
Abstract
Background
Nasal carriers of Staphylococcus aureus have an increased risk of acquiring skin and soft tissue infections, which could manifest as outbreaks, especially in crowded settings. Current prevention programs are ineffective, antibiotic resistance is rising and risk factors for becoming a carrier are incompletely understood. We aimed to examine whether a behavior, the neglect of skin wounds, is a risk factor for becoming a Staphylococcus aureus carrier during training.
Methods
We conducted a field-based cohort study among male infantry trainees in three seasons in Israel during 2011–12. Participants underwent anterior nares cultures and answered structured questionnaires on potential risk factors on two occasions: before and 3 weeks after start of training (N = 542). Attitudes and practices toward neglect of skin wounds were defined as perseverance in training at all costs, despite having a wound. Samples were processed within 18 hours for identification of Staphylococcus aureus. Univariable and multivariable logistic regression analyses were performed to assess risk factors for becoming a carrier.
Results
Carriage prevalence increased by 43.3 % during training, from 33.2 % to 47.6 % (p < 0.01). One-fourth (25.4 %) of those with a negative culture before training became carriers. None of the socio-demographic characteristics was a risk factor for becoming a carrier while the risk was lower in the winter (Odds ratio [OR] = 0.42; 95 % confidence interval [CI]: 0.23-0.78, p < 0.01) and spring (OR = 0.46; 0.26-0.81, p < 0.01) seasons compared to the summer season. Neglect of skin wounds in practice and attitude was a risk factor for becoming a carrier (OR = 2.40; 1.13-5.12, p = 0.02), as well as neglect in practice or attitude (OR = 1.86; 1.04-3.34, p = 0.04) compared to no neglect when controlled for season. The preventable fraction in the population attributed to neglect of skin wounds was 33 %.
Conclusions
Neglect of skin wounds is an independent, common and strong risk factor for becoming a Staphylococcus aureus carrier during training. This preventable behavior should not be ignored and should be addressed in public health programs during training and in other settings. Further research on behavioral determinants of Staphylococcus aureus carriage and infection is warranted.
Similar content being viewed by others


Background
Staphylococcus aureus is both a human commensal and a pathogen frequently causing clinically important infections such as skin and soft tissue infections (SSTIs), as well as life-threatening infectious diseases including pneumonia and sepsis [1]. Sporadic and epidemic SSTIs, frequently caused by S. aureus, are common among young adults. The burden of morbidity is even higher in crowded settings with close contact and intensive physical activity, such as on sport teams and in military settings [2–4]. The optimal SSTIs prevention strategy remains unclear, antibiotic resistance is rising and current prevention programs are ineffective [5]. Although carriers can carry S .aureus in multiple body sites, the anterior nares of the nose are the most frequent site [6]. Nasal carriers of S. aureus have an increased risk of acquiring an infection [7, 8]. Longitudinal studies show that about 20 % (range 12-30 %) of individuals are persistent nasal carriers, 30 % (16-70 %) are intermittent carriers, and 50 % (16-69 %) non-carriers [9]. van Belkum et al. suggested that intermittent carriers and non-carriers belong to the same type of nasal carriers [10]. Risk factors for becoming a nasal carrier are incompletely understood, and the investigation of possible risk factors, such as the rarely studied behavioral risk factors, may be useful in developing new preventive strategies [9]. Higher carriage prevalence has been found among individuals engaging in activities leading to skin wounds and those with skin infections [9]. Carriage prevalence, both of methicillin-susceptible S. aureus (MSSA) and methicillin-resistant S. aureus (MRSA), may be even higher among soldiers [11].
SSTI outbreaks have been reported frequently in the Israel Defense Forces (IDF) over the last decade with attack rates of up to 95 % among groups of infantry trainees [12, 13]. This epidemic and sporadic illness has been associated with a high burden of lost training days, significant clinical complications and deaths of infantry trainees in recent years [14].
Against this background, we aimed to examine whether S. aureus carriage prevalence increases during infantry training and whether a behavior, the neglect of skin wounds, is a risk factor for becoming a S. aureus nasal carrier.
Methods
Study design, settings and population
We conducted this field-based cohort study in three consecutive cohorts, drafted to three different IDF infantry training bases in July 2011 (“summer”), November 2011 (“winter”) and March 2012 (“spring”). Participants, all young adult males, underwent anterior nares cultures and answered structured questionnaires on potential risk factors on two occasions: just before and three weeks after start of training. The study was population-based, with no exclusion criteria. However, candidates undergo medical screening, and individuals with underlying medical conditions that could affect the performance of an infantry soldier in field conditions are excluded from infantry training and hence from the study. During the first three weeks of training, soldiers lived under crowded communal conditions (12–16 persons per room). This period included basic military training, physical exercises, classroom lessons and a short but intensive training period conducted in the field.
The study was conducted by trained medical personnel from the Preventive Medicine Branch staff. Participants privately answered questionnaires in writing and were notified that data collected will not be known to base cadre and will not have any effect on their training or service. Military cadre were excluded from the study presentation and data collection in order to insure the participants' informed consent and to prevent any coercion or influence of commanders on their subordinates. Each participant signed an informed consent form before recruitment to the study. The study was approved and supervised by the IDF Medical Corps Institutional Review Board.
Variables and data sources
Season (summer; winter; spring) was based on timing of data collection, and also represent training base. Participants gave information on history of skin infections, life-style and socio-demographic factors, such as smoking status (nonsmoker; current smoker), country of birth (native Israeli; immigrant), number of children in household (0; ≥1) and age. Data on antimicrobial therapy prescription between the two samplings was retrieved from the military computerized medical records.
Questions on attitudes before and during training (identical questions) and questions on practices during training were scored on a 1–5 scale and grouped for analysis into two categories: 1-3/4-5, as in a previous study [15]. Attitudes and practices toward neglect of skin wounds (no neglect; neglect) were defined as perseverance in training at all costs, despite having a wound. In infantry basic training settings, the implication is lack of any attention to the wound. Attitude question was: “If the skin is wounded during training (cuts/abrasions), it is very important to continue training at all costs, despite the wound". Practice question was: “I, personally, persevere in my training at all costs, even if my skin is wounded (cuts/abrasions)”.
In addition, care of skin wounds in attitude (appropriate care; inappropriate care) was based on the response to the question: "The immediate care of a skin wound includes washing, cleaning and disinfection".
Additional practices assessed included share of personal drinking cup and share of personal towel (no share; share).
Laboratory procedures
The samplings were conducted in the same manner on two occasions: before and three weeks after start of training by a trained team of healthcare workers and followed a written protocol. Nasal samples, from both anterior nares, were collected using an AMIES applicator (Copan, Brescia, Italy) and cultured within 18 hours at the IDF Central Medical Laboratory according to standard protocols. Samples were plated on tryptic soy agar plates with 5 % sheep blood agar and on chromogenic plates CHROMagar StaphAureus/ CHROMagar MRSA (Hy-labs, Rehovot, Israel) at 35 °C. After a 48 hours incubation period, S. aureus was identified by colony morphology, DNAse and staphytect plus (oxoid) agglutination kit. Screening for MRSA was conducted using 30 μg Cefoxitin discs on Mueller- Hinton agar (Hy-labs) by disc-diffusion, according to the recommendations of the Clinical and Laboratory Standards Institute (CLSI) [16]. S. aureus isolates were preserved at −70 °C on Hy-transport medium (Hy-labs).
Statistical methods
We calculated carriage prevalence by dividing the number of participants with positive S. aureus nasal culture by the appropriate denominator of valid samples. We calculated overall and season-specific prevalence, before and during training. We compared prevalence before and prevalence during training, overall and by season, using McNemar's test. We defined becoming a S. aureus carrier as having a negative culture before training and a positive culture during training and calculated the proportion who became carriers with 95 % confidence interval (CI). We performed univariable analyses to assess risk factors for becoming a carrier using χ2 tests. In order to assess dose–response pattern, we created two composite variables for neglect of skin wounds and assessed them in the multivariable logistic regression models:
-
1)
Attitude before and attitude during training (no neglect before and during training; neglect before or during training; neglect before and during training).
-
2)
Practice and attitude during training (no neglect in practice and attitude; neglect in practice or attitude; neglect in practice and attitude).
We calculated odds ratios (OR) and their 95 % confidence intervals (CI) as measures of association for relative difference. We calculated preventable fraction in the population as a measure of association for absolute difference, according to Levin’s Population Attributable Risk formula [(qpop-qunexposed)/qpop] [17]. We performed statistical analysis with SAS software, version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Population characteristics
Of the 797 male recruits approached to participate in the study, 674 (84.6 %) agreed to participate and underwent sampling before start of training. Three weeks after start of training, 19.6 % were lost to follow-up and not included in the analysis, yielding the study population (N = 542). There were no differences in socio-demographic characteristics or carriage prevalence before training between study participants and those who were lost to follow-up, except for the lower proportion of current smokers among study participants (18 % vs. 26 %). Mean participant age was 18.9 years (SD = 1.1), and 95 % of participants were aged 18–20 (see Table 1).
S. aureus carriage prevalence
S. aureus carriage prevalence before training was 33.2 % (180/542) and did not differ by season or socio-demographic characteristics (data not shown).
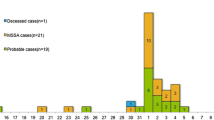
Carriage prevalence increased during training by 43.3 % (95 % CI: 24-66 %, p < 0.01), from 33.2 % to 47.6 %. In each of the three seasons, carriage prevalence increased during training (p < 0.01), most notably in the summer, by 76.8 %, from 29.9 % to 52.9 % (see Fig. 1).

Staphylococcal aureus carriage prevalence by season, before and three weeks after start of training (N = 542)a. aIncrease in carriage prevalence during training was significant (p < 0.01) for each season
Almost all (92.2 %, 166/180) carriers before training remained carriers, with similar proportions in the three seasons (summer: 53/56 = 94.6 %; winter: 59/64 = 92.2 %; spring: 54/60 = 90 %). A single isolate, cultured during summer, was identified as MRSA, while all other isolates were MSSA.
Risk factors for becoming a carrier
Among 362 with a negative culture before training, 25.4 % (95 % CI: 21.1-30.1 %) became S. aureus carriers during training. Data on attitudes and practices were missing for seven participants, three of whom became carriers; yielding a sample of 355 participants for analysis of risk factors. Socio-demographic characteristics (smoking status, country of birth, number of children in household and age), history of skin infections and antimicrobial therapy prescription were not risk factors for becoming a carrier.
The risk of becoming a carrier was lower in the winter (OR = 0.42; 95 % CI: 0.23-0.78) and spring (OR = 0.46, 0.26-0.81) seasons compared to the summer season (see Table 2).
Inappropriate care of skin wounds in attitude during training (11 % of the population) was a possible risk factor (OR = 1.87; 95 % CI: 0.92-3.81), and this subgroup had the highest risk of becoming a carrier (36.8 %).
Neglect of skin wounds in attitude before (60 % of the population) or neglect during (55 %) training was each a risk factor for becoming a carrier (OR = 1.68; 95 % CI: 1.00-2.81) and (OR = 1.99; 95 % CI: 1.20-3.30), respectively.
Neglect of skin wounds in practice (78 % of the population) was a possible risk factor (OR = 1.90; 95 % CI: 0.99-3.63). Those who did not neglect skin wounds in practice had the lowest risk of becoming a carrier (16.9 %), leading to a preventable fraction in the population attributed to neglect of skin wounds in practice of 33 %. In contrast, share of drinking cup or towel were not risk factors for becoming a S. aureus carrier.
We assessed correlations between neglect of skin wounds in attitudes and practices by Spearman correlation coefficients, which were 0.57 for practice and attitude during training (p < 0.01), and 0.42 for attitude before and during training (p < 0.01). Therefore, each time we re-introduced one risk factor (original or composite variable) into the multivariable logistic regression models, controlling for season which was the only significant covariate at a significance level of 0.05.
Risk factors magnitude and direction remained similar or was slightly accentuated after controlling for season (see Table 3). The composite variables exhibited a dose–response pattern, with gradient risk by having 2, 1 or 0 risk factors of neglect. Neglect of skin wounds in attitude before and during training was a risk factor for becoming a carrier (OR = 2.98; 95 % CI: 1.48-6.00), as well as possibly an attitude before or during training (OR = 1.68; 95 % CI: 0.95-2.96) compared to no neglect, controlled for season.
Neglect of skin wounds in practice and attitude during training, was a risk factor for becoming a carrier (OR = 2.40; 95 % CI: 1.13-5.12), as well as in practice or attitude (OR = 1.86; 95 % CI: 1.04-3.34) compared to no neglect, controlled for season.
Discussion
In this study, S. aureus carriage prevalence among trainees increased drastically three weeks after start of training, reaching a prevalence of nearly 50 %. Almost all carriers before training remained carriers, while one fourth of those with a negative culture before training became carriers, with the highest risk in the summer. To the best of our knowledge, this cohort study is the first to discover that a behavior, the neglect of skin wounds, is a risk factor for becoming a S. aureus carrier. Neglect of skin wounds was an independent, common and strong risk factor, both in attitude and/or in practice, before and/or during training, with a dose–response pattern. The preventable fraction in the population attributed to neglect of skin wounds was 33 %, implying that prevention of this behavior could carry significant benefits.
The observed increase in S. aureus carriage prevalence during training was relatively high, increasing from 33 % to 47 %. MRSA was a rare finding in our population, as it was in another study among Chinese soldiers [18]. Nevertheless, the high prevalence of carriage and the fact that one fourth became a carrier of MSSA during training underscore the high risk in this crowded setting with close contact and intensive physical activity, and help explain previous reports of SSTI outbreaks during military training [19]. Military training is a risky period for bacterial transmission of other pathogens as well, as we previously shown for Streptococcus pneumoniae [15].
We discovered that neglect of skin wounds in practice and/or attitude is common among trainees and is a strong risk factor for becoming a S. aureus carrier. These findings are unlikely explained by chance, selection bias or differential information bias, given our study methods. Confounding by season or training base cannot explain the findings, as we controlled for these factors. As in any study, we cannot rule out residual confounding by other unknown factors. However, our findings appear to be specific to neglect of skin wounds and are not likely confounded by other behaviors, as no association was found with other behaviors such as smoking or sharing of drinking cup or towel. The relation between neglect of skin wounds and the risk of becoming a S. aureus carrier is further supported by temporality in our cohort study, strength of association, dose–response pattern and robustness of association across different measures for neglect of skin wounds, including attitudes and practices at various time points as well as another attitude toward appropriate care of skin wounds. These findings are plausible, taken previous observations of higher carriage prevalence among individuals conducting activities leading to skin wounds and those with skin infections [9]. The next step would be to replicate our findings in other populations and examine whether prevention programs addressing neglect of skin wounds are effective in reducing S. aureus carriage and burden of infectious diseases.
The prevention of SSTIs is complex and evidence for the effectiveness of commonly employed preventive measures is lacking. Current guidelines emphasize the importance of health education at the population level and heightened hygiene measures for individual patients with SSTIs, while less focus has been directed toward primary prevention efforts [20]. However, in a recent well-designed cluster randomized controlled trial, personal hygiene and education measures, including weekly use of chlorhexidine body wash, did not prevent SSTIs in general, nor MRSA SSTIs in particular, among a high-risk population of military trainees [5]. This study did not specifically address the issue of neglect of skin wounds. In contrast, retrospective surveillance analyses have shown a reduction of 30 % in SSTIs in a military training center following a comprehensive hygiene-based primary prevention program [21].
Our study suggests that summer season is a risk factor for becoming a S. aureus carrier during training. This finding reconfirms the established seasonality of SSTIs [22]. Each sampling season was conducted in a different training base and time, hence location or cohort effect, although unlikely, cannot be ruled out as a possible contributing factor. Season remains the most plausible explanation as we were unable to identify any substantial differences over time or in population characteristics (i.e. country of birth, number of children in household and age), behavior, training regimens or environmental conditions between the bases.
Our study has several limitations. First, the sample size was not powered to rule out weaker or less common risk factors (such as appropriate care of skin wounds). Second, only 80 % of the study population was available for follow up, raising the theoretical concern of a selection bias, unlikely in light of similar characteristics of those who were lost to follow-up. Third, our ability to identify carriage state was limited by having only two nasal cultures. Fourth, neglect of skin wounds was assessed by questionnaires and not direct observation, potentially biasing the results, i.e. due to social desirability. However, such potential bias would be non-differential and could only bias the results toward the null.
Conclusions
Neglect of skin wounds is an independent, common and strong risk factor for becoming a Staphylococcus aureus carrier. This preventable behavior should not be ignored and should be addressed in public health programs during training and in other settings. Further research on behavioral determinants of Staphylococcus aureus carriage and infection is warranted.
Abbreviations
- CI:
-
Confidence interval
- IDF:
-
Israel Defense Forces
- MSSA:
-
Methicillin-susceptible S. aureus
- MRSA:
-
Methicillin-resistant S. aureus
- OR:
-
Odds ratio
- S. aureus:
-
Staphylococcus aureus
- SD:
-
Standard deviation
- SSTIs:
-
Skin and soft tissue infections
- Vs.:
-
Versus
References
Lowy FD. Staphylococcus aureus infections. The New England journal of medicine. 1998;339(8):520–32.
Kazakova SV, Hageman JC, Matava M, Srinivasan A, Phelan L, Garfinkel B, et al. A clone of methicillin-resistant Staphylococcus aureus among professional football players. New England Journal of Medicine. 2005;352(5):468–75.
Landrum ML, Neumann C, Cook C, Chukwuma U, Ellis MW, Hospenthal DR, et al. Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005–2010. JAMA. 2012;308(1):50–9.
Morrison-Rodriguez SM, Pacha LA, Patrick JE, Jordan NN. Community-associated methicillin-resistant Staphylococcus aureus infections at an Army training installation. Epidemiology and infection. 2010;138(5):721–9.
Ellis MW, Schlett CD, Millar EV, Wilkins KJ, Crawford KB, Morrison-Rodriguez SM, et al. Hygiene strategies to prevent methicillin-resistant Staphylococcus aureus skin and soft-tissue infections: a cluster-randomized controlled trial among high-risk military trainees. Clinical Infectious Diseases. 2014;58(11):1540–8.
Kluytmans J, van Belkum A, Verbrugh H. Nasal carriage of Staphylococcus aureus: epidemiology, underlying mechanisms, and associated risks. Clinical microbiology reviews. 1997;10(3):505–20.
Kluytmans JA, Mouton JW, Ijzerman EP, Vandenbroucke-Grauls CM, Maat AW, Wagenvoort JH, et al. Nasal carriage of Staphylococcus aureus as a major risk factor for wound infections after cardiac surgery. The Journal of infectious diseases. 1995;171(1):216–9.
Wertheim HF, Vos MC, Ott A, van Belkum A, Voss A, Kluytmans JA, et al. Risk and outcome of nosocomial Staphylococcus aureus bacteraemia in nasal carriers versus non-carriers. Lancet. 2004;364(9435):703–5.
Wertheim HF, Melles DC, Vos MC, van Leeuwen W, van Belkum A, Verbrugh HA, et al. The role of nasal carriage in Staphylococcus aureus infections. The Lancet infectious diseases. 2005;5(12):751–62.
van Belkum A, Verkaik NJ, de Vogel CP, Boelens HA, Verveer J, Nouwen JL, et al. Reclassification of Staphylococcus aureus nasal carriage types. The Journal of infectious diseases. 2009;199(12):1820–6.
Ellis MW, Griffith ME, Jorgensen JH, Hospenthal DR, Mende K, Patterson JE. Presence and molecular epidemiology of virulence factors in methicillin-resistant Staphylococcus aureus strains colonizing and infecting soldiers. Journal of clinical microbiology. 2009;47(4):940–5.
Wasserzug O, Balicer RD, Boxman J, Klement E, Ambar R, Zimhony O. A cluster of septic olecranon bursitis in association with infantry training. Military medicine. 2011;176(1):122–4.
Wasserzug O, Valinsky L, Klement E, Bar-Zeev Y, Davidovitch N, Orr N, et al. A cluster of ecthyma outbreaks caused by a single clone of invasive and highly infective Streptococcus pyogenes. Clinical Infectious Diseases. 2009;48(9):1213–9.
Levine H, Mimouni D, Bader T, Block C, Glikman D, Ben Dov D, et al. Prevention and treatment of invasive skin infections in the Israeli Defence Forces: Findings and recommendations of a multidisciplinary expert panel. Journal of Israeli Military Medicine. 2012;1:12–7 [In Hebrew].
Levine H, Balicer RD, Zarka S, Sela T, Rozhavski V, Cohen D, et al. Dynamics of pneumococcal acquisition and carriage in young adults during training in confined settings in Israel. PloS one. 2012;7(10):e46491.
Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-first Informational Supplement M100-S21. PA, USA: CLSI; 2011.
Szklo M, Nieto FJ: Epidemiology: beyond the basics: Jones & Bartlett Publishers; 2014.
Qu F, Cui E, Guo T, Li H, Chen S, Liu L, et al. Nasal colonization of and clonal transmission of methicillin-susceptible Staphylococcus aureus among Chinese military volunteers. Journal of clinical microbiology. 2010;48(1):64–9.
Campbell KM, Vaughn AF, Russell KL, Smith B, Jimenez DL, Barrozo CP, et al. Risk factors for community-associated methicillin-resistant Staphylococcus aureus infections in an outbreak of disease among military trainees in San Diego, California, in 2002. Journal of clinical microbiology. 2004;42(9):4050–3.
Gorwitz RJ, Jernigan DB, Powers J, Jernigan J. Strategies for clinical management of MRSA in the community: summary of an experts’ meeting convened by the Centers for Disease Control and Prevention. DC: Washington; 2006.
Morrison SM, Blaesing CR, Millar EV, Chukwuma U, Schlett CD, Wilkins KJ, et al. Evaluation of methicillin-resistant Staphylococcus aureus skin and soft-tissue infection prevention strategies at a military training center. Infection Control and Hospital Epidemiology. 2013;34(8):841–3.
Klein EY, Sun L, Smith DL, Laxminarayan R: The changing epidemiology of methicillin-resistant Staphylococcus aureus in the United States: a national observational study. American journal of epidemiology 2013:kws273.
Acknowledgments
We thank the IDF Preventive Medicine Branch staff for patiently collecting information and samples; IDF Central Medical Laboratory staff for meticulously carrying out lab analysis; bases clinic staff for facilitating and assisting in sample collection coordination; and the volunteers for their participation in the study. This work was supported by research grant of the IDF Medical Corps and Israeli Ministry of Defense. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Part of the study was presented at the 1st Annual Conference of the Israeli Public Health Physicians Association and Schools of Public Health, Ramat Gan, Israel, May 2014.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing interests.
Authors’ contributions
HL conceived and designed the study, led the analyses and interpretation, and drafted the manuscript. He takes responsibility for the integrity of the data and the accuracy of the data analyses. MH designed and oversaw the study, obtained funding, and significantly contributed to the analyses, interpretation and manuscript. RK, TS and SY contributed to design and coordinated acquisition of data. VR contributed to design, acquisition of data and statistical analyses. IRG and ATF contributed to design and acquisition of data and were medical directors of the study. OG and TH contributed to the design and interpretation, as well as led the laboratory analyses. All authors read, revised and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Levine, H., Kayouf, R., Rozhavski, V. et al. Neglect of skin wounds and the risk of becoming a Staphylococcus aureus nasal carrier: a cohort study. BMC Public Health 15, 749 (2015). https://doi.org/10.1186/s12889-015-2104-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-015-2104-8