
Abstract
Background
At present, only a few studies have focused on the risk factors for depression in elderly diabetic patients, and there is little evidence for the effect of metformin in depressed elderly patients with diabetes than on its effect on blood glucose. The aim of the current work was to study the risk factors for depression in elderly diabetic patients and to ascertain the effects of metformin on the depressive state.
Methods
We initiated a 1:4 matched case–control study. The case group comprised 110 elderly diabetic patients with depression from nine communities in Shenyang in 2017. The control group comprised 440 non-depressed elderly diabetic patients from the same communities, which were matched by gender and age (± 2 years of age) with the case group. Depression was measured using the Geriatric Depression Scale-15, and we performed matched univariate and multivariate logistic regression analyses.
Results
In the multivariate analysis, overweight status, poor physical capabilities and low activity level, and the presence of more than two additional illnesses were risk factors for depression in elderly patients with diabetes. For these risk factors, the adjusted ORs (all P < 0.05) were as follows: an adjusted OR of 2.031 and 95% CI of 1.180–3.495; an adjusted OR of 2.342 and 95% CI of 1.465–3.743; and an adjusted OR of 5.350 and 95% CI of 2.222–12.883, respectively. Patients taking metformin had a lower risk of depression than those taking no medication, with an adjusted OR of 0.567 and 95% CI of 0.323–0.997 (P < 0.05).
Conclusions
Overweight status, poor physical capabilities and low activity level, and the presence of more than two additional illnesses were risk factors for depression in elderly diabetic patients, and metformin was a protective factor against depression in elderly diabetic patients.
Similar content being viewed by others


Background
China has a large, rapidly expanding elderly population, and it currently leads the world in this category. Since 1980, China’s population of individuals over 60 years of age has, in fact, grown by an average of 3.2% annually; and, currently, the proportion of those individuals 60 years and older in China is 17.3% of the total. In 2017, China became the only country in the world to have more than 200 million elderly [1].
Diabetes mellitus, a chronic metabolic disease, has reached epidemic status; and it now poses one of the major threats to human health of the twenty-first century. In 2017, the International Diabetes Federation (IDF) estimated that 425 million individuals worldwide were suffering from diabetes mellitus, and it is expected that the number will rise to 629 million in 2045 [2]. Complications of diabetes mellitus can cause increased morbidity, disability, and mortality, enough to pose a threat to the economies of all countries, especially those that are still developing [3]. Over the past few decades, prediabetes and diabetes have become more common in both the developed and developing parts of China. A recent national study of a representative sample of 170,287 adults from 31 provinces on the Chinese mainland reported the age-standardized prevalence of diabetes and prediabetes to be 10.9 and 35.7%, respectively. The prevalence of elderly patients with diabetes and prediabetes was 20.2 and 45.8%, respectively [4].
Depression is a multifaceted phenomenon that involves loss of satisfaction, hope, energy, and interest; and it is often accompanied by feelings of helplessness, worthlessness, boredom, and a loss of interest in previously enjoyed activities [5, 6]. The prevalence of depression also differs across different parts of China. Presently, diabetes and depression are prevalent in both developed and developing countries; and it has been confirmed that diabetes can increase the risk of depressive symptoms to some extent, while depression can increase the risk of developing diabetes [7, 8]. Depression can impinge on a patient’s self-management ability and hinder her or his adherence to treatment regimens [9]. Although there have been tremendous advancements in the diagnosis and treatment of diabetes, depression in diabetic patients remains underdiagnosed and undertreated [10]. Unrecognized and untreated depression in diabetic patients lead to a higher prevalence of depression and a probability of greater severity; which in turn causes poor glycemic control, lower adherence to medication, higher treatment costs, and a higher mortality rate [11]. Furthermore, the available studies have suggested that the presence of depression—co-morbid with diabetes—is associated with a poorer self-reported health status and more adverse outcomes [12,13,14]. According to other published studies, the prevalence of depression is approximately 20% of patients with type 2 diabetes mellitus (T2DM) [14, 15]. A meta-analysis by Knol found that adults with depression have a 37% increased risk of developing T2DM [16]. In another study, the authors observed a bidirectional relationship between new-onset diabetes and depression, and showed depression to be associated with a 60% increased risk of T2DM; whereas T2DM showed a more modest association with depression [17]. The great increase in the risk of co-morbid depression in diabetic patients might be attributed to the psychosocial burden of disease, poor social support, awareness of having a chronic disease or its related complications and disabilities, and the consequential psychologic burden [11]. Also, co-morbid depression among persons living with diabetes is associated with poor markers of diabetes control, including glycemic control, retinopathy, nephropathy, neuropathy, micro-vascular complications, and sexual dysfunction [18].
Metformin, which is widely used as a first-line treatment for patients with T2DM, has been in use for over 60 years. It can reduce hepatic glucose output and increase the insulin-mediated utilization of glucose [19, 20]. In addition to its hypoglycemic activity, metformin has been shown to elicit marked anti-inflammatory, antioxidant, and neuroprotective activities and to improve memory function and learning [10, 21, 22]. Another study also indicated that metformin treatment (especially long-term usage) was associated with a lower risk of cognitive impairment in older adults with diabetes [23]. The pleiotropic pharmacologic activities of metformin, then, makes it suitable for the treatment of diabetes mellitus and co-morbid depression, the latter involving a myriad of pathophysiologic characteristics. The aforementioned study confirmed that metformin improved hyperglycemia and depressive-like behavior primarily through synergistic effects on the HPA axis and on oxidative stress and monoamine transmission [10]. The Saghar study also suggested that metformin ameliorated methamphetamine-induced depression, cognition impairment, and neurodegeneration in rats via the CREB/BDNF and Akt/GSK3 signaling pathways [24].
Various studies on diabetes and depression and on depression and the elderly have been published [25, 26]. However, only a few studies have focused on the risk factors for depression in elderly diabetic patients, and there is less evidence for the effects of metformin in depressed elderly patients with diabetes than for its effect on blood glucose. Our primary aim, therefore, was to identify the risk factors for depression in elderly diabetic patients and to determine the effects of metformin on this group.
Methods
Study design and participants
We used United Nations (UN) guidelines, which define elderly individuals as 60 years old and older [27]. The subjects in our study were examined and recruited from May to October 2017, and the source population consisted of nine residential communities in Shenyang, Liaoning, located in northeastern China. We used the Geriatric Depression Scale (GDS) score and selected a case group of 110 elderly diabetic subjects with depression and a control group of elderly diabetic subjects without depression using 1:4 matching according to sex and age (+ 2 years). Our study was approved by the Ethics Committee of China Medical University (Shenyang, China, AF-SOP-07-1.0–01), and all procedures were conducted in accordance with ethical standards. All participants provided written consent after being informed of the use of their personal information, benefits of the study, inherent medical programs, and confidentiality agreements. For illiterate participants, we obtained written informed consent from their relatives.
Study patient consent and measurements
Data were collected during a single visit to the clinic by endocrinologists and trained nurses in face-to-face interviews that used a standard questionnaire. Before the survey was administered, we required that all eligible investigators attend an organized training session. This training included providing the purpose of the study, instructions for administering the questionnaire, the standard methods of measurement used, the importance of standardization, and the study procedures themselves. All investigators were required to undergo rigorous testing after the training, and only those who scored perfectly on our test were allowed to proceed further. Our inspectors were given further instruction and support during the data collection period.
Data on demographic characteristics, such as name, gender, age, cultural level, marital status, health insurance coverage, pension status, previous medical history (including hypertension, cerebrovascular disease, diabetes, and other health problems), and lifestyle factors (such as diet, smoking, and alcohol consumption) were obtained by interview with a standardized questionnaire. Educational level was divided into primary school or less, middle school, and high school or more. Smoking status was divided into a non-smoking group, a smoking group, and a former smoking group. Drinking status over the past year was based upon consumption of alcohol beverage at least twice per week, with an average alcohol consumption of 40 g at one sitting; participants were divided into a non-drinking group, a drinking group, and a former drinking group. Physical capability and activity were divided into two groups: good ability and activity (can climb at least 4 flights of stairs) vs. poor ability and activity.
Physical examination included height and weight. We measured height and weight to the nearest 0.1 cm and 0.1 kg, respectively, while the subjects were fasting and wearing light-weight clothing, with their feet parallel and without shoes. Body mass index (BMI) was calculated as the weight in kilograms divided by the (height in meters) squared. The diagnostic criteria of obesity in China are derived from the common knowledge of experts on the prevention and treatment of adult obesity in China [28]. Individuals with BMI ≥24 kg/m2 were considered to be overweight and those with BMI ≥28 kg/m2 were considered to be obese.
Fasting blood samples from participants were collected by standard venipuncture, and separation of serum was performed by double centrifugation with a laboratory centrifuge. All blood samples were collected and stored at − 80 °C until analyzed. Plasma glucose levels were measured using the glucose oxidase method, and plasma glycated hemoglobin (HbA1c) levels were detected using an automated glycosylated hemoglobin analyzer (Bio-Rad, US).
The presence of type 2 diabetes mellitus for allocation into groups was diagnosed based upon the 1999 World Health Organization criteria [29]. A diagnosis of diabetes is often prompted by such symptoms as increased thirst and urine volume, recurrent infections, unexplained weight loss, and, in severe cases, drowsiness and coma. High levels of glycosuria are usually present, with a fasting plasma glucose concentration ≥ 7.0 mmol/L or 2 h post glucose load ≥11.1 mmol/L, or both. The diagnosis of diabetes should always be confirmed by repeating the test on another day unless there is unequivocal hyperglycemia with acute metabolic decompensation or obvious symptoms [29]. All health-related diseases except diabetes were self-reported, and this has shown satisfactory diagnostic accuracy in epidemiologic studies. In many cases, the findings have been further confirmed by medical records [30, 31].
We ascertained the depression status of patients at the time of recruitment using the Geriatric Depression Scale (GDS)-15 as the evaluation tool. The GDS-15 is a short, 15-item self-reporting scale for assessing depression and is a validated depression scale. Each item can have 2 answers, i.e., yes or no; the highest possible score is 15, which indicates the most severe depressive state. We also used a cut-off point of 5 or more, as the original version of GDS-15 had a sensitivity of 97% and a specificity of 95% [6, 32]. A score of 0–4 was considered normal; 5–8 indicated mild depression; 9–11 indicated the presence of moderate depression; and 12–15 indicated severe depression.
At baseline, anti-diabetic medications taken by the participants were ascertained from self-reports. Participants were divided into a no-medication group, metformin users, and those using other hypoglycemic drugs. Metformin users were further divided into subgroups. All metformin regimens in this group fell within a dosage range of 1.0–2.0 g/d, but some patients used metformin alone and others used it combined with other hypoglycemic drugs. Anti-diabetic medications (hypoglycemic agents) other than metformin included sulfonylureas, glinide class drugs, glycosidase inhibitors, thiazolidinediones, DPP-4 inhibitors, a GLP-1 receptor agonist, SGLT2 inhibitors, and insulin.
Exclusion criteria
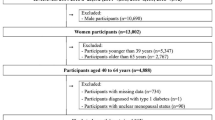
In the first round of selection, we excluded participants who were non-diabetic, who were under 60 years of age, and those who had depression or other mental illnesses. We also excluded from analyses those individuals who had incomplete data, and those who had an illness that was either terminal (such as cancer), or who required urgent medical attention. The final participant population consisted of 550 subjects (110 in the case group and 440 matched controls) from a community in Shenyang City in Liaoning Province, China.
Statistical analyses
EpiData was used to build the database. We performed conditional univariate and multivariate logistic regression analyses due to the matching design using SPSS 20.0 software. Odds ratios (OR) are reported with their respective 95% confidence intervals (CI), and values of P < 0.05 were considered statistically significant.
Results
General study conditions
A total of 550 participants were included in the present study: there were 110 elderly diabetic subjects with depression selected as the case group; and there were 86 cases who were classified as having mild depression, 14 cases with moderate depression, and 10 cases with severe depression. The mean age (± standard deviation) of the participants was 70.15 ± 6.50 years, with a male-to-female ratio of 1:1.6. There were an additional 440 elderly diabetic subjects without depression who were selected as the control group by 1:4 matching according to sex and age (+ 2 years). Descriptions of all demographic and clinical characteristics of cases and controls are given in Table 1.
1:4 Matched univariate logistic regression analysis
Univariate logistic regression analysis showed that diabetic subjects taking metformin had a lower risk of depression than those taking no medication, with an adjusted OR of 0.506 and a 95% CI of 0.299–0.856 (P < 0.05). However, patients taking other hypoglycemic drugs showed no significant differences from controls with respect to the prevalence of depression. Those with depression were more likely to be overweight, have poorer physical capabilities and activity, or manifest more than two additional illnesses. All differences were statistically significant at P < 0.05. There were no significant differences in the prevalence of depression among groups with respect to fasting blood-glucose, HbA1c, education, presence of a companion, having a pension, sleep duration, alcohol use, or smoking status (P > 0.05) (Table 2).
1:4 Matched multivariate logistic regression analysis
The factors showing statistical differences in the above univariate analysis were then introduced into the multivariate paired logistic model for a stepwise regression analysis. The results showed that type of hypoglycemic drug, BMI, physical capability and activity, and number of additional illnesses were statistically significant; i.e., overweight status, poor physical capability and activity, and more than 2 additional illnesses were risk factors for depression in elderly patients with diabetes—with an adjusted OR of 2.031 and a 95% CI of 1.180–3.495, an adjusted OR of 2.342 and 95% CI of 1.465–3.743, and an adjusted OR of 5.350 and 95% CI of 2.222–12.883, respectively (P < 0.05 for all comparisons). Patients who took metformin had a lower risk of depression than those taking no medication, with an adjusted OR of 0.567 and 95% CI of 0.323–0.997 (P < 0.05), while patients taking other hypoglycemic drugs showed no significant differences from patients who did not take any medication (Table 3).
Discussion
To the best of our knowledge, this is the first matched case–control study to evaluate the risk factors for depression in elderly diabetic patients and also the first to assess the association of metformin with the depressive state.
Some investigators have established that age, female gender, low family income, lower educational levels, higher HbA1c levels, and higher BMI are risk factors for concomitant depression in individuals with T2DM [33, 34]. Such individuals feel dissatisfied with their lives, abandon many of their activities and interests, and feel an emptiness to their lives. However, diabetes control can be improved by increasing a patients’ self-efficacy and ability to care for their own illnesses [35]. Notably, female patients with diabetes are likely to have a higher prevalence of depressive symptoms than men. Another study reported that female gender, age, poor glycemic control, obesity, diabetic complications, and insulin therapy in the Chinese population were risk factors for T2DM when combined with depression [36]. However, there are also studies establishing that the association of diabetes and depression was independent of an individual’s education and household income. Additionally, the presence of depression was not affected by other sociodemographic factors, BMI, hypertension, or the number of diabetes-associated complications [37]. We here used a 1:4 matched case–control design, which was different from the cross-sectional research design reported in the aforementioned study. In the current study, the participants were over 60 old; and their age and gender were matched to those of the controls, since variability in these factors might have an untoward impact on the results. Case matching was performed to render the research more efficient and to ensure the reliability of the results. In the present study we suggest that the association of diabetes and depression in the elderly was independent of companionship, having a pension, and tobacco use. This may be because a high proportion (81.45%) of people in our group had partners and a high proportion (91.6%) had pensions. Smokers constituted only 12.4% of the total. Also, we reported that neither poor fasting blood glucose control nor high HbA1c levels increased the risk of depression in elderly diabetics. This may be because our research population was not a completely cross-sectional study group and that the number of cases was relatively small. Additionally, in our study, the relative score of our depressed population was lower and the degree of depression was milder. Among the 110 cases, 86 exhibited mild depression, which may have had an effect on the results.
Although there were no significant differences in the prevalence of depression among elderly diabetic patients with respect to sleep duration (overall p value > 0.05), our study showed that relatively longer sleep duration prone to protect diabetes patients from depressive symptoms, which was similar to previous studies [8, 38]. However, no consistent conclusion as to the effect of educational level on depression: some investigators have observed that people with a lower educational level are prone to depression [33, 34], while others observed that there was no correlation between educational level and depression [14, 37]. Our study also show that, in elderly patients with diabetes mellitus, there was no correlation between educational level and depression although it seems that patients with higher educational background tended to manifest depression. It may be that more highly educated and elderly diabetic patients in China tend to obsess over the disease and become more prone to depression. This was similar to a study in China where ruminative thinking was a predictor of future depressive symptoms among the elderly in nursing homes [39]. The effect of alcohol consumption on depression is also controversial, and our study showed that there was no correlation between alcohol use and depression, although the prevalence of depression in elderly diabetic with current alcohol use was higher than in non-drinkers.
Multivariate analysis revealed that, among elderly diabetic patients, those who were overweight, with poor physical capability and activity, and having multiple additional illnesses, had an increased risk of depression; while the use of metformin decreased the risk of depressive symptoms. We, however, reached no uniform conclusion as to the relationship between BMI and depression. While some studies have also shown a lack of correlation between BMI and depression [8, 40], other investigators observed that BMI was associated with depression [41, 42]. The risk of depression increased with increasing BMI, but the average BMI in our study was less than 24 [36]. Studies have also reported that changes in BMI were significantly closely correlated with changes in depression, i.e., that patients who lost more weight experienced greater improvements in depressive symptoms [43,44,45]. Our study showed that the prevalence of depression in the overweight group was higher than that in the normal-weight group (although this difference was not statistically significant, the incidence of depression tended to be higher with obesity). It is conceivable that Chinese are generally thinner than people from other countries. Once people become overweight, they may then become more depressed as their BMI increases; although obese people may not care as much about weight, which may leave them less anxious. Elderly people who have good physical capabilities and activity can generally go for walks, exercise, and talk with people in the community; and as a result their mood can be relatively pleasant, with a lower risk of depression. This is similar to the conclusions reported by Narita et al., where physical activity helped ameliorate depression in patients with diabetes [46]. Elderly people with multiple diseases are also likely to suffer from depression, which is similar to the findings of another recent study [47]. One reason for this may be the possibility of increased physical discomfort and increased psychologic burden caused by multiple diseases, and the another reason might be that the disease involves greater financial costs.
Metformin is a first-line hypoglycemic drug for type 2 diabetics. Recent research, however, has suggested that metformin also exerts an antidepressant effect through improvement of cognitive function in depressed patients with diabetes mellitus [22]. Additionally, it has been reported that both metformin monotherapy and its metformin used in combination with telmisartan can normalize depressive moods, reduce proinflammatory mediators, and ameliorate dysfunctions of the hypothalamic-pituitary-adrenal (HPA) axis, thereby providing beneficial effects in diabetes-induced depression [48]. In older men with type 2 diabetes, metformin reduced the likelihood of depression by 5.0, 2.8, and 15.6% in the high cancer risk class, the high CVD risk class, and the high frailty risk class, respectively [49]. Shivavedi observed that monotherapy with metformin and combination therapy with both metformin and ascorbic acid induced significant reductions in plasma corticosterone concentrations and adrenal weight. The effects of metformin and metformin in combination with ascorbic acid also caused significant reductions in oxidative stress and proinflammatory cytokines. Our current study suggests that metformin therapy could be a potential strategy to treat T2DM and co-morbid depression [10]. One study showed that individuals with undiagnosed depression might be at increased risk for non-adherence to metformin use [50], and other studies have shown that metformin does not improve depression. For example, for patients with post-stroke depression combined with T2DM, metformin did not ameliorate the depressive symptoms [51]. Co-administration of pioglitazone or metformin with low-dose fluoxetine did, however, improve mechanical allodynia, thermal hyperalgesia, and neurohistopathologic changes; and co-administration of pioglitazone improved depressive-like behavior in the peripheral nerve injury model of neuropathic pain in rats but co-administration of metformin, did not [52]. It was also reported that metformin had minimal effects on depressive symptoms (comparable to placebo), although it changed the HOMA-IR [53]. One underdiagnosed side effect of metformin is the increased risk of cobalamin (vitamin B12) deficiency due to diminished uptake of cobalamin by the terminal ileum, and cobalamin deficiency was associated with an increased risk of depression and decreased cognitive performance. It follows, then, that metformin might increase the risk of depression [54]. However, in our study, we found that in elderly diabetic patients, those on metformin exhibited a lower risk of depression than those on other hypoglycemic drugs or those on no medication—a finding similar to that reported in previous studies in which metformin alleviated depression [10, 22, 48, 49]. The mechanisms underlying this finding, however, require further study.
One advantage of this study is the close matching of cases to controls. Because the purpose of this work was to assess the relationship between metformin and depression, we controlled for the age and gender of the study participants at the recruitment stage, considering both potential confounding factors. Both cases and controls were recruited by the same research assistant from the same population of the same source to reduce confounding bias. The study also had a number of limitations. First, all health-related diseases except diabetes were self-reported, and because the study was a matched design, the associations of age and gender with depression in study participants could not be determined. Second, the subjects with diabetes in our study had all received treatment, and we did not include any participants who were newly diagnosed. One possible influencing factor for depression that was not taken into account was the duration of diabetes mellitus. Fourth, because many of the participants who had depression or other mental illnesses might have been taking anti-depressant medications or antipsychotics, and since these medications may reduce the burden of depressive symptoms and thus reduce the association of risk factors with current symptoms, we excluded them. Fifth, the group of metformin users included only those who used metformin or those who used metformin along with other hypoglycemic drugs. The control group was treated with monotherapy or a combination of hypoglycemic drugs other than metformin. We did not evaluate effects of hypoglycemic drugs other than metformin between the two groups. There were also some defects in our study design, but the observed association between metformin and depression was attributable to the effects of metformin alone and not the interactive effects of metformin with other hypoglycemic drugs. Such factors could conceivably create some study bias.
Conclusions
In summary, we here showed that the risk factors for depression in elderly patients with diabetes mellitus are complicated, including overweight status, poor physical capabilities and activity, and more than two additional illnesses. While these were risk factors for depression in elderly diabetic patients, metformin was found to be a protective factor against depression in this group.
Availability of data and materials
Inquiries regarding the availability of primary data should be directed to the principal investigator, Professor Difei Wang.
Abbreviations
- BMI:
-
Body mass index
- CIs:
-
Confidence intervals
- FPG:
-
Fasting plasma glucose
- GDS-15:
-
Geriatric Depression Scale-15
- HPA:
-
Hypothalamic-pituitary-adrenal axis
- ORs:
-
Odds ratios
- T2DM:
-
Type 2 diabetes mellitus
- UN:
-
United Nations
- WC:
-
Waist circumference
References
National Bureau of Statistics of the People's Republic of China. Statistical bulletin of the national economic and social development of the People's Republic of China in 2017 [N]. People's Daily. 2018;(010).
Ogurtsova K, da Rocha Fernandes JD, Huang Y, Linnenkamp U, Guariguata L, Cho NH, Cavan D, Shaw JE, Makaroff LE. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50.
Papatheodorou K, Papanas N, Banach M, Papazoglou D, Edmonds M. Complications of diabetes 2016. J Diabetes Res. 2016;2016:6989453.
Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, Li Y, Zhao Z, Qin X, Jin D, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. Jama. 2017;317(24):2515–23.
Lloyd CE, Sartorius N, Cimino LC, Alvarez A, Guinzbourg de Braude M, Rabbani G, Uddin Ahmed H, Papelbaum M, Regina de Freitas S, Ji L, et al. The INTERPRET-DD study of diabetes and depression: a protocol. Diabet Med. 2015;32(7):925–34.
Imai H, Yamanaka G, Ishimoto Y, Kimura Y, Fukutomi E, Chen WL, Matsuoka S, Tanaka M, Sakamoto R, Wada T, et al. Factor structures of a Japanese version of the geriatric depression scale and its correlation with the quality of life and functional ability. Psychiatry Res. 2014;215(2):460–5.
de Groot M, Doyle T, Averyt J, Risaliti C, Shubroo J. Depressive symptoms and type 2 diabetes mellitus in rural appalachia: an 18-month follow-up study. Int J Psychiatry Med. 2015;48(4):263–77.
Yu S, Yang H, Guo X, Zheng L, Sun Y. Prevalence of depression among rural residents with diabetes mellitus: a cross-sectional study from Northeast China. Int J Environ Res Public Health. 2016;13(6):E542.
Kramer MK, Kriska AM, Venditti EM, Miller RG, Brooks MM, Burke LE, Siminerio LM, Solano FX, Orchard TJ. Translating the diabetes prevention program: a comprehensive model for prevention training and program delivery. Am J Prev Med. 2009;37(6):505–11.
Shivavedi N, Kumar M, Tej G, Nayak PK. Metformin and ascorbic acid combination therapy ameliorates type 2 diabetes mellitus and comorbid depression in rats. Brain Res. 2017;1674:1–9.
Khaledi M, Haghighatdoost F, Feizi A, Aminorroaya A. The prevalence of comorbid depression in patients with type 2 diabetes: an updated systematic review and meta-analysis on huge number of observational studies. Acta Diabetol. 2019;56(6):631–50.
Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the world health surveys. Lancet (London, England). 2007;370(9590):851–8.
Lin EH, Rutter CM, Katon W, Heckbert SR, Ciechanowski P, Oliver MM, Ludman EJ, Young BA, Williams LH, McCulloch DK, et al. Depression and advanced complications of diabetes: a prospective cohort study. Diabetes Care. 2010;33(2):264–9.
Wang X, Shen B, Zhuang X, Weng W. Investigating factors associated with depressive symptoms of chronic kidney diseases in China with type 2 diabetes. J Diabetes Res. 2017;2017:1769897.
Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of co-morbid depression in adults with type 2 diabetes: a systematic review and meta-analysis. Diabet Med. 2006;23(11):1165–73.
Knol MJ, Twisk JW, Beekman AT, Heine RJ, Snoek FJ, Pouwer F. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia. 2006;49(5):837–45.
Mezuk B, Eaton WW, Albrecht S, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care. 2008;31(12):2383–90.
Niraula K, Kohrt BA, Flora MS, Thapa N, Mumu SJ, Pathak R, Stray-Pedersen B, Ghimire P, Regmi B, Macfarlane EK, et al. Prevalence of depression and associated risk factors among persons with type-2 diabetes mellitus without a prior psychiatric history: a cross-sectional study in clinical settings in urban Nepal. BMC Psychiatry. 2013;13:309.
He L, Sabet A, Djedjos S, Miller R, Sun X, Hussain MA, Radovick S, Wondisford FE. Metformin and insulin suppress hepatic gluconeogenesis through phosphorylation of CREB binding protein. Cell. 2009;137(4):635–46.
Labuzek K, Suchy D, Gabryel B, Bielecka A, Liber S, Okopien B. Quantification of metformin by the HPLC method in brain regions, cerebrospinal fluid and plasma of rats treated with lipopolysaccharide. Pharmacol Rep. 2010;62(5):956–65.
Pintana H, Apaijai N, Pratchayasakul W, Chattipakorn N, Chattipakorn SC. Effects of metformin on learning and memory behaviors and brain mitochondrial functions in high fat diet induced insulin resistant rats. Life Sci. 2012;91(11–12):409–14.
Guo M, Mi J, Jiang QM, Xu JM, Tang YY, Tian G, Wang B. Metformin may produce antidepressant effects through improvement of cognitive function among depressed patients with diabetes mellitus. Clin Exp Pharmacol Physiol. 2014;41(9):650–6.
Ng TP, Feng L, Yap KB, Lee TS, Tan CH, Winblad B. Long-term metformin usage and cognitive function among older adults with diabetes. J Alzheimers Dis. 2014;41(1):61–8.
Keshavarzi S, Kermanshahi S, Karami L, Motaghinejad M, Motevalian M, Sadr S. Protective role of metformin against methamphetamine induced anxiety, depression, cognition impairment and neurodegeneration in rat: the role of CREB/BDNF and Akt/GSK3 signaling pathways. Neurotoxicology. 2019;72:74–84.
Oh DJ, Han JW, Min BJ, Jeong HG, Kim TH, Choi SH, Lim S, Lee JJ, Park JH, Lee SB, et al. Association of up-Regulated Plasma Adiponectin with Risk of incident depression in a community-dwelling elderly population. J Clin Psychiatry. 2018;79(3):17m11695.
Pun VC, Manjourides J, Suh HH. Association of neighborhood greenness with self-perceived stress, depression and anxiety symptoms in older U. S adults. Environ Health. 2018;17(1):39.
World Health Organization (WHO). Definition of an older or elderly person. Health statistics and information systems 2014.
Department of Obesity, Endocrinology, Chinese Medical Association. Consensus of Chinese experts on prevention and treatment of adult obesity. Chin J Endocr Metab. 2011;27(9):711–7.
World Heath Organization. Definition, diagnosis and classification of diabetes mellitus and its complications: part 1: report of a WHO consultation: diagnosis and classification of diabetes mellitus. Geneva: World Health Org; 1999.
Miller DR, Rogers WH, Kazis LE, Spiro A 3rd, Ren XS, Haffer SC. Patients’ self-report of diseases in the Medicare health outcomes survey based on comparisons with linked survey and medical data from the veterans health administration. J Ambul Care Manag. 2008;31(2):161–77.
Kotsani M, Chatziadamidou T, Economides D, Benetos A. Higher prevalence and earlier appearance of geriatric phenotypes in old adults with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2018;135:206–17.
Balogun RA, Balogun SA, Kepple AL, Ma JZ, Turgut F, Kovesdy CP, Abdel-Rahman EM. The 15-item geriatric depression scale as a predictor of mortality in older adults undergoing hemodialysis. J Am Geriatr Soc. 2011;59(8):1563–5.
Katon W, von Korff M, Ciechanowski P, Russo J, Lin E, Simon G, Ludman E, Walker E, Bush T, Young B. Behavioral and clinical factors associated with depression among individuals with diabetes. Diabetes Care. 2004;27(4):914–20.
Engum A, Mykletun A, Midthjell K, Holen A, Dahl AA. Depression and diabetes: a large population-based study of sociodemographic, lifestyle, and clinical factors associated with depression in type 1 and type 2 diabetes. Diabetes Care. 2005;28(8):1904–9.
Rashid AA, Zuhra H, Tan CE. Social support, self-efficacy and their correlation among patients with type 2 diabetes mellitus: a primary care perspective. Med J Malaysia. 2018;73(4):197–201.
Chen G, Wu Y, Wang T, Liang J, Lin W, Li L, Wen J, Lin L, Huang H. Association between serum endogenous secretory receptor for advanced glycation end products and risk of type 2 diabetes mellitus with combined depression in the Chinese population. Diabetes Technol Ther. 2012;14(10):936–42.
Islam SM, Ferrari U, Seissler J, Niessen L, Lechner A. Association between depression and diabetes amongst adults in Bangladesh: a hospital based case-control study. J Glob Health. 2015;5(2):020406.
Sakamoto N, Nanri A, Kochi T, Tsuruoka H, Pham NM, Kabe I, Matsuda S, Mizoue T. Bedtime and sleep duration in relation to depressive symptoms among Japanese workers. J Occup Health. 2013;55(6):479–86.
Gan P, Xie Y, Duan W, Deng Q, Yu X. Rumination and loneliness independently predict six-month later depression symptoms among Chinese elderly in nursing homes. PLoS One. 2015;10(9):e0137176.
Fung ACH, Tse G, Cheng HL, Lau ESH, Luk A, Ozaki R, So TTY, Wong RYM, Tsoh J, Chow E, et al. Depressive symptoms, co-morbidities, and glycemic control in Hong Kong Chinese elderly patients with type 2 diabetes mellitus. Front Endocrinol. 2018;9:261.
Jantaratnotai N, Mosikanon K, Lee Y, McIntyre RS. The interface of depression and obesity. Obes Res Clin Pract. 2017;11(1):1–10.
Mannan M, Mamun A, Doi S, Clavarino A. Prospective associations between depression and obesity for adolescent males and females- a systematic review and meta-analysis of longitudinal studies. PLoS One. 2016;11(6):e0157240.
Burgmer R, Legenbauer T, Muller A, de Zwaan M, Fischer C, Herpertz S. Psychological outcome 4 years after restrictive bariatric surgery. Obes Surg. 2014;24(10):1670–8.
Mitchell JE, King WC, Chen JY, Devlin MJ, Flum D, Garcia L, Inabet W, Pender JR, Kalarchian MA, Khandelwal S, et al. Course of depressive symptoms and treatment in the longitudinal assessment of bariatric surgery (LABS-2) study. Obesity (Silver Spring). 2014;22(8):1799–806.
Faulconbridge LF, Wadden TA, Thomas JG, Jones-Corneille LR, Sarwer DB, Fabricatore AN. Changes in depression and quality of life in obese individuals with binge eating disorder: bariatric surgery versus lifestyle modification. Surg Obes Relat Dis. 2013;9(5):790–6.
Narita Z, Inagawa T, Stickley A, Sugawara N. Physical activity for diabetes-related depression: a systematic review and meta-analysis. J Psychiatr Res. 2019;113:100–7.
Birk JL, Kronish IM, Moise N, Falzon L, Yoon S, Davidson KW. Depression and multimorbidity: considering temporal characteristics of the associations between depression and multiple chronic diseases. Health Psychol. 2019; [Epub ahead of print].
Aswar U, Chepurwar S, Shintre S, Aswar M. Telmisartan attenuates diabetes induced depression in rats. Pharmacol Rep. 2017;69(2):358–64.
Wang CP, Lorenzo C, Habib SL, Jo B, Espinoza SE. Differential effects of metformin on age related comorbidities in older men with type 2 diabetes. J Diabetes Complicat. 2017;31(4):679–86.
Gonzalez JS, Peyrot M, McCarl LA, Collins EM, Serpa L, Mimiaga MJ, Safren SA. Depression and diabetes treatment nonadherence: a meta-analysis. Diabetes Care. 2008;31(12):2398–403.
Hu Y, Xing H, Dong X, Lu W, Xiao X, Gao L, Cui M, Chen J. Pioglitazone is an effective treatment for patients with post-stroke depression combined with type 2 diabetes mellitus. Exp Ther Med. 2015;10(3):1109–14.
Murad H, Ayuob N. Co-Administration of Pioglitazone Improves Fluoxetine's Antinociceptive, neuroprotective, and antidepressant effects in chronic constriction injury in rats. Pain physician. 2015;18(6):609–20.
Kashani L, Omidvar T, Farazmand B, Modabbernia A, Ramzanzadeh F, Tehraninejad ES, Ashrafi M, Tabrizi M, Akhondzadeh S. Does pioglitazone improve depression through insulin-sensitization? Results of a randomized double-blind metformin-controlled trial in patients with polycystic ovarian syndrome and comorbid depression. Psychoneuroendocrinology. 2013;38(6):767–76.
Biemans E, Hart HE, Rutten GE, Cuellar Renteria VG, Kooijman-Buiting AM, Beulens JW. Cobalamin status and its relation with depression, cognition and neuropathy in patients with type 2 diabetes mellitus using metformin. Acta Diabetol. 2015;52(2):383–93.
Acknowledgements
Not applicable.
Funding
This work was supported by the Liaoning Department of Education (L2015564), Shenyang Municipal Science and Technology Project (F17–231–1-56), and the Science and Technology Plan Project of Liaoning (AF-SOP-07-1.0–01).
Author information
Authors and Affiliations
Contributions
FQ Chen analyzed the data and wrote the paper. FQ Chen, GZ Wei, YF Wang, TT Liu, T Huang, Q Wei, and GJ Ma enrolled participants and collected data. DF Wang was responsible for designing the study and performing data analyses. All the authors contributed to the interpretation of the data and the critical revision and approval of the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of China Medical University (Shenyang, China, AF-SOP-07-1. 0–01). All procedures were performed in accordance with ethical standards. Written consent was obtained from all participants after they had been informed of the objectives, benefits, medical items, and confidentiality agreement regarding their personal information.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chen, F., Wei, G., Wang, Y. et al. Risk factors for depression in elderly diabetic patients and the effect of metformin on the condition. BMC Public Health 19, 1063 (2019). https://doi.org/10.1186/s12889-019-7392-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-7392-y