
Abstract
Background
Breast cancer represented the leading cause of cancer deaths among women in Japan. Although physical activity has been reported protective against breast cancer, scientific evidence is limited on the risk of breast cancer according to job category or occupational activity in Japanese. Our objective was to examine the association of job category and occupational activity with breast cancer incidence in Japanese female workers using the data from the Japan Collaborative Cohort (JACC) Study.
Methods
A prospective cohort study involving 19,041 women aged 40–79 years who have reported their occupational data and followed-up from 1988 to 2009. All variables were assessed by a self-administered questionnaire. Cancer incidence data were obtained from 24 areas of the JACC study through cancer population data registration, or review of hospital records. The Cox proportional hazard models were operated to calculate the hazard ratios (HRs) and corresponding 95% confidence intervals (CIs).
Results
There were 138 incident cases of breast cancer during 13.3 years median follow-up period. Office workers compared with manual workers were at a higher risk of breast cancer after adjusting for reproductive health factors and physical activity indicators; the multivariable HR (95% CI) was 1.65 (1.07–2.55). Also, women who had mainly a sitting position during work compared with those moving during work had the higher risk: the multivariable HR (95%CI) of 1.45 (1.01–2.12). The excess risk of breast cancer was observed for office workers when time spent in walking was < 30 min/ day; HR (95% CI) was 1.11 (1.01–1.23), and for women mainly at a sitting position during work when time spent in walking was 30–59 min or < 30 min/day; HRs (95% CIs) were 1.87 (1.07–3.27) and 1.74 (1.07–2.83), respectively.
Conclusion
The job category and occupational activity were associated with risk of breast cancer incidence. A high risk was observed in office workers and in women with a sitting position during work. These observed increased risks were evident in women with less daily walking activity.
Similar content being viewed by others


Background
Breast cancer is the most common cancer in women worldwide. Since 1975, the incidence rate of breast cancer in Japan has been increasing, especially among women aged 40 years and above. In 2018, there were 157,000 cases of cancer mortality in Japanese women, and breast cancer was the leading cause of cancer death (9%) [1].
Prolonged exposures to estrogen critically contribute to the development of breast cancer [2,3,4]. Regular physical activity can reduce the adverse effect of estrogen [5]; physical activity decreases the luteal phase length of the ovulation cycle which reduces the cumulative ovarian hormone exposure [6,7,8,9].
Previous studies have indicated the association between the type of occupation and the breast cancer risk [8,9,10,11,12]. The initial investigations were extended to examine the effects of physical activity during [8, 10, 11] and outside work [9, 11, 12] on the risk of breast cancer. A previous report on the Japan Collaborative Cohort (JACC) study stated that the risk of mortality from breast cancer was lower among female manual workers than female office workers. However, the researchers in this report did not account for physical activity that occurs during work [13]. A study on Nordic countries reported that among the national population of women, women who work outdoors (e.g., gardeners, farmers, and woodworkers) had a lower risk of developing breast cancer compared with the entire national females [14]. Many studies on Western and Asian countries have shown that involving in physically active jobs is inversely associated with the risk of breast cancer, while sedentary or office work has a positive association [10, 15,16,17,18,19]. However, a pooled analysis of two case-control studies in Australia and Canada reported no association between occupational activity level and the risk of developing breast cancer [20].
The discussion thus far highlights the lack of scientific evidence for Japanese women on the risk of developing breast cancer on the basis of job category or occupational activity. Thus, we aimed in our research to assess the associations of job category (manual, office, professional, and unclassified) and occupational activity (moving, mainly standing and mainly sitting) with the risk of breast cancer incidence among Japanese female workers. We conducted stratified analyses on the basis of physical activity indicated by walking time per day (indoor, work, home and outdoor). We hypothesized that job category and occupational activity are associated with the risk of breast cancer incidence among Japanese female workers and that the level of physical activity (walking time) would influence these associations.
Methods
Study population and setting
A description of the population and research settings has been provided previously [21]. The JACC study is one of the largest multicenter collaborative cohort studies and was conducted from 1988 to 2009 across 45 areas in Japan, comprising three towns in Hokkaido; five towns in Tohoku district; five towns in Kanto district; one city, three towns, and two villages in Chubu district; eight towns and two villages in Kinki district; one city and one town in Chugoku district; and four cities, nine towns, and one village in Kyushu district.
For a follow-up period of approximately 20 years, data on all-cause deaths and cause-specific mortalities were assessed along with their associated risk factors. The purpose of the JACC Study was to evaluate the impact of lifestyle on human health including cancer and cardiovascular diseases.
The cancer incidence data in the JACC study were available for 24 Japanese areas with cancer incidence data registry, covering all of Japan from Hokkaido, Tohoku, Kanto, Chubu, Kinki, and Chugoku, to Kyushu. The follow-up was completed for one area each in 1994, 1999, 2000, 2002, and 2003; for two areas each in 1997, 2006, and 2008; and for 13 areas in 2009 [21].
Of the women living in the 24 areas, a total of 38,613 participants aged between 40 to 79 years took part in the baseline survey of the JACC study. In a self-administered questionnaire (details were published elsewhere [21]), women were asked to specify their job type into employed, self-employed, part-time, housewife, or unemployed, and accordingly we excluded 6913 women who were unemployed. We further excluded 3731 women living in two areas where the occupation-related questions were not asked, and 8928 women who did not answer the occupation-related questions (6732 women with missing data on the job category and 2196 women with missing data on the occupational activity). Thus, the total number of eligible respondents for this study was 19,041 women (Fig. 1).

Flow chart for the calculation of respondents
Assessments of job category, occupational activity and other covariates
In a self-administered questionnaire, participants were further asked to classify their job category into office, manual and others. Based on the Japan Standard Industry Classification (JSIC) published by the Ministry of Internal Affairs and Communication of Japan which included a wide range of specific jobs coded from 1 to 99 [22], the participants who answered the job category as others were allocated to manual (for examples; sales, restaurant, forestry, fisheries workers, etc.), office (for examples; clerk, postal, management staff, etc.), professional (for examples; health worker, judges, accountant, musician, etc.) and unclassified job categories. For the current research, we reclassified job categories into four categories namely manual, office, professional and unclassified. The occupational activity was classified according to the position during work as moving, mainly standing and mainly sitting.
Other covariates included on the questionnaire were used as confounding factors to strengthen the results: body mass index (BMI) calculated as weight in kg divided by squared height in m (< 18.5, 18.5–24.9, 25–29.9, ≥ 30 kg/m2); smoking status (never, ex-smoker, or current smoker); alcohol intake (never, ex-drinker, or current drinker); education (≤ 15 years, or ≥ 16 years), family history of cancer (yes or no), feeling daily stress (stressful, normal, or less stressful); and reproductive health factors, such as marital status (married and unmarried), age at menarche (< 14 years or ≥ 14 years), age at menopause (≤ 50 years or > 50 years), and number of deliveries (0, 1, 2, or ≥ 3). The last group of confounding factors were those specific to our priori set hypothesis for physical activity indicators: walking time (< 30 min/ day, 30–59 min/ day, or ≥ 1 h/ day) and sport time (< 1 h/ week, 1–2 h/ week, or ≥ 3 h/ week). Dummy variables representing missing observations of each confounder were added to the model.
Outcome assessment
Breast cancer incidence data, comprising the diagnosis date and primary site of cancer, were confirmed through records in the population-based cancer registries for each cohort study area, supplemented by a systematic review of death certificates and medical records from major local hospitals in the 24 study areas [21, 23,24,25]. Breast cancer diagnosis was determined as per code C50 in the International Classification of Diseases, ninth revision (ICD-9), used from the baseline JACC survey to 1994; and the tenth revision (ICD-10) used post-1995 [21, 23,24,25,26,27]; in both, C50 codes for malignant neoplasm of the breast, not including ductal carcinoma, in situ.
Statistical analysis
The baseline risk characteristics were presented as mean values (standard deviations) and proportions. The risk of breast cancer according to the job category and occupational activity was assessed by estimating the hazard ratios (HRs) with 95% confidence intervals (CIs) using the Cox proportional hazards regression models adjusted for the abovementioned confounding factors.
Additionally, the associations of the breast cancer risk with the job category and occupational activity were tested after the stratification by walking time (< 30 min/day, 30–59 min/day, or ≥ 1 h/day).
Next, a sensitivity analysis was conducted by excluding participants who reported they were housewives under the job type question. The objective of this analysis was to determine the strength of the relationship that job category and occupational activity has with the incidence of breast cancer.
Ethical statement
Informed consent was obtained from the study participants or their community representatives prior to their participation in this study. The ethics committees of Nagoya University School of Medicine and Osaka University approved the protocol for this study.
Results
Participants characteristics
Table 1 shows the baseline characteristics of Japanese women according to the job category and occupational activity. The averages age and BMI of women were between 50.1 to 59.2 years and 22.4 to 22.8 kg/m2, respectively. Women who worked in office and women engaged in moving occupational activity were more likely to be drinkers. A family history of breast cancer was more commonly observed among women who were manual workers and women reporting mainly a standing position during work. Women who reported working in office jobs and women in mainly a sitting position during work had high perceived stress levels, were less likely to be multigravida for ≥3 children and were less likely to walk for ≥1 h/day.
The median follow-up time for this research was 13.3 years, and the number of newly diagnosed breast cancer cases was 138 among 19,041 women at risk.
Job category and risk of breast cancer
Table 2 shows that women who worked in an office were at a higher risk of developing breast cancer than manual workers even after controlling for reproductive health factors, education and BMI. However, the risk was slightly attenuated after controlling for the physical activity indicators; the multivariable HR (95% CI) was 1.65 (1.07–2.55) in the fully adjusted model. There was no excess risk of breast cancer in professional or unclassified workers compared with manual workers.
Occupational activity and risk of breast cancer
A higher risk of breast cancer was observed among women with mainly a sitting occupation activity than in those with a moving occupation activity. The association was slightly attenuated after controlling for the physical activity indicators; the multivariable HR (95% CI) was 1.45 (1.01–2.12) (Table 2).
Sensitivity analysis
Excluding the 3626 women who reported their type of job as housewives attenuated the association of office work and mainly a sitting occupational activity with breast cancer incidence risk. The multivariable HRs (95% CIs) were 1.54 (0.97–2.44) and 1.45 (0.97–2.18), respectively (Additional file 1).
Stratified analyses
Table 3 shows the HRs of breast cancer incidence for each job category and occupational activity after stratification by the daily walking time. The observed associations of office versus manual job categories and sitting versus moving occupational activities with the risk of higher breast cancer were evident for women who walked less frequently on a daily basis. The multivariable HR (95% CI) for breast cancer among office versus manual workers who walked for < 30 min/ day was 1.11 (1.01–1.23). The respective risk estimates for women with a sitting versus a moving occupational activity were 1.87 (1.07–3.27) among women who walked 30–59 min/ day and 1.74 (1.07–2.83) among those who walked < 30 min/ day.
Discussion
This cohort study supports the evidence for the associations of job category and occupational activity with the risk of breast cancer incidence among Japanese women. Office workers were at a higher risk of developing breast cancer than manual workers. In addition, women who were mainly in a sitting position during work were at a higher risk of developing breast cancer than those who were moving during work. These associations were evident for women who report less walking activity on a daily basis.
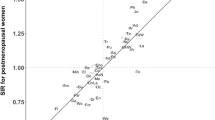
Several previous studies on non-Asian [14, 28, 29] and Asian population [7, 13, 16, 30,31,32] have shown similar associations between occupation and risk of breast cancer. A case-control study in Massachusetts on women aged ≤74 years (6835 cases of breast cancer and 9453 controls) reported a higher risk of breast cancer among women who worked in administrative occupations (multivariable OR = 1.15, 95% CI = 1.06–1.24) than in housewives [28]. Another study highlighted that among 7.5 million Nordic women, women with manual jobs reported a lower risk of breast cancer, such as gardeners (age-adjusted relative risk: RR = 0.76, 95% CI = 0.74–0.78), farmers (RR = 0.80, 95% CI = 0.78–0.82), and woodworkers (RR = 0.75, 95% CI = 0.70–0.81), whereas the risk was higher among women who were dentists (RR = 1.43, 95% CI = 1.31–1.56) and physicians (RR = 1.35, 95% CI = 1.26–1.46) in reference to the entire national female study population [14]. In a study on women in Shanghai, the lowest standardized incidence ratios (SIR) for breast cancer were observed for manual workers, such as women working in construction (SIR = 0.5, 95% CI = 0.3–0.9) or production (SIR = 0.6, 95% CI = 0.5–0.8), whereas the highest SIRs were found in women who worked in office such as researchers (SIR = 3.3,95% CI = 1.4–6.5) and administrative clerks (SIR = 1.6,95% = 1.3–1.9) [31]. Similar results were observed in another Chinese study, where an inactive job classification was associated with higher SIRs not only of breast cancer, but also for uterine and ovarian cancer [7]. A previous report on the JACC study suggested that, compared with office workers, female manual workers were at a lower risk of breast cancer mortality (area-adjusted HR = 0.41, 95% CI = 0.19–0.92) [13].
In this study, female workers were at a higher risk of developing breast cancer if their occupational activity involved mainly a sitting rather than a moving position during work. The association between occupational activity and risk of breast cancer was consistent with the findings from previous non-Asian [8, 18, 19, 33,34,35,36] and Asian [7, 13, 16, 24, 30, 31, 37] studies. A case-control study of women aged 35–93 years in Stettin, Poland found that women aged > 55 years with a medium-level occupational physical activity were at a lower risk of developing breast cancer than those who had a sedentary occupational activity (multivariable OR = 0.40, 95% CI 0.20–0.81) [35]. Similar results were also reported by a Swedish population-based cohort study on 29,524 women (with 1506 breast cancer cases within the 24 years of follow-up). Compared with women who worked in non-sedentary occupations, the risk of developing breast cancer was higher for women who worked in sedentary occupations (HR = 1.54; 95% CI = 1.20–1.96), but not for women who worked in mixed occupations (HR = 1.08; 95% CI = 0.85–1.37) [19]. A prospective cohort study in China on a population of 73,049 Chinese women also reported that women with the lowest average occupational sitting time (< 3.69 h/ day) were at a lower risk of developing breast cancer (HR = 0.69; 95% CI 0.57–0.54) than those with an average sitting time ≥ 4 h/ day [16]. Two case-control studies in other Asian countries (India and China) have also reported that high occupational activity and exercise can help reduce the risk of breast cancer [37, 38].
The results of this study are also in line with the conclusion of two meta-analyses. The first meta-analysis was conducted on 14 case-control studies and 7 cohort studies with 2,625,772 participants and 82,630 breast cancer patients, and found an increased risk of breast cancer in women with a sedentary behaviour, including prolonged occupational sitting time (OR = 1.10, 95% CI = 1.02–1.18) [39]. The second meta-analysis was performed on 31 prospective studies involving 63,786 women and examined the association between physical activity and breast cancer risk [15]. This meta-analysis found that physical activity from occupational and non-occupational settings (i.e., leisure-time and household activities) was inversely associated with the risk of breast cancer. The analysis reported that the multivariable RR with 95% CI was 0.87 (0.83–0.91) for non-occupational activity and 0.90 (0.83–0.97) for occupational activity.
On the other hand, a prospective cohort study of 9539 twin Swedish women aged 42–70 years indicated no association of total physical activity, including both leisure and work activities with the risk of breast cancer; the age-adjusted RR (95% CI) was 0.9 (0.7–1.2) for active occupations in reference to sedentary occupations [40]. In addition, the prospective cohort study by European Prospective Investigation into Cancer and Nutrition (EPIC) found no difference in the risk of breast cancer among sedentary, standing and manual and heavy workers. In comparison with sedentary activities, the multivariable-adjusted HRs (95%CIs) were 0.92 (0.81–1.05) for standing, 1.08 (0.91–1.29) for manual and heavy manual labour activities [41]. Our study did not examine the risk of breast cancer incidence for the occupational activity of mainly standing position during work because of the small number of cases; however, a previous report on the JACC study stated that women who were generally required to stand during work were at a higher risk of mortality due to breast cancer (HR = 3.00, 95% CI = 1.06–8.42) than women who did sedentary work only [13]. The variations in the results between the EPIC study and our analysis can be attributed to the different definitions of the occupational activity categories and assessments of the physical activity. For example, the EPIC study [41], accounted for unemployed women under sedentary occupational activities (reference group), whereas our study excludes unemployed women. Previous studies have shown that unemployed women are at a higher risk of breast cancer [42]. Moreover, it is well-known that unemployment hinders breast cancer screening behavior among females in both Japan [43] and the United States [44].
In this study, the excess risk of breast cancer was still evident for office workers who walked for a duration of < 30 min/ day, when compared to manual workers. Also, an excess risk of breast cancer was observed among women who mainly sat during work compared to those who moved during work, and was particularly high when their walking duration was < 1 h/ day. This supports the evidence on the effect of physical activity, not only occupational, but also leisure activities, on the risk of developing breast cancer [6, 7, 10, 12, 15, 24]. A Swedish case-control study that included 3455 controls and 3347 post-menopausal cases of breast cancer found that working women with sedentary jobs and who rarely engaged in leisure-time activity were at a three-fold higher risk of breast cancer than women who were active within both inside and outside of workplace [6]. A previous report on the JACC study showed that the multivariable HR (95% CI) for breast cancer incidence was 0.45 (0.25–0.78) among women who walked ≥1 h per day and engaged in sport for ≥1 h/ day compared with women who walked < 1 h/ day and engaged in sport for < 1 h/ day [24]. However, the report did not account for physical activity during work or the job category. The Shanghai Women’s Health Study examined a joint effect of occupational sitting and adulthood exercise on the risk of breast cancer in post-menopausal women and showed a 30% risk reduction of breast cancer incidence in women who had either less occupational sitting time (≤ 2.1 h/ day) or who engaged in adequate exercise (≥ 8 metabolic equivalent units/ week) compared with women who reported both longer occupational sitting time (≥ 4 h/ day) and inadequate exercise (< 8 metabolic equivalent units/week). However, contrary to the present study, that study found no statistically significant interaction between occupational and leisure activities [16].
The breast cancer incidence risk is closely related to imbalances in sex hormones, and this is one mechanism that could explain our findings. High exposure to estrogen and other ovarian hormones plays an important role in the development of breast cancer [5, 6, 45]. Hormone imbalance is closely related to lifestyle factors, such as being physically inactive (indoors and outdoors) [2, 45]. Physical activity reduces the level of steroid sex hormones and this reduction decreases the risk of hormone-related cancers [45,46,47]. The 17-β-estradiol (E2) is an indicator of the development and prognosis of breast cancer [5]. A Polish study on urban and rural women showed that the concentration of this estradiol in saliva was 21% higher in low-activity groups than in high-activity groups [5]. Reduced exposures to insulin and insulin-like growth factors (IGFs) are potent stimulators of cell growth related to the development of breast cancer [39,40,41]. Physical activity increases the production of insulin-like growth factor-binding protein-1 (IGFBP-1), which down regulates IGFs [48, 49].
Our study makes several important contributions. We investigated a large population-based sample of women, with a high response rate and a long follow-up period. In addition, the prospective cohort design of our research allowed us to reduce several types of bias, especially recall bias. However, several limitations of this study need to be addressed. The use of a simple questionnaire at baseline to collect information about the job category, activity during work, and physical activity in general could result in some inevitable misclassifications. In addition, while the main analyses of job category and occupational activity with the risk of breast cancer beard reasonable numbers of cases in each category, the stratification analyses had small numbers of cases for certain categories and thus, lacked sufficient power to detect real associations. Therefore, the results from our stratified analyses should be carefully interpreted. The occupational and covariates data were obtained once and were self-reported; such data could have been changed during the extensive follow-up period. Further, some women reported being a housewife while classified their job category as office (n = 354), manual (n = 2265), or professional (n = 688); this might have led to some misclassifications by women in such job categories and still taking care of the housework. Excluding these participants attenuated the association, although the trend for a positive association of the office jobs and sitting occupational activity with the risk of breast cancer persisted. Finally, while we controlled for a wide range of possible confounders, the effect of certain residual confounding factors, such as the use of hormone replacement therapy, remains to be addressed.
Conclusion
In conclusion, the job category and occupational activity were associated with breast cancer incidence risk. Women who worked in office and those whose jobs mainly required them to sit were at the higher risk of developing breast cancer. The higher risk of breast cancer in office jobs and mostly sitting during work was evident among women whose walking activities were limited. Our findings imply that women who work in offices and mainly sit during the workday should increase their physical activity to reduce their risk of developing breast cancer.
Availability of data and materials
The data can be made available from the corresponding author under reasonable request.
Abbreviations
- JACC:
-
Japan Collaborative Cohort
- EPIC:
-
European Prospective Investigation into Cancer and Nutrition
References
Research F for P of C. Cancer Statistics in Japan - 2018. 2018;4–11. https://ganjoho.jp/data/reg_stat/statistics/brochure/2018/cancer_statistics_2018.pdf. Accessed 5 June 2019. .
Travis RC, Key TJ. Oestrogen exposure and breast cancer risk. Breast Cancer Res. 2003;5:239–47. https://doi.org/10.1186/bcr628.
Adraskela K, Veisaki E, Koutsilieris M, et al. Physical exercise positively in fl uences breast Cancer evolution. Clin Breast Cancer. 2017;17:408–17. https://doi.org/10.1016/j.clbc.2017.05.003.
Saika K, Sobue T. Epidemiology of breast cancer in Japan and the US. Japan Med Assoc J. 2009;52:39–44 http://www.med.or.jp/english/pdf/2009_01/039_044.pdf.
Jasienska G, Ziomkiewicz A, Thune I, et al. Habitual physical activity and estradiol levels in women of reproductive age. Eur J Cancer Prev. 2006;15:439–45. https://doi.org/10.1097/00008469-200610000-00009.
Moradi T, Olof N, Zack M, et al. Breast cancer risk and lifetime leisure-time and occupational physical activity ( Sweden ). Cancer Causes Control. 2000;11:523–31.
Chow W, Gao T. Occupational Physical Activity and the Incidence of Cancer of the Breast , Corpus Uteri , and Ovary in Shanghai. Cancer. 1993;71:3620–4.
Coogan PF, Newcomb PA, Clapp RW, et al. Physical activity in usual occupation and risk of breast cancer ( United States ). Cancer Causes Control. 1997;8:626–31.
Steindorf K, Ritte R, Eomois PP, et al. Physical activity and risk of breast cancer overall and by hormone receptor status: the European prospective investigation into cancer and nutrition. Int J Cancer. 2013;132:1667–78. https://doi.org/10.1002/ijc.27778.
George SM, Irwin ML, Matthews CE, et al. Beyond recreational physical activity: examining occupational and household activity, transportation activity, and sedentary behavior in relation to postmenopausal breast cancer risk. Am J Public Health. 2010;100:2288–95. https://doi.org/10.2105/AJPH.2009.180828.
Kyu HH, Bachman VF, Alexander LT, et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the global burden of disease study 2013. BMJ. 2016;354:1–10. https://doi.org/10.1136/bmj.i3857.
Levi F, Pasche C, Lucchini F, et al. Original paper occupational and leisure time physical activity and the risk of breast Cancer. Eur J Cancer. 1999;35:40–3.
Fujino Y. Occupational Factors and Mortality in the Japan Collaborative Cohort Study for Evaluation of Cancer (JACC). Asian Pac J Cancer Prev 2007;8 Suppl:97–104.www.ncbi.nlm.nih.gov/pubmed/18260708.
Katuwal S, Martinsen JI, Kjaerheim K, et al. Occupational variation in the risk of female breast cancer in the Nordic countries. Cancer Causes Control. 2018;29:1027–38. https://doi.org/10.1007/s10552-018-1076-2.
Wu Y, Zhang D, Kang S. Physical activity and risk of breast cancer: a meta-analysis of prospective studies. Breast Cancer Res Treat. 2013;137:869–82. https://doi.org/10.1007/s10549-012-2396-7.
Pronk A, Ji BT, Shu XO, et al. Physical activity and breast cancer risk in Chinese women. Br J Cancer. 2011;105:1443–50. https://doi.org/10.1038/bjc.2011.370.
Kruk J. Lifetime occupational physical activity and the risk of breast cancer: a case-control study. Cancer Detect Prev. 2007;31:18–28. https://doi.org/10.1016/j.cdp.2006.12.003.
Ekenga CC, Parks CG, Sandler DP. A prospective study of occupational physical activity and breast cancer risk. Cancer Causes Control. 2016;118:6072–8. https://doi.org/10.1002/cncr.27633.Percutaneous.
Johnsson A, Broberg P, Johnsson A, et al. Occupational sedentariness and breast cancer risk. Acta Oncol (Madr). 2017;56:75–80. https://doi.org/10.1080/0284186X.2016.1262547.
Boyle T, Fritschi L, Kobayashi LC, et al. Sedentary work and the risk of breast cancer in pre - and post - menopausal women: a pooled analysis of two case-control studies. Occup Environ Med. 2016;73:1–25 https://api.research-repository.uwa.edu.au/files/20411529/Boyle_et_al_2016_Sedentary_work_and_the_risk_of_breast_cancer_in_pre_and_post_menopausal_women.pdf.
Tamakoshi A, Ozasa K, Fujino Y, et al. Cohort profile of the Japan collaborative cohort study at final follow-up. J Epidemiol. 2013;23:227–32. https://doi.org/10.2188/jea.je20120161.
Ministry of Internal Affairs and Communications Statistics Bureau Japan. 業種 (産業) 分類コード表 (Industry classification code) in Japanese. Minist. Intern. Aff. Commun. Stat. Bur. (Japan Stand. Ind. Classif. Revis. Oct. 2013). 2013;25. https://www.shidaikyo.or.jp/apuji/book/pdf/syusyoku2017_002.pdf. Accessed 10 June 2019.
Mori M, Sakauchi F, Washio M, et al. Survey for incidence of cancer as a measure of outcome in the JACC study. J Epidemiol. 2005;15 https://www.jstage.jst.go.jp/article/jea/15/Supplement_I/15_Supplement_I_S80/_pdf.
Suzuki S, Kojima M, Tokudome S, et al. Effect of physical activity on breast cancer risk: findings of the Japan collaborative cohort study. Cancer Epidemiol Biomark Prev. 2008;17:3396–401. https://doi.org/10.1158/1055-9965.EPI-08-0497.
Cao J, Eshak ES, Liu K, et al. Sleep duration and risk of breast cancer: the JACC study. Breast Cancer Res Treat. 2018;174:219–25. https://doi.org/10.1007/s10549-018-4995-4.
Fujino Y, Mori M, Tamakoshi A, et al. A prospective study of educational background and breast cancer among Japanese women. Cancer Causes Control. 2008;19:931–7. https://doi.org/10.1007/s10552-008-9154-5.
Cao J, Eshak ES, Liu K, et al. Television viewing time and breast cancer incidence for Japanese premenopausal and postmenopausal women: the JACC study. Cancer Res Treat. 2019;51:509–1517. https://doi.org/10.4143/crt.2018.705.
Coogan PF, Clapp RW, Newcomb PA, et al. Variation in female breast cancer risk by occupation. Am J Ind Med. 1996;30:430–7. https://doi.org/10.1002/(SICI)1097-0274(199610)30:4<430::AID-AJIM8>3.0.CO;2-Z.
Sritharan J, MacLeod JS, Dakouo M, et al. Breast cancer risk by occupation and industry in women and men: results from the occupational disease surveillance system (ODSS). Am J Ind Med. 2019;62:205–11. https://doi.org/10.1002/ajim.22942.
Liu Y, Zhang J, Huang R, et al. Influence of occupation and education level on breast cancer stage at diagnosis, and treatment options in China: A nationwide, multicenter 10-year epidemiological study. Medicine (Baltimore). 2017;96:e6641. https://doi.org/10.1097/MD.0000000000006641.
Petralia SA, Chow WH, McLaughlin J, et al. Occupational risk factors for breast cancer among women in Shanghai. Am J Ind Med. 1998;34:477–83. https://doi.org/10.1002/(SICI)1097-0274(199811)34:5<477::AID-AJIM8>3.0.CO;2-N.
Ji BT, Blair A, Shu XO, et al. Occupation and breast cancer risk among Shanghai women in a population-based cohort study. Am J Ind Med. 2008;51:100–10. https://doi.org/10.1002/ajim.20507.
Gammon MD, John EM, Britton JA. Recreational and occupational physical activities and risk of breast Cancer. J Natl Cancer Inst. 1998;90:100–17.
Moradi T, Adami H, Bergstro R, et al. Occupational physical activity and risk for breast cancer in a nationwide cohort study in Sweden. Cancer Causes Control. 1999;10:423–30.
Kruk J, Aboul-Enein HY. Occupational physical activity and the risk of breast cancer. Cancer Detect Prev. 2003;27:187–92. https://doi.org/10.1016/S0361-090X(03)00032-1.
Dorn J, Vena J, Brasure J, et al. Lifetime physical activity and breast cancer risk in pre- and postmenopausal women. Med Sci Sports Exerc. 2003;35:278–85. https://doi.org/10.1249/01.MSS.0000048835.59454.8D.
Mathew A, Gajalakshmi V, Rajan B, et al. Physical activity levels among urban and rural women in South India and the risk of breast cancer: a case-control study. Eur J Cancer Prev. 2009;18:368–76. https://doi.org/10.1097/CEJ.0b013e32832e1c46.
Matthews CE, Shu XO, Jin F, et al. Lifetime physical activity and breast cancer risk in the Shanghai breast cancer study. Britihs J Cancer. 2001;84:994–1001. https://doi.org/10.1054/bjoc.2001.1671 on http://www.bjcancer.com L.
Zhou Y, Zhao H, Peng C. Association of sedentary behavior with the risk of breast cancer in women: update meta-analysis of observational studies. Ann Epidemiol. 2015;25:687–97. https://doi.org/10.1016/j.annepidem.2015.05.007.
Moradi T, Adami HO, Ekbom A, et al. Physical activity and risk for breast cancer a prospective cohort study among Swedish twins. Int J Cancer. 2002;100:76–81. https://doi.org/10.1002/ijc.10447.
Lahmann PH, Friedenreich C, Schuit AJ, et al. Physical activity and breast cancer risk: the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomark Prev. 2007;16:36–42. https://doi.org/10.1158/1055-9965.EPI-06-0582.
Coughlin SS. Social determinants of breast cancer risk, stage, and survival. Breast Cancer Res Treat Published Online First: 2019. doi:https://doi.org/10.1007/s10549-019-05340-7.
Tsunematsu M, Kawasaki H, Masuoka Y, et al. Factors affecting breast cancer screening. Asian Pacific J Cancer Prev J Cancer Prev. 2013;14:6041–8. https://doi.org/10.7314/APJCP.2013.14.10.6041.
Catalano RA, Satariano WA. Unemployment and the likelihood of detecting early-stage breast cancer. Am J Public Health. 1998;88:586–9. https://doi.org/10.2105/AJPH.88.4.586.
Friedenreich CM, Orenstein MR. Physical Activity and Cancer Prevention: Etiologic Evidence and Biological Mechanisms. J Nutr. 2002;132:3456S–64S. https://doi.org/10.1093/jn/132.11.3456s.
Adams SA, Matthews CE, Hebert JR, et al. Association of physical activity with hormone receptor status: the Shanghai breast cancer study. Cancer Epidemiol Biomark Prev. 2006;15:1170–8. https://doi.org/10.1158/1055-9965.EPI-05-0993.
Carpenter CL, Ross RK, Paganini-Hill A, et al. Lifetime exercise activity and breast cancer risk among post-menopausal women. Br J Cancer. 1999;80:1852–8. https://doi.org/10.1038/sj.bjc.6690610.
McTiernan A. Behavioral risk factors in breast cancer: can risk be modified? Oncologist. 2003;8:326–34 http://www.ncbi.nlm.nih.gov/pubmed/12897329.
Verloop J, Rookus MA, Van Der Kooy K, et al. Physical Activity and Breast Cancer Risk in Women Aged 20–54 Years. J Natl Cancer Inst. 2000;92:128–35.
Acknowledgements
The authors thank you very much for all staff members who implicated in action in JACC study in organize the baseline survey and follow-up.
Funding
This research was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan (MEXT) (Monbusho); Grants-in-Aid for Scientific Research on Priority Areas of Cancer; and Grants-in-Aid for Scientific Research on Priority Areas of Cancer Epidemiology from MEXT (MonbuKagaku-sho) (Nos. 61010076, 62010074, 63010074, 1010068, 2151065, 3151064, 4151063, 5151069, 6279102, 11181101, 17015022, 18014011, 20014026, 20390156, and 26293138), Comprehensive Research on Cardiovascular and Life-Style Related Diseases (H26-Junkankitou [Seisaku]-Ippan-001and H29–Junkankitou [Seishuu]–Ippan–003), JSPS KAKENHI Grant Number JP 16H06277, and Grants-in-Aid for China Scholarship Council (CSC file No. 201608050113). The study sponsor has no involvement in the study design, data collection, analysis and interpretation of data.
Author information
Authors and Affiliations
Contributions
GNS, ESE and KS designed the study. GNS, ESE, KS and YF developed methods to measure occupation and occupational activity. AT and HI coordinated the research. GNS analysed the data. GNS, ESE and HI drafted the manuscript. All authors read and approved the final manuscript
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained and written individually by each participants that they will be participated to the JACC study in the baseline questionnaire. The ethics committees of Nagoya University School of Medicine and Osaka University approved the protocol of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Supplementary Table
. Age-adjusted and multivariable hazard ratios (95% confidence intervals) of incident breast cancer according to job category and occupational activity after exclusion of housewives in occupation
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sari, G., Eshak, E.S., Shirai, K. et al. Association of job category and occupational activity with breast cancer incidence in Japanese female workers: the JACC study. BMC Public Health 20, 1106 (2020). https://doi.org/10.1186/s12889-020-09134-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-09134-1