], we estimate that 25 participants from 7 intervention and 7 control clusters – leading to 350 participants in total – will be sufficient to detect the relevant difference between groups. The Netherlands had 168.066 births in the year 2020 [72]. Three hundred fifty participants represent < 0.25% of pregnancies in the Netherlands, and therefore expected to be achievable.
Data collection and assessments
At enrolment, participants will give their informed consent through consent forms. Subsequently, participants will be provided with two online quantitative questionnaires to fill out, utilizing baseline data for the study (T0). Upon completion of P4HP, participants are provided the same two online quantitative questionnaires (minus sociodemographic data) to respond to the post-intervention assessment (T1) (Fig. 3). The first questionnaire assesses diet quality [73]. The term diet quality has been used in recent decades to evaluate the dietary habits or patterns of a population and the efficacy of dietary interventions [74,75,76]. Diet quality is a suitable term to present multiple food components, assessed using an index to evaluate the extent of adherence to dietary guidelines. The second questionnaire includes all other assessments and is distributed using Qualtrics. Access to all data collection tools and databases is strictly limited and regulated through personal user profiles. Both platforms are password-protected and all data will be regularly backed up into a password-protected database.

P4HP C-CRT SPIRIT diagram
Sociodemographic data
Questions to collect name, year of birth, phone number, email, postal code digits, living situation, ethnicity, educational level, and personal and household income.
BMI
Two questions to collect height and body weight.
Diet quality
We derive scores for diet quality using Eetscore [77]. Eetscore is a validated web-based screening tool to determine the diet quality of Dutch adults and suitable for assessing change in diet quality over time. Eetscore consists of a short food frequency questionnaire in an accessible writing style that is scored with the Dutch Healthy Diet index 2015 (DHD2015-index) to assess adherence to the Dutch food based dietary guidelines of 2015 of the Dutch health Council [73]. The DHD2015-index has been validated with 24 h dietary recall and FFQ data. In addition, to the DHD2015-index, a 16th component for unhealthy choices has been added. The questionnaire to determine this diet quality score consists of 40 questions with sub-questions inquiring about the consumption of 54 foods or food groups. Based on the answers a total score and 16 sub scores will be calculated. Sub scores of Eetscore are available for 1) vegetables, 2) fruit, 3) whole grain products, 4) legumes, 5) nuts, 6) dairy, 7) fish, 8) tea, 9) fats and oils, 10) coffee, 11) red meat, 12) processed meat, 13) sugar-containing beverages, 14) alcohol, 15) sodium and 16) unhealthy choices. Each component will be scored on a scale ranging from 0 (non-adherence) to 10 (complete adherence), providing a total score between 0 and 160. For the calculation of the scores, specific cut-off and threshold values are used. Since Eetscore is developed for the general Dutch adult population, it has been adapted to fit the requirements of pregnant women. The (sub)scores were adapted based on the dietary recommendations for pregnant women provided by the Dutch Health Council and the Netherlands Nutrition Centre [78]. We use the web-based version of Eetscore which can be filled out in about 10-15 min.
Empowerment
Empowerment will be assessed using the Pregnancy-Related Empowerment Scale (PRES). This is a valid and reliable assessment containing 16 questions on women’s health-related empowerment during pregnancy [79].
SOC
We derive SOC scores from the three-item SOC questionnaire (SOC-3) [80, 81]. This validated questionnaire includes three questions; all corresponding to the three components of SOC: comprehensibility (“Do you usually feel that the things that happen to you in your daily life are hard to understand?”), manageability (“Do you usually see solutions to problems and difficulties that other people find hopeless?”), and meaningfulness (“Do you usually feel that your daily life is a source of personal satisfaction?”) [80,81,82,83]. Participants can indicate their answer as 1 (yes, usually), 2 (yes, sometimes), or 3 (no). The sum of these three items (after reverse coding of the comprehensibility item) reflects the total SOC, with higher scores indicating a weaker SOC. Participants are divided into three SOC groups: weak (scores 6–9), intermediate (scores 4–5), and strong (score 3) - in line with previous studies [80, 84, 85]. We use a Dutch version of the SOC-3, a short version of the original to alternatively measure change, as previously used by Herens [85,86,87]. SOC can be influenced by interventions and has been previously linked to the concept of empowerment [56, 57].
QoL
We derive a score for global QoL using a Visual Analogue Scale (VAS): a horizontal line of 100 mm, with stops (“anchors”) at both extremes – 0 (worst imaginable QoL) to 100 (perfect QoL) – representing the limits of self-rated QoL. A QoL VAS is a frequently used single-item technique with good to excellent levels of reliability, validity, and sensitivity [88,89,90].
SRH
We derive a score for SRH using a General Self-Rated Health (GSRH) question. Asking people to rate their health in surveys provides an easily assessed, common indicator of health [91,92,93,94,95]. Respondents are asked to rate their health, in general, as ‘excellent’, ‘very good’, ‘good’, ‘fair’ or ‘poor’.
Process evaluation
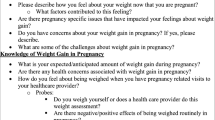
To perform a process evaluation, P4HP will be evaluated in terms of multidisciplinary collaboration, facilitators, and barriers by in-depth interviews with a purposeful sample of midwives, dieticians and pregnant women involved in the C-RCT. Semi-structured interview guides will be prepared for each of the interviews with midwives, dieticians, and pregnant women. 10-15 interviews will be performed with each of the three groups, depending on data saturation, and performed at T1.
Intervention
P4HP is a non-invasive empowerment intervention and consists of four extra moments for pregnant women to discuss nutrition with their midwife and a dietician. P4HP distinguishes itself from standard birth care by its empowering approach towards improving diet quality during pregnancy. The intervention is free of charge for the women and takes place in an individual or group setting (via CenteringPregnancy). P4HP is designed to be flexible, meaning that the professional has the freedom to adapt to what the individual or group needs at each session. This research is in line with current Dutch policy regarding empowerment, dietary guidelines, and prevention [96,97,98,99].
Table 1 provides an overview of the P4HP-elements. For each element of the intervention, it explains the goal(s), the activity, the estimated time that is needed for the activity, and the tools as well as who guides the activity. The exact time investment per session topic will be discussed with and adapted to the possibilities of the midwives and dieticians.
The financial compensation for the invested time by midwives and dieticians will be reimbursed. Participating women will not have additional costs as compared to standard birth care.
Control
Midwifery practices in control clusters will provide participating women with standard birth care (according to the present Dutch birth care standards [100]) and the usual information on nutrition during pregnancy. There is no standard protocol for nutrition communication in antenatal care, so the amount of time and content can vary between the control practices. It is common practice to dedicate a small amount of time (2-10 min) to the discussion of nutrition at the first consultation, focusing on foods that cannot be safely consumed during pregnancy. In standard birth care, pregnant women may be referred to organizations such as the Netherlands Nutrition Centre for questions, nutritional guidelines, or advice. Frequently used tools such as the app ZwangerHap [101] are likely used by pregnant women in the control group. In addition, the newest dietary guidelines for pregnant women of the Dutch Health Council are freely available for health professionals and pregnant women. Being part of the control group in no way limits the use of such nutritional resources, as they are part of standard birth care. Outcome measures will be obtained in the same way for participants in the control clusters as for those in intervention clusters at baseline (T0) and follow-up (T1).
Ethical consideration
Ethics approval was given by Medical Research Ethics Committee Utrecht, the Netherlands on September 21st 2021. The committee thereby declares that the proposal satisfactorily deals with ethical issues and that it complies with the Netherlands Code of Conduct for Scientific Practice. Because of negligible risk for participants, the MREC Utrecht has granted this study exemption from the obligation to the insurance that covers damage caused by the research through injury of the participant. Therefore, adverse events are currently not foreseen, due to the nature of the study and intervention. Informed consent will be obtained from each participant, after the purpose and possible consequences of the study have been explained. This study will be conducted according to the principles of the Declaration of Helsinki (October 2013) and according to the Medical Research Involving Human Subjects Act (WMO).
Participation in the study is voluntary and participants can leave the study at any time for any reason if they wish to do so without any consequences. They are asked to inform either the principal investigator or intervention deliverer (midwife or dietician) about their decision. Participants are not obliged to inform the researchers about their reason to withdraw. The investigator can decide to withdraw a participant from the study for urgent medical reasons, such as having a miscarriage or a pregnancy with extreme complications. The reason for withdrawal reason will be kept for the record for further study. Since P4HP is possibly delivered in a group format, there will be no replacement of individual participants after withdrawal.
Data analyses
Quantitative analyses C-RCT
Statistical analyses will be carried out using IBM SPSS Version 25 (Statistical Package for Social Sciences). Data cleaning will be performed before the final review to check for missing data or outliers. We expect data missing will be at random, and if so, all available data from T0 and T1 will be used to conduct the analyses.
All data will be quantitatively presented in tables (Tables 2 and 3). BMI, the DHD2015-index, PRES score, SoC-3 score, QoL VAS score, and GSRH-score will be presented as ordinal data. Ethnicity, education, and living situation will be presented as nominal data. All data will be entered and verified, and scores will be calculated for multiple-item instruments (i.e. DHD2015-index, PRES, SoC-3). Descriptive statistics will be performed to tabulate mean (or median) values of all study characteristics and baseline values of the independent variables. Chi-square (for categorical variables) and Student’s t-tests (for continuous variables) will be used to compare the descriptive statistics between study groups and to identify potential covariates. The number of participants, as well as means (standard deviations, SDs), median or % (numbers of patients), will be tabulated where appropriate.
Linear mixed models will be used to analyse the data. Using linear mixed models allows for the analysis of different sources of variation in data and for unequal variances and correlations. This flexible method is suitable for analysis of the clustered data as it allows to calculate the treatment effect. When there are multiple levels, such as pregnant women seen by the same midwifery practice, the variability in the outcome can be thought of as either within-group or between-group. Pregnant women-level observations are not independent, as within a midwifery practice pregnant women and their guidance are more similar. Units samples at the highest level (in our research, midwifery practices) are regarded as independent. With this method also confounders can be taken into account [102]. After performing the linear mixed models analysis, the final results will be presented in Table 3. This table will display means and standard errors, the between-group differences, and the p-values for the treatment effect for all primary and secondary outcomes.
All primary and secondary outcomes will be tested via linear mixed models. Other subgroup analyses include age, ethnicity, individual or group (CenteringPregnancy) consultation, educational level, living situation, working situation, and income level. These variables will be checked if they differ across the groups using an independent Student’s t-test when continuous and normally distributed. If skewed, a Wilcoxon signed-rank test will be done. Variables that are not continuous, will be checked for differences between groups using a chi-square test. Two-sided p values < 0.05 will be regarded as statistically significant.
Qualitative analyses process evaluation
Stakeholder interviews will be recorded, transcribed verbatim, and analysed in Atlas.ti using inductive coding to derive themes, theories, or concepts from the raw data and to reveal underlying structures of experiences or processes [103]. The coding process will be done by at least two researchers to increase the validity of the process.
Discussion
This paper describes the study protocol for a mixed methods study consisting of a C-RCT with an intervention group and a control group and a process evaluation. The study protocol includes the evaluation of P4HP, an empowerment intervention to improve diet quality among pregnant women. To our knowledge, this is the first C-RCT that evaluates the effectiveness of an empowerment intervention to improve diet quality in The Netherlands. Research in this field is needed because there is limited evidence of effective empowerment interventions regarding diet quality during pregnancy. To ensure that P4HP fits into standard birth care, various stakeholders have been involved in all steps of the development process. Our study will provide important and unique information on how to empower pregnant women to achieve improved diet quality by midwives and dieticians. Having both a quantitative and qualitative evaluation of P4HP will create a comprehensive overview of both the impact of P4HP and how best to implement it more broadly in practice.
P4HP will be assessed on diet quality, empowerment, SOC, QoL, and SRH. Although these assessments were selected intentionally based on previous research, the intervention may still produce an effect that is not directly assessed by our quantitative assessments. The process evaluation is therefore added to capture these indirect effects using semi-structured interviews. Innovative is that outcome measures include empowerment and SOC, something not common in C-RCT studies. Previous studies found evidence that SOC significantly changed and that those with a weaker SOC were more likely to have a stronger SOC after the intervention that included experimental learning [86, 104], as these groups have most to gain. In case we find change in SOC, it indicates that participants of P4HP benefit from the intervention; providing a more complete picture of the interventions’ successes. Two limiting factors of using Eetscore to assess diet quality are that it is only available in Dutch and oriented to a Dutch dietary pattern. Consequently, this unfortunately limits women who do not speak Dutch and with other diet patterns from participating.
Materials and language used in P4HP are designed to be suitable for low SES pregnant women – the group who will mostly benefit from this intervention because of a general sub-optimal adherence to dietary guidelines [8,9,10]. We assume P4HP thus aligns with women of all SES groups. As it is not ethical to discriminate the inclusion of participants on their SES-status, all SES-groups visiting participating midwifery practices will be included in this study. In the results we will report on differences in outcomes between SES groups.
This study will make a significant and to our knowledge unique scientific and socially relevant contribution about using an empowerment intervention to improve the diet quality of pregnant women in the Netherlands. If P4HP improves pregnant women’s diet quality, empowerment and other health-related outcomes, the impact may have health, social, and economic benefits. We anticipate that the study outcomes have the potential to change the way nutrition is addressed during pregnancy. The findings will directly benefit pregnant women and their children, as well as inform academics and others who strive to produce interventions that can be effectively implemented in routine care using multisectoral collaboration. If P4HP proves to be an effective and feasible intervention, further research will be done on the extension towards the preconception and postpartum phase.
Trial status
The cluster randomized trial of P4HP will starts Q1 2022. After implementation and evaluation, the final results will be available by Q4 2023.
Availability of data and materials
Data sharing does not apply to this article as no datasets have yet been generated or analysed.
Change history
14 February 2022
A Correction to this paper has been published: https://doi.org/10.1186/s12889-022-12714-y
Abbreviations
- C-RCT:
-
Cluster randomized controlled trial
- DHD2015- index:
-
The Dutch Healthy Diet index 2015
- GSRH:
-
General Self-Rated Health
- P4HP:
-
Power 4 a Healthy Pregnancy
- PRES:
-
Pregnancy Related Empowerment Score
- QoL:
-
Quality of Life
- SES:
-
Socioeconomic status
- SOC:
-
Sense of Coherence
- SRH:
-
Self-Rated Health
- SPIRIT:
-
Standard Protocol Items Recommendations for Interventional Trials
- VAS:
-
Visual Analogue Scale
References
Harding JE. The nutritional basis of the fetal origins of adult disease. Int J Epidemiol. 2001;30(1):15–23.
Henriksen T. Nutrition and pregnancy outcome. Nutr Rev. 2006;64(5):19–23.
Ramakrishnan U, Grant F, Goldenberg T, Zongrone A, Martorell R. Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: a systematic review. Paediatr Perinat Epidemiol. 2012;26:285–301.
Stang J, Huffman LG. Position of the academy of nutrition and dietetics: obesity, reproduction, and pregnancy outcomes. J Acad Nutr Diet. 2016;116(4):677–91.
Lucas C, Charlton KE, Yeatman H. Nutrition advice during pregnancy: do women receive it and can health professionals provide it? Matern Child Health J. 2014;18(10):2465–78.
Garnweidner ML, Sverre Pettersen K, Mosdøl A. Experiences with nutrition-related information during antenatal care of pregnant women of different ethnic backgrounds residing in the area of Oslo, Norway. Midwifery. 2013;29(12):e130–7.
Szwajcer E, Hiddink G, Koelen M, Woerkum C. Nutrition-related information-seeking behaviours before and throughout the course of pregnancy: consequences for nutrition communication. Eur J Clin Nutr. 2005;59(Suppl 1):S57–65.
Malek L, Umberger W, Makrides M, Zhou SJ. Adherence to the Australian dietary guidelines during pregnancy: evidence from a national study. Public Health Nutr. 2015;19(7):1155–63.
Geurts M, van Rossum CTM, Geurts M, Van Rossum CTM. De Nederlandse voedselconsumptie vergeleken met de Richtlijnen voedselkeuze. Resultaten op basis van de Nederlandse Voedselconsumptiepeiling 2007-2010. Bilthoven: RIVM; 2014. Available from: https://www.rivm.nl/bibliotheek/rapporten/2014-0135.pdf
Baron R, Manniën J, te Velde SJ, Klomp T, Hutton EK, Brug J. Socio-demographic inequalities across a range of health status indicators and health behaviours among pregnant women in prenatal primary care: a cross-sectional study. BMC Pregnancy Childbirth. 2015;15(1):261.
Hure A, Young A, Smith R, Collins C. Diet and pregnancy status in Australian women. Public Health Nutr. 2009;12(6):853–61.
Mei Z, Cogswell ME, Looker AC, Pfeiffer CM, Cusick SE, Lacher DA, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1999–2006. Am J Clin Nutr. 2011;93(6):1312–20.
Pinto E, Barros H, dos Santos Silva I. Dietary intake and nutritional adequacy prior to conception and during pregnancy: a follow-up study in the north of Portugal. Public Health Nutr. 2009;12(7):922–31.
Rifas-Shiman S, Rich-Edwards JW, Kleinman KP, Oken E, Gillman MW. Dietary quality during pregnancy varies by maternal characteristics in project viva: A US cohort. J Am Diet Assoc. 2009;109(6):1004–11.
Watts V, Rockett H, Baer H, Leppert J, Colditz G. Assessing diet quality in a population of low-income pregnant women: a comparison between native Americans and whites. Matern Child Health J. 2007;11(2):127–36.
Blumfield ML, Hure AJ, Macdonald-Wicks L, Smith R, Collins CE. Systematic review and meta-analysis of energy and macronutrient intakes during pregnancy in developed countries. Nutr Rev. 2012;70(6):322–36.
Stothard KJ, Tennant PWG, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies. JAMA. 2009;301(6):636.
Edvardsson K, Ivarsson A, Eurenius E, Garvare R, Nyström ME, Small R, et al. Giving offspring a healthy start: parents’ experiences of health promotion and lifestyle change during pregnancy and early parenthood. BMC Public Health. 2011;11(1):936.
Olson CM. Tracking of food choices across the transition to motherhood. J Nutr Educ Behav. 2005;37(3):129–36.
Szwajcer EM, Hiddink GJ, Koelen MA, van Woerkum CMJ. Nutrition awareness and pregnancy: implications for the life course perspective. Eur J Obstet Gynecol Reprod Biol. 2007;135(1):58–64.
Lindqvist M, Lindkvist M, Eurenius E, Persson M, Mogren I. Change of lifestyle habits – motivation and ability reported by pregnant women in northern Sweden. Sex Reprod Healthc. 2017;13:83–90.
WHO. Good maternal nutrition the best start in life. Copenhagen: WHO Regional Office for Europe; 2016. Available from: https://www.euro.who.int/__data/assets/pdf_file/0008/313667/Good-maternal-nutrition-The-best-start-in-life.pdf
Baron R, Heesterbeek Q, Manniën J, Hutton EK, Brug J, Westerman MJ. Exploring health education with midwives, as perceived by pregnant women in primary care: a qualitative study in the Netherlands. Midwifery. 2017;46:37–44.
Bookari K, Yeatman H, Williamson M. Informing nutrition care in the antenatal period: pregnant women’s experiences and need for support. Biomed Res Int. 2017;2017:4856527.
Beulen YH, Super S, Rothoff A, van der Laan NM, de Vries JHM, Koelen MA, et al. What is needed to facilitate healthy dietary behaviours in pregnant women: a qualitative study of Dutch midwives’ perceptions of current versus preferred nutrition communication practices in antenatal care. Midwifery. 2021;103:103159.
Szwajcer E, Hiddink GJ, Maas L, Koelen MA, van Woerkum C. Nutrition awareness before and throughout different trimesters in pregnancy: a quantitative study among Dutch women. Fam Pract. 2012;29(Suppl 1):i82–8.
McCann MT, Newson L, Burden C, Rooney JS, Charnley MS, Abayomi JC. A qualitative study exploring midwives’ perceptions and knowledge of maternal obesity: reflecting on their experiences of providing healthy eating and weight management advice to pregnant women. Matern Child Nutr. 2018;14(2):e12520 2017/09/25 ed.
Schmied VA, Duff M, Dahlen HG, Mills AE, Kolt GS. ‘Not waving but drowning’: a study of the experiences and concerns of midwives and other health professionals caring for obese childbearing women. Midwifery. 2011;27(4):424–30.
Arrish J, Yeatman H, Williamson M. Midwives’ role in providing nutrition advice during pregnancy: meeting the challenges? A qualitative study. Nurs Res Pract. 2017;2017:7698510.
Aquino MRJRV, Olander EK, Needle JJ, Bryar RM. Midwives’ and health visitors’ collaborative relationships: a systematic review of qualitative and quantitative studies. Int J Nurs Stud. 2016;62:193–206.
Psaila K, Schmied V, Fowler C, Kruske S. Interprofessional collaboration at transition of care: perspectives of child and family health nurses and midwives. J Clin Nurs. 2014;24(1–2):160–72.
Watson BM, Heatley ML, Gallois C, Kruske S. The importance of effective communication in interprofessional practice: perspectives of maternity clinicians. Health Commun. 2015;31(4):400–7.
McCann MT, Newson L, Burden C, Rooney JS, Charnley MS, Abayomi JC. A qualitative study exploring midwives’ perceptions and knowledge of maternal obesity: reflecting on their experiences of providing healthy eating and weight management advice to pregnant women. Matern Child Nutr. 2018;14(2):1–9.
Arrish J, Yeatman H, Williamson M. Midwives and nutrition education during pregnancy: a literature review. Women Birth. 2014;27(1):2–8.
Arrish J, Yeatman H, Williamson M. Australian midwives and provision of nutrition education during pregnancy: a cross sectional survey of nutrition knowledge, attitudes, and confidence. Women Birth. 2016;29(5):455–64.
Szwajcer EM, Hiddink GJ, Koelen MA, van Woerkum CMJ. Written nutrition communication in midwifery practice: what purpose does it serve? Midwifery. 2009;25(5):509–17.
Baron R, Martin L, Gitsels-van der Wal JT, Noordman J, Heymans MW, Spelten ER, et al. Health behaviour information provided to clients during midwife-led prenatal booking visits: findings from video analyses. Midwifery. 2017;54:7–17.
Driessens K, van Regenmortel T, Vansevenant K. Bind-Kracht in Armoede: Krachtgerichte hulpverlening in dialoog. Maatwerk. 2010;11:17–9.
Aubel J. Communication for empowerment: strengthening partnerships for community health and development. New York: Unicef; 2001. (UNICEF Working Paper Series)
Heyden MLM, Fourné SPL, Koene BAS, Werkman R, Ansari SS. Rethinking ‘top-down’ and ‘bottom-up’ roles of top and middle managers in organizational change: implications for employee support. J Manag Stud. 2017;54(7):961–85.
Njøs R, Fosse JK. Linking the bottom-up and top-down evolution of regional innovation systems to policy: organizations, support structures and learning processes. Ind Innov. 2018;26(4):419–38.
Super S, Wagemakers A. Understanding empowerment for a healthy dietary intake during pregnancy. Int J Qual Stud Health Well Being. 2021;16(1):1857550.
Beulen YH, Super S, de Vries JHM, Koelen MA, Feskens EJM, Wagemakers A. Dietary interventions for healthy pregnant women: a systematic review of tools to promote a healthy antenatal dietary intake. Nutrients. 2020;12(7):1981.
Beulen YH, Geelen A, de Vries JH, Super S, Koelen MA, Feskens EJ, et al. Optimizing low–socioeconomic status pregnant women’s dietary intake in the Netherlands: protocol for a mixed-methods study. JMIR Res Protoc. 2020;9(2):e14796.
Super S, Beulen Y, Wagemakers A. Collaboration between midwives and dietitians in improving dietary intake of low SES women. Eur J Pub Health. 2019;29(4):ckz186.119.
Sallis JF, Owen N. Ecological models of health behavior. In: Health behavior: theory, research, and practice. 5th ed. Hoboken: Jossey-Bass/Wiley; 2015. p. 43–64.
Vaandrager L, Wagemakers A, Saan H. Evidence in gezondheidsbevordering. Tijdschr Gezondheidswetenschappen. 2010;88(5):271–7.
Cyril S, Smith BJ, Renzaho AMN. Systematic review of empowerment measures in health promotion. Health Promot Int. 2016;31(4):809–26.
Brandstetter S, Rüter J, Curbach J, Loss J. A systematic review on empowerment for healthy nutrition in health promotion. Public Health Nutr. 2015;18(17):3146–54.
Onah MN, Horton S, Hoddinott J. What empowerment indicators are important for food consumption for women? Evidence from 5 sub-Sahara African countries. PLoS One. 2021;16(4):e0250014.
Kruse M. Assessing the role of women empowerment for food security and nutrition: empirical evidence from Tunisia and India [Dissertation]. Goettingen: Georg-August-University; 2019. Available from: https://ediss.uni-goettingen.de/handle/21.11130/00-1735-0000-0003-C169-D
Sraboni E, Quisumbing A. Women’s empowerment in agriculture and dietary quality across the life course: evidence from Bangladesh. Food Policy. 2018;81:21–36.
Misgina KH, van der Beek EM, Boezen HM, Bezabih AM, Groen H. Pre-conception and prenatal factors influencing gestational weight gain: a prospective study in Tigray region, northern Ethiopia. BMC Pregnancy Childbirth. 2021;21(1):718.
Moattari M, Ebrahimi M, Sharifi N, Rouzbeh J. The effect of empowerment on the self-efficacy, quality of life and clinical and laboratory indicators of patients treated with hemodialysis: a randomized controlled trial. Health Qual Life Outcomes. 2012;10(1):115.
Bravo P, Edwards A, Barr PJ, Scholl I, Elwyn G, McAllister M, et al. Conceptualising patient empowerment: a mixed methods study. BMC Health Serv Res. 2015;15(1):252.
Super S, Wagemakers ME, Picavet HSJ, Verkooijen KT, Koelen MA. Strengthening sense of coherence: opportunities for theory building in health promotion. Health Promot Int. 2016;31(4):869–78.
Koelen MA, Lindström B. Making healthy choices easy choices: the role of empowerment. Eur J Clin Nutr. 2005;59:S10–6.
Kim J-R, Jeong B, Park K, Kang Y-S. The associations of empowerment and social capital with self-rated health in communities with poor health. J Agric Med Community Health. 2012;37(3):131–44.
Rohrer JE, Wilshusen L, Adamson SC, Merry S. Patient-centredness, self-rated health, and patient empowerment: should providers spend more time communicating with their patients? J Eval Clin Pract. 2008;14(4):548–51.
Milte CM, Thorpe MG, Crawford D, Ball K, McNaughton SA. Associations of diet quality with health-related quality of life in older Australian men and women. Exp Gerontol. 2015;64:8–16.
McNaughton SA, Crawford D, Ball K, Salmon J. Understanding determinants of nutrition, physical activity and quality of life among older adults: the Wellbeing, Eating and Exercise for a Long Life (WELL) study. Health Qual Life Outcomes. 2012;10(1):109.
Kye S-Y, Yun E-H, Park K-H. Factors related to self-perception of diet quality among south Korean adults. Asian Pac J Cancer Prev. 2012;13(4):1495–504.
Lindmark U, Stegmayr B, Nilsson B, Lindahl B, Johansson I. Food selection associated with sense of coherence in adults. Nutr J. 2005;4(1):9.
Collins CE, Young AF, Hodge A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J Am Coll Nutr. 2008;27(1):146–57.
Goodwin DK, Knol LL, Eddy JM, Fitzhugh EC, Kendrick OW, Donahue RE. The relationship between self-rated health status and the overall quality of dietary intake of US adolescents. J Am Diet Assoc. 2006;106(9):1450–3.
Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586.
Chan A-W, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–7.
Hemming K, Eldridge S, Forbes G, Weijer C, Taljaard M. How to design efficient cluster randomised trials. BMJ. 2017;358:j3064.
Research Methods Resources. National Institutes of Health. Available from: https://researchmethodsresources.nih.gov/. Accessed 12 Dec 2021.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: L. Erlbaum Associates; 1988. p. 567.
Duijzer G, Haveman-Nies A, Jansen SC, ter Beek J, van Bruggen R, Willink MGJ, et al. Effect and maintenance of the SLIMMER diabetes prevention lifestyle intervention in Dutch primary healthcare: a randomised controlled trial. Nutr Diabetes. 2017;7(5):e268.
Centraal Bureau voor de Statistiek. Hoogste aantal geboorten in 10 jaar tijd. Centraal Bureau voor de Statistiek. Available from: https://www.cbs.nl/nl-nl/nieuws/2021/46/hoogste-aantal-geboorten-in-10-jaar-tijd. Accessed 21 Dec 2021.
Looman M, Feskens EJ, de Rijk M, Meijboom S, Biesbroek S, Temme EH, et al. Development and evaluation of the Dutch healthy diet index 2015. Public Health Nutr. 2017;20(13):2289–99.
Patterson RE, Haines PS, Popkin BM. Diet quality index: capturing a multidimensional behavior. J Am Diet Assoc. 1994;94(1):57–64.
Drewnowski A, Henderson SA, Shore A, Fischler C, Preziosi P, Hercberg S. Diet quality and dietary diversity in France: implications for the French paradox. J Am Diet Assoc. 1996;96(7):663–9.
Alkerwi A. Diet quality concept. Nutrition. 2014;30(6):613–8.
de Rijk MG, Slotegraaf AI, Brouwer-Brolsma EM, Perenboom CW, Feskens EJ, de Vries JH. Development and evaluation of a diet quality screener to assess adherence to the Dutch food-based dietary guidelines. Br J Nutr. 2021:1–28. https://doi.org/10.1017/S0007114521004499.
Gezondheidsraad. Voedingsaanbevelingen voor zwangere vrouwen. Den Haag: Gezondheidsraad; 2021. p. 74. Report No.: 2021/26
Klima CS, Vonderheid SC, Norr KF, Park CG. Development of the pregnancy-related empowerment scale. nh. 2015;3(5):120–7.
Lundberg O, Peck MN. A simplified way of measuring sense of coherence: experiences from a population survey in Sweden. Eur J Pub Health. 1995;5(1):56–9.
Eriksson M, Lindström B. Validity of Antonovsky’s sense of coherence scale: a systematic review. J Epidemiol Community Health. 2005;59(6):460–6.
Olsson M, Gassne J, Hansson K. Do different scales measure the same construct? Three sense of coherence scales. J Epidemiol Community Health. 2009;63(2):166–7.
Généreux M, Schluter PJ, Hung KK, Wong CS, Pui Yin Mok C, O’Sullivan T, et al. One virus, four continents, eight countries: an interdisciplinary and international study on the psychosocial impacts of the COVID-19 pandemic among adults. IJERPH. 2020;17(22):8390.
Lindfors P, Lundberg O, Lundberg U. Sense of coherence and biomarkers of health in 43-year-old women. Int J Behav Med. 2005;12(2):98–102.
Super S, Verschuren WMM, Zantinge EM, Wagemakers MAE, Picavet HSJ. A weak sense of coherence is associated with a higher mortality risk. J Epidemiol Community Health. 2014;68(5):411–7.
Thompson K, Herens M, van Ophem J, Wagemakers A. Strengthening sense of coherence: evidence from a physical activity intervention targeting vulnerable adults. Prev Med Rep. 2021;24:101554.
Herens M, Bakker EJ, van Ophem J, Wagemakers A, Koelen MA. Health-related quality of life, self-efficacy and enjoyment keep the socially vulnerable physically active in community-based physical activity programs: a sequential cohort study. PLoS One. 2016;11(2):e0150025.
Bowling A. Just one question: if one question works, why ask several? J Epidemiol Community Health. 2005;59(5):342–5.
Fayers PM, Hand DJ. Causal variables, indicator variables and measurement scales: an example from quality of life. J R Stat Soc Ser A (Stat Soc). 2002;165(2):233–53.
de Boer AGEM, van Lanschot JJB, Stalmeier PFM, van Sandick JW, Hulscher JBF, de Haes JCJM, et al. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual Life Res. 2004;13(2):311–20.
Schnittker J, Bacak V. The increasing predictive validity of self-rated health. PLoS One. 2014;9(1):e84933.
DeSalvo KB, Jones TM, Peabody J, McDonald J, Fihn S, Fan V, et al. Health care expenditure prediction with a single item, self-rated health measure. Med Care. 2009;47(4):440–7.
DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. J Gen Intern Med. 2006;21(3):267–75.
Daniilidou NV, Gregory SP, Zavras DJ, Pavi EA, Athanasakis KP, Lionis CD, et al. Comparison between two different measures of self-rated health: a single-question measure and a visual analogue scale. Folia Med (Plovdiv). 2010;52(1):63–9.
FORUM. Older Americans 2020 - key indicators of well-being. Washington, DC: The Federal Interagency Forum on Aging-Related Statistics (Forum); 2020. Available from: https://agingstats.gov/docs/LatestReport/OA20_508_10142020.pdf
Boumans J. Naar het hart van empowerment Deel 1. Een onderzoek naar de grondslagen van empowerment van kwetsbare groepen. Utrecht: Movisie; 2012.
Ministerie van Sociale Zaken en Werkgelegenheid. Empowerment: zet mensen in hun kracht - Durf, doe, divers - Uitvoering van Beleid. Ministerie van Sociale Zaken en Werkgelegenheid; 2018. Available from: https://www.uitvoeringvanbeleidszw.nl/subsidies-en-regelingen/gelijke-kansen-en%2D%2Dnon-discriminatie/doe-je-mee/tips-en-verslagen/empowerment-zet-mensen-in-hun-kracht. Accessed 1 Dec 2021.
Voedingscentrum. Hoe eet ik gezond tijdens mijn zwangerschap? Available from: https://www.voedingscentrum.nl/nl/zwanger-en-kind/zwanger/gezond-eten-tijdens-de-zwangerschap.aspx. Accessed 1 Dec 2021.
Ministerie van Volksgezondheid, Welzijn en Sport. Nationaal Preventiekkoord: Naar een gezonder Nederland. Den Haag: Ministerie van Volksgezondheid, Welzijn en Sport; 2018. p. 76.
Expertgroep Zorgstandaard Integrale Geboortezorg. Zorgstandaard Integrale Geboortezorg. Utrecht: Expertgroep Zorgstandaard ‘Integrale geboortezorg’; 2016. p. 67. Report No.: 1.1. Available from: https://www.nvog.nl/wp-content/uploads/2019/04/Integrale-Geboortezorg-2016.pdf
Zwangerschap app: ZwangerHap | Voedingscentrum. Available from: https://www.voedingscentrum.nl/nl/thema/apps-en-tools-voedingscentrum/zwangerschap-app-zwangerhap.aspx. Accessed 6 Dec 2021.
Poelman T. Continue variabelen analyseren met ANCOVA. Minerva. 2014;13(8):103.
Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–46.
Hochwälder J. Sense of coherence: notes on some challenges for future research. SAGE Open. 2019;9(2):2158244019846687.
Acknowledgments
We thank dr. Joao Paulo for statistical advice regarding Linear Mixed Models.
Funding
Funding has been provided by ZonMw, The Netherlands Organisation for Health Research and Development, and Regiodeal Foodvalley. Both funders had no role in the design of this study and writing of the manuscript and will not have any role during its execution, analysis, interpretation of data, or submission of outcomes.
Author information
Authors and Affiliations
Contributions
RL is the principal investigator of this trial. RL, SC, JV, and AW conceptualized and designed the trial. EF carried out the sample size estimation. RL and SC carry out the study. RL, SC, JV, and AW repeatedly read and revised the manuscript. All authors approved the final manuscript.
Authors’ information
RM (Renske) van Lonkhuijzen, MSc, is promovendus at the WUR chair group Health and Society. After obtaining a Bachelor in Health and Society, she graduated cum laude from the Master’s degree in Communication, Health and Life Sciences (specialization in Health and Society) from WUR. Her current research focuses on improving the diet quality of pregnant women using empowerment. In addition, her research interests are women’s health, health inequalities, and the stigma surrounding menstruation.
S (Susanne) Cremers, MSc, is a researcher at the WUR chair group Health and Society. She holds a MSc in Business administration from the University of Potsdam in Germany and a MSc in Nutrition & Health from WUR. After working as a medical advisor in cardiovascular and metabolic diseases in pharmaceutical companies, she returned to WUR as a researcher, where she focuses on the empowerment of pregnant women with low socioeconomic status by implementing and evaluating an integral strategy to improve dietary intake. In addition to a university nutrition background, she has completed lifestyle coach training, which means that she is in an excellent position to recruit and support midwifery practices and dietitians in executing the strategy and taking care of data collection. Besides her work at WUR, Susanne works as a trainer at Mom in Balance, where she works on the empowerment of (pregnant) women by providing outdoor workouts.
dr. JHM (Jeanne) de Vries is Assistant Professor at the WUR division of Human Nutrition and Health. She is an expert in the assessment of dietary intake and dietary advice in different target groups, including pregnant women. Jeanne de Vries is a nutritionist with a background in dietetics. As a project leader, she had an important role in the development of the dietary assessment tool Eetscore to monitor diet quality. Her experience in working together with dieticians and her experience in nutrition research will particularly contribute to this project.
prof.dr.ir. EJM (Edith) Feskens is chair of the WUR group Global Nutrition. She has wide experience in nutritional epidemiology, including the use and validation of various tools of dietary exposure, including diet histories, FFQs, and biomarkers. She has been involved in projects relating diet to obesity and prevention of type 2 diabetes, focusing on nutrients and foods as well as dietary patterns, and including low SES risk groups. She currently heads a WUR-based longitudinal study NQplus and WP1 of the large collaborative project Regiodeal Foodvalley Nutrition and Health.
dr.ir. MAE (Annemarie) Wagemakers is Associate Professor at the WUR chair group Health and Society. She has wide experience with complex public health promotion projects, including projects focusing on midwives and pregnant women. She is project leader and (co-)promotor in the projects ‘Why pregnant women eat what they eat’, ‘Empowerment of pregnant women to have a healthier dietary intake. The development, implementation, and evaluation of an integral strategy’ and several other projects on community-based health promotion with a focus on facilitating and evaluating intersectoral collaboration and participation. Many of her public health projects use mixed methods and interdisciplinary approaches to collect data and build strongly on stakeholder participation including low SES groups.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This project has been approved by the Medical Research Ethics Committee Utrecht, code 21/526D, dossier NL78194.041.21. All participating pregnant women will be asked to provide their written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article has been updated to correct the author names.
Supplementary Information
Additional file 1.
Completed SPIRIT guidelines checklist for this P4HP cluster randomized trial protocol article.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
van Lonkhuijzen, R.M., Cremers, S., de Vries, J.H.M. et al. Evaluating ‘Power 4 a Healthy Pregnancy’ (P4HP) – protocol for a cluster randomized controlled trial and process evaluation to empower pregnant women towards improved diet quality. BMC Public Health 22, 148 (2022). https://doi.org/10.1186/s12889-022-12543-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12543-z