
Abstract
Background
Occupational stressors in police work increase the risk for officer mental health morbidities. Officers’ poor mental wellbeing is harmful to the individual, can affect professionalism, organisational effectiveness, and public safety. While the impact of operational stressors on officers’ mental wellbeing is well documented, no review has systematically investigated organisational stressor impacts. This study aimed to conduct a systematic review to assess the relationship between organisational stressors and police officer mental wellbeing.
Methods
Systematic review conducted following PRISMA and Cochrane Collaboration guidelines. Literature search was undertaken from 1990 to May 2017 on four databases (EBSCOHOST Medline/SocINDEX/PsycINFO/OVID Embase) and grey literature. Included articles were critically appraised and assessed for risk of bias. Narrative and evidence syntheses were performed by specific mental health outcomes.
Results
In total, 3571 results were returned, and 15 studies met the inclusion criteria. All included studies were published in English between 1995 and 2016, had cross-sectional study designs, spanned across four continents and covered 15,150 officers. Strong evidence of significant associations was identified for organisational stressors and the outcomes of: occupational stress, psychiatric symptoms/psychological distress, emotional exhaustion and personal accomplishment. The organisational stressors most often demonstrating consistently significant associations with mental health outcomes included lack of support, demand, job pressure, administrative/organisational pressure and long working-hours.
Conclusions
This review is the first to systematically examine organisational stressors and mental health in police officers. Organisational stressors that can be targeted by interventions and policy changes to secure officer wellbeing, a healthy work environment, and benefits to the organisation and the public are identified.
Similar content being viewed by others


Background
Mental wellbeing (MW) in police officers
Mental health (MH) disorders are a leading cause of long-term work incapacity and sickness absence [1]. The rise in MH problems over the past decade in the working population has spurred increased public, policy and academic interest [2,3,4], leading to a focus of research on the role of work environments and lifestyle behaviours on mental wellbeing (MW) across occupational groups [5,6,7].
The police work environment has many occupational stressors and exposures that can lead to increased risk for mental health morbidities [8]. Policing is one of the most stressful occupations as maintained by academic researchers, police practitioners, health-care professionals and psychologists [9,10,11,12] and it ranks in the top three occupations in the Occupational Disease Intelligence Network (ODIN) system for Surveillance of Occupational Stress and Mental Illness (SOSMI) [13]. Police officers experience the same combination of MH issues as the general working population [14, 15]; however, their work is compounded by frequent exposure to inherently dangerous situations, which require a different level of physical and mental ability to respond effectively [16,17,18]. While this can predispose police officers to stress, some research suggests that individual coping mechanisms can become embedded in police officers personalities, allowing them to cope and accept stressful situations as natural requirements of their role [19, 20] and be more resilient to stress than civilians [5]. Fitness for work is central to professional police standards [21, 22]. Therefore, determining which occupational stressors are related to specific MW outcomes may improve police officer wellbeing and contribute to organisational effectiveness [22].
Occupational stressors in police work
Intrinsic to police work is the daily experience of intensely stressful situations in often higher frequencies than most other occupations [23, 24]. Constant exposure to people suffering distress and pain, threats to officer safety and wellbeing, having to be in control of emotions when provoked, the inconclusive nature of police work, the responsibility of being in possession of a firearm and more importantly the responsibility of protecting the lives of citizens have been recognised as significant sources of stress [25]. These daily activities are constantly under scrutiny due to the societal and political expectations put on human-service professions [26]. As human-service jobs entail a great deal of interaction with the public, police officers are often expected to display and/or manage particular feelings as part of their job, considered a form of ‘emotional labour’ [27, 28].
Territo and Vetter [29] suggested the stressors affecting police officers could be grouped into four categories (organisational practices and characteristics, criminal justice system practices and characteristics, public practices and characteristics and police work itself). These four categories can be further classified into operational and organisational stressors [30, 31]; the former associated with the very nature of police work, including job-related violence [32], exposure to danger and facing the unknown [32], court overtime [33, 34], and the latter related to organisational administration, management, structure and processes [32].
Organisational stressors have been suggested to be a greater source of stress for police officers [35, 36] because officers may recognise them as oppressive [37], unnecessary [37], unavoidable [37] and uncontrollable [38, 39]. Organisational stressors suggested to contribute to the manifestation of stress include lack of support, heavy work load [32], interpersonal conflict with colleagues and supervisors [40], inadequate resources, time pressure, and an overly bureaucratic organisational system, punitive of staff and strictly managed [40, 41]. These findings seem to hold over cross-cultural comparisons cross the UK [30, 42, 43], USA [44, 45], South Africa [46, 47] and other foreign police agencies [44, 45]. Within the existing evidence base the MW outcomes commonly demonstrating or suggested to be associated with organisational stressors in police officers are occupational stress [48, 49], anxiety [50], depression [50, 51], psychiatric symptoms (PS)/psychological distress (PD) [51, 52], burnout [51, 53] and suicidal ideation [54].
Rationale
Understanding the risk factors to mental wellbeing in the police workforce is paramount [11, 42, 55], as police play a vital role in the maintenance of society. A previous systematic review [56], assessed coping behaviours adopted by police but did not focus on associations between occupational stressors and MW. The aim of our review, is to examine the associations of organisational stressors in police work with the mental wellbeing outcomes of: occupational stress, anxiety, depression, psychological distress (PD), psychiatric symptoms (PS), burnout (a composite measure of depersonalisation (DP), personal accomplishment (PA) and emotional exhaustion (EE)), and suicidal ideation.
Methods
Aim
Systematically review the literature to assess the relationship between organisational stressors and police officer mental wellbeing.
Review methodology
The review was carried out systematically following the Cochrane Handbook for Systematic Reviews [57] and PRISMA Statement [58] guidance; the narrative synthesis followed the Economic and Social Research Council (ESRC) guidelines [59, 60].
Eligibility criteria
Inclusion criteria were set priori and were based on the Population, Intervention, Comparison and Outcome (PICO) framework [59, 61] (Additional file 2: Table S2). A scoping search was conducted in EMBASE to pre-test the suitability and adequacy of the PICO criteria. Inclusion criteria included: police personnel from various ranks of any age or gender, including trainees and recruits; studies that considered other occupational groups as well as the police were suitable if a separate analysis of the relationship between organisational stressors and police MW could be extracted (study population); studies identifying one or more organisational stressors in relation to police MW (exposure); MH outcomes measured by general measures of wellbeing such as self-reported perceptions of health status, subjective MH, studies considering physiological, organisational or personal outcomes as well as MW outcomes, were suitable if a separate analysis of the relationship between organisational stressors and police MW outcomes could be extracted (outcomes); all study designs were included.
Studies were excluded if they involved correctional, prison, probation officers, police veterans, military, army and navy personnel, police forensic personnel, civilian (non-sworn police) and traffic police; stressors not inherent in police work; physiological/biological indicators of MH and organisational and personal outcomes (i.e. job satisfaction, job commitment); poster articles and information pieces; and studies that only assessed the prevalence of organisational stressors or MW outcomes.
Databases and information sources
A comprehensive literature search was conducted from the period of 10th May to 16th May 2017. The electronic medical and social science databases consulted were Medline, PsycINFO, SocINDEX and Embase. In addition, grey literature sources were searched using the same criteria [62]. Prior to checking grey literature sources, a literature search on police accountability and governance was conducted to ensure all professional bodies and regulators relevant to the police force were considered. The final grey literature sources consulted are reported in Additional file 2: Table S3. Additionally, experts in the field of police stress literature were contacted (Personal Communication 1, See Additional file 1: Table S1).
Search strategy
An initial scoping search with no restrictions or limitations was conducted using a combination of free-text search terms [63]. Returned search results were reviewed to identify potentially relevant subject headings, free-text terms and phrases. The final search strategies were constructed from combinations of MeSH and keywords/free-text terms, adjusted for each database. Search results were limited to studies published in English with no geographic restrictions (potential concerns due to cultural differences were noted [64]). Studies published between 1990 to search date (16th May 2017) were considered. The detailed search strategies are presented in Additional file 2: Tables S4, S5, S6 and S7.
Study selection
The PICO inclusion criteria were incorporated into an electronic screening tool [65], to standardise the selection process (Additional file 3: Table S8); and piloted on 30 studies [59, 66]. All titles and abstracts were then screened for eligibility using the PICO criteria [67]. Full-texts were screened by one reviewer (AP) and analogous to abstract and title screening, 10% of full-text studies were screened independently by a second reviewer (ED). Hand searching was conducted on the reference lists (AP). Grey literature sources and Google scholar results were also screened (AP) using the electronic screening tool on abstracts and titles. Sources, which could inform the review, but did not satisfy the inclusion criteria were noted. A data extraction form was developed to facilitate and standardise data extraction [59, 68, 69]; this was piloted on 10 included studies [57]. Study authors were contacted if further information or clarification was required (Personal Communication 2, See Additional file 1: Table S1).
Risk of Bias assessment
Eligible studies were assessed for risk of bias [57, 58], using a previously modified version of the Newcastle-Ottawa Scale (NOS) [70, 71]. Studies scored as high (7–10 stars), intermediate (5–7 stars) or low quality (1–4 stars) [72,73,74,75]. The modified NOS, was piloted on five studies prior to use [65]. A single reviewer (AP) assessed and ranked each study based on total score and the results were then discussed with the second reviewer (ED). Data extraction occurred prior to risk of bias assessment, to protect against reporting bias [65].
Narrative & Evidence Synthesis
The results were narratively synthesised, and findings presented by MW outcome of interest. Evidence synthesis was a stepwise process analysed by MW outcome and was based on study design, methodological quality, consistency with regards to the presence or absence of associations between organisational stressors and specific MW outcomes and the magnitude of these associations [76,77,78].
The reporting of the organisational stressors was mapped onto the WHO Organisational Stress-related Hazard Categorisation [79]. Six of the nine categories were represented in the findings: organisational culture; workload and work pace; working hours; interpersonal relationships; participation and control, and career development, status and pay. For the purposes of this review, workload, work pace and working hours were combined into one category. The evidence synthesis process involved combining the degree of evidence with the magnitude of respective association.
A rating system was used to assess the degree of evidence wherein the modified NOS risk of bias grade of each included study was combined with a second assessment which graded the degree of adjustment by confounders conducted within each included study. The rating system was adapted from previous systematic reviews [71, 76,77,78] and the underlying developmental process was in accordance with expert recommendations (Personal Communication 3, See Additional file 1: Table S1). Evidence was graded as Strong: if consistent findings were reported in more than two studies of high quality (at least one study adjusted for participant demographics and additional exposure variables); Moderate: if consistent findings were reported in two studies of high quality or one high quality study and one intermediate quality study, or between more than two studies of intermediate quality (at least one study has adjusted for participant demographics or additional exposure variables); and Insufficient: if identification of only one study or inconsistent findings across studies.
To assess the magnitude of associations the process included: Step 1-the organisational stressors reported were coded/re-coded under the WHO categories [79] to standardise the reporting of the same/similar organisational stressors presented with different terminology. Step 2 addressed the heterogeneity in the reported measures of effect, including correlation and unstandardized/standardised-beta coefficients, and odds ratios, by developing and applying threshold values previously reported in the literature [71, 76,77,78] for each effect measure. The final threshold value criteria (see Table 1), were discussed with colleagues having expertise in evidence synthesis (Personal Communication 3, See Additional file 1: Table S1), Using these threshold values (see Table 1), the effect size of each organisational stressor and MW outcome relationship was graded and scored (a weight to indicate each grade’s relative importance) as High (+++/3 points), Intermediate (++/2 points), Low association (+/1 point), No association (−/0 point) and unclear (±/0 point). In Step 3, a weighted average was estimated to account for the levels of relative importance across the five grades by: (i) multiplying the number of effect sizes per grade by the number of points (weight) allocated to that grade; (ii) adding the results across all grades for each MH outcome; and (iii) dividing the total by the sum of the weights (number of grades applied per MW outcome). This weighted average resulted in the mean magnitude of association of included studies by MW outcome. Finally, in Step 4 a RAG (Red, Amber and Green) threshold scale was applied to the overall magnitude of association, where a score of 0 to 1.9 was deemed ‘low/no association’ (Red), 2 to 3.9 was ‘intermediate association’ (yellow), and ≥ 4 was ‘high association’ (green). See Supplementary Material S12 for further detailed process.
Results
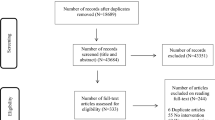
The study selection process is documented in Fig. 1. No concerns were raised following second reviewer input in screening titles, abstracts or full-text studies. In total, 15 studies [82,83,84,85,86,87,88,89,90,91,92,93,94,95,96] met the inclusion criteria and 134 full text studies were excluded (see Fig. 1 and Additional file 4: Table S9).

Study selection PRISMA Flow Diagram [58]
Study characteristics
The characteristics of the 15 included studies are summarised in Table 2. All studies were published in English, between 1995 and 2016. No RCTs or cohort studies met the inclusion criteria; all included studies had a cross-sectional study design. The majority were undertaken in the developed world; five from North America [82, 88, 90, 92, 93], five from Europe [84,85,86, 89, 91], three from Asia [87, 95] and two from Africa [83, 94]. Included studies covered a total of 15,150 male and female police officers, with the smallest study [90] having 78 participants and the largest [86] 3272 participants. Three studies failed to report final response rates [90, 94, 95], the remaining 12 studies included response rates ranging from 33.9% [82] to 96% [96]. The studies which provided information on gender [82,83,84,85,86,87, 89,90,91,92,93,94, 96] covered 9706 male and 2592 female study participants; for those that provided mean age, the mean age of participants ranged from 33 to 40 years [82,83,84,85,86,87, 90, 91, 94]. Two studies [93, 96] adopted an ordinal scale for age; one study [89] dichotomised age; and three studies failed to provide any information on the participant age [88, 92, 95]. Police work tenure ranged from 2.9–17.2 years [82,83,84,85, 89, 91, 92, 94, 96]. Only three studies provided information on rank, which included police constables, corporals, sergeants, inspectors, captains, superintendents and senior superintendents [83, 89, 94]. Several studies reported educational background [83, 84, 87, 88, 90,91,92, 94, 96], marital status [84,85,86, 90, 91, 94, 96] and race or ethnicity [88, 92,93,94]. Only one study failed to report participant demographics [95].
Outcomes reported across studies
The included studies reported a number of outcomes of interest including occupational stress [88, 93, 96], anxiety [86], depression [86, 87], PD [82, 89, 90], PS [84], burnout [95] (a composite measure of EE [82, 83, 85, 86, 89, 91, 92, 94, 95], DP [85, 86, 89, 91, 94, 95], PA [86, 89, 91, 95]) and suicidal ideation [86].
Risk of Bias
All studies were cross-sectional, therefore the modified NOS [70] was used to assess risk of bias. Overall 13 studies were ranked as high [82,83,84,85,86,87,88,89,90,91, 93, 94, 96], one as intermediate [92] and one as low quality [95] (Additional file 5: Tables S10, S11). The cross-sectional design of the included studies precludes causal inference [97] and the direction of association cannot be established.
Response rates varied, and all studies employed self-reporting questionnaires. Questionnaires are considered appropriate, as they can provide information about health status, attitudes and behaviours of police officers [98], especially those experiencing MW issues [89]. However, self-reporting questionnaires can lead to method variance bias [99], resulting in overestimation of associations [100] and raise issues of recall bias [101]. Online questionnaires were adopted by three studies [82, 89, 92]. Online surveys often have good data quality and generally confer lower measurement errors, however low response rates are often a challenge [102]. This is demonstrated in these cases, which reported response rates of 33.85 to 57% [82, 89, 92].
Since all studies failed to provide information on the demographics of both respondents and non-respondents, non-response bias cannot be assessed. Response bias may be a problem for topics concerning mental wellbeing, particularly in masculine environments such as policing. One study [88] employed Dillman’s Total Design Method [103] to achieve high response rate and mitigate non-response bias [104]. Eight studies [82, 84, 86, 87, 89, 93, 94, 96] adjusted for additional exposure variables, such as operational stressors and ten studies [83,84,85,86, 89,90,91, 93, 94, 96] controlled for potential confounders, enhancing internal validity.
Eight studies failed to report the sampling method [82, 84, 86, 89, 90, 94,95,96]. The other studies, adopted probability sampling [83, 85, 88, 91,92,93] of which one study adopted random gender stratified sampling [85] and four studies used random sampling [83, 88, 91, 92]. One study failed to provide information on the type of probability sample adopted [93]. Purposeful sampling was adopted by one study [87]. None of the studies accounted for officers who were not in work (e.g. court, special assignment, annual leave, off sick) and therefore not included in the study samples. Present state bias cannot be ruled out, if officers more vulnerable to stress have left the profession, creating a more resilient population than that of the general police population [102]. All studies involved voluntary participation, as such all were prone to volunteer bias; which could affect external validity [105].
Synthesis of results by outcome
All MW outcomes identified in the initial scoping search were reported in the included studies. The results from the included studies are presented by outcome of interest (see also Supplementary material S12–13) [57, 58]. Table 3 shows the organisational stressor and MW outcome associations of included studies by outcome, the assigned effect size grades and corresponding significance levels.
Occupational stress
Three high quality studies [88, 93, 96] assessed occupational stress, covering a total of 3060 participants, almost half of which (47%; n = 1427) were from one study [88].
Most organisational stressors had low or no association with occupational stress (Table 3). Only ‘ridicule and set-ups’ had an intermediated effect size grade in one study [96], and this was the strongest association observed [88, 93, 96] (Table 3). In this study on South Korean police officers [96], ‘ridicule and set-ups’ was significantly associated with occupational stress (ß = .53, p < .01) following adjustment for both participant demographics and additional exposure variables, including sexual/language harassment, feeling invisible, length of service, rank etc. In a study on US officers [93], the same association was graded as low but the relationship remained significant (ß = .12, p < .01) following adjustment for participant demographics and other exposure variables, including lack of advancement opportunity or influence, bias, etc.
Dealing with ‘bias’ from co-workers was predictive of occupational stress in US police officers when adjusting for participant demographics and additional exposure variables (ß = .29, p < .01) [93]. Officers who exhibited high levels of occupational stress reported stress as a consequence of ethnic or racial bias [93]. Moreover, officers reported considerable time and energy was spent helping co-workers deal with this prejudice and bias, consequently elevating their levels of occupational stress [93]. High levels of ‘superior support’ resulted in low levels of occupational stress in the study conducted on South Korean police officers [96] (ß = -.26, p < .01), after adjustment for participant demographics and exposure variables including public disrespect and expressed feelings. However, no evidence of a significant association between high levels of ‘work group support’ and occupational stress was observed (ß = .04, p = ns) in US police officers [93]. Τhe organisational stressor poor ‘personnel relations’ (b = .055, p = ns) was not significantly associated with occupational stress in a study of police executives either, although should be noted that this study did not account for possible confounding variables [88].
‘Department issues’ (e.g. the department budget, personnel retention and employee labour organisations) was significantly associated (‘low’ effect size grade) with occupational stress (b = .197, p < .05) [88]. A ‘lack of influence’ over the way policing is conducted, procedures and policies, was significantly associated with occupational stress (ß = .18, p < .01), however ‘lack of advancement opportunity’, (ß = .03, p = ns) was not, following adjustment for participant demographics and additional exposure variables [93] .
The organisational stressor ‘language harassment’ was significantly associated with occupational stress in US police officers (ß = .10, p < .01) [93], controlling for participant demographics and exposure variables including stigma and appearance and feeling invisible. In the same study, ‘sexual harassment’ was significantly negatively associated with occupational stress (ß = −.08, p < .05) [93]. Yet, in the study [96] conducted on South Korean police officers no significant association between occupational stress and either ‘language harassment’ (ß = .07, p = ns) or ‘sexual harassment’ (ß = .01, p = ns) was reported.
Anxiety
One high quality study, covering 3272 participants, assessed anxiety, and demonstrated that ‘job pressure’ was a significant predictor of anxiety symptoms (OR 2.0, 95%; 95%CI:1.5–2.7; p < .001) after adjustment for demographics and other exposure variables such as lack of support, subjective health complaints, etc., whereas ‘lack of support’ (OR 1.2; 95%CI: 0.9–1.7; p = ns) was not [86].
Depression
Two high quality studies [86, 87] covering 4104 participants, with 80% (n = 3272) originating from one study [86], assessed depression. Significant associations, graded as intermediate (Table 3), were reported between ‘heavy workload’ (OR 1.73; 95%CI:1.19–2.50; p = .004) and ‘judgement from peers’ and depression (OR 2.35; 95%CI:1.31–4.23; p = .004) after controlling for exposure variables, such as judgement from peers, little time to spend with families, job performance, etc. [87]. There was no evidence of a significant association between ‘job pressure’ (OR 1.0, 95%CI:0.7–1.4; p = ns) or ‘lack of support’ (OR 1.3, 95%CI:0.9–1.99; p = ns) and depression in the adjusted models [86].
Psychological distress (PD) and psychiatric symptoms (PS)
Four high quality studies assessed psychological distress (PD) and psychiatric symptoms (PS) [82, 84, 89, 90]. These covered 1854 police officers, of which 66% (n = 1226) were from one study [89].
The strongest predictor of PS, high effect size grade, was ‘lack of support from superiors and organisation’ (OR 3.58, 95%CI:1.58–8.13; β = 1.28; p = .002), after controlling for additional exposure variables such as inadequate work schedule, high mental/intellectual demand, etc. [84]. Intermediate but significant predictors of PS were ‘inadequate work schedule’ (OR 2.84, 95% CI:1.22–6.62; β = 1.04, p = .016) and ‘high mental/intellectual demand’ (OR 2.56, 95%CI:1.12–5.86; β = .94, p = .026) in adjusted models [84].
For PD, ‘long working hours’ (≥ 49 h/week) demonstrated a high and significant association (OR 2.05, 95%CI:1.57–2.68; p < .05), after controlling for age, gender, rank, departmental tenure and years of service [89]; while ‘insider social stressors’- defined as stress arising from co-workers and supervisors- displayed an intermediate but significant association (β = .45, p < .01) when controlling for outsider social stressors (e.g. stressor from interactions with civilians/suspects) [82]. The odds of PD caseness in participants working ‘long working hours’, was double that of officers working ‘normal working hours’ (≤48 h/week) following full adjustment [89]. ‘Effort-reward imbalance’ (β = .24, p < .05) and ‘over-commitment’ (β = .40, p < .01) were low but significant predictors of PD, after adjusting for age, gender, marital status and education [90].
Burnout (defined as a composite measure of EE, DP and PA)
Only one low quality study, assessed burnout as a composite measure of emotional exhaustion (EE), depersonalisation (DP) and personal accomplishment (PA) [95]; but nine studies assessed associations of organisational stressors and EE [82, 83, 85, 86, 89, 91, 92, 94, 95]. Of the latter, six studies further assessed DP [85, 86, 89, 91, 94, 95] and four of these studies additionally assessed PA [86, 89, 91, 95]. Seven of the studies investigating EE, DP and/or PA were of high quality [82, 83, 85, 86, 89, 91, 94], one of medium quality [92], and one of low quality [95]. The studies covered 10,853 participants, 30% of which (n = 3272) were from one study [86].
Burnout (composite measure of EE, DP and PA)
‘Police stress’ measured by the Police Stress Survey (r = .301, p < .01) and ‘administrative organisational pressure’ (r = .347, p < .01) were significantly correlated and had low associations with burnout, however the authors did not adjust for participant demographics or additional exposure variables [95].
Emotional exhaustion (EE)
Four of the nine studies- three of high [85, 86, 94] and one of low [95] quality- investigating EE demonstrated that the strongest predictor of EE was the ‘demand’ inherent in police work. A significant relationship between high ‘demand’ and EE in both male (OR 5.97; 95%CI:3.32–10.71; p < .05) and female police officers (OR 7.69; 95%CI:4.21–14.03; p < .05) was reported after adjusting for age [85]. Job ‘demands’ (β = .22, p < .001) and ‘lack of resources’ (β = .20, p < .001) both exhibited low but significant relationships with EE, after controlling for both participant demographics and other exposure variables, including conscientiousness, emotional stability, etc. [94]. Intermediate and significant associations were reported for ‘job pressure’ and EE (OR 2.1; 95%CI:1.8–2.5; p < .001) [86]. The odds of high EE in police officers working long hours (> 49 h/ week) were double that of officers working normal hours (< 48 h/ week) (OR 1.99, 95%CI:1.52–2.59; p < .05) [89]. However, another study found no significant association in adjusted models between ‘overtime work’ and EE (β = .07, p = ns) [91].
Similar to burnout, ‘police stress’ (r = .256, p < .01) and ‘administrative/organisational pressure’ (r = .310, p < .01) were significantly correlated with EE [95]. Low ‘decision latitude’ demonstrated intermediate and significant associations with EE in both female (OR 2.44; 95%CI:1.38–4.30; p < .05) and male police officers (OR 3.94; 95%CI:2.02–7.70; p < .05), following adjustment for age [85]. Yet, lack of ‘autonomy’ was not a significant predictor of EE (β = −.10, p = ns) [91].
Several social stressors exhibit intermediate and low associations with EE [82, 85, 86, 91, 92]. Social support from colleagues and superiors is generally associated with lower levels of EE [85, 86, 91, 92], concluded that ‘lack of support’ was significantly associated with EE (OR 1.8; 95%CI:1.5–2.2; p < .001). Martinussen et al. [91] (β = −.25, p < .05) and McCarty et al. [92] (b = −.44, p < .05) demonstrated that as levels of social support increased levels of EE decreased; while ‘social support’ was significantly associated with EE in both male (OR 3.47; 95%CI:2.02–5.96; p < .05) and female police (OR 2.79; 95%CI:1.73–4.51; p < .05), after controlling for age [85]. ‘Internal social stressors’ were significantly associated with EE (β = .44, p < .01) when controlling for ‘outsider social stressors’ [82]. Work conflict (β = .01, p = ns) [91] was not found to be a significant predictor of EE. In the same study, ‘leadership’ was not identified as a significant predictor of EE (β = −.11, p = ns) [85, 91]. Similarly, Backteman-Erlanson et al. [85] did not identify a significant association between ‘leadership’ and EE in both male (OR 0.72, 95% CI:0.53–0.99, p = ns) and female police officers (OR 0.56, 95% CI:.42–.75, p = ns).
In terms of workplace climate and culture, ‘organisational climate’ and ‘organisational culture’ showed intermediate and significant associations with EE in both female (climate: OR 2.48, 95%CI:1.79–3.45; p < .05 & culture: OR 2.28, 95%CI:1.61–3.21; p < .05)) and male police (climate: OR 2.17, 95%CI:1.56–3.01; p < .05 and culture: OR 2.09, 95%CI:1.44–3.04; p < .05) following adjustment for age [85]. Two studies, further examined a component of organisational culture by investigating ‘overall perceived fairness’ of police organisations [83, 92]. The first study, reported that 10% of the total variance in EE experienced by participants was attributed to ‘perceived workplace fairness’; and that as ‘perceived workplace fairness’ increased levels of EE decreased (β = −.23, p < .01) [83]. Similarly, the second study demonstrated that ‘unfairness of the organisation’ was significantly associated with EE (b = .31, p < .05) [92].
Depersonalisation (DP)
The organisational stressor demonstrated to be the strongest predictor of DP was low ‘decision latitude’ and this association was identified in both male (OR 2.68; 95%CI:1.37–5.24; p < .05) and female (OR 1.77, 95%CI:1.05–2.99; p < .05) police officers, following adjustment for age [85]. On the contrary, another study did not find any evidence of a significant association between lack of ‘autonomy’ and DP (β = −.04, p = ns) after adjustment for confounding [91].
Four studies investigated the impact of high job demand and pressure on DP [85, 86, 94, 95] and three found intermediate [85] and low [94, 95], but significant associations. High job ‘demand’ was significantly associated with DP (β = .11, p < .001) after controlling for confounding [94], and similarly was a significant predictor of DP in both male (OR 1.96, 95%CI:1.20–3.20; p < .05) and female police officers (OR 2.54, 95%CI:1.57–4.13; p < .05) after adjusting for age [85]. ‘Administrative/organisational pressure’ (r = .218, p < .01) and ‘police stress’ (r = .165, p < .01) were significantly associated with DP [95]. Conversely, one study found no evidence of an association between ‘job pressure’ and DP (OR 0.9, 95%CI:0.8–1.1; p = ns) in the adjusted model [86]. Analogous to EE, ‘long working hours’ (OR 1.30; 95%CI:1.00–1.71; p < .05) [89] and ‘lack of resources’ (β = .17, p < .001) [94] were significantly associated with DP, while ‘overtime work’ (β = .06, p = ns) was not [91] .
Three studies investigated organisational stressors related to interpersonal relationships at work [85, 86, 91]. Similar to EE, high levels of ‘social support’ from co-workers and supervisors resulted in decreased levels of DP (β = −.33, p < .001) [91], while the lack of ‘social support’ significantly predicts DP in both male (OR 2.18; 95%CI:1.28–3.71; p < .05) and female (OR 1.62, 95%CI:1.06–2.48; p < .05) police officers following adjustment for age [85]. However, one study found no significant association between ‘lack of support’ and DP (OR 0.9, 95% CI:0.8–1.1; p = ns) [86] . Similar to EE, there was no significant association between ‘work conflict’ and DP (β = .07, p = ns) [91].
Assessing stressors related to organisational culture demonstrated that adoption of appropriate ‘leadership’ significantly decreased DP levels (β = −.24, p < .01) [91], but another study found no association between appropriate ‘leadership’ and DP in both male (OR 0.85; 95%CI:0.62–1.15; p = ns) and female police officers (OR 0.94, 95%CI:0.73–1.22; p = ns) [85]. Poor ‘organisational culture’ was identified as a significant risk factor for DP in both male (OR 1.59, 95%CI:1.12–2.25; p < .05) and female police officers (OR 1.49, 95%CI:1.11–1.99; p < .05), whereas ‘organisational climate’ was as a significant risk factor for female police officers only (OR 1.64, 95%CI: 1.22–2.19; p < .05) and not for males (OR 1.27, 95%CI:0.94–1.73; p = ns) [85].
Personal accomplishment (PA)
Of the four studies investigating PA, the organisational stressors, social support and job pressure were the strongest predictors of PA, as examined in two high quality studies [86, 91] and one low quality study [95]. ‘Job pressure’ was significantly related to PA (OR 1.3, 95% CI:1.1–1.6; p < .001), after controlling for age, gender, lack of support, anxiety, depression, subjective health complaints, suicidal ideation, EE and DP [86]. Similarly, ‘police stress’ (r = .167, p < .01) and ‘administrative/organisational pressure’ (r = .152, p < .01) were statistically significant correlated with PA, independent of adjustment for confounders [95]. Neither ‘long working hours’ (OR 0.99, 95%CI:0.75–1.32; p = ns) [89], nor ‘overtime work’ (β = .01, p = ns) [91] were significantly associated with PA.
After adjusting for leadership, work conflict, overtime work, autonomy, work-family pressures, age and gender, high levels of ‘social support’ from co-workers and supervisors (β = .23, p < .01) and PA [91] were significantly correlated. This relationship however was not significant in the study conducted by [86] (OR 1.1, 95% CI: 0.9–1.2; p = ns). No significant relationship with PA was observed for ‘leadership’ (β = .13, p = ns) [91], ‘work conflict’ (β = −.03, p = ns) [91] and ‘autonomy’ (β = .09, p = ns) [91] in adjusted models.
Suicidal ideation
One high quality study [86] assessed the association between organisational stressors and suicide ideation, covering 3272 participants. This study revealed that neither ‘job pressure’ (OR 0.8, 95%CI:0.6–1.19; p = ns) nor ‘lack of support’ (OR 1.3, 95%CI:0.9–1.7; p = ns) were significantly associated with suicidal ideation after controlling for confounders [86].
Evidence synthesis
Thirty-six organisational stressors were identified, of which twenty-five demonstrated significant associations with one or more MW outcomes (Table 3). Overall, a strong degree of evidence with a high magnitude of associations between organisational stressors and MW outcomes (Table 4 and Additional file 6: Table S12 and S13), was observed for the outcomes of PS/PD [82, 84, 89, 90], EE [82, 83, 85, 86, 89, 91, 94, 95] and DP [85, 86, 89, 91, 94, 95]. Strong evidence of intermediate magnitude was identified for studies investigating the relationship between organisational stressors and occupational stress [88, 93, 96] and PA [86, 89, 91, 95]. Studies investigating burnout [95], anxiety [86] and depression [86, 87] provided an insufficient degree of evidence, however the magnitude of associations was rated as intermediate. The degree of evidence and the magnitude of associations were insufficient and low, respectively, for suicidal ideation [86].
The thirty-six organisational stressors were mapped under the amended WHO Organisational Stress-related Hazard Categories: organisational culture; workload and working hours; working hours; interpersonal relationships; participation and control and career development. Within the organisational culture category stressors included ‘organisational climate’ and ‘organisational culture’ both of which were significant predictors of EE [85] and DP [85]. ‘Perceived workplace fairness’/‘unfairness of the organisation’ were significant risk factors for EE [83, 92] only. ‘Department issues’ was a significant risk factor for occupational stress [88], while ‘leadership’ was identified as a significant predictor for DP only [91]. ‘Job demands’ [85, 94], high mental/intellectual demand [84], pressure [86, 95] and heavy workload [87], were shown to be significant predictors of PS/PD [84], anxiety [86], burnout [95], EE [85, 86, 94, 95], DP [85, 94, 95], PA [86, 95] and depression [87].
Within the Workload and working hours category, ‘long working hours (≥ 49h/week)’ [89] demonstrated an increased risk of PS/PD [89], EE [89] and DP [89] however did not increase risk of PA [89]. A ‘lack of resources’ [94] in the organisation was recognised as increasing the risk of EE [94] and DP [94]. The Interpersonal relationships category comprised of stressors including ‘lack of support’, ‘ridicule and set ups’ and ‘bias’. ‘Lack of support’ significantly increased the risk of number of MW outcomes including occupational stress [96], PS/PD [82, 84], EE [82, 85, 91, 92], DP [85, 91], and PA [91]. ‘Ridicule and set ups’ [93, 96], ‘sexual and language harassment’ [93] and ‘bias’ [93] predicted occupational stress, whilst ‘judgement from peers’ was identified as a significant risk factor for depression [87]. There were a small number of stressors which fell under the Participation and Control category. Low ‘decision latitude’ was a significant predictor of EE and DP [85], while ‘lacking influence’ in one’s work was predictive of occupational stress [93]. ‘Autonomy’ was not identified as a significant risk factor when investigated in relation to EE, DP and PA [91].
Organisational stressors in the Career Development category, included ‘effort-reward imbalance’ [90], ‘over commitment’ [90] and ‘lack of advancement’ [93]. The former two were significant predictors for PD/PS [90], while the latter was not a significant risk factor for occupational stress.
Discussion
Summary of findings
This review systematically summarises the organisational stressors intrinsic to police work that significantly contribute to the adverse MW outcomes of occupational stress, anxiety, depression, PS/PD, Burnout, EE, DP, and suicidal ideation. The findings are based on the available evidence established through a systematic search using predefined PICO inclusion criteria set for this review. Fifteen studies met the inclusion criteria, covering relationships between 36 different organisational stressors with MW outcomes, of which twenty-five, including examples such as: organisational culture and climate, perceived workplace fairness/unfairness, leadership, department issues, job demands, high mental/intellectual demand, job pressure, heavy workload, long working hours, lack of resources and support, ridicule and set ups, sexual and language harassment, bias, judgement from peers, low decision latitude, lacking influence, effort-reward imbalance and over commitment, were identified as statistically significant predictors of MW outcomes and demonstrated a strong degree of evidence with high or intermediate magnitudes of associations with the MW outcomes studied..
Review in the context of previous studies
The majority of the evidence collated for this review has indicated the MW outcomes PS/PD [82, 84, 89, 90], EE [82, 83, 85, 86, 89, 91, 94, 95] and DP [85, 86, 89, 91, 94, 95] demonstrate the strongest relationships with organisational stressors, including lack of support from superiors and organisation, long working hours, inadequate work schedule, high mental/intellectual demand, job demand, organisational climate, organisational culture and low decision latitude. Within the wider literature ‘job demand’ is identified as an important risk factor for the manifestation of MW outcomes, analogous to our review findings. In a systematic review covering the general working population, there was strong evidence that high job demand was a significant predictor of PD [106]. A narrative review of ‘high quality’ longitudinal studies, conducted by de Lange et al., [107] found evidence of causal effects of job demands on PS, concluding that the psychosocial work environment at work is vital for mental health. While this narrative review did not consider police personnel specifically, its purpose was to test the effects of a combination of job characteristics (demand, control and support) on PS [107], all of which are inherent in police work [35].. Our review did not identify any studies investigating the impact of job demand on depression, anxiety and occupational stress, however a review on the general population, demonstrated that high job demands are associated with increased rates of depression, anxiety and occupational stress [1] .Moreover, within the broader law enforcement literature occupational stress and burnout have been reported to arise as a result of high job demands [108]; and with emotional exhaustion in a recent study of German police officers [109], illustrating the spectrum of MW outcomes associated with exposure to this stressor.
On consideration of other organisational stressors related to workload and working hours, job pressure, was identified as the strongest predictor of anxiety, PA and burnout. This finding is in line with reviews on correctional officers where job pressure was identified as a significant predictor of burnout [110, 111] and with a recent study where effort-reward imbalance was positively associated with burnout scores in police officers [112]. Long working hours was identified as increasing the risk of PS/PD, EE and DP in police officers within our review. Two reviews were identified that have investigated the relationship between atypical working hours and MW outcomes in the general working population [113, 114] and the results attest similar findings. One concluded that working more than 48 h a week increased the risk of psychological health difficulties [113], whilst the second concluded that working more than 40 h per week or more than 8 h a day increased the risk of developing symptoms of anxiety or depression [114]. No systematic review or meta-analyses that examined the impact of long working hours on police officers were identified.
The impact of interpersonal relationships was examined within our review. Research on correctional officers have illustrated that relationships with co-workers and the resultant feelings of isolation are significant predictors of occupational stress [110]. Confirming the impact of interpersonal relationships on MW, were the results of a study conducted on 1206 police officers that demonstrated that co-worker discourteous and disrespectful behaviours were significant sources of occupational stress [115]. However, this study did not formally assess associations between stressors and MW outcomes. A recent study showed that job resources (team support, shared values and perceived fairness) predicted wellbeing and decreased EE in police officers [109]. Furthermore, judgement from peers was identified as a significant risk factor for depression, consistent with studies on the general working population which provide strong evidence of relationships between workplace bullying and increased depression symptoms [116], anxiety [117], and stress related psychological symptoms [117]. This emotional demand interpersonal relationships can pose on police officers is often referred to as emotional labour [115], where officers have to manage the display of their emotions and maintain the appropriate demeanour expected by both their work and the greater public. The presence of such interpersonal relationship organisational stressors can have consequential effects, given that police officers rely on colleagues in their work [118].
In the wider organisational stress literature, high levels of social support at work from colleagues and supervisors have been found to be protective of mental health [5, 106, 110, 119]. Systematic reviews on the general working population have indicated that low levels of support result in increased levels of PD [106] and predict the onset of depression [119]. Another review of 14 longitudinal studies revealed that lack of social support enhanced depression [120], and a review on correctional officers demonstrated increased levels of occupational stress resulting from lack of support [110]. A study conducted on a special police force unit demonstrated lack of support was a significant risk factor for DP [5]. Similarly, our review identified that low levels of social support resulted in an increased risk of a number of MW outcomes including occupational stress [96], PS/PD [84], EE [86, 91, 92], DP [85, 91] and PA [91]. Only one study in our review investigated the relationship with anxiety and found no evidence of an association [86], whereas no study investigated the relationship between social support and depression.
Lack of support showed no association with suicidal ideation, although only one study investigated this relationship [86]. Only two systematic reviews exist, to the best of our knowledge, which investigate the issue of suicide in the police – Cantor et al. [121] and Hem et al. [122]. Following a review of ten studies, four of which had sample size of 10 or less, Cantor et al. [121] reported evidence of elevated suicide rates in police officers, however specific relationships between suicide and organisational stressors could not be extracted in this study. Hem et al. [122] compared levels of suicide in the police with the general working population and contrarily reported no elevated suicide rates in police officers.
Strengths & Limitations
The primary strength of this review is that it is the first to our knowledge that examines associations across a number of organisational stressors and police officer MW outcomes. Included studies either only looked at police officer populations or carried out sub-analyses, that allowed the relationship between organisational stressors and police officer MW to be extracted. The review was performed and reported in accordance with guidance for undertaking a systematic review [57, 63], adhered to the PRISMA checklist [58], and adopted guidelines for the narrative synthesis where possible [60], making it methodologically robust and reproducible. While the study was not included in an international review database, we have documented every step in a transparent and reproducible fashion (see Additional files 1, 2, 3, 4, 5 and 6). One reviewer undertook selection/assessment of studies, with a proportion checked by second reviewer, to reduce bias and enable discrepancies to be resolved via discussion [57]. Expert opinions and advice were sought from systematic review and epidemiology academics on the development of the research protocol.
All included studies were rated as either high (13 of the 15 included studies) or intermediate (1 of the 15 included studies) quality and adopted self-reporting validated measures for both exposure and outcome data.
Summarising the evidence without or with incomplete statistical pooling has been advocated as useful for reviews but can be considered arbitrary and subjective [123, 124]. Whilst, the labels adopted within the evidence synthesis, should be interpreted with caution, the advantage of the followed strategy is that the underlying process is explicit and reproducible.
The studies included in this review were undertaken across four continents, i.e. Europe, North America, Africa and Asia. In general, all demonstrated similar findings regarding the associations between specific organisational stressors and MW outcomes in police officers, with some differences noted, thereby strengthening the generalizability of the results on an international scale.
As with all systematic reviews, new potentially eligible studies may have been published since the literature search was conducted, which could be a limitation. We have identified three studies that have been published since our search that examine organisational risk factors (shift work [36], job demands and resources [109] and supervisor support [125]) and mental health outcomes (stress [36, 125], EE and wellbeing [109]). The results of these studies are in agreement with the outcomes of our review [109, 125], and present a new significant association between shift work and occupational stress [36]. Additionally, a number of potentially eligible studies could not be accessed in full-text. In addressing this limitation, efforts were made to document the studies which could not be accessed, as well as the efforts undertaken to attempt to retrieve these studies (see Additional file 7: Table S14). Whilst strategies were employed to reduce the odds of missing studies on this subject, the chance that a study was omitted cannot be excluded. Moreover, due to the cross- sectional nature of all included studies, causal relationships could not be established. As demonstrated the significant relationships are complex and of varying strengths, with many stressors occurring concurrently and impacting on numerous outcomes. It cannot be discounted that some organisational stressor and MW outcome relationships have not been identified in the evidence collated for this review. Moreover, due to the paucity of literature on this topic it is possible that a number of organisational stressor and MW outcome relationships still require investigation.
Public health and policy implications
Beneficiaries from a mentally healthy police workforce include the police officers themselves, police organisations, their families, and the public [126]. Reducing poor police officer MW can increase morale, productivity, effectiveness, efficiency and general wellbeing [127], as well as having the potential to reduce compensations claims, on-the-job accidents, civil liabilities for counter-productive behaviour, early retirement and negative perceptions from both the media and public [127].
This review has highlighted the organisational stressors which can be targeted by policies and interventions to reduce the hazard they pose to police officer MW. The organisational stressors shown to impact on police officer mental wellbeing, including lack of support, demand, and interpersonal relationships with colleagues and supervisors, are all amenable to change. It is important therefore to identify the interventions, workplace and other policy changes which address these organisational stressors to promote optimal MW in police officers and these should be incorporated into policing organisational and public health strategies [82]. In addressing lack of support, potential interventions could be aimed at changing the police culture by expanding training and promotion programmes. Flattening the hierarchal structure has also been proposed [41]. Moreover, training specifically for police leaders has been recommended, focusing on awareness of the organisational stressors their employees face, to help reduce their occurrence and mitigate their effects [88].
The success of the recommendations outlined, rely on the resources available to the policing profession. Budget cuts, for instance in the UK police force, in the past decade have seen a decrease in police officer numbers, therefore increasing the demand placed on active officers [128]. Scarce resources allocation could be optimised through increasing police officer numbers; prioritising interventions aimed at promoting support seeking and support services for police officers, therefore shifting the police culture from one that values self-reliance and stoicism to one that promotes the overall wellbeing of their employees [129].
Conclusion
The findings of this review, examining the relationship between organisational stressors and MW in police officers, provide evidence of an association between organisational stressors and occupational stress, depression, PS/PD, Burnout, EE, DP, PA. Those organisational stressors which demonstrated significant relationships with the MW outcomes considered included lack of support from colleagues, supervisors and the organisation, ridicule and set ups, job demand and pressure, and long working hours.
The evidence identified suggests that due to the extent to which police organisational culture, structure and practice can create stressors, strategies which address how officers treat each other, promote support seeking for mental health issues, and provide police leaders with the knowledge to identify and mitigate occupational stress, could be the most effective. However, there is still a lack of evidence surrounding many organisational stressors and specific MW outcomes and especially a lack of evidence on the effectiveness of proactive and reactive strategies to reduce occupational stressors within policing, reinforcing the need for further research. The evidence base should be enhanced with more longitudinal studies, including understudied factors such as interpersonal conflicts and emotional demands [106]. Advancement in this field can lead to improvement in the MW of this occupational group and concomitantly result in benefits for both policing organisations as well as the greater public in which they serve.
Availability of data and materials
All data collected from the literature and analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- CRD:
-
Centre for Reviews and Dissemination
- DP:
-
Depersonalisation
- DRPST:
-
Disaster Related Psychological Screening Test
- ESRC:
-
Economic and Social Research Council
- GHQ:
-
General Health Questionnaire
- HADS:
-
Hospital Anxiety and Depression Scale
- HMICS:
-
Her Majesties Inspectorate of Constabulary Scotland
- HSE:
-
Health and Safety Executive
- ICMJE:
-
International Committee of Medical Journal Editors
- JSS:
-
Job Stress Survey
- MBI:
-
Maslach Burnout Inventory
- MBI-GS:
-
Maslach Burnout Inventory- General Survey
- MBI-HSS:
-
Maslach Burnout Inventory-Human Service Survey
- MH:
-
Mental Health
- MW:
-
Mental Wellbeing
- NOS:
-
Newcastle Ottawa Scale
- ODIN:
-
Occupational Disease Intelligence Network
- ONS:
-
Office for National Statistics
- PA:
-
Personal Accomplishment
- PD:
-
Psychological Distress
- PS:
-
Psychiatric Symptoms
- PSS:
-
Police Stress Survey
- RAG:
-
Red, Amber, Green
- SOSMI:
-
Surveillance of Occupational Stress and Mental Illness
- WHO:
-
World Health Organisation
References
Harvey SB, Modini M, Joyce S, Milligan-Saville JS, Tan L, Mykletun A, Bryant RA, Christensen H, Mitchell PB. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup Environ Med. 2017;74(4):301–10.
Office for National Statistics (ONS), Full report: Sickness absence on the labour market, February 2014. In.: Office for National Statistics (ONS); 2014. Available from: https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/labourproductivity/articles/sicknessabsenceinthelabourmarket/2014-02-25.
Executive HS. Work related stress, anxiety and depression statistics in Great Britain 2016. Suffolk: Health and Safety Executive; 2016.
Deschamps F, Paganon-Badinier I, Marchand A-C, Merle C. Sources and assessment of occupational stress in the police. J Occup Health. 2003;45(6):358–64.
Garbarino S, Cuomo G, Chiorri C, Magnavita N. Association of work-related stress with mental health problems in a special police force unit. BMJ Open. 2013;3(7).
Cherry NM, Chen Y, McDonald JC. Reported incidenc and precipitating factors of work-related stress and mental ill-health in the United Kingdom (1996-2001). Occup Med. 2006;56:414–21.
Garbarino S, Guglielmi O, Puntoni M, Bragazzi NL, Magnavita N. Sleep quality among police officers: implications and insights from a systematic review and meta-analysis of the literature. Int J Environ Res Public Health. 2019;16(5):885.
Penalba V, McGuire H, Leite JR. Psychosocial interventions for prevention of psychological disorders in law enforcement officers. Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.: CD005601. https://doi.org/10.1002/14651858.CD005601.pub2.
Cooper C, Davidson M, Robinson P. Stress in the police service. J Occup Med. 1982;24(1):30–6.
Cooper C, Grimley PJ. Stress among police detectives. J Occup Med. 1983;25(7):534–40.
Biggam FH, Power KG, MacDonald RR, Carcary WB, Moodie E. Self-perceived occupational stress and distress in a Scottish police force. Work Stress. 1997;11(2):118–33.
Brown JM, Campbell EA. Stress and policing: sources and strategies. Oxford: Wiley; 1994.
COEH CfOEH. Occupational physicians reporting activiity. Quarterly report. Manchester: University of Manchester; 2000.
Mind UK [http://www.mind.org.uk].
Bell S, Eski Y. ‘Break a leg- its all in the mind’: police officers’ attitudes towards colleagues with mental health issues. Policing. 2016;10:1–7.
Rollinson D. Organisational behaviour and analysis: an integrated appraoch. 3rd ed. London: Pearson Education Limited; 2005.
Anshel MH. A conceptual model and implications for coping with stressful events in police work. Crim Justice Behav. 2000;27(3):375–400.
Agolla JE. Occupational stress among police officers: the case of Botswana police service. Res J Bus Manag. 2009;3:25–35.
Rand SR, Manuele CA. Stress and police officer performance: an examination of effective coping behavior. Police Stud. 1987;10:122–31.
Ward GE. Physiological, psychological and social issues specifically related to the police profession. Law Order. 1979;27(1):12.
Standards of Professional Behaviour [http://www.scotland.police.uk/assets/pdf/327931/327936/327976/328759/standards-of-professional-behaviour].
Policing Co. Code of ethics a code of practice for the principles and standards of professional behaviour for the policing profession of England and Wales. Coventry: College of Policing Ltd; 2014.
Jaramillo F, Nixon R, Sams D. The effect of law enforcement stress on organizational commitment. Policing. 2005;28(2):321–36.
Goldstein H. Policing a free society. Cambridge: Ballinger Publishing; 1977.
Justice NIo. On-the-job stress in policing reducing it, preventing it. Washington: National Institute of Justice; 2000.
ICMJE ICoMJEI. Recommendations on the conduct, reporting, editing and publication of scholarly work in medical journals. USA: International Committee of Medical Journal Editors (ICMJE); 2015.
Ballard D, McGlone M. Work pressures: new agendas in communication. New York: Routledge; 2017.
Schaufeli WB, Maslach C, Marek T. Profesional burnout: recent developments in theory and research. Washington: Taylor & Francis; 1993.
Territo L, Vetter HJ. Stress and police personnel. J Police Sci Adm. 1981;9(2):195–208.
Alexander DA, Walker LD, Innes G, Irving BL. Police stress at work. London: The Police Foundation; 1993.
Evans BJ, Coman GJ. General versus specific measures of occupational stress: an Australian police survey. Stress Med. 1993;9(1):11–20.
Kop N, Euwema M, Schaufeli W. Burnout, job stress and violent behaviour among Dutch police officers. Work Stress. 1999;13(4):326–40.
Savery L, Soutar G, Weaver J. Stress and the police officer: some Western Australian evidence. Police J. 1993;66(3):227–90.
Crank J, Cullberton R, Hewit J, Regoli B. An assessment of work stress among police executives. J Crim Just. 1993;21:313–24.
UNISON. 2014 police staff stress survey report. London: UNISON; 2014.
Galanis P, Fragkou D, Kaitelidou D, Kalokairinou A, Katsoulas TA. Risk factors for occupational stress among Greek police officers. Policing: An Int J. 2019;42(4):506–19.
Kroes WH. Society’s victims- the police: an analysis of job stress in policing. 2nd ed. Springfied: Charlie Thomas; 1985.
Davey JD, Obst PL, Sheehan MC. Demographic and workplace characteristic which add to the prediction of stress and job satisfaction within the police workplace. J Police Crim Psychol. 2001;16(1):29–39.
Alexander DA, Innes G, Irving BL, Sinclair S, Walker LG. Health, stress and policing: a study in Grampion police. London: The Police Foundation; 1991.
Luceño-Moreno L, García-Albuerne Y, Talavera-Velasco B, Martín-García J. Stress in Spanish police force depending on occupational rank, sex, age and work-shift. Psicothema. 2016;28(4):389–93.
Brough P, Biggs A: Occupational stress in police and prison staff. In: The Cambridge handbook of forensic psychology. Edited by Brown JM, Campbell EA. New York: Cambridge University Press; 2010: 707–717. Brown JM, Campbell EA.
Brown JM, Campbell EA. Sources of occupational stress in the police. Work Stress. 1990;4(4):305–18.
Alexander D, Walker L, Innes G, Irving B. Police stress at work. UK: Police Foundation; 1993.
Violanti JM, Aron F. Ranking police stressors. Psychol Rep. 1994;75(2):824–6.
Kirkcaldy B, Cooper CL, Ruffalo P. Work stress and health in a sample of U.S. police. Psychol Rep. 1995;76(2):700–2.
Koortzen P. The dimensionality of police stressors. Acta Criminologiae et Medicinae Legalis Japonica. 1996;9(2):55–63.
Guelle G, Tredoux C, Foster D. Inherent and organizational stress in the SAPS: an empirical survey in the Western cape. S Afr J Psychol. 1998;28:129–34.
Kim JL, Wells W, Vardalis JJ, Johnson SK, Lim H. Gender difference in occupational stress: a study of the south Korean National Police Agency. Int J Law Crime Justice. 2016;44:163–82.
Oweke JA, Muola J, Ngumi O. Causes of occupational stress in relation to level of occupational stress among police constables in Kisumu County, Kenya. J Humanit Soc Sci. 2014;19(11):13–20.
Husain W. The levels of depression, anxiety and stress in police officers. Acad Res Int. 2014;5(4):458–65.
Marchand A, Durand P. Psychological distress, depression, and burnout: similar contribution of the job demand-control and job-demand-control-support models. J Occup Environ Med. 2011;53(2):185–9.
Liberman AM, Best SR, Metzler TJ, Fagan JA, Weiss DS, Marmar CR. Routine occupational stress and psychological distress in police. Policing: An Int J Police Strateg Manag. 2002;25(2):421–39.
Burke RJ. Work-family stress, conflict, coping, and burnout in police officers. Stress Med. 1993;9(3):171–80.
McCafferty Fl MCE, McCafferty MA. Stress and suicide in police officers: paradigm of occupational stress. South Med J. 1992;85(3):233–43.
Health and Safety Executive (HSE). Striking the balance between operational and health and safety duties in the police service. Suffolk: Health and Safety Executive; 2008.
Kapade-Nikam P, Shaikh M. Occupational stress, burnout and coping in police personnel: findings from a systematic review. Am Int J Res Humant Arts Soc Sci. 2014;14(377):144–8.
Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions version 5.0.2. London: The Cochrane Collaboration; 2009.
Moher D, Liberati A, Fau - Tetzlaff J, Tetzlaff J, Fau - Altman DG, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement; 2015. p. 1539–3704. (Electronic)
Bettany-Saltikov J. How to do a systematic literature review in nursing a step-by-step guide. England: Open University Press; 2012.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, Britten N, Roen K, Duffy S. Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme. Final report. Lancaster University: Lancaster; 2006.
Torgerson C. Systematic reviews. London: Continuum; 2003.
Song F, Parekh S, Hooper L, Loke YK, Ryder J. Dissemination and publication of research findings: an updated review of related biases. Health Technol Assess. 2010;14(8):234.
CRD CfRaDC. Systematic reviews: CRD’s guidance for undertaking reviews in health care. York: Centre for Reviews and Dissemination; 2009.
Bioethics NCo. The findings of a series of engagement activites exploring the culture of scientific research in the UK. London: Nuffield College of Bioethics; 2014.
Boland A, Cherry G, Dickson R. Doing a systematic review a students guide. London: SAGE Publications; 2014.
Aveyard H, Payne S, Preston N. A post-graduates guide to doing a literature review in health and social care. England: Open University Press; 2016.
Whittaker A. Research skills for social work. 2nd ed. London: Learning Matters; 2012.
Data extraction forms [http://dplp.cochrane.org/data-extraction-forms].
Savage E, Callery P. Parental participation in the care of hospitalised children: a review of the research evidence. In: Glasper EA, Ireland L, editors. Evidence based child health care: challenges for practice. Houndmills: Macmillan; 2000. p. 57–87.
The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp].
Herzog R, Álvarez-Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health. 2013;13:154.
Takahashi N, Hashizume M. A systematic review of the influence of occupational organophosphate pesticides exposure on neurological impairment. BMJ Open. 2014;4(6):e004798.
Patra J, Bhatia M, Suraweera W, Morris SK, Patra C, Gupta PC, Jha P. Exposure to second-hand smoke and the risk of tuberculosis in children and adults: a systematic review and meta-analysis of 18 observational studies. PLoS Med. 2015;12(6):e1001835.
Hermont AP, Oliveira PAD, Martins CC, Paiva SM, Pordeus IA, Auad SM. Tooth Erosion and eating disorders: a systematic review and meta-analysis. PLoS One. 2014;9(11):e111123.
McPheeters ML, Kripalani S, Peterson NB, Idowu RT, Jerome RN, Potter SA, Andrews JC. Quality improvement interventions to address health disparities. Closing the quality gap: revisiting the state of the science. Evidence report no.208. Rockville: Agency for Healthcare Research and Quality (ARHQ); 2012.
Rodriguez-Jareño MC, Demou E, Vargas-Prada S, Sanati KA, Škerjanc A, Reis PG, Helimäki-Aro R, Macdonald EB, Serra C. European working time directive and doctors’ health: a systematic review of the available epidemiological evidence. BMJ Open. 2014;4(7):e004916.
Bernard B. A critical review of epidemiological evidence for work-related muscoloskeletal disorders of the neck, upper extremity and low back. Cincinnati: National Institute for Occupational Safety and Health; 1997.
Steenstra I, Verbeek J, Heymans M, Bongers P. Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: a systematic review of the literature. Occup Environ Med. 2005;62(12):851–60.
Leka S, Griffiths A, Cox T. Protecting workers health series No 3: Work organization & stress. Geneva: World Health Organization (WHO); 2004.
Krehbiel TC. Correlation coefficient rule of thumb. Decis Sci J Innov Educ. 2004;2(1):97–100.
How large can a standardized coefficient be? [http://www.ssicentral.com/lisrel/techdocs/HowLargeCanaStandardizedCoefficientbe.pdf].
Adams GA, Buck J. Social stressors and strain among police officers: It’s not just the bad guys. Crim Justice Behav. 2010;37(9):1030–40.
Adebayo DO, Sunmola AM, Udegbe IB. Workplace fairness and emotional exhaustion in Nigeria police: the moderating role of gender. Anxiety Stress Coping. 2008;21(4):405–16.
Arial M, Gonik V, Wild P, Danuser B. Association of work related chronic stressors and psychiatric symptoms in a Swiss sample of police officers; a cross sectional questionnaire study. Int Arch Occup Environ Health. 2010;83(3):323–31.
Backteman-Erlanson S, Padyab M, Brulin C. Prevalence of burnout and associations with psychosocial work environment, physical strain, and stress of conscience among Swedish female and male police personnel. Police Pract Res. 2013;14(6):491–505.
Berg AM, Hem E, Lau B, Ekeberg Ø. An exploration of job stress and health in the Norwegian police service: a cross sectional study. J Occup Med Toxicol (London, England). 2006;1:26.
Chen H-C, Chou FH-C, Chen M-C, Su S-F, Wang S-Y, Feng W-W, Chen P-C, Lai J-Y, Chao S-S, Yang S-L, et al. A survey of quality of life and depression for police officers in Kaohsiung, Taiwan. Qual Life Res. 2006;15(5):925–32.
Crank JP, Regoli R, Hewitt JD, Culbertson RG. Institutional and organizational antecedents of role stress, work alienation, and anomie among police executives. Crim Justice Behav. 1995;22(2):152–71.
Houdmont J, Randall R. Working hours and common mental disorders in English police officers. Occup Med (Oxford, England). 2016;66(9):713–8.
Janzen BL, Muhajarine N, Zhu T, Kelly IW. Effort-reward imbalance, overcommitment, and psychological distress in Canadian police officers. Psychol Rep. 2007;100(2):525–30.
Martinussen M, Richardsen AM, Burke RJ. Job demands, job resources, and burnout among police officers. J Crim Just. 2007;35(3):239–49.
McCarty WP, Skogan WG. Job-related burnout among civilian and sworn police personnel. Police Q. 2013;16(1):66–84.
Morash M, Haarr R, Hoon Kwak D. Multilevel influences on police stress. J Contemp Crim Justice. 2006;22(1):26–43.
Mostert K, Rothmann S. Work-related well-being in the south African police service. J Crim Just. 2006;34(5):479–91.
Xavier P, Prabhakar K. A study of police stress and burnout among Tamil Nadu police. Int J Pharm Sci Rev Res. 2016;38(2):159–61.
Morash M, Kwak D, Hoffman V, Lee C, Cho S, Moon B. Stressors, coping resources and strategies, and police stress in South Korea. J Crim Just. 2008;36(3):231–9.
Sedgwick P. Cross sectional studies: advantages and disadvantages. Br Med J. 2014;349:g2276.
Breakwell GM, Smith JA, Wright DB. Research methods in psychology. 4th ed. London: SAGE Publications; 2012.
Gorrell G, Ford N, Madden A, Holdridge P, Eaglestone B. Countering method bias in questionnaire-based used studies. J Doc. 2011;67(3):507–24.
Schaufeli WB, Enzmann D, Girault N. Measurement of burnout: a review. In: Schaufeli WB, Maslach C, Marek T, editors. Professional burnout: recent developments in theory and research. Washington D.C: Taylor and Francis; 1993. p. 199–215.
Donnelly E. Work-related stress and posttraumatic stress in emergency medical services. Prehosp Emerg Care. 2012;16(1):76–85.
Babbie E. The basics of social research. 6th ed. USA: CENGAGE Learning; 2014.
Hoddinott SN, Bass MJ. The Dillman Total design survey method. Can Fam Physician. 1986;32:2366–8.
Phillips AW, Reddy S, Durning SJ. Improving response rates and evaluating nonresponse bias in surveys: AMEE guide no. 102. Med Teach. 2016;38(3):217–28.
Bhopal R. Concepts of epidemiology. 3rd ed. Oxford: Oxford University Press; 2016.
Nieuwenhuijsen K, Bruinvels D, Frings-Dresen M. Psychosocial work environment and stress-related disorders, a systematic review. Occup Med (Lond). 2010;60(4):277–86.
de Lange AH, Taris TW, Kompier MAJ, Houtman IL, Bongers PM. ‘The very best of the Millenium’ : longitudinal research and the demand-control-(support) model. J Occup Health Psychol. 2003;8(4):282–305.
Whitehead J, Lindquist C. Job stress and burnout among probation/parole officers: perceptions and causal factors. Int J Offender Ther Comp Criminol. 1985;29(2):109–19.
Wolter C, Santa Maria A, Wörfel F, Gusy B, Lesener T, Kleiber D, Renneberg B. Job demands, job resources, and well-being in police officers—a resource-oriented approach. J Police Crim Psychol. 2019;34(1):45–54.
Finney C, Stergiopoulos E, Hensel J, Bonato S, Dewa CS. Organizational stressors associated with job stress and burnout in correctional officers: a systematic review. BMC Public Health. 2013;13:82.
Schaufeli WB, Peeters MCW. Job stress and burnout among correctional officers: a literature review. Int J Stress Manag. 2000;7(1):19–48.
Violanti JM, Mnatsakanova A, Andrew ME, Allison P, Gu JK, Fekedulegn D. Effort-reward imbalance and Overcommitment at work: associations with police burnout. Police Q. 2018;21(4):440–60.
Sparks K, Cooper C, Fried Y. The effects of hours of work on health: a meta-analytic review. J Occup Organ Psychol. 1997;70:391–408.
Bannai A, Tamakoshi A. The association between long working hours and health: a systematic review of epidemiological evidence. Scand J Work Environ Health. 2014;40:5–18.
Collins PA, Gibbs AC. Stress in police officers: a study of the origins, prevalence and severity of stress-related symptoms within a county police force. Occup Med (Oxford). 2003;53(4):256–64.
Theorell T, Hammarstrom A, Aronssen G. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health. 2015;15:738.
V B, Atasayi S, Molendijk ML. Workplace bullying and mental health: a meta-anlysis on cross-sectional and longitudinal data. PLoS One. 2015;10(8):e0135225.
Graf F. The relationship between social support and occupational stress among police offciers. J Police Sci Adm. 1986;14:178–86.
Stansfeld S, Candy B. Psychosocial work environment and mental health- a meta-analytic review. Scand J Environ Health. 2006;32(6):443–62.
Netterstrom B, Conrad N, Bech P, Fink P, Olsen O, Rugulies R, Stansfeld S. The relation between work-related psychosocial factors and the development of depression. Epidemiol Rev. 2008;30:118–32.
Cantor CH, Tyman R, Slater PJ. A historical survey of police suicide in Queensland Australia 1843-1992. Suicide Life Threat Behav. 1995;25:499–507.
Hem E, Berg AM, Ekeberg AO. Suicide in police--a critical review. Suicide Life Threat Behav. 2001;31(2):224–33.
de Vet HC, Van Tulder MW, Bouter LM. Levels of evidence: intellectual aid or absolute judgement. J Clin Epidemiol. 2003;56:917–78.
Ferreira PH, Ferreira ML, Maher CG. Effect of applying different ‘levels of evidence’ criteria on conclusios of Cochrane reviews of interventions for low back pain. J Clin Epidemiol. 2002;55:1126–9.
Li JCM, Cheung JCK, Sun IY. The impact of job and family factors on work stress and engagement among Hong Kong police officers. Policing: An Int J. 2019;42(2):284–300.
Dewa CS, McDaid D, Ettner SL. An international perspective on worker mental health problems: who bears the burden and how are costs addressed? Can J Psychiatr. 2007;52(6):346–56.
Finn P, Tomz JE. Developing a law enforcement stress program for officers and their families. In: Issues and practices in criminal justice. Washington D.C: National Insitute of Justice; 1996.
Elliot-Davies M, Houdmont J. Officer demand, capacity and welfare survey descriptive statistics summary report: mental health and wellbeing January 2017. Surrey: Police Federation of England and Wales (PFEW); 2017.
Brown J. From cult of masculinity to smart macho: gender perspectives on police occupational culture. In: O’Neil M, Marks M, Singh AM, editors. Police occupational culture: new debates and discussion. Oxford: Elsevier; 2007. p. 189–210.
Acknowledgements
AP would like to acknowledge the advice and assistance of Dr. Cathy Johnman, Dr. Hilary Thompson, Ms. Mhairi Campbell, and Paul Cannon on approaches, methodology and searches.
Funding
Medical Research Council (MC_PC_13027) to ED for her fellowship. The views and opinions expressed are those of the authors and do not necessarily reflect those of the Medical Research Council. The funding body had no role in the study design, in the collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
AP conducted all the literature searches, screened the studies, conducted data extraction and analysis and drafted the manuscript. ED screened a proportion of studies, contributed to data interpretation and writing of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
No conflict of interest. ED is a member of the editorial board (Associate Editor) of BMC Public Health. After undertaking this review, ED has received part-funding from a police organisation to conduct a different project on police wellbeing issues.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
Personal Communications with experts.
Additional file 2: Tables S2, S3, S4, S5, S6
and S7. PICO Statement (S2), Grey literature sources (S3), and Search Strategies Adopted for Systematic Review (Table S4-S7).
Additional file 3: Table S8.
PICO Screening Template (Table S8).
Additional file 4: Table S9.
Excluded Studies with Reason for Exclusion (Table S9).
Additional file 5: Tables S10
and S11. Results of Modified NOS Risk of Bias Assessment for all Included Studies (Table S10) and Summary of Included Studies (Table S11).
Additional file 6: Tables S12
and S13. Process Adopted to Determine Overall Magnitude of Association of Included Studies by Outcome (Table S12) and Overall Degree of Evidence Grade by MW Outcome (Table S13).
Additional file 7: Table S14.
Eligible Studies following Title and Abstract Screening, which could not be accessed in Full-text (Table S14).
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Purba, A., Demou, E. The relationship between organisational stressors and mental wellbeing within police officers: a systematic review. BMC Public Health 19, 1286 (2019). https://doi.org/10.1186/s12889-019-7609-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-7609-0