
Abstract
Background
Data on use and health benefits of active travel in rural low- and middle- income country settings are sparse. We aimed to examine correlates of active travel, and its association with adiposity, in rural India and Bangladesh.
Methods
Cross sectional study of 2,122 adults (≥18 years) sampled in 2011–13 from two rural sites in India (Goa and Chennai) and one in Bangladesh (Matlab). Logistic regression was used to examine whether ≥150 min/week of active travel was associated with socio-demographic indices, smoking, oil/butter consumption, and additional physical activity. Adjusting for these same factors, associations between active travel and BMI, waist circumference and waist-to-hip ratio were examined using linear and logistic regression.
Results
Forty-six percent of the sample achieved recommended levels of physical activity (≥150 min/week) through active travel alone (range: 33.1 % in Matlab to 54.8 % in Goa). This was more frequent among smokers (adjusted odds ratio 1.36, 95 % confidence interval 1.07–1.72; p = 0.011) and those that spent ≥150 min/week in work-based physical activity (OR 1.71, 1.35–2.16; p < 0.001), but less frequent among females than males (OR 0.25, 0.20–0.31; p < 0.001). In fully adjusted analyses, ≥150 min/week of active travel was associated with lower BMI (adjusted coefficient −0.39 kg/m2, −0.77 to −0.02; p = 0.037) and a lower likelihood of high waist circumference (OR 0.77, 0.63–0.96; p = 0.018) and high waist-to-hip ratio (OR 0.72, 0.58–0.89; p = 0.002).
Conclusions
Use of active travel for ≥150 min/week was associated with being male, smoking, and higher levels of work-based physical activity. It was associated with lower BMI, and lower risk of a high waist circumference or high waist-to-hip ratio. Promotion of active travel is an important component of strategies to address the growing prevalence of overweight in rural low- and middle- income country settings.
Similar content being viewed by others

Background
Over recent decades, urbanisation and industrialisation have led to declines in physical activity in many countries [1–3]. This has been associated with substantial increases in overweight and obesity, as well as excess cardiovascular- and cancer-related morbidity and mortality [4]. Physical inactivity is now estimated to be the fourth leading cause of death worldwide [4], and a major contributor to non-communicable diseases (NCDs). This is particularly important in low-and-middle-income countries (LMICs), where 80 % of deaths from NCDs occur [5], and urbanisation and industrialisation are increasing in many settings.
In view of the relatively high cardiovascular risk in South Asia [6], physical activity trends in this region, and their associations with cardiovascular risk factors including overweight and obesity, are of interest. The limited data available for India indicate that urban living is associated with reductions in work-based physical activity and increasingly sedentary lifestyles [3, 7]. Trends in rural areas are less clear, but there is some evidence of a reduction in agricultural work and a growing motor vehicle market [8]. India’s large rural population (69 % rural in 2011, compared to 55 % in China and 13 % in Brazil [9]), together with its relatively slow rate of decline in physical activity to date [3], may reflect maintenance of physical activity levels in the rural population.
Active travel (walking, cycling and public transport use) is being promoted as an important component of strategies to increase physical activity levels internationally [5]. This is consistent with a well-developed evidence base from high-income settings demonstrating a protective effect of active travel against overweight/obesity, cardiovascular risk factors and associated mortality [10, 11]. Predictors of active travel in high-income settings include environmental factors (such as low traffic volumes, higher public transport convenience and perceived safety, and a relatively pleasant general environmental aesthetic [12–14]) and individual factors (such as younger age, male sex, urban living, lower distance to work and lower income [13–15]). There is a relative lack of information regarding correlates of physical activity in LMICs [16]. A recent study of middle-income countries, including India, demonstrated associations between higher levels of active travel and male sex, younger age and lower income, in these contexts [17]. This study, additional studies from China [18, 19], and a study using an occupation-based sample from India [20], also indicate that active travel benefits cardiovascular risk factors, including measures of adiposity, in these countries as it does in high-income settings. Data on use and health benefits of active travel in rural LMIC settings specifically are sparse. We conducted the analysis of rural populations in India and Bangladesh reported here, to examine:
-
1.
the socio-demographic correlates of active travel, and
-
2.
associations between active travel and adiposity.
Methods
Study design and subjects
Data were obtained from the Chronic Disease Risk Factor Survey, a cross-sectional survey conducted at three rural South Asian sites: Goa and Chennai in India, and Matlab in Bangladesh. Each site was selected on the basis of being a typical rural community in each setting, reflecting the local demographics and containing healthcare facilities to support collection of physical measurements. At each site, households in consecutive village sections, from the healthcare centre outwards, were sampled until households numbered ≥250 and all included sections were fully sampled (n = 308 households in Matlab, 309 in Goa, 257 in Chennai). All household residents of 2+ years resident in the area for ≥6 months of the year were invited to participate (n = 1143 in Matlab, 1212 in Goa, 940 in Chennai). Participants <18 years, and those for whom physical measurements were not available (see below), were excluded from our analyses.
Data collection
Data were collected between 06/2011–05/2012 (Matlab), 10/2011–03/2013 (Goa), and 11/2011–03/2013 (Chennai). Trained field-workers (four per site) conducted house-to-house interviews using structured back-translated questionnaires in the local language. Data regarding demographics and chronic disease symptoms, history and risk factors, were collected. Physical activity data were collected using the Global Physical Activity Questionnaire (GPAQ) [21]. Respondents were asked whether they typically undertook ≥10 min episodes of moderate/vigorous physical activity at work or for leisure, and/or for active travel (travel via cycling or walking). The typical duration spent in each type of activity per week was recorded. Participants who completed the questionnaire were invited to attend a field clinic where trained personnel took physical measurements. The measurements included two of standing height (to the nearest 1 mm, using a portable stadiometer (Leicester)), two of weight (to the nearest 100 g, using portable digital scales (Tanita), with participants in light clothing and no shoes), and two of each of waist- and hip-circumference (to the nearest 1 mm, using a taut plastic tape). Measurement equipment was calibrated daily.
Socio-demographic and additional lifestyle variables
The collected data were used to produced variables describing sex, education (categories: ‘no formal’, ‘any school’, or ‘any higher’ education), smoking status (ever-/never-smoker), moderate/vigorous leisure- and work- related activity (both dichotomised using the 150-min/week cut-off), and oil/butter consumption (categorised as more or less than 1 L/month, based on estimated household consumption, adjusted for number of household residents).
Active travel variables
A binary active travel variable was used as our main predictor variable. In line with international physical activity guidance [4], participants were dichotomised according to whether they undertook ≥150-minutes of active travel/week. A categorical active travel variable (categories: 0 versus >0 to 150 versus ≥150 min/week) was also produced, in order to consider possible dose-response between the amount of active travel and outcomes. Analyses using this categorical exposure variable were the same as main analyses.
Adiposity variables
Anthropometric measures were used to generate outcome variables. Body Mass Index (BMI) was calculated using mean height and weight measurements. BMI cut-offs of both ≥23 kg/m2 (recommended for Asian populations [22]) and ≥25 kg/m2 were used to define overweight and obesity. Obesity (≥30 kg/m2) was not considered as an outcome as it was infrequent (n = 55, 2.6 %). Mean waist- and hip-circumference measurements were used to calculate waist-to-hip ratios. Binary variables for both waist circumference and waist-hip ratios were produced, using cut-offs recommended for Asian populations (high waist circumference: >85 cm for males, >80 cm for females; high waist-hip ratio: ≥0.9 for males, ≥0.8 for females) [23, 24].
Statistical analyses
A descriptive summary of study variables was produced for each site. Comparisons between sites were made using chi-square and Kruskal-Wallis tests for categorical and continuous variables (which failed tests of normality and equal variance), respectively. Logistic regression was used to examine associations between ≥150 min/week of active travel and socio-demographic factors as well as lifestyle indices including other modes of physical activity. Linear and logistic regression was used to examine associations between ≥150 min/week of active travel and measures of adiposity. Robust standard errors that allow for correlation within households were used in the regression analyses. Partially adjusted models included age and sex. Fully adjusted models additionally adjusted for site, education, smoking status, oil/butter consumption, and work- and leisure-related physical activity. The analyses examining associations between ≥150 min/week of active travel and adiposity measures were repeated with the categorical active travel variable, and a sensitivity analysis (excluding those ≥65 years; n = 166, 7.8 %) was performed. Individuals with missing data were excluded from the regression analyses (n = 15 (0.7 %) for analysis of correlates of active travel; n = 36 (1.7 %) for analyses of BMI outcomes; n = 41 (1.9 %) for analyses of waist circumference and waist hip ratio outcomes).
Ethics statement
Ethical approval was obtained from the Public Health Foundation of India, Sangath (Goa), Voluntary Health Services (Chennai), the International Centre for Diarrhoeal Disease Research (Matlab), and the Indian Health Ministry (No. 50/5/Indo-CVD/DP/2010-NCD-II). Informed consent was obtained from participants.
Results
In Goa, Chennai and Matlab, 1143, 1212 and 940 individuals were invited to participate, respectively. Individual level response rates were 92.9 % (Goa), 96.1 % (Chennai) and 96.1 % (Matlab). Non-participation was due to non-consent or no availability after repeated visits. Clinic attendance rates were 99.6 % (Matlab), 85.8 % (Goa) and 97.0 % (Chennai). After excluding individuals <18 years (n = 1138) and those that did not attend for clinical measurements (n = 145), 2122 participants were included: 740 from Matlab, 734 from Goa, 648 from Chennai. A summary of their socio-demographic characteristics, activity patterns, and adiposity measures are presented in Table 1. Individual components of the socio-demographic/lifestyle data were missing for <0.5 % of participants, components of activity data for <2.0 %, and at least one weight-related outcome for <1.5 %.
Socio-demographic and lifestyle indices
Mean participant age was lower in Chennai than in Goa and Matlab (37.2 versus 40.7 and 41.3 years, respectively; p < 0.001). The proportion with no formal education was higher in Chennai than Matlab or Goa (39.4 % versus 27.6 % and 28.1 %; p < 0.001). Participants in Matlab were less likely to be ever-smokers than those in Goa and Chennai (18.1 % versus 85.8 % and 72.7 %; p < 0.001). Oil/butter consumption was lower in Goa than in Matlab and Chennai (95.9 % consumed ≤1 L/month, versus 74.7 % and 70.7 %; p < 0.001).
Physical activity indices
Forty-six percent of the sample achieved recommended physical activity levels (≥150 min/week) using active travel alone (Table 1). This was less common in Matlab than in Goa and Chennai (33.1 % versus 54.8 % and 49.7 %, respectively; p < 0.001). Total physical activity levels were higher in Chennai than in Goa and Matlab (1285 versus 612 and 419 min/week; p < 0.001), reflecting higher work-related physical activity levels in Chennai (e.g. 1011 min/week in Chennai, 175 in Matlab). Leisure-related activity was relatively low across all sites: 5.9 % achieved ≥150 min/week.
Measures of adiposity
Mean BMI was higher in Goa than in Chennai and Matlab (21.8 kg/m2 versus 21.2 and 21.3; p = 0.002; Table 1). Similar trends were observed for overweight/obese classification (BMI ≥23 kg/m2: 35.8 % in Goa, 31.0 % in Chennai, 27.4 % in Matlab; p = 0.002), high waist circumference (32.3 % in Goa, 24.7 % in Chennai, 26.7 % in Matlab, p = 0.004) and high waist-hip-ratio (70.4 % in Goa, 59.5 % in Chennai, 58.5 % in Matlab; p < 0.001).
Correlates of active travel
Achievement of recommended physical activity levels using active travel (≥150 min/week) was more common in Goa than in Matlab (adjusted odds ratio: 2.13, 95 % CI: 1.59-2.86, p < 0.001; Table 2; for Chennai versus Matlab, OR = 1.22, 0.91–1.63, p = 0.181). It was also less common among females than males (OR: 0.25, 0.20–0.31, p < 0.001). This sex difference persisted when those in the ‘homemaker’ occupational category (n = 781/1219 females and 30/903 males) were excluded: OR 0.56, 0.43–0.73, p < 0.001 (a posteriori test). No association with age was observed (e.g. among those aged 50+ cf. 18–25 years, OR: 0.81, 0.58–1.12, p = 0.195). Ever-smokers were more likely to achieve recommended physical activity levels by active travel than never-smokers (OR: 1.36, 1.07–1.72, p = 0.011), although this association was only statistically significant in Matlab. Achievement of ≥150 min/week of active travel was more common among individuals who completed ≥150 min/week of work-related physical activity (OR 1.71, 1.35–2.16, p < 0.001).
Associations between active travel and adiposity
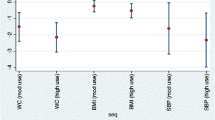
In unadjusted models, persons achieving ≥150 min/week of active travel had significantly lower BMI and were significantly less likely to be overweight, have a high waist circumference or have a high waist-hip ratio. Findings slightly attenuated in fully adjusted models (Table 3) leaving the overweight finding no longer significant (OR 0.83, 0.68–1.02, p = 0.093). The associations between ≥150 min/week of active travel and a lower BMI and lower likelihood of high waist circumference and high waist-hip ratio remained significant in the adjusted models: coefficient for BMI: −0.39 (−0.77 to −0.02; p = 0.037), OR for high waist circumference: 0.77 (0.63–0.96; p = 0.018), OR for high waist-hip ratio: 0.72 (0.58–0.89; p = 0.002). Outcomes of the analyses excluding those >65 years were consistent with these results (see Additional file 1: Table S1).
Outcomes of analyses using the categorical active travel variable were again similar and suggested the duration of active travel was relevant (see Additional file 2: Table S2). There were 677, 476 and 969 participants in the groups reporting no active travel, >0 to <150 min/week and ≥150 min/week, respectively. For the >0 to <150 min/week group, mean weekly duration of active travel was 90.5 min (SD 37.4). For the ≥150 min/week group this was 521.5 min (SD 476.7). In the fully adjusted models, BMI, waist circumference and waist-hip ratio were all observed to trend downwards with increasing levels of active travel. For high waist-hip ratio, differences compared with the group undertaking no active travel were observed for both active travel groups (OR 0.58 (0.41–0.80; p = 0.001) in the >0 to <150 min/week group, 0.55 (0.42–0.71; p < 0.001) in the ≥150 min/week group). For BMI and high waist circumference outcomes, differences compared with the group undertaking no active travel were observed only for the higher active travel group (BMI: coefficient = −0.28 (−0.84, 0.28; p = 0.324) in the >0 to <150 min/week group, −0.54 (−1.00, −0.07; p = 0.023) in the ≥150 min/week group; waist circumference: OR = 0.90 (0.66, 1.22; p = 0.485) in the >0 to <150 min/week group, 0.73 (0.56,0.96; p = 0.027) in the ≥150 min/week group).
Discussion
Summary of results
We found that 45.7 % of adults achieved recommended physical activity levels (≥150 min/week) through active travel in rural settings in South Asia. Both males and those that achieved recommended weekly physical activity levels through work-based activity were more likely to achieve this. After adjusting for a variety of socio-demographic factors and other physical activity, ≥150 min/week of active travel was associated with reduced adiposity. Evidence of association was relatively strong for BMI, high waist circumference and high waist-to-hip ratio. Findings using binary BMI-based overweight/obese classifications were consistent, but evidence of association was weaker.
Correlates of active travel
Few other data regarding active travel are available for South Asian populations. However, in keeping with our observed sex difference in participation in active travel, a recent review demonstrated lower physical activity levels in females, compared with males, in almost all studies of South Asian populations [25]. This review suggested that cultural expectations—including those surrounding care-giving and other domestic activities—likely limit the time available for physical activity among females [25]. Relatively high levels of gender inequality, as demonstrated by Social Institutions and Gender Index (SIGI) scores, in both India and Bangladesh [26], may also be relevant. Country-level analyses have demonstrated an inverse relationship between these scores and active travel among females [27]. Various factors such as monetary costs, safety issues, ethnicity, cultural and religious factors, have been suggested as relevant to this relationship. While the associations between these factors and active travel have been studied in other settings [28–30], as far as we are aware, they have not been studied for South Asian populations, and this area may benefit from future research.
Active travel and measures of adiposity
The observed associations between active travel and measures of adiposity are in keeping with previous data from India indicative that active travel is associated with a lower risk of overweight/obesity, hypertension and diabetes [17, 20]. The associations are consistent with studies from elsewhere that observed similar associations between active travel, overweight/obesity [11, 18, 31–33], other cardiovascular risk factors [10, 11, 33], cardiovascular disease [10], and related mortality [10]. Additionally, a recent review of observational data from LMICs has demonstrated a role for physical activity more generally, in limiting cardiovascular disease, cancer and all-cause mortality in these settings [34].
Strengths and limitations of study
This study presents some of the first data on correlates of active travel and associations with adiposity in rural South Asia. The study used representative sampling of populations, with high participation rates, and data collection that allowed for control of important covariates. The main limitation of the study is the use of a cross sectional design, meaning that it remains unclear whether any inference regarding causation is appropriate. The sample size was insufficient for stratified analyses by study site or sex. Physical activity data were based on self-report, and collected via the GPAQ [21]. The GPAQ is similar to the International Physical Activity Questionnaire (IPAQ), which has been associated with overestimation of physical activity levels [35, 36]. Moreover, the particular back-translated version of the GPAQ used here has not been validated. Previous tests of GPAQ reliability and validity versus the IPAQ in a largely LMIC sample showed reasonable correlation between outcomes from the two questionnaires [37]. Both were developed for surveillance studies, and the GPAQ for surveillance in LMICs specifically. There is additional potential for residual confounding as we were unable to account for all factors that may influence both our predictor and outcome measures. For example, ambient temperature and weather conditions, which are likely to have varied across the different sites studied, are important predictors of active travel [27], impact on other forms of physical activity [38], and influence food intake [39, 40]. Additional environmental issues potentially relevant to active travel in South Asian countries include the relatively high levels of road traffic accidents and air pollution [41, 42]. We were unable to consider these, or lung function, all of which may not only influence active travel usage, but also alter the overall benefit-cost ratio relating to active travel in these rural populations.
Policy implications
Our results suggest that active travel may protect against weight gain in South Asian populations. Although no large-scale evaluation of the costs and benefits of active travel in the South Asian setting has yet been carried out, it appears likely that the overall impact of active travel in rural South Asia would be positive (e.g. [43]). Our data would therefore support the application of current World Health Organization guidelines [5]—which recommend promotion of active travel as a NCD control strategy—in India and Bangladesh. Although current NCD strategies for Bangladesh do encourage environments that facilitate active travel [44], this is less obvious for India [45], and both are non-specific, and lack direct guidance that could help to motivate, as well as facilitate, this behavior. In this regard the lack of data regarding social and environmental impact on active travel in these contexts is concerning, particularly as data from several other contexts suggest that many such factors may have adverse effect on use of active travel. These include road safety concerns, and road infrastructure issues with consequences for traffic density and public transportation, both of which are relatively prevalent in South Asia [46, 47].
Ongoing research on active travel in LMICs is particularly important given the rapidly changing economic, environmental and cultural contexts, including the rapid growth in motor vehicle ownership in many settings. Future research should include a greater emphasis on interventional studies and evaluation of natural experiments to better determine ‘what works’ to increase active travel in LMIC settings. Investigation of the intersection between active travel, social issues such as gender inequality, and potentially relevant environmental factors—including air pollution, road safety, and ambient temperature—would also help shape policy.
Conclusions
Active travel is a major component of physical activity in rural South Asian populations. It was found to be associated with being male, smoking, and relatively high levels of work-based physical activity. Active travel was associated with more favourable adiposity outcomes. Promotion of active travel is an important component of strategies to address the growing prevalence of overweight in rural LMIC settings.
Abbreviations
- OR:
-
Odds ratio
- BMI:
-
Body mass index
- NCD:
-
Non-communicable disease
- LMICs:
-
Low- and middle- income countries
- GPAQ:
-
Global physical activity questionnaire
- CI:
-
Confidence interval
- SIGI:
-
Social institutions and gender index
References
Brownson RC, Boehmer TK, Luke DA. Declining rates of physical activity in the United States: what are the contributors? Annu Rev Public Health. 2005;26:421–43.
Ng SW, Norton EC, Popkin BM. Why have physical activity levels declined among Chinese adults? Findings from the 1991–2006 China Health and Nutrition Surveys. Soc Sci Med. 2009;68:1305–14.
Ng SW, Popkin B. Time use and physical activity: a shift away from movement across the globe. Obes Rev. 2012;13:659–80.
World Health Organization (2010) Global recommendations on physical activity for health. © World Health Organization 2010.
World Health Organization. Global Action Plan for the Prevention and Control of Non-communicable Diseases 2013–2020. Geneva: World Health Organization; 2013.
Gupta M, Singh N, Verma S. South Asians and Cardiovascular Risk: What Clinicians Should Know. Circulation. 2006;113:e924–29.
Pucher J, Zr P, Mittal N, Zhu Y, Korattyswaroopam N. Urban transport trends and policies in China and India: impacts of rapid economic growth. Transport Reviews. 2007;27:379–410.
Mishra N, Shankar R. The great Indian equalization. Credit Suisse (Hong Kong) Ltd. India Market Strategy, 2012. Available at: https://doc.research-and-analytics.csfb.com/docView?language=ENG&source=ulg&format=PDF&document_id=963737241&serialid=8NZUwe7tqav3kKHhl%2FQ%2BbXy8%2BCEeydk5Zp5XRRo5Uo4%3D. Last accessed: May 2015
Ahluwalia IJ, Kanbur R, Mohanty PK. Challenges of urbanisation in India: an overview. In: Ahluwalia IJ, Kanbur R, Mohanty PK (eds.) Urbanisation in India: challenges, opportunities and the way forward. New Delhi: SAGE Publications; 2014.
Hamer M, Chida Y. Active commuting and cardiovascular risk: a meta-analytic review. Prev Med. 2008;46:9–13.
Gordon-Larsen P, Boone-Heinonen J, Sidney S, Sternfeld B, Jacobs Jr DR, Lewis CE. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med. 2009;169:1216–23.
Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Personal and environmental correlates of active travel and physical activity in a deprived urban population. Int J Behav Nutr Phys Act. 2008;5:43.
Dalton AM, Jones AP, Panter JR, Ogilvie D. Neighbourhood, Route and Workplace-Related Environmental Characteristics Predict Adults' Mode of Travel to Work. PLoS ONE. 2013;8:e67575.
Bopp M, Kaczynski AT, Campbell ME. Health-Related Factors Associated with Mode of Travel to Work. J Environ Public Health. 2013;2013:9. Article ID 242383.
Hutchinson J, White PCL, Graham H. Differences in the social patterning of active travel between urban and rural populations: findings from a large UK household survey. Int J Public Health. 2014;59:993–8.
Pratt M, Perez LG, Goenka S, Brownson RC, Bauman A, Sarmiento OL, et al. Can population levels of physical activity be increased? Global evidence and experience. Prog Cardiovasc Dis. 2015;57:356–67.
Laverty AA, Palladino R, Lee JT, Millett C. Associations between active travel and weight, blood pressure and diabetes in six middle income countries: a cross-sectional study in older adults. Int J Behav Nutr Phys Act. 2015;12:65.
Qin L, Stolk RP, Corpeleijn E. Motorized transportation, social status, and adiposity: The China Health and Nutrition Survey. Am J Prev Med. 2012;43:1–10.
Du H, Li L, Whitlock G, Bennett D, Guo Y, Bian Z, et al. Patterns and socio-demographic correlates of domain-specific physical activities and their associations with adiposity in the China Kadoorie Biobank study. BMC Public Health. 2014;14:826.
Millett C, Agrawal S, Sullivan R, Vaz M, Kurpad A, Bharathi AV, et al. Associations between Active Travel to Work and Overweight, Hypertension, and Diabetes in India: A Cross-Sectional Study. PLoS Med. 2013;10:e1001459.
Department of Chronic Diseases and Health Promotion, World Health Organization. Global Physical Activity Questionaire 2. Available at: http://www.who.int/chp/steps/GPAQ%20Instrument%20and%20Analysis%20Guide%20v2.pdf Last accessed: May 2015
Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus statement for diagnosis of obesity, abnormal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009;57:163–70.
Obesity in Asia Collaboration. Waist circumference thresholds provide an accurate and widely applicable method for the discrimination of diabetes. Diabetes Care. 2007;30:3116–18.
World Health Organization. Waist circumference and WHR: report of a WHO expert consultation, Geneva, 8–11 December 2008. Geneva: World Health Organization; 2011.
Ranasinghe CD, Ranasinghe P, Jayawardena R, Misra A. Physical activity patterns among South-Asian adults: a systematic review. Int J Behav Nutr Phys Act. 2013;10:116.
Organisation for Economic Co-operation and Development - Development Centre Social Cohesion Unit. Social Institutions and Gender Index: 2014 Synthesis Report. OECD, 2014. Available at: http://www.genderindex.org/sites/default/files/docs/BrochureSIGI2015.pdf. Last accessed: May 2015
Bosdriesz JR, Witvliet MI, Visscher TLS, Kunst AE. The influence of the macro-environment on physical activity: a multilevel analysis of 38 countries worldwide. Int J Behav Nutr Phys Act. 2012;9:110.
Araki K, Kodani I, Gupta N, Gill DL. Experiences in Sport, Physical Activity, and Physical Education Among Christian, Buddhist, and Hindu Asian Adolescent Girls. J Prev Med Public Health. 2013;46:S43–9.
Babakus WS, Thompson JL. Physical activity among South Asian women: a systematic, mixed-methods review. Int J Behav Nutr Phys Act. 2012;9:150.
Caperchione CM, Kolt GS, Mummery WK. Physical activity in culturally and linguistically diverse migrant groups to Western society: a review of barriers, enablers and experiences. Sports Med. 2009;39:167–77.
Wen LM, Orr N, Millett C, Rissel C. Driving to work and overweight and obesity: findings from the 2003 New South Wales Health Survey, Australia. Int J Obes. 2006;30:782–6.
Frank LD, Andresen MA, Schmid TL. Obesity relationships with community design, physical activity, and time spent in cars. Am J Prev Med. 2004;27:87–96.
Laverty AA, Mindell JS, Webb EA, Millett C. Active travel to work and cardiovascular risk factors in the United Kingdom. Am J Prev Med. 2013;45:282–8.
Milton K, Macniven R, Bauman A. Review of the epidemiological evidence for physical activity and health from low- and middle-income countries. Glob Public Health. 2014;9:369–81.
Rzewnicki R, Vanden Auweele Y, De Bourdeaudhuij I. Addressing overreporting on the International Physical Activity Questionnaire (IPAQ) telephone survey with a population sample. Public Health Nutr. 2003;6:299–305.
Ekelund U, Sepp H, Brage S, Becker W, Jakes R, Hennings M, et al. Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults. Public Health Nutr. 2006;9:258–65.
Bull FC, Maslin TS, Armstrong T. Global Physical Activity Questionnaire (GPAQ): Nine Country Reliability and Validity Study. J Phys Act Health. 2009;6:790–804.
Chan CB, Ryan DA. Assessing the effects of weather conditions on physical activity participation using objective measures. Int J Environ Res Public Health. 2009;6:2639–54.
Brobeck JR. Food intake as a mechanism of temperature regulation. Yale J Biol Med. 1948;20:545–52.
Marriott BM, editor. Nutritional needs in hot environments. Washington, DC: National Academy Press; 1993.
World Health Organization. Burden of disease from household air pollution for 2012. World Health Organization, 2014. Available at: http://www.who.int/phe/health_topics/outdoorair/databases/FINAL_HAP_AAP_BoD_24March2014.pdf?ua=1. Last accessed: May 2015
World Health Organization. Global status report on road safety 2013. World Health Organization, 2013. Available at: http://www.who.int/violence_injury_prevention/road_safety_status/2013/en/. Last accessed: May 2015
Woodcock J, Edwards P, Tonne C, Armstrong BG, Ashiru O, Banister D, et al. Public health benefits of strategies to reduce greenhouse-gas emissions: urban land transport. Lancet. 2009;374:1930–43.
Directorate General of Health Services, Ministry of Health and Family Welfare, World Health Organization. Strategic plan for surveillance and prevention of non-communicable diseases in Bangladesh 2011–2015. Dhaka: NCD Unit, Directorate General of Health Services; 2011.
Ministry of Health and Family Welfare, Government of India. National programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke (NPCDCS): Operational guidelines. Available at: http://www.mohfw.nic.in/index1.php?lang=1&level=3&sublinkid=661&lid=652. Last accessed: May 2015
Jain AK. Sustainable urban mobility in Southern Asia: Regional study prepared for Global Report on Human Settlements 2013. Nairobi, 2011. Available at: http://unhabitat.org/wp-content/uploads/2013/06/GRHS.2013.Regional.Southern.Asia_.pdf. Accessed August 2015.
World Health Organization. Road safety status in the WHO South-East Asia region, 2013. Available at: http://www.searo.who.int/entity/disabilities_injury_rehabilitation/topics/fact_sheet_road_safety_final.pdf. Accessed: August 2015.
Acknowledgments
The Chronic Disease Risk Factor Survey was supported by the Wellcome Trust Strategic Award for the South Asia Network for Chronic Disease, Public Health Foundation of India (Grant No. WT 084674).
Funding
None
Guarantor
Christopher Millett
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contribution
KS, DA, AD, JW, SE and PKD developed survey instruments and carried out the data collection. AJM and AAL cleaned and analysed the data. AJM, AAL and CM wrote the first draft of the manuscript. All authors provided input and approved the final version for submission.
Additional files
Additional file 1: Table S1.
Associations between active travel status and weight-related outcomes among participants < 65 years. (DOCX 91 kb)
Additional file 2: Table S2.
Associations between active travel status and weight-related outcomes. (DOCX 105 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
McKay, A.J., Laverty, A.A., Shridhar, K. et al. Associations between active travel and adiposity in rural India and Bangladesh: a cross-sectional study. BMC Public Health 15, 1087 (2015). https://doi.org/10.1186/s12889-015-2411-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-015-2411-0