
Abstract
Background
The Qatar Biobank aims to collect extensive lifestyle, clinical, and biological information from up to 60,000 men and women Qatari nationals and long-term residents (individuals living in the country for ≥15 years) aged ≥18 years (approximately one-fifth of all Qatari citizens), to follow up these same individuals over the long term to record any subsequent disease, and hence to study the causes and progression of disease, and disease burden, in the Qatari population.
Methods
Between the 11th-December-2012 and 20th-February-2014, 1209 participants were recruited into the pilot study of the Qatar Biobank. At recruitment, extensive phenotype information was collected from each participant, including information/measurements of socio-demographic factors, prevalent health conditions, diet, lifestyle, anthropometry, body composition, bone health, cognitive function, grip strength, retinal imaging, total body dual energy X-ray absorptiometry, and measurements of cardiovascular and respiratory function. Blood, urine, and saliva were collected and stored for future research use. A panel of 66 clinical biomarkers was routinely measured on fresh blood samples in all participants. Rates of recruitment are to be progressively increased in the coming period and the recruitment base widened to achieve a cohort of consented individuals broadly representative of the eligible Qatari population. In addition, it is planned to add additional measures in sub-samples of the cohort, including Magnetic Resonance Imaging (MRI) of the brain, heart and abdomen.
Results
The mean time for collection of the extensive phenotypic information and biological samples from each participant at the baseline recruitment visit was 179 min. The 1209 pilot study participants (506 men and 703 women) were aged between 28–80 years (median 39 years); 899 (74.4 %) were Qatari nationals and 310 (25.6 %) were long-term residents. Approximately two-thirds of pilot participants were educated to graduate level or above.
Conclusions
The pilot has proven that recruitment of volunteers into the Qatar Biobank project with intensive baseline measurements of behavioural, physical, and clinical characteristics is well accepted and logistically feasible. Qatar Biobank will provide a powerful resource to investigate the major determinants of ill-health and well-being in Qatar, providing valuable insights into the current and future public health burden that faces the country.
Similar content being viewed by others


Background
Over the past 50 years Qatar has experienced major economic growth and demographic and socio-economic changes. During this time the population of the country has risen rapidly, from 369,079 in 1986 [1], to over 2.4 million in 2015 (1.9 million aged over 15 years) [2] - most of this increase was driven by an influx of economic migrants, and there are estimated to be 300,000 Qatari nationals (~14 % of the total population). The population has experienced a major shift in diet with increasing availability of western type foods, and consequent increasing consumption of fat rich foods, meat and meat products, refined sugar, and industrially processed foods. In addition, similar to other high income countries, food has become relatively inexpensive compared to the average purchasing power. In parallel, changes in the economic, industrial, and urban landscape have led to a substantial reduction in physical activity, mirroring what has happened over the past decades in most of the economically developed world [3]. In this societal context, obesity has become increasingly prevalent in Qatar as it has in many countries around the world [4]. The 2012 national STEPwise survey reported that approximately 70 % of the population is overweight or obese (body mass index (BMI) ≥25 kg/m2) [3]. Obesity related comorbidities are now as common in Qatar as in most neighbouring countries, with the 2012 national STEPwise survey reporting high prevalence of hypertension (32.9 % of respondents ages 18-64) and diabetes (17.6 % of men and 15.9 % of women) [3]. As a comparison, the prevalence of hypertension across the UK adult population age 20–59 is around 15.0 % [5] and the prevalence of diabetes at all ages is 6.0 % [6]. Overall, in Qatar, chronic diseases such as cardiovascular diseases, diabetes, and cancer were estimated to account for 69 % of all deaths in 2008 [7].
Chronic diseases are caused by the complex interplay between environmental factors (such as diet, lifestyle, and the built environment) and genetic predisposition. To understand the aetiological role of environmental, behavioural, and genetic factors and their interactions, large-scale population cohorts have been established, mainly in Europe, North America, China, Japan, and Korea [8–16]. No such large population based studies currently exist in the Gulf Region. The Qatar Biobank was set up by the Qatar Foundation and the Supreme Council of Health in collaboration with Imperial College London, as the first Qatar national population based prospective cohort study, and includes the collection of biological samples, with long-term storage of data and samples for future research (biobank). Up to 60,000 men and women Qatari nationals and long-term residents (defined as individuals living in Qatar for 15 years and over) will be recruited into the cohort over the coming years, with extensive baseline clinical, metabolic and behavioural phenotypic data, and blood, urine, and saliva samples collected and stored. The Qatar Biobank will thus provide a powerful resource to investigate the role of environmental factors, lifestyle factors, genetics and their interactions in subsequent disease occurrence. As well as studying the causes of diseases, the Qatar Biobank will also provide insights into the current and future public health burden that faces the country.
Here we describe the design and methods of the Qatar Biobank study. The questionnaires, clinical measurements, biological sampling protocols and Standard Operating Procedures (SOPs) were developed during pre-plot testing and a pilot study, and we also provide here demographic and clinical referral information for the 1209 pilot study participants.
Methods
The Qatar Biobank involves collection of extensive questionnaire information, clinical phenotyping and biological samples from Qatari nationals and long-term residents (≥15 years living in Qatar) aged 18 or more years, who comprise the eligible population. A computerised clinic based system was developed for the pilot study to facilitate data collection, tracking of the participant data (and linked samples) throughout the visit and digital download from the clinical devices to minimise manual data entry. A summary of the data collected in the pilot study and for the full study (including follow-up) is shown in Fig. 1.

A summary of the data collected in the Qatar Biobank pilot and full study (including follow-up)
Recruitment into the pilot study
For the full study, it is intended that participants will be broadly representative of the eligible Qatari population. However, for the pilot study, recruitment focused initially on selected occupational groups and word of mouth to provide a ready means to test the study protocols and SOPs. Recruitment to the pilot was initiated on the 11th December 2012 and we report on data collected to 20th February 2014.
For the pilot study, initially potential participants were contacted via a small number of public and private employers by setting up information booths at their workplace. Subsequently, most participants were recruited by personal recommendations of friends and family. At baseline, participants were invited to a visit at the Qatar Biobank facility at Hamad Medical City where they underwent a 5-stage interview and physical and clinic measurement sequence, with an average duration of 179 min (Fig. 2; Table 1). All participants gave informed consent. Institutional Review Board approval was obtained from the Hamad Medical Corporation Ethics Committee.

Summary of the Qatar Biobank pilot study baseline visit
Self-completed health and lifestyle questionnaire
The design of the Qatar Biobank health and lifestyle questionnaire was informed by pre-pilot testing phases among Qatari volunteers, who provided information about the feasibility and acceptability of different versions of the questionnaire. The computer administered health and lifestyle section of the questionnaire contains detailed questions on socio-demographic factors, current and past health, family history of health conditions, current and past smoking habits (cigarettes and water pipe or shisha), occupational information, mobile phone use, physical activity levels, sleeping patterns, reproductive health (women), and cognitive and psychological state. Collection of information on cultural and lifestyle characteristics of the Qatari population for the pilot study was based on adaptation of widely used and validated instruments including from the European Prospective Investigation into Cancer and Nutrition (EPIC) study (smoking history, female reproductive history) [9], UK Biobank (e.g. sleep pattern questions) [10, 11], COSMOS (mobile phone use) [17, 18], the Patient Health Questionnaire (PHQ-9) (depression) [19], and the shortened form of the International Physical Activity Questionnaire (IPAQ) [20], which was augmented by questions on inactivity. In response to pre-pilot testing feedback, the health and lifestyle questions presented on the computer screen were tailored to the participant’s age, gender, and marital status. Similarly, a question skip pattern was applied to conditional questions as appropriate (e.g. non-smokers were not asked smoking history questions) and various logic and consistency checks were built into the software to reduce error rates. A trained nurse was available for participant assistance upon request.
Dietary assessment
In the absence of an established questionnaire for assessment of diet in Qatar, the instrument used in Qatar Biobank was developed based on field assessment of the local food environment, focus groups, and consultation with local nutrition researchers. The computer-administered diet questionnaire assessed the intake of 96 food and beverage items, with either five or six frequency options depending on the nature of the item. The diet questionnaire also incorporated general questions on dietary habits, including reasons for recent dietary modification (if applicable), frequency of eating from a common plate, and snacking between meals. In order to assess the internal validity of the questionnaire, general questions on frequency of consuming broad categories of foods (chicken, meat, fish, fast and take-away foods, snacks, salads) were examined in relation to the sum of individual items within the broader categories (e.g. all fast food items), with Spearman’s rank correlations ranging from 0.30 (for sweet and savoury snacks) to 0.74 (for fish consumption).
Cognitive function tests
Computer based self-administered tests were completed to assess cognitive function, specifically a choice reaction time test and a paired episodic memory test [21].
Nurse administered interview questionnaire
In a face-to-face interview, administered by a trained nurse, participants were asked to report any previous or prevalent health conditions they or their family members may have suffered from; plus information on over-the-counter and prescription medication use and reproductive history (women only).
Physical and clinical measurements
Various physical measurements were collected from each participant. Anthropometric measurements comprised body weight, height (sitting and standing) using the Seca stadiometer, hip and waist circumferences as well as bioimpedance (Tanita). To assess muscle strength, grip strength was measured in the participants’ right and left hands using a hydraulic hand dynamometer (Jamar J00105) [22]. Participants had an electrocardiogram (ECG) using the Atria 6100 automated system [23]. Arterial stiffness was assessed by the VICORDER device [24]. For blood pressure, using the Omron 705 automated device [25], two diastolic and systolic blood pressure measurements were obtained, and if these differed by 5 mmHg or more, a third measurement was made. Respiratory function was assessed by spirometry using the Pneumotrac Vitalograph [26].
Several imaging technologies were used. These included: 3D carotid ultrasound to measure intima media thickness (IMT) and carotid plaques using a Philips ultrasound system and mechano‐transducer probe [27]; full body dual energy X-ray absorptiometry (iDXA; General Electric) scan to assess bone mineral density and body composition [28]; and “microscopic” features of the optic nerve and macula assessed by use of a Topcon TRC-NW6S retinal camera [29]. Cardiorespiratory fitness was tested by a graded treadmill test of 5 to 11 min duration (dependent on self-rated fitness) using the h/p/cosmos quasar device [30]. For the full study, magnetic resonance imaging (MRI) of the brain, heart and abdomen is planned among a sub-sample of participants.
Biological material collected
During the baseline recruitment visit, pilot participants provided samples of blood, saliva and urine. Approximately 60 ml of blood was collected from each participant. A proportion of the blood was used for the measurement of the 66 clinical biomarkers routinely measured (Table 2). Haematology and blood biochemistry were analysed by the laboratories of the Hamad Medical Centre Laboratory, Doha. The remainder, plus the urine and saliva, was subdivided into a number of aliquots, and then transferred into 2 dimensional barcode labelled microtubes for long-term cryogenic storage. A participant’s sample aliquots were split for storage in two separate locations—one for active use stored at −80 °C and one as a long-term backup (in liquid nitrogen vapour phase for the full study). The EDTA blood samples were centrifuged to separate blood into its constituent components, in the form of layers: plasma, buffy coat (leucocytes) and erythrocytes.
Results
Age of the 1209 participants recruited in the pilot study ranged between 25 and 80 years, with a median age of 39 years; 42 % were men, 58 % women (Fig. 3). The majority of participants were Qatari nationals (74 %) and 19 % were long-term residents of Arabic origin; the remaining 6 % were long-term residents of non-Arabic origin. Approximately two-thirds of men (67.6 %) and women (64.1 %) in the pilot study were educated to university graduate level and above (Table 3). Paid employee was the most common employment status for both men (74.5 %) and women (45.5 %).

Age distribution of men and women recruited into the Qatar Biobank pilot study (N = 1209, mean = 39.89 years, SD = 12.92; median = 39 years)
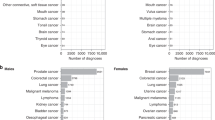
Clinical referrals were made for participants with out of range values of clinical data, based on review by a doctor or a nurse. During the pilot study, 520 of the 1209 participants (43 %) were clinically referred. Most of these referrals were made for diabetes related tests (N = 198 participants; 16.3 %), low forced expiratory volume in one second based on spirometry (predicted FEV1 less than 80 % based on the best spirometry attempt, N = 173; 14.3 %), and indications of poor bone health based on iDXA scan measurement of bone density and low vitamin D levels (N = 160; 13.2 %).
Discussion
The Qatar Biobank offers an unprecedented opportunity to study the causes and public health burden of diseases affecting the Qatari population which has undergone a major health transition over the past 50 years. It is collecting a broad range of phenotypic data. These include data from questionnaires, extensive clinical measurements and imaging, and biological samples (blood, urine, and saliva), which are being stored long-term, with consent, for future (unspecified) research use including for genetic studies. The pilot study was well accepted with high satisfaction levels reported by participants; 94 % (N = 1136) reported that if given the opportunity they would take part again. Following completion of the pilot, the study is now entering a phase of progressive increase in the number of participants attending the baseline visit, with recruitment widened to capture a sample designed to be as representative as possible of the eligible Qatari population, aiming for a total sample size of up to 60,000 individuals. A dedicated high-specification building has been assigned to the Qatar Biobank, including a clinic facility, laboratory, liquid nitrogen storage facility, offices for clinic and research staff, and an MRI suite. Data collection for the full study is planned over the next several years to achieve the projected sample size.
Already, the Qatar Biobank is having an impact on the health of participants due to the rigorous system of clinical referrals based on out of range values from the extensive clinical phenotypic information collected. Clinical measurements and biochemical data are fed back to participants by a doctor or nurse and clinical referrals (with consent) are made as necessary. Clinical referrals following face-to-face feedback of results to participants 3 to 6 weeks after their initial visit are an important and unique feature of the Qatar Biobank; such referrals have not been included in the protocol of most large-scale population based prospective studies. The feedback from study participants indicates that this process is highly valued. There was a high proportion of participants who were clinically referred in the pilot study, reflecting high prevalence of chronic conditions such as diabetes, low bone density and Vitamin D deficiency. The referral criteria for the extensive clinical phenotypic information collected are being further evaluated to optimise sensitivity and specificity of the referral procedure.
The Qatar Biobank will be a unique resource with large numbers of the eligible population enrolled. Additionally, the breadth and depth of phenotypic information and biological samples collected from participants is unparalleled by any other study in the Middle East and Asia. The imaging modules will be further augmented in the full study when a sub-sample of participants will undergo MRI scans of the brain, heart and abdomen. Again to our knowledge, such a comprehensive and state-of-the-art imaging protocol has not been implemented in large-scale population cohorts in the Middle East and Asia.
Participants will be followed up long-term through data linkage to clinical records (with consent) and occurrences of health related outcomes will be recorded. Furthermore, it is planned that participants will be re-contacted actively in the future for the collection of repeat phenotypic and medical condition information.
Conclusion
The Qatar Biobank is a major new prospective cohort study in the Gulf region, with extensive data collection and storage of biological samples and linkage to health records for follow up. This will provide unprecedented opportunity to study the future health and disease burden as they evolve over the coming years among the Qatari population.
Abbreviations
- BMI:
-
body mass index
- ECG:
-
electrocardiogram
- IMT:
-
intima media thickness
- iDXA:
-
dual energy X-ray absorptiometry
References
Qatar Information Exchange. Worksheet List [http://www.qix.gov.qa/discoverer/app/explorer?node=2&event=expand&state=%2826%29&root=0&partial=&source=expl&stateStr=eNolyEsKgDAMANHLxKz9gLvsvIfUNAVR0mJD1dtb6eoxA6yAhY1y8ch6EIfVDf0ALkE3zj5001I9G7mh3PT%2FBnnSCZgToUYvhFJEjTCbs1pXjDXuzWgEtjdB2eWW6wNOsST9&partialTargets=]. [accessed 23rd November 2015].
Ministry of Development Planning and Statistics. Monthly figures on total population in Qatar [http://www.mdps.gov.qa/portal/page/portal/gsdp_en/statistics_en/monthly_preliminary_figures_on_population_en]. [accessed 23rd November 2015].
Haj Bakri A, Al-Thani A. Chronic Disease Risk Factor Surveillance: Qatar STEPS Report 2012. Qatar: The Supreme Council of Health; 2013.
Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet. 2011;377:557–67.
Joffres M, Falaschetti E, Gillespie C, Robitaille C, Loustalot F, Poulter N, et al. Hypertension prevalence, awareness, treatment and control in national surveys from England, the USA and Canada, and correlation with stroke and ischaemic heart disease mortality: a cross-sectional study. BMJ Open. 2013;3:e003423.
Diabetes UK. Diabetes: Facts and Stats. 2014. [https://www.diabetes.org.uk/Documents/About%20Us/Statistics/Diabetes-key-stats-guidelines-April2014.pdf]. [accessed 23rd November 2015].
World Health Organization. Qatar - NCD Country Profile. 2011. [http://www.who.int/nmh/countries/qat_en.pdf?ua=1]. [accessed 23rd November 2015].
Riboli E, Kaaks R. The EPIC Project: rationale and study design. European Prospective Investigation into Cancer and Nutrition. Int J Epidemiol. 1997;26:S6.
Riboli E, Hunt KJ, Slimani N, Ferrari P, Norat T, Fahey M, et al. European Prospective Investigation into Cancer and Nutrition (EPIC): study populations and data collection. Public Health Nutr. 2002;5:1113–24.
Allen N, Sudlow C, Downey P, Peakman T, Danesh J, Elliott P, et al. UK Biobank: Current status and what it means for epidemiology. Health Policy and Technology. 2012;1:123–6.
Collins R. What makes UK Biobank special? Lancet. 2012;379:1173–4.
Cho SY, Hong EJ, Nam JM, Han B, Chu C, Park O. Opening of the National Biobank of Korea as the Infrastructure of Future Biomedical Science in Korea. Osong Public Health and Research Perspectives. 2012;3:177–84.
Chen Z, Lee L, Chen J, Collins R, Wu F, Guo Y, et al. Cohort Profile: The Kadoorie Study of Chronic Disease in China (KSCDC). Int J Epidemiol. 2005;34:1243–9.
Colditz GA, Manson JE, Hankinson SE. The Nurses’ Health Study: 20-year contribution to the understanding of health among women. J Womens Health. 1997;6:49–62.
Watanabe S, Tsugane S, Sobue T, Konishi M, Baba S. Study design and organization of the JPHC study. Japan Public Health Center-based Prospective Study on Cancer and Cardiovascular Diseases. J Epidemiol. 2001;11:S3–7.
German National Cohort (GNC) Consortium. The German National Cohort: aims, study design and organization. Eur J Epidemiol. 2014;29:371–82.
Toledano MB, Smith RB, Chang I, Douglass M, Elliott P: Cohort profile: UK COSMOS - a UK cohort for the study of environment and health. International Journal of Epidemiology 2015. (in press).
Schuz J, Elliott P, Auvinen A, Kromhout H, Poulsen AH, Johansen C, et al. An international prospective cohort study of mobile phone users and health (Cosmos): Design considerations and enrolment. Cancer Epidemiol. 2011;35:37–43.
Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire- 2: Validity of a Two-Item Depression Screener. Med Care. 2003;41:1284–92.
Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–95.
Gallacher J, Collins R, Elliott P, Palmer S, Burton P, Mitchell C, et al. A Platform for the Remote Conduct of Gene-Environment Interaction Studies. PLoS One. 2013;8:e54331.
Spruit MA, Sillen MJH, Groenen MTJ, Wouters EFM, Franssen FME. New Normative Values for Handgrip Strength: Results From the UK Biobank. J Am Med Dir Assoc. 2013;14:775.
Goloba M, Nelson S, Macfarlane P. The Electrocardiogram in Pregnancy. Computing in Cardiology. 2010;37:693–6.
Keehn L, Milne L, McNeill K, Chowienczyk P, Sinha MD. Measurement of pulse wave velocity in children: comparison of volumetric and tonometric sensors, brachial-femoral and carotid-femoral pathways. J Hypertens. 2014;32:1464–9.
Elliott P, Vergnaud AC, Singh D, Neasham D, Spear J, Heard A. The Airwave Health Monitoring Study of police officers and staff in Great Britain: Rationale, design and methods. Environ Res. 2014;134:280–5.
Cleutjens FAHM, Spruit MA, Ponds RWHM, Dijkstra JB, Franssen FME, Wouters EFM, et al. Cognitive Functioning in Obstructive Lung Disease: Results from the United Kingdom Biobank. J Am Med Dir Assoc. 2014;15:214–9.
van Engelen A, Wannarong T, Parraga G, Niessen WJ, Fenster A, Spence JD, et al. Three-Dimensional Carotid Ultrasound Plaque Texture Predicts Vascular Events. Stroke. 2014;45:2695–701.
Carver TE, Christou NV, Court O, Lemke H, Andersen RE. In-Vivo Precision of the GE Lunar iDXA for the Assessment of Lumbar Spine, Total Hip, Femoral Neck, and Total Body Bone Mineral Density in Severely Obese Patients. J Clin Densitom. 2014;17:109–15.
Murgatroyd H, Ellingford A, Cox A, Binnie M, Ellis JD, MacEwen CJ, et al. Effect of mydriasis and different field strategies on digital image screening of diabetic eye disease. Br J Ophthalmol. 2004;88:920–4.
Brage S, Ekelund U, Brage N, Hennings MA, Froberg K, Franks PW, et al. Hierarchy of individual calibration levels for heart rate and accelerometry to measure physical activity. J Appl Physiol. 2007;103:682–92.
Acknowledgements
Qatar Biobank is funded by the Qatar Foundation for Education, Science and Community Development and the Supreme Council of Health.
We thank all the participants and staff of the Qatar Biobank pilot study for their contributions. P.E. and ER are supported by the Imperial College London Healthcare NHS Trust and Imperial College Biomedical Research Centre. PE is supported by the Medical Research Council and Public Health England (MRC-PHE) Centre for Environment and Health, the National Institute for Health Research (NIHR) Health Protection Research Unit on Health Impact of Environmental Hazards and is an NIHR Senior Investigator.
The funding body played no role in the study design; the analysis and interpretation of data; the writing of the manuscript; or in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HAK, AAT, AAM, AAK contributed to the overall concept, design and oversight of the study; HA, NA and FQ contributed to study management, quality control and acquisition of data; QC, IT, HW, and NM performed the statistical analysis and contributed to interpretation of the data and drafting of the manuscript; PD contributed to development and scientific review of study protocols; ER and PE contributed to the design of the study, development of study protocols, study oversight, and drafted and revised the paper. All authors read and approved the final manuscript for submission.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Al Kuwari, H., Al Thani, A., Al Marri, A. et al. The Qatar Biobank: background and methods. BMC Public Health 15, 1208 (2015). https://doi.org/10.1186/s12889-015-2522-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-015-2522-7