
Abstract
Background
Little is known about longitudinal associations of exercise with different types of cancer, particularly in Asian populations. The purpose of this research was to estimate the association between the duration of exercise and all-cause and cancer-specific mortality.
Method
Data were obtained from the Korean Metabolic Syndrome Mortality Study (KMSMS), a prospective cohort study of 303,428 Korean adults aged 20 years or older at baseline between 1994 and 2004 after exclusion of individuals with missing variables on smoking and exercise. Death certificate-linked data until 31 December 2015 were provided by the Korean National Statistical Office. Cox regression models were constructed to evaluate the associations of exercise with cancer mortality after adjusting for potential confounders such as age, alcohol consumption and smoking status.
Results
During the follow-up period of 15.3 years (4,638,863 person-years), a total of 16,884 participants died. Both men and women who exercised showed approximately 30% decreased hazards of mortality, compared to those who did no exercise (hazard ratio (HR) 0.70, 95% confidence interval (CI)=0.68-0.73 for men, HR=0.71, CI : 0.67-0.75). A notable observation of this study is the curvilinear associations between the total duration of exercise per week and cancer mortality, with the lowest risk being observed at the low-to-medium levels of exercise; this trend of associations was found for esophagus, liver, lung, and colorectal cancer mortality in men, and all-cause, all-cancer and lung cancer mortality in women.
Conclusions
Individuals who exercised showed considerably lower all-cause and cancer mortality risks compared with those who did no exercise. Policies and clinical trials aimed at promoting minimal or moderate participation in exercise may minimize cancer mortality risk.
Similar content being viewed by others

Background
Cancer is one of the leading causes of death worldwide. Globally, cancer accounts for approximately 8.2 million deaths in 2012, with more than 14 million new cancers diagnosed. [1]. In Korea, 180,530 deaths are predicted for all cancers excluding non-melanoma skin cancer in 2035, with more than 375,250 new cancers diagnosed [1].
According to expert review by Anand et al, up to almost 95% of cancer events are attributable to lifestyle factors such as physical inactivity, cigarette smoking, poor diet, alcohol, and obesity, and thus are potentially preventable [2]. Physical activity is defined as any bodily movement produced by skeletal muscles that results in energy expenditure, while exercise is a subcategory of physical activity, which is defined as a planned, repetitive, and purposive in the sense that improvement or maintenance of one or more components of physical fitness is an objective [3].
Association between exercise duration and cancer mortality was introduced by previous studies. According to large meta-analysis conducted by Li et al, high level of physical activity lowered the risk of cancer mortality in the general population and cancer survivors compared to inactivity, specifically individuals underwent the highest levels of physical activity had a 17% reduction in cancer mortality [4].
Convincing evidence indicates that regular participation in exercise is associated with reduced risk of mortality [5, 6], a recent meta-analysis study found regular physical activity to be protective against a wide variety of types of cancer incidence, using data pooled from 12 large prospective cohort studies comprising over 1.4 million people (with nearly 190,000 cases of cancer) from the United States and Europe [7].
A few other cohort studies [8,9,10,11,12] have also demonstrated inverse associations between physical activity and cancer risk, but all prior research have used data of individuals from Western countries.
Moon et al have reported that Asians have a lower body mass index (BMI) but higher percentage body fat than whites, and have a different fat distribution from whites [13]. Wang et al. reported that Asians had more upper body subcutaneous fat than did whites [14]. Therefore, increased health risks associated with obesity appear to occur at a lower BMI in Asians. In the context of physical activity, relatively low levels of leisure time physical activity and exercise among South Asian people were reported [15]. Nonetheless, a few previous studies investigating physical activity in relation to cancer in Asian populations were either cross-sectional or had low statistical power due to the small sample size [16,17,18,19]. Therefore, the purpose of this research was to examine the associations of exercise per week with all-cause and cancer-specific mortality using data from a large-scale prospective cohort study of Koreans.
Methods
Study population
Data were obtained from the Korean Metabolic Syndrome Mortality Study (KMSMS), a prospective cohort study of 560,543 Korean adults aged 20 years or older at baseline between 1994 and 2004 [19]. After the exclusion of individuals with missing variables on smoking and exercise, a final sample of 303,428 participants were included in the present analysis (171,594 men and 131,834 women).
Data collection
Demographic information, smoking status (never, past, or current), and a medical history of comorbidities including atherosclerotic cardiovascular disease and cancer were assessed by written questionnaires. Information on exercise was obtained by asking “Do you exercise regularly?” (Yes/No) If participants answered “Yes,” they were asked to indicate the frequency of exercise per week in on a continuous scale, which we then categorized into 4 comparison groups (0, 1-2 times, 3-4 times, or ≥5 times per week). The next question asked about average hours and minutes spent per exercise session. We multiplied the exercise frequency per week by the average time spent per exercise session (hours and minutes) to obtain the total duration (i.e. overall volume) of exercise per week (<100, 100-249, 250-399, ≥400 minutes/week). We suggested the type of exercise to the participants; jogging, freehand exercise, walk, hiking, fitness, yoga, swimming, aerobics, golf, jump rope, etc.
Weight and height measurements were taken while participants were wearing light clothing. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters.
Mortality follow-up
Death certificate-linked data until 31 December 2015 were provided by the Korean National Statistical Office. Mortality outcomes were ascertained from the causes of death listed on death certificates. A computerized search of death certificate data from the National Statistical Office in Korea was performed, using unique identification numbers assigned at birth. Cancer mortality was defined as any deaths due to cancer using the primary cause of death based on the International Classification of Diseases Tenth Revision codes C00-C97; codes used to classify specific types of cancer mortality are provided in the Additional file 1: Table S1.
Statistical analysis
Descriptive analyses were performed to summarize the means and standard deviations for continuous variables and percentages for categorical variables in men and women separately. Age-standardized cause-specific mortality rates were calculated across these categories using the Korean Population and Housing Census data in 2010 as a standard population.
Cox regression models were used to estimate the association between exercise duration and cancer with adjustment for potential confounders (age, alcohol intake [yes/no], and smoking status [non-smoker, ex-smoker, current smoker]). Proportional assumption was tested by using Schoenfeld residuals. The survival curve according to exercise level was plotted using the life-table method. To calculate attributable fractions of non-exercise for mortality, individuals who reported that they exercised served as the reference group. All analyses were performed using SAS version 9.4. All statistical tests were two-sided, and statistical significance was determined at an alpha level of 5%.
Results
The average (standard deviation) age of KMSMS subjects was 46.0 (10.6) years in men and 46.2 (11.3) years in women. Table 1 shows characteristics of the study participants by exercise categories. Compared to those who did not exercise, those who exercised were more likely to have higher age, BMI, and drinking rates or lower smoking rates.
During the follow-up period of 15.3 years (4,638,863 person years), a total of 16,884 (11,919 men and 4,965 among women) participants died, providing sufficient statistical power to examine the association between exercise and cancer mortality. Table 2 shows age adjusted mortality rates and hazard ratios (HR) of all-cause, cancers, and cancer types by exercise status in men. Men who exercised had lower all-cause and all-cancer mortliaty rates per 100,000 person-years compared with those who did not exericse. Compared with men who did no exercise, those who exercised showed 0.70 (95% confidence interval [CI]: 0.68-0.73) and 0.77 (95% CI: 0.73-0.81) times lower hazards of all-cause and all-cancer mortality, respectively. In addition, men who exercised showed lower hazards of esophageal (HR=0.67; 95% CI: 0.47-0.97, liver (HR=0.83 95% CI: 0.74-0.94), lung (HR=0.71 95% CI: 0.64-0.79), colorectal (HR=0.65 95% CI: 0.53-0.80), and stomach cancer (HR=0.62 95% CI: 0.53-0.73) than those who did not exercise. When men who exercised were set as the reference, those who did no exercise showed 1.42 (95% CI: 1.37-1.48) times higher risk of mortality. Non-exercise prevalence was found to be 53.7%, while attributable fractions of non-exercise for all-cause and all-cancer mortality were 18.4% and 13.9%, respectively.
In addition, Table 2 shows associations between the total duration of exercise per week and mortality from all causes, cancer, and specific types of cancer in men. Regarding all-cause mortality, the exercise group showed lower rates (HR=0.69 for <150 minutes per week; HR=0.67 for 150-299 minutes per week; HR=0.67 for ≥300 minutes per week) than the non-exercise group. Analyses for all-cancer mortality showed similar rates of HR=0.74 (<150 minutes per week), HR=0.78 (150-299 minutes per week), and HR=0.73 (≥300 minutes per week).
Table 3 presents age-adjusted mortality rates and hazard ratios (HR) of all-cause, cancers, and cancer types by exercise status in women. Likewise, women who exercised had lower all-cause and all-cancer mortliaty rates per 100,000 person-years compared with those who did not exericse. Table 3 also shows associations between the total duration of exercise per week and mortality from all causes, cancer, and specific types of cancer in women. Regarding all-cause mortality, the exercise group showed lower rates (HR=0.73 for <150 minutes per week; HR=0.65 for 150-299 minutes per week; HR=0.69 for ≥300 minutes per week) than the non-exercise group.
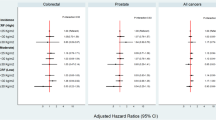
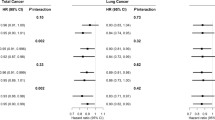
Table 4 shows associations between the total duration of exercise per week with different categories and mortality from all causes and all cancers in men and women. We found that those who did at least 100 minutes per week showed significant reduction and reduced until less than 400 minutes per week in men and women. In other words, the largest reduction in all cause and all cancer mortality risk was observed in the minimal or middle levels of duration of exercise per week rather than in the highest categories, providing J-shaped associations. In general, the intermediate levels of exercise duration (i.e. categories of 100-249min and 250-399min) showed the lowest (statistically significant) HR values for all-cause, all-cancer, and lung; the HRs in the highest duration category were slightly higher (although not significantly for all causes and all cancer (Fig. 1).

Hazard ratios and 95% group specific confidence intervals of all causes and all cancer mortality, the Korean Metabolic Syndrome Mortality Study
Discussion
To the best of our knowledge, this study is the first investigation examining the longitudinal associations of exercise with various cancer mortality outcomes in Asian adult populations. We found that over 15.3-year follow-up (4,638,863 person-years; 16,884 deaths) both men and women who exercised showed over 20% decreased hazards of all-cause and all-cancer mortality, respectively, compared to those who did no exercise. A notable observation of this study is the curvilinear associations between the total duration of exercise and cancer including all-cause, all-cancer, esophagus, lung, colorectal, and stomach cancer in men and all cause, all cancer and lung cancer in women. This finding specifically indicates that risk of cancer mortality was not lowest in the highest level of exercise, but in the minimal or intermediate level of exercise, suggesting that public and clinical efforts may not necessarily need to focus on encouraging people to participate in maximal levels of exercise in order to minimize cancer risk. Since our study merely analyzed the association in exercise, further study is required in order to examine whether the similar J-shape appears in the moderate type of physical activity like active walking, commuting activity, and household chores.
A recent systematic review showed the continuous does-response relations between physical activity and cancer including 35 articles for breast cancer and 19 for colon cancer from the study on Global Ageing and Adult health conducted in China, Ghana, India, Mexico, Russia, and South Africa and US National Health and Nutrition Examination Surveys [20]. People who achieve total physical activity levels several times higher than 150 minutes of moderate-to-vigorous physical activity per week as recommended by World Health Organization [6, 21] showed a significant reduction in the risk of cancers studied [17]. Our results showed that individuals who accumulated 150 minutes of exercise per week had substantially lower risks of cancer mortality (i.e. HR=0.70 for all-cause death, HR=0.74 for all-cancer death). Another review study [22] synthesized and summarized evidence from 32 epidemiologic studies that evaluated exercise-cancer mortality associations in cancer patients, and showed significantly lower risks of cancer-specific mortality in cancer patients with higher exercise levels [22]. However, cautious interpretation is required in comparing the results from previously reported study due to the difference in definition between exercise and smoking. Physical activity is defined as any bodily movement produced by skeletal muscles that results in energy expenditure, while exercise is a subcategory of physical activity, which is defined as a planned, repetitive, and purposive in the sense that improvement or maintenance of one or more components of physical fitness is an objective [3].
In contrast to the previous study [20], the present study found J-curve associations, showing maximal levels of engagement in exercise were not associated with lowest levels of cancer risk. Additional research using more rigorous methodologies (e.g., repeated measures, objectively measured exercise information) is required to further explore the true associations between exercise and cancer in Asian populations.
The results of our study regarding breast, colorectal and prostate cancer were somewhat different with the results previously reported studies. In our study, breast cancer mortality between women who exercised, compared to those who did not exercise was not statistically significant 1.06 (0.75–1.50). Also, prostate cancer risk among men was not statistically significant (0.62, 0.32-1.50). However, both men and women showed decreased mortality among those who exercised for equal or more than 100 minutes per week. However, while previously reported studies were focusing on breast cancer, prostate cancer, colorectal cancer and other types of cancer, our study examined the association between exercise and cancer mortality on esophagus, lung, colorectal, and stomach cancer, thereby direct comparison between such studies are limited.
Results in our study generally demonstrated reducing cancer mortality for exercise for the above listed cancers. One thing was clear: 400-minute increase in exercise per week was not consistently associated with decreased mortality risk (Table 4).
A recent epidemiological study on exercise and all cause and cardiovascular disease mortality showed similar results as the present study in terms of identifying J-shaped associations [5, 23]. For example, the largest reduction in the risk of cancer mortality was observed in the middle categories of various running behaviors. As such, a seminal study also provided evidence on extremely high levels of exercise may not provide additional benefits for cardiovascular disease prevention [24]. However, no attention has been paid to disentangling the right amount of exercise for prevention of various types of cancer outcomes, in particular in Asian populations. In the present study using a large-scale prospective cohort of Korean adults, we provided convincing evidence for the first time that engaging in considerably high levels of exercise may not be associated with maximal reductions in risk of various cancer mortality outcomes. More research is clearly needed to confirm the J-shaped associations of various exercise indicators (including physical activity indicators) with each specific cancer outcome in Asian as well as Western populations.
To date, the mechanisms through which greater exercise levels lead to reduced risks of developing different types of cancer have been largely unknown. However, evidence suggests that engaging in exercise can cause favorable changes on body composition, sex hormone levels, systemic inflammation, and immune cell functions, all of which are important predictors of cancer [25]. Several previous studies have been proposed that may explain the mechanisms of reduction in cancer incidence or mortality by exercise [25, 26]. Natural killer cells are the most responsive immune cells to exercise, displaying an acute mobilization to circulation during physical exertion. In general, maximal mobilization of the Natural killer cells is achieved within 30 minutes of endurance training, after which continued exercise does not lead to further increase in Natural killer cell numbers [27].
There are several limitations. Information on exercise was obtained using a self-report method, so there may be measurement errors in the quantification of exercise levels due to recall bias and social desirability [28]. Self-reported activity data are deemed less accurate than objectively measured activity data using accelerometry [29]. However, contemporary accelerometers cannot distinguish exercise from physical activity although they can capture activity intensities. Hence, using self-reports in research (including the present analysis) to assess exercise as opposed to physical activity appears an inevitable, effective methodology. Another limitation is the use of data only from baseline. It is highly likely that individuals’ exercise levels and patterns change over time, but the present study was not able to take into account the variation in exercise in the analyses. Participants were recruited without employing any sampling strategy aimed at collecting a representative sample of adults. Hence, results from the present study may not be generalizable to the whole Korean adult population and adults from other countries. Also the participatns in our study had exercise and smoking data. Although physical activity involves various kinds of domain of physical activity and sedentary behavior which should be included in models to estimate mortality risk, our study only provided information on exercise. Among those who said that they had exercise, those who did not have information of the total duration of exercise per week was approximately 21%, and this might be regarded as an another limitation of our study. Our study also need to be interptreted carefully since those who exercise tend to be more interested in health, and as they are more likely to participate in health screening, they can lead to early detection of disease.
Especially, the longer the exercise period, the more pronounced this trend is. However, studies that have closely examined this mechanism are rare and need to be discussed in further studies.
Conclusions
In conclusion, our study using a sample of over 300,000 Korean adults over 15 years of follow-up demonstrated that individuals who exercised showed considerably lower all-cause and cancer mortality risks than those who did no exercise. However, the associations of weekly exercise or duration with cancer mortality were J-shaped: all-cause and all-cancer death rates in both men and women with 400-minute increase in exercise per week. This observation indicates that risk of cancer mortality was lowest when participating in minimal or moderate levels of exercise, not in the highest level of exercise. Clinical trials and public health policies aimed at reducing cancer risk should encourage individuals to engage in exercise. However, cancer mortality risk may be minimized when such efforts are targeted for sedentary or physically inactive individuals to perform minimal or moderate levels of exercise.
Abbreviations
- BMI:
-
body mass index
- CI:
-
confidence interval
- HR:
-
hazard ratios
- KMSMS:
-
Korean Metabolic Syndrome Mortality Study
References
WHO. Global Health Observatory, NCD mortality and morbidity 2012. 2016. Available at: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx accessed online on February 2018
Anand P, Kunnumakkara AB, Sundaram C, Harikumar KB, Tharakan ST, Lai OS, et al. Cancer is a preventable disease that requires major lifestyle changes. Pharm Res. 2008;(9):2097–116. https://doi.org/10.1007/s11095-008-9661-9. Epub 2008 Jul 15. Review. Erratum in: Pharm Res. 2008 Sep;25(9):2200. Kunnumakara, Ajaikumar B [corrected to Kunnumakkara, Ajaikumar B]
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–31.
Li T, Wei S, Shi Y, Pang S, Qin Q, Yin J, et al. The dose–response effect of physical activity on cancer mortality: findings from 71 prospective cohort studies. Br J Sports Med. 2016;50(6):339–45.
Lee DC, Pate RR, Lavie CJ, Sui X, Church TS, Blair SN. Leisure-time running reduces all-cause and cardiovascular mortality risk. J Am Coll Cardiol. 2014(5):472-481. doi: https://doi.org/10.1016/j.jacc.2014.04.058. Erratum in: J Am Coll Cardiol. 2014;64(14):1537.
Liss MA, White M, Natarajan L, Parsons JK. Exercise Decreases and Smoking Increases Bladder Cancer Mortality. Clin Genitourin Cancer. 2017;3:391–5.
Moore SC, Lee IM, Weiderpass E, Campbell PT, Sampson JN, Kitahara CM, et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1. 44 Million Adults. JAMA Intern Med. 2016;176(6):816–25.
Arem H, Matthews CE, Lee IM. Physical Activity Is Key for Successful Aging-Reply: Even a Little Is Good. JAMA Intern Med. 2015;175(11):1863.
Arem H, Moore SC, Patel A, Hartge P, Berrington de Gonzalez A, et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA Intern Med. 2015;175(6):959–67.
Lee IM, Manson JE, Ajani U, Paffenbarger RS Jr, Hennekens CH, Buring JE. Physical activity and risk of colon cancer: the Physicians’ Health Study (United States). Cancer Causes Control. 1997;8(4):568–74.
Hildebrand JS, Gapstur SM, Campbell PT, Gaudet MM, Patel AV. Recreational physical activity and leisure-time sitting in relation to postmenopausal breast cancer risk. Cancer Epidemiol Biomarkers Prev. 2013;22(10):1906–12.
Sinner P, Folsom AR, Harnack L, Eberly LE, Schmitz KH. The association of physical activity with lung cancer incidence in a cohort of older women: the IowaWomen’s Health Study. Cancer Epidemiol Biomarkers Prev. 2006;15(12):2359–63.
Moon OR, Kim NS, Jang SM, Yoon TH, Kim SO. The relationship between body mass index and the prevalence of obesity related diseases based on the 1995 National Health Interview Survey in Korea. Obes Rev. 2002:191–6.
Wang J, Thornton JC, Russell M, Burastero S, Heymsfield S, Pierson RN Jr. Asians have lower body mass index (BMI) but higher percent body fat than do whites: comparisons of anthropometric measurements. Am J Clin Nutr. 1994;60(1):23–8.
Williams ED, Stamatakis E, Chandola T, Hamer M. Assessment of physical activity levels in South Asians in the UK: findings from the Health Survey for England. J Epidemiol Community Health. 2011;6:517–21.
Kang SJ. The association of physical activity and colorectal and breast cancer: The Fifth Korea National Health and Nutrition Examination Survey (2008-2011). J Exerc Rehabil. 2015;11(3):155–60.
Chung JY, Lee DH, Park JH, Lee MK, Kang DW, Min J, et al. Patterns of physical activity participation across the cancer trajectory in colorectal cancer survivors. Support Care Cancer. 2013;21(6):1605–12.
Park J, Kim JH, Lee HJ, Park SJ, Hong SP, Cheon JH, et al. The Effects of Physical Activity and Body Fat Mass on Colorectal Polyp Recurrence in Patients with Previous Colorectal Cancer. Cancer Prev Res (Phila). 2017;10(8):478–84.
Mok Y, Jeon C, Lee GJ, Jee SH. Physical Activity Level and Colorectal Cancer Mortality. Asia Pac J Public Health. 2016;28(7):638–47.
Kyu HH, Bachman VF, Alexander LT, Mumford JE, Afshin A, Estep K, et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ. 2016;9:354–i3857.
World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. http://www.who.int/chp/steps/resources/GPAQ_Analysis_Guide.pdf.
Cormie P, Zopf EM, Zhang X, Schmitz KH. The Impact of Exercise on Cancer Mortality, Recurrence, and Treatment-Related Adverse Effects. Epidemiol Rev. 2017;39(1):71–92.
Vainshelboim B, Müller J, Lima RM, Nead KT, Chester C, Chan K, Kokkinos P, Myers J. Cardiorespiratory fitness, physical activity and cancer mortality in men. Prev Med. 2017;100:89–94.
Eijsvogels TM, Molossi S, Lee DC, Emery MS, Thompson PD. Exercise at the extremes: the amount of exercise to reduce cardiovascular events. JACC. 2016;67(3):316–29.
Idorn M, Thor Straten P. Exercise and cancer: from "healthy" to "therapeutic"? Cancer Immunol Immunother. 2017;66(5):667–71.
Pedersen L, Idorn M, Olofsson GH, Lauenborg B, Nookaew I, Hansen RH, et al. Voluntary Running Suppresses Tumor Growth through Epinephrine- and IL-6-Dependent NK Cell Mobilization and Redistribution. Cell Metab. 2016;23(3):554–62.
Timmons BW, Cieslak T. Human natural killer cell subsets and acute exercise: a brief review. Exerc Immunol Rev. 2008;14:8–23.
Mâsse LC, Watts AW. Stimulating innovations in the measurement of parenting constructs. Child Obes. 2013 Aug;9(Suppl):S5–13. https://doi.org/10.1089/chi.2013.0041.
Firth J, Stubbs B, Vancampfort D, Schuch FB, Rosenbaum S, Ward PB, Firth JA, Sarris J, Yung AR. The Validity and Value of Self-reported Physical Activity and Accelerometry in People With Schizophrenia: A Population-Scale Study of the UK Biobank. Schizophr Bull. 2017. https://doi.org/10.1093/schbul/sbx149. [Epub ahead of print]
Acknowledgment
We thank the staff of the Korean Statistical Office.
Funding
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (1631020). This study was a research project funded by the Ministry of Health and Welfare and was supported for data collection.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
YJ performed the statistical analysis, arranged ethical approvals, prepared figures and drafted the manuscript; YK provide statistical analysis advice, commented on the manuscript and figures; SJ and MR conceived the study, helped with data management and helped to finalize the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Because the study involved routinely collected medical data, participant consent was not specifically obtained. The study was approved by the institutional review boards of Yonsei University.
Competing interests
The authors declare that we have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. List of cancers included in the study based on the International Classification of Diseases Tenth Revision codes. (DOCX 16 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Jee, Y., Kim, Y., Jee, S. et al. Exercise and cancer mortality in Korean men and women: a prospective cohort study. BMC Public Health 18, 761 (2018). https://doi.org/10.1186/s12889-018-5669-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-018-5669-1