
Abstract
Background
In Eritrea, facility delivery rates show great discrepancy within urban centers. This study was conducted in Akordet, a multi-cultural lowland town of Gash-Barka Region, aiming at assessing the factors influencing facility delivery.
Methods
A community based analytical cross-sectional study was conducted among a total of 282 mothers who gave birth within the 2 years preceding the data collection time. Data collection was carried out by going house-to-house and interviewing the mothers using a structured closed ended questionnaire. Bivariate and multivariate logistic regressions were used to determine the magnitude of the relationship between place of delivery and the explanatory variables (Religion, Ethnicity, Mother’s educational level, Husband’s Educational level, Place of delivery preceding last pregnancy, Birth order of last child, Any complications during previous delivery, First ANC Visit during last pregnancy, Number of ANC visits during last pregnancy and Any complication during last pregnancy.). For this study, p-value ≤0.05 was considered as statistically significant.
Results
The rate of facility delivery in this setting was found to be 82.3%. Almost all (96.1%) the mothers had at least one ANC visit during their last pregnancy, with the majority (59.7%) visiting ANC clinics during second trimester for the first time. Mothers whose educational level is junior and above (AOR 8.8, CI: 1.18–65.64), whose husband’s educational level is junior and above (AOR 3.92, CI: 1.03–14.54), who gave birth in health facility before the last pregnancy (AOR 8.16, CI: 3.41–19.48), and those who had complications during last pregnancy (AOR 2.24, CI: 1.04–4.82) were more likely to deliver in a health facility. Mothers whose last child’s birth order was 4th -6th were less likely (AOR 0.24, CI: 0.090.62) to deliver at health facility.
Conclusions
Early initiation of ANC and regularity in attendance should be emphasized. Health educations given to pregnant mothers should try to persuade the mothers that each pregnancy and ensuing delivery is unique. Empowering the community in general and women in particular by increasing the level of participation in education might payoff in high level of facility delivery.
Similar content being viewed by others


Introduction
Maternal mortality has dropped by 45% worldwide, from 1990 through 2013. [1] However, globally about 830 women die every day due to preventable pregnancy related causes [2], 99% of this occurring in developing countries. [3] The maternal mortality ratios (MMR) show huge discrepancies between the developed (16 per 100,000 live births) and the developing nations (240 per 100,000 live births), and more than half (56%) of these maternal deaths occur in the sub-Saharan Africa. [4] Furthermore, the maternal mortality shows grater discrepancy within sub-Saharan countries. [5, 6] The large number of maternal deaths, especially in developing countries, has been attributed to the low levels of maternal health care seeking behavior, as evidenced by low proportions of antenatal care utilization and extremely low deliveries attended by a skilled-person. [7, 8]
The quality of child delivery outcome can only be enhanced through proper antenatal-care (ANC) coupled with better choice of place of delivery as recommended by health authorities. [9,10,11] Furthermore, place of delivery is found to be one of the key predictors of neonatal mortality. [12] The World Health Organization (WHO) has been recommending at least four antenatal care (ANC) visits during pregnancy, and that postnatal care should be provided at 6 h, 6 days, 6 weeks, and 6 months after childbirth to ensure women’s physical and mental wellbeing. [13] As such, chances are very low for the women who gave birth at home to get this important postnatal care. [14]
Despite the encouraging trends in antenatal care service utilization coverage, delivery in health facilities is still challenging in developing countries. Several studies have presented that poor availability of resources and services as the major cause of underutilization of maternal health services. [15, 16] Nevertheless, in some settings, even if the services are readily available, these facilities are not always available to women of some socio-economic classes. [17]
Access to and utilization of available skilled birth attendance services is hampered by a number of factors including social and cultural contexts, religious beliefs, inadequate skilled health personnel, and long distances to health facilities. [1, 6] This means, there is still a lot of work that needs to be done in order to register significant increase in skilled birth attendance.
Eritrea is one of the three Sub Saharan African countries that has achieved the Millennium Development Goal 5 [18] and has made significant progress in maternal health by reducing the maternal mortality (MMR) from 998/100,000 in 1995 [19] to 352/100,000 in 2010 [20]. However, the current average annual decline rate of 6.5%, 1990–2015, is projected to ask Eritrea, two decades to match with the global average MMR of 210/100,000 [18]. This requires the country to invest a lot of resources into the Maternal and Child Health program to reach the Sustainable Development Goal 3, which calls reduction of global maternal mortality ratio to less than 70 per 100,000 live births and to end preventable deaths of newborns and under-five children by the year 2030. [21] A study done in Eritrea, back in 2004, reported that 16% of maternal deaths occurred during pregnancy, 48% during childbirth, and 36% during the postpartum period. This study also identified four delays as the causes of the maternal death; failure or delay in recognition of danger signs, delay in deciding to seek care, delay in reaching appropriate care, and delay in receiving appropriate care. [22]
Although antenatal care coverage in Eritrea is very high, ranging from 84.2% in rural areas to 97.3% in urban areas, skilled birth attendance in health facilities is still very low, from 16.5% in rural to 73.2% in urban settings. [20] This low level of health facility delivery rate is occurring despite the fact that roughly each community in Eritrea now has maternal and child health (MCH) services free of charge. All urban centers have at least one health center within a reasonable distance for the majority of the residents, but still the 2010 Eritrean Population and Health Survey (EPHS) shows a great discrepancy in the rate of facility delivery within urban centers, from 92.5% in the capital, Asmara, to an average of 62.5% in other towns. [20] This suggests that factors other than availability and accessibility of health facilities are playing in the background to reduce facility delivery attendance. A qualitative study conducted by Chol et al. [23] in Asmara, Eritrea, recognized two main factors as facilitators of women’s access and utilization of maternal health services. These factors were health education, either through mass media or sessions in the health facility, and women’s empowerment. Another study conducted in rural Eritrea identified several socioeconomic and demographic factors, related both to the mother and the husband, as determinants of facility delivery. In addition, this study identified some health facility related factors, like distance and quality of care, to affect choice of place of delivery. [24] This calls for localized evidence on determinants of place of delivery to understand the phenomenon. This is vital in identifying key priority areas for policy and practice, and increasing the rate of facility delivery.
Gash-Barka, the largest administrative region in the country, is where the lowest rate of facility delivery was observed, with only 18% of women giving birth in health facilities, and the most common reason mentioned being distance to health facility. [20] This study was conducted in Akordet, a multi-cultural lowland town of Gash-Barka region, aiming at assessing the socio-demographic factors of women which influence facility delivery.
Data and methods
Study design and setting
A community based analytical cross-sectional study was conducted on December 2017 in the town of Akordet, Eritrea. The town has one hospital and one health center that provides maternal and child health services. The target population was women who have had at least one delivery. Women who gave birth within 2 years preceding the data collection date and who were permanent residents of the town were included in this study. Severely sick, mentally ill and primigravida women, who were pregnant during the data collection time, were excluded from the study.
Sample size and sampling technique
Initially, this study was meant to be a census type of study. According to the town Administration Office, there were a total of 313 women who gave birth within the 2 years preceding the data collection time. Based on the data from the Office, a list of eligible mothers was prepared. Once the study participants were identified, community health agents helped data collectors to identify individual mother’s house. However, in this study, a total of 282 mothers, who fulfilled the inclusion criteria, were included. The main reason for the failure of women from participating in the study was unavailability of the mother at home during data collection time.
Data collection tools and methods
Data collection was carried out by interviewing the mothers using a structured closed ended questionnaire. The questionnaire was developed after a vigorous review of literature on determinants of place of delivery in similar settings. This questionnaire was composed of several parts, which included socio-demographic characteristics of the mothers, ANC visits, pregnancy and child birth experience, and place of delivery. The questionnaire was distributed to experts on the field for content assessment in respect to the study setting. Then pretest of the questionnaire was conducted 2 weeks prior to the actual data collection time, to make the data collection tool more understandable and culture sensitive. Based on the insight gained during the pretest the question “income of the household”, which is sensitive, was changed with “perceived wealth index”. The reliability of the questionnaire was identified using Guttman’s λ3 coefficient, and it was found to be 0.76.
Outcome and explanatory variables
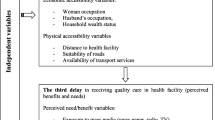
The mothers were asked about the place of their last delivery, which had a dichotomous outcome, either home or health facility. Thus, in this study place of delivery was the outcome variable. Based on a review of the literature and the study setting, we selected to analyze 17 explanatory variables which have the potential to influence place of delivery. This includes; maternal age, marital status, sex of household head, religion, ethnicity, maternal education, husband education, perceived wealth class, ownership of means of transportation, birth order of last child, adverse birth outcomes during delivery preceding the last pregnancy, regular ANC visit during the last pregnancy, time of the first ANC visit, number of total ANC visits during the last pregnancy, any pregnancy related problem during the last pregnancy, and sex of ANC provider.
Data analysis method
After checking the data for completeness, it was coded and feed into Statistical Package for Social Sciences version 23 for analysis. Simple frequencies and proportions were used to describe the socio-demographic and pregnancy related characteristics of the respondents and Chi-square test was used to assess the relationship between place of delivery and the explanatory variables. Variables found to have statistically significant association with the dependent variable, during chi-square analysis, were further assessed by using bivariate and multivariate logistic regression to determine the magnitude of the relationship between the outcome variable and the independent variables, if there was any. For this study, p-value ≤0.05 was considered as statistically significant.
Results
This study included a total of 282 mothers. The age of the participants ranged between 17 and 42 years, with a median age of 27 and inter-quartile range of 8 [IQR 23–31]. Women who were in the age group of 26 up to 35 years accounted the highest proportion (47.5%) of the participants. Almost all the mothers were married (96.5%), and male headed households accounted 66.7%. Most (78.7%) of the participants were Muslims and from the Tigre ethnic group (68.1%). Almost half (49.6%) of the mothers had elementary level of education and 91.8% were housewives. Ownership of Means of Transportation was found to be only 8.5% and most (64.2%) of the participants perceived their wealth class to be “Middle Class”. Most of the husbands’ had educational level of elementary and above, and 42.6% were government employees. (Table 1).
The most common (68.8%) age at first delivery was between 18 and 24 years old, with only 7.4% of the mothers giving their first birth after they reached their 25th birthday. However, 34.4% of the mothers were 30 years old or above, and 7.4% were between the ages of 16–19 years old when they gave their last birth. Majority (57.8%) of the mothers’ last child’s birth order was 1st to 3rd and 12.8% of the mothers had complications during delivery preceding the last pregnancy. Only 35.5% of the mothers gave birth in health facility preceding the last delivery. However, during the last delivery this number rose to 82.3%. The most common reasons mentioned for home delivery were lack of Transportation and the Comfort to give birth at home, 46 and 32% respectively. Out of all the participants only 1.1% received postnatal care. The mothers were asked as to the “ideal place of delivery” and 64.9% said at health facility, 29.1% said at home by skilled birth attendant while 6% opted for home delivery by a traditional birth attendant (TBA). (Table 2).
Almost all (96.1%) of the mothers had at least one ANC visit during their last pregnancy, with the majority (59.7%) of them visiting ANC clinics during the second trimester of the pregnancy for the first time. Of these mothers, only 70% reported to be regular attendees of ANC services and only 58.1% had visited ANC clinics for four times or more. Majority (89.7%) of the participant were attended in ANC clinics by male health workers. The most common reasons mentioned for not attending ANC were “lack of knowledge” (26.7%) and being “busy at home” (26.7%). (Table 3).
Bivariate analysis
In this study seventeen explanatory variables were set to be assessed, out of which eleven were found to be significant predictors of place of delivery using bivariate analysis (p ≤ 0.05). Mothers whose religion is Christian (COR 2.79, CI: 1.05–7.39), had elementary level of education (COR 2.24, CI: 1.13–4.45) or junior and above (COR 9.91, CI: 2.2–44.4) level of education, have husband with junior and above level of education (COR 5.45, CI: 2.03–14.62), who gave birth in health facility before the last pregnancy (COR 3.85, CI:2.03–7.28), who had experienced complications during previous deliveries (COR 2.22, CI: 1.06–4.68), who had visited ANC for 4 to 6 times (COR 2.33, CI:1.2–4.5) or ≥ 7 times (COR 5, CI:1.12–22.27), and who had complications during last pregnancy (COR 1.9, CI:1.02–3.52) were more likely to deliver at health facility. On the other hand, mothers from Tigre (COR 0.34, CI: 0.12–0.91) or the other ethnicities (COR 0.11, CI: 0.03–0.39) were less likely to deliver in a health facility as compared to the mothers from the Tigrinya ethnic group. In addition, mothers whose last child’s birth order was 4th- 6th (COR 0.37, CI: 0.18–0.73) or ≥ 7th (COR 0.24, CI: 0.09–0.63), and who made their first ANC visit, during their last pregnancy, at some stage in the third trimester (COR 0.18, CI: 0.05–0.59) were less likely deliver at health facility. (Table 4).
Multivariate analysis
Out of the eleven variables which were found to have a statistically significant association with place of delivery, in the bivariate analysis, only five variables remained to be significant predictors of place of delivery in the multivariate analysis. Mothers whose educational level is junior and above (AOR 8.8, CI: 1.18–65.64), whose husband’s educational level is junior and above (AOR 3.92, CI: 1.03–14.54), who gave birth in health facility before the last pregnancy (AOR 8.16, CI: 3.41–19.48), and those who had complications during last pregnancy (AOR 2.24, CI: 1.04–4.82) were more likely to deliver in a health facility as compared to their counterparts. Those mothers whose last child’s birth order was 4th -6th were less likely (AOR 0.24, CI: 0.090.62) to deliver at health facility. (Table 4).
Discussion
This study found that the proportion of mothers who gave birth at a health facility to be 82.3% in this urban setting. This proportion is much higher than the zonal and overall urban average of 18 and 63% respectively and slightly lower than that of Asmara, the capital city, which was 93% in 2010. [20] The reason for this high proportion of facility delivery could be due to increased awareness of the population since 2010, given the fact that the proportion of facility delivery within this study group increased from 35.5% in previous delivery to 82.3% during the last delivery. Another reason could be due to the fact that this study included only women living in the town of Akordet, who can have relatively good access to health facilities and transportation services as compared to women living in the satellite settlements of the sub-zone. This high facility delivery rate in this setting, which approximated the rate in Asmara, is commendable, as, though classified as urban centers, the two settings markedly defer in their level of urbanization. The rate of facility delivery in this study was higher when compared to study findings from other similar settings, like local studies from Ethiopia (73.2%), Nigeria (65%), Tanzania (56%) and Kenya (42%). [25,26,27] This could be due to the inherent difference between these setting in accessibility to health facility and socio-cultural structure.
Transportation problem was the most frequently mentioned reason by the mothers who gave birth at home. This seems to be a legitimate problem as 91.5% of the mothers in this study reported to have no means of transportation of their own. This is supported by the 2010 EPHS finding where distance was mentioned as a barrier for facility delivery by 40% of Gash-Barka women. [20] The second most common reason for home delivery was “comfort”, mentioned by 32% for the mothers, which seems an opinion of most of the mothers in this study; as almost third of them mentioned home delivery with skilled birth attendant as an “ideal” environment for childbirth. These women who chose home delivery might have had previous experience with home delivery that had no complications, and therefore, opted for the same place, where they can be comforted in a familiar setting with their beloved ones neighboring them during delivery. [28] In this study home delivery by TBAs was mentioned as an ideal setting for child delivery by 6 % of the participants. Taking into account the study setting and the high ANC coverage, the reason for this choice can be attributed to the prevailing faith in the skills and expertise of TBAs, easy availability when needed and the traditional views and religious beliefs regarding delivery as in many other settings. [29,30,31]
The ANC service attendance seems to be a common place in this setting as 96.1% of the study participants had at least one visit. Again this finding is higher than that of the zonal average of 84.7%, the national average of 89% [20] and the Sub-Saharan Africa average of (49%) [8]. However, the regularity in attendance (70.0%) and the proportion of mothers having the recommended four or more ANC visits, which was 58.1%, though higher than the national average of 57.4%, is not satisfactory as compared to the 74.9% for women living in other towns of the country. [20] The reason for this reduction could be the way women perceive the whole concept of ANC, aside from getting some material support like bed-nets which are distributed at first contact with the pregnant mother. Another factor can be the timing of first ANC visit, the later the mother’s first visit the lower the chance for her to have four or more visits. This is supported by other finding from this study, as only 20.5% of the mothers had their first ANC visit during the first trimester. This proportion was lower than the national and urban-setting average of 26.6 and 39.1% respectively [20] and 25.5% of an Ethiopian study [32]. Several reasons have been put forward as to why pregnant women start ANC later during pregnancy, most of them being related to socioeconomic factors. [33] However, this needs to be studied further in this setting. This low frequency and irregularity of ANC visit needs to be dealt with as antenatal care remains to be a vital health care tool to reduce the risk of pregnancy and delivery related complications. [34, 35] The most common reasons for not attending ANC in this study were being busy with home chores and lack of knowledge on ANC, mentioned by 26.7% of the participants who never attended ANC.
Factors associated with facility delivery
Several socio-demographic and personal experiences related factors were found to determine the place of delivery on logistic regression analysis. Religion was one of the factors influencing institutional delivery in this setting. Mothers who are Christians were 2.7 (COR) times more likely to deliver in health facility. This was similar with studies done in Nigeria and Ethiopia where Christian mothers were more likely to deliver in a health facility as compared to Muslim mothers. [36,37,38] On the other hand, a qualitative study conducted to uncover the effect of religion on place of deliver found no difference in preference between Muslim and Christian mothers. [39] This calls for a better-quality analysis of the pathways in which religion affects the choice of place of delivery. Another factor affecting place of delivery was mother’s negative experience in previous deliveries, as women with this experience were found to have 2.2 (COR) times higher odds of delivering in health facility. This indicates that women’s personal belief, as to the safety of oneself during delivery, can be the main reasons for why women choose to get facility or skilled delivery. [40] In this study only 64.9% of the mothers mentioned health facility as the “ideal place” to give birth, despite the large proportion of facility delivery. This indicates that facility delivery could be high, even if the clients prefer to deliver at home, because of safety reasons.
Educational level is also one of the most important factors in determining selection of place of delivery. Women with educational level of junior and above were 8.8 (AOR) times more likely to give birth in health facility as compared to those who have lower levels of education. Similarly, husbands’ educational level was also important in determining place of delivery as women whose husbands had junior and above level of education found to have higher odds of facility delivery (AOR = 3.92). This finding was similar with results of several studies where educational level of the mother and her partner was found to significantly affect the choice of place of delivery. [37, 41,42,43,44] The reason for this could be the effect of educational level in increasing the person’s cognitive ability to comprehend health education materials which in turn helps the persons to take better health choices, though the effects might be direct or indirect. [45, 46]
Increased frequency of ANC visit was associated with facility delivery as mothers who had four or more ANC visits were 2.7 (COR) times more likely to deliver at health facility as compared to those who had less than four visits, which is consistent with other study findings. [47, 48] This could be due to the fact that increased contact time with health care providers creates a platform to put emphasis on the importance of facility delivery [34, 49] or because those mothers who have high ANC visits are those who already have good health seeking behavior. These women with high ANC visit could also be mothers with some pregnancy related complications, who were told to visit ANC frequently by the health care providers and subsequently told to delivery at a health facility. This can be supported by the fact that, in this study women who had any pregnancy related complication were found to be 1.9 (COR) times more likely to delivery at health facility. Nonetheless, the relationship between increased number of ANC visit and facility delivery implies the WHO’s new guideline, which requires every pregnant mother to have at least 8 ANC visits, [50] will contribute towards increased facility delivery.
Previous experience of facility delivery was found to be a strong predictor of place of delivery, as those women who delivered in health facility during the pregnancy preceding the last one were 8.6 (AOR) times more likely to choose the same setting for the next delivery. This could be influenced by being familiar with the heath facility delivery setting and the trust the mothers built on it. Birth order of the last child was also one of the variables which predict place of delivery. As the birth order of the child increases, the probability of facility delivery decreases. As compared to the mothers whose child’s birth order was 1st to 3rd, those with 4th to 6th were 76% (AOR 0.24) less likely to give birth in a health facility. This was similar with the EPHS 2010 [20] findings, where Forty-eight percent of first order births delivered in health facilities, as compared to only 23% of the 6+ birth orders, and findings from other studies. [43, 51]
Another factor that was found to negatively affect the probability of facility delivery was the trimester in which the mothers visited ANC for the first time. Mothers who visited ANC during the last trimester were 0.18 times less likely to deliver at hospital. This finding was similar to a study conduced in rural Ghana, where it was found women who stared ANC visit after the second trimester were less likely to have facility delivery. [48] This seems like mothers who go to ANC during the end of the pregnancy are doing so, to check their status before deciding the place of delivery, as it was found in a phenomenological study of home delivery conducted in Ethiopia. [52]
The effect of ethnicity in determining the place of delivery in this setting was assessed and the results of bivariate logistic regression showed that mother from the Tigre and other ethnic groups were 65.6 and 89% less likely to give birth in a health facility as compared to the mothers from the Tigrinya ethnic group. This difference could be attributed to the fact that the people of the Tigrinya ethnic group in this study setting are either a government workers or engage in business, which increases their probability to be affluent. Affluence was found to be one of the most important determinants of facility delivery in many developing countries. [15, 20, 53] Furthermore, since these ethnicities differ culturally and religion wise, Tigrinya mothers, who came from other place, may not easily get TBAs who knows their tradition of delivery. This may force them to opt to use facility delivery, although it requires further research to understand the direct effect of culture and religion on choice of place of delivery in this setting.
Limitation of the study
The study was conducted among women living within the town of Akordet, which limits its ability to generalize about women living in the Sub-Zone. There might be some recall bias with regard to initiation and frequency of ANC service. In addition, this study was not able to assess the wealth quintile of the family objectively, rather used perceived wealth class, which may affect the result of the statistical test.
Conclusion
This study founds out that the rate of facility delivery in Akordet town to be high. The ANC coverage was universal with limitations in frequency and regularity of checkups. Emphasis should be put on the importance of starting ANC visits as early as possible. Mother’s level of education, husband’s level of education, place of preceding delivery, birth order of last child and complications during pregnancy were independent predictors of place of delivery in the study setting. The choice of home delivery with health professional was high in this community which needs to be given due attention, since comfort was one of the main reasons for home delivery. The issue of transportation during the time of delivery, which was the main reason for home delivery, should also be addressed by providing ambulance services to help the mothers get easy physical access to health facilities. To address the effect of religion and culture on utilization of maternal health services, health education programs on maternal health should include religious leaders and community elders as target audiences. Health educations given to pregnant mothers, through mass media and in ANC clinics, should persuade the mothers that each pregnancy and the ensuing delivery is unique, in order to avert deterioration on personal appraisal of the need for facility delivery in subsequent births. Empowering the community in general and women in particular by increasing their level of participation in education might payoff in high level of facility delivery. The findings of this study call for a prompt adoption and enforcement of the new WHO guideline on ANC by the health authorities, at all levels of health services delivery. In addition, it is empirical to study the need and the feasibility of introducing skilled-person assisted home delivery, by learning from experiences of settings that have already adopted it. Finally, national public health policies should give room for local and context specific community requirements to make the maternal health services acceptable to local consumers.
Availability of data and materials
The data set analyzed during this study is available from the corresponding author on reasonable request.
Abbreviations
- ANC:
-
Antenatal Care
- AOR:
-
Adjusted Odds Ratio
- COR:
-
Crude Odds Ratio
- EPHS:
-
Eritrean Population and Health Survey
- MCH:
-
Maternal and Child Heath
- MMR:
-
Maternalmortality ratios
- TBA:
-
Traditional Birth Attendants
- WHO:
-
World Health Organization
References
World Health Organization. United Nations agencies report steady progress in saving mothers’ lives: news release 2014, Available at: https://www.who.int/mediacentre/news/releases/2014/maternal-mortality/en/.
World Health Organization. Maternal mortality. Fact sheet no 348. Geneva: WHO; 2015.
UNICEF. Fact of the week. 99%: the proportion of maternal deaths that occur in developing countries 2015, Available at: https://www.unicef.org/factoftheweek/index_39707.html.
UNFPA. UNFPA support to maternal health 2000-2011. Thematic Evaluation. 2012:2.
Alliance for Maternal and Newborn Health Improvement. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in South Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Health 2018, 6: e1297–308. https://doi.org/10.1016/S2214-109X(18)30385-1
Henry VD, Sangwani NS, Maryam AA. Health facility delivery in sub-Saharan Africa: successes, challenges, and implications for the 2030 development agenda. BMC Public Health. 2018;18(765). https://doi.org/10.1186/s12889-018-5695-z.
Christiana RT, Michael JD, Christine LR. Factors associated with underutilization of antenatal care services in Indonesia: results of Indonesia demographic and health survey 2002/2003 and 2007. BMC Public Health. 2010;10:485.
Maureen NS, Thembelihle SPN, Thandeka JB. Access and utilization of antenatal care services in a rural community of eThekwini district in KwaZulu-Natal. International Journal of Africa Nursing Sciences. 2018;7:1–7.
Raatikainen K, Heiskanen N, Heinonen S. Under-attending free antenatal care is associated with adverse pregnancy outcomes. BMC Public Health. 2007;7:268.
Chen X-K, Wen SW, Yang Q, Walker MC. Adequacy of prenatal care and neonatal mortality in infants born to mothers with and without antenatal high-risk conditions. Australian & New Zealand Journal of Obstetrics & Gynecology. 2007;47(2):122–7.
Jana K, Sebastian V. Antenatal care services and its implications for vital and health outcomes of children: evidence from 193 surveys in 69 low-income and middle-income countries. BMJ Open. 2017;7. https://doi.org/10.1136/bmjopen-2017-017122.
Justice A, Honorati M, Renay W, Shalom AA, Owusu-Agyei S. Impact of place of delivery on neonatal mortality in rural Tanzania. International Journal of MCH and AIDS. 2012;1(1):49–59.
World Health Organization. Provision of effective antenatal care: Integrated Management of Pregnancy and Childbirth (IMPAC) 2016.
Daniel A, Diana M, Mark K. Determinants of postnatal care use in Kenya. Afr Popul Stud. 2014;28(3):447–59.
Asmeret MM. Levels and determinants of use of institutional delivery care services among women of childbearing age in Ethiopia: analysis of EDHS 2000 and 2005 data. Demographic and health surveys. USAID 2013.
Mohammad HP, MdNasim-Us S, Jalal U, Ulrika E. Progress in the utilization of antenatal and delivery care services in Bangladesh: where does the equity gap lie? BMC Pregnancy and Childbirth. 2016;16:200. https://doi.org/10.1186/s12884-016-0970-4.
Suleman HI, Mohammed NS, Muhammed SI. Barriers to utilisation of maternal health services in a semi-urban community in northern Nigeria: the clients’ perspective. Niger Medical Journal. 2013;54(1):27–32. https://doi.org/10.4103/0300-1652.108890.
Charles O, Emily WK,Yerdanos T. Assessment report of the government of the state of Eritrea (GoSe) and UNFPA 4th country Programme (2013–2016). International Development Institute Africa 2016.
National Statistics Office. Eritrea Demographic and Health Survey. Macro international Inc. Maryland USA: Calverton; 1995. p. 1997.
National Statistics Office. Eritrea population and health survey 2010. Fafo institute for applied international studies Oslo, Norway. 2013.
Sachs JD. From millennium development goals to sustainable development goals. Lancet. 2012;379:2206–11.
Mismay G, Mona S, Khama R, et al. Magnitude and causes of maternal deaths at health facilities in Eritrea in 2007. Journal of Eritrean Medical Association.
Chol C, Cynthia H, Berhane D, et al. Stakeholders’ perspectives on facilitators of and barriers to the utilisation of and access to maternal health services in Eritrea: a qualitative study. BMC Pregnancy and Childbirth. 2018;18(35). https://doi.org/10.1186/s12884-018-1665-9.
Meron MK, Hana FK, Hermon TG, Goitu SA, Michael BA. Health facility or home delivery? Factors influencing the choice of delivery place among mothers living in rural communities of Eritrea. J Health Popul Nutr. 2018;37(22).
Woiynshet GK, Aschalech A, Asefa T, Shitaye S, Simret H, Dinkalem G, Mesfine M. Assessment of factors affecting institutional delivery service utilization among mother who gave birth in last two years, Arbaminch town, GamoGofa zone, Snnpr, Ethiopia. Science Journal of Public Health. 2016;4(6):458–62. https://doi.org/10.11648/j.sjph.20160406.17.
Shehu CE, Ibrahim MTO, Oche MO, Nwobodo EI. Determinants of place of delivery: a comparison between an urban and a rural community in Nigeria. Journal of Public Health and Epidemiology. 2016;8(6):91–101. https://doi.org/10.5897/JPHE2016.0817.
Kpenpuun JR. Influence of religious beliefs on healthcare practice. International Journal of Education and Research. 2014;2(4):37–48.
Maternal and Child Health Integrated Program. Factors Affecting Delivery Location in Indonesia. Gillings School of Global Public Health, University of North Carolina 2011.
Bidhan KS, Musfikur R, Tawhidur R, Jahangir H, Laura R, Dipak KM. Reasons for preference of home delivery with traditional birth attendants (TBAs) in rural Bangladesh: a qualitative exploration. PLoS One. 2016;11(1):1–19. https://doi.org/10.1371/journal.pone.0146161.
Cephas S, Karlijn M, Davidson HH, Robert AC. Reasons for home delivery and use of traditional birth attendants in rural Zambia: a qualitative study. BMC Pregnancy and Childbirth. 2015;15(216). https://doi.org/10.1186/s12884-015-0652-7.
Bidhan KS, Musfikur R, Tawhidur R, Jahangir H, Laura R, Dipak KM. Reasons for preference of home delivery with traditional birth attendants (TBAs) in rural Bangladesh: a qualitative exploration. PLoS One. 2016;11(1). https://doi.org/10.1371/journal.pone.0146161.
Solomon W, Ashenaf D, Kedir E, Melba CP, Kidisti T, Almaz B, Tsige A, et al. Late antenatal care initiation: the case of public health centers in Ethiopia. BMC Research Notes. 2018;11(562). https://doi.org/10.1186/s13104-018-3653-6.
Gezahegn T, Deborah L, Catherine C, Agumasie S, Roger Smith. Delayed initiation of antenatal care and associated factors in Ethiopia: a systematic review and meta-analysis. Reprod Health 2017, 14(150). DOI https://doi.org/10.1186/s12978-017-0412-4.
World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience 2016, ISBN 978 92 4 154991 2.
World Health Organization. WHO Recommendations on Maternal Health: Guidelines Approved by the Who Guidelines Review Committee 2017, (WHO/MCA/17.10). Licence: CC BY-NC-SA 3.0 IGO.
Abubakar SU, Samuel BB. Determinants of institutional delivery in Yobe state, Nigeria. American Journal of Public Health Research. 2016;4(1):1–7. https://doi.org/10.12691/ajphr-4-1-1.
Roman TY, Sena BK. Assessment of factors affecting choice of delivery place among pregnant women in Jimma zone, south West Ethiopia: cross sectional study. Journal of Women’s Health Care. 2014;4(1). https://doi.org/10.4172/2167-0420.1000211.
Bola LS, Olusegun AO, Ambrose A, Samson OO. Religion as a social determinant of maternal health care service utilisation in Nigeria. Afr Popul Stud. 2015;29(2):1868–81.
Maryam A, Llewellyn JC, Hadiza G, Salome E, Joshua NO, Olusegun AA, Nadia AS. Evaluating religious influences on the utilization of maternal health services among Muslim and Christian women in north-Central Nigeria. Hindawi Publishing Corporation BioMed Research International. 2016. https://doi.org/10.1155/2016/3645415.
Gillian H, Carol B, Mary F, Lisa B, Tina L. Factors influencing choice in birth place; an exploration of the views of women, their partners and professionals. Evidence Based Midwifery 2008.
Kwamena SD, Kenneth SA, Hubert A. What influences where they give birth? Determinants of place of delivery among women in rural Ghana. International Journal of Reproductive Medicine 2016, Hindawi Publishing Corporation https://doi.org/10.1155/2016/7203980.
Idris SH, Gwarzo UMD, Shehu AU. Determinants of place of delivery among women in a semi-urban settlement in Zaria, northern Nigeria. Annals of African Medicine. 2006;5(2):68–72.
Shahabuddin ASM, Vincent DB, Ramesh A, Alexandre D, Azucena B, Therese D. Determinants of institutional delivery among young married women in Nepal: evidence from the Nepal demographic and health survey 2011. BMJ Open. 2017. https://doi.org/10.1136/bmjopen-2016-012446.
Aggarwal R, Thind A. Effect of maternal education on choice of location for delivery among Indian women. National Journal of Medicine India. 2011;24(6):328–34 Available at: https://www.ncbi.nlm.nih.gov/pubmed/22680256.
Emily BZ, Steven HW, Amber H. Understanding the relationship between education and health. In: Agency for Healthcare Research and Quality 2015. Available at: https://www.ahrq.gov/professionals/education/curriculum-tools/population-health/zimmerman.html.
Sonia B, Damian C. Maternal Education and Maternal Mortality: Evidence from a Large Panel and Various Natural Experiments. 2013.
Ishaku AB, Eje DU, Livinus E. Utilization of antenatal and delivery services: a cross sectional survey of mothers in Makurdi, Benue state, Nigeria. Journal of Family Medicine & Community Health. 2017;4(2).
Michael B, Abraham BM, Emmanuel AA. They receive antenatal care in health facilities, yet do not deliver there: predictors of health facility delivery by women in rural Ghana. BMC Pregnancy and Childbirth. 2018;18(125):1–10. https://doi.org/10.1186/s12884-018-1749-6.
Irene TO. The role of antenatal Care in Predicting Health Facility Delivery among women in Kenya: further analysis of data from the 2008–09 KDHS. DHS WORKING PAPERS 2013, 86.
World Health Organization. Highlights and key messages from the World Health Organization’s 2016 global recommendations for routine antenatal care. WHO recommendations on antenatal Care for a Positive Pregnancy Experience 2018, Available at: https://apps.who.int/iris/bitstream/handle/10665/259947/WHO-RHR-18.02-eng.pdf?sequence=1.
Tesfaye G, Desta G, Kelali T, Brhane H, Mesfin A, Worku T, et al. Magnitude and predictors of skilled delivery service utilization: A health facility-based, cross-sectional study in Tigray. The Ethiopian Journal of Health Development 2014, 28. SSN 1021–6790.
Yohannes MA, Netsanet AA, Yimenu MA. Why do some Ethiopian women give birth at home after receiving antenatal care? Phenomenological study. HindawiBioMed Research International 2018, https://doi.org/10.1155/2018/3249786
John K, Sarah L, Gail D. Factors influencing place of delivery for women in Kenya: an analysis of the Kenya demographic and health survey, 2008/2009. BMC Pregnancy and Childbirth. 2013;13(40) http://www.biomedcentral.com/1471-2393/13/40.
Acknowledgements
The authors would like to thank the mothers who participated in this study for sharing their time and experience.
Funding
Not Applicable.
Author information
Authors and Affiliations
Contributions
AZ, DA, TK and YA conceived the idea and all the authors participated in the design of the research. AZ, DA, TK and YA collected the data. NG analyzed the data and wrote the manuscript. All authors reviewed, refined, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Research and Ethical Clearance Committee of the Asmara College of Health Sciences. After explaining the aim of the study, a written informed consent was taken from individual participants and only volunteered mothers were included in the study. Participants had the right to quit from the study at anytime during the interview. Confidentiality of data collected was maintained as no name or personal identifying information was collected in the course of the study.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Gebregziabher, N.K., Zeray, A.Y., Abtew, Y.T. et al. Factors determining choice of place of delivery: analytical cross-sectional study of mothers in Akordet town, Eritrea. BMC Public Health 19, 924 (2019). https://doi.org/10.1186/s12889-019-7253-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-7253-8