
Abstract
Background
Obesity is one of the most significant risk factors for hypertension. However, there is controversy regarding which measure is the best predictor of hypertension risk. We compared body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), and waist-to-height ratio (WHtR) in subjects as predictive indicators for development of hypertension.
Methods
The data were obtained from the Korean Genome and Epidemiology Study (KoGES), a large population-based prospective cohort study. A total of 4,454 subjects (2,128 men and 2,326 women) aged 40–69 years who did not have hypertension at baseline were included in this study. Incident hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or anti-hypertensive medication use during the 4-year follow up. Receiver operating characteristic (ROC) analysis was used to compare discrimination abilities for anthropometric indices for hypertension. Hazard ratios were calculated by Cox proportional hazard model with adjustment for age, smoking status, alcohol consumption, diabetes and family history of hypertension by sexes.
Results
In men, the area under the ROC curve (AROC) was 0.62 for WC, WHR, and WHtR and 0.58 for BMI. In women, the AROCs for BMI, WC, WHR, and WHtR were 0.57, 0.66, 0.68, and 0.68, respectively. After adjustment for risk factors, a 1 standard deviation increase in BMI, WC, WHR, WHtR were significantly related to incident hypertension, respectively (hazard ratio: 1.39, 1.50, 1.40 and 1.49 in men, 1.31, 1.44, 1.35 and 1.48 in women).
Conclusions
The central obesity indices WC, WHR, and WHtR were better than BMI for the prediction of hypertension in middle-aged Korean people. WHtR facilitates prediction of incident hypertension because of the single standard regardless of sex, ethnicity, and age group. Therefore, WHtR is recommended as a screening tool for the prediction of hypertension.
Similar content being viewed by others


Background
Obesity increases the risk of hypertension, and the prevalence of obesity in middle-aged and elderly people has increased continuously [1-4]. In Korea, the prevalences of obesity among adults (age ≥30) as defined by body mass index (BMI) and waist circumference (WC) were reported to be 35.3% and 26.3%, respectively [4]. Notably, obesity can be defined by anthropometric indices, such as BMI, WC, waist-to-hip ratio (WHR), and waist-to-height ratio (WHtR). These anthropometric indices have been frequently used in epidemiological studies as they can be determined easily and at low cost [5]. BMI is the most widely used indicator of obesity, but it does not reflect central fat distribution, whereas WC, WHR, and WHtR are used as surrogate markers for body fat centralization [5-7]. A central distribution of body fat has been shown to be strongly associated with hypertension [5,8,9]. However, controversy remains regarding the best predictor of hypertension. Obesity has been defined as a BMI ≥30 kg/m2 in Western populations and ≥25 kg/m2 in Korean and other Asian populations [10]. Asians have higher body fat levels than Western people for the same BMI and WC according to epidemiologic studies on Asian populations [11,12]. The cut-off points for abdominal obesity in Korean adults were proposed to be a WC ≥90 cm in men and ≥85 cm in women by the Korean Society for the Study of Obesity (KSSO) [13]. The cut-off points of BMI for hypertension in men vary from 22.0 kg/m2 to 25.4 kg/m2 in different Asian countries [14]. This last study suggests the importance of applying ethnically appropriate cut-off points for anthropometric indices for hypertension. Most published research on obesity indices in relation to blood pressure is based on cross-sectional studies [2,8,13-17]. Only a few prospective studies of cut-off points for anthropometric indices for cardiovascular disease (CVD) have been conducted in Korea [18,19]. The purpose of this study was to evaluate and compare the abilities of BMI, WC, WHR, and WHtR as anthropometric indices to predict incident hypertension and to assess their associations in a Korean population aged 40 to 69 years.
Methods
Study population
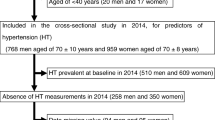
The Korean Genome and Epidemiology Study (KoGES) is an ongoing community-based prospective cohort study of 10,038 participants. It was started in 2001 with the support of the Korean National Institute of Health. A baseline examination was performed on randomly selected participants in 2001–2002 and biennial follow-up examinations were subsequently conducted. The initial 2- and 4-year follow-up data are available to researchers (http://biomi.cdc.go.kr), and we obtained data for all participants from the Centers for Genome Science at the National Institute of Health, Korea. At the 2- and 4-year follow-up examinations, 7,260 participants were eligible in the present study after exclusion of 2,778 subjects who refused to participate or who had died. Of those participants, 7,233 aged 40 to 69 years were selected to participate in a baseline survey. We excluded 2,224 participants with hypertension at baseline. Additionally, 434 participants with previous CVD were excluded. Finally, after those with incomplete data were excluded, 4,454 participants remained eligible for this analysis (Figure 1). The criteria for exclusion based on hypertension at baseline were systolic blood pressure (SBP) ≥140 mmHg, diastolic blood pressure (DBP) ≥90 mmHg, or anti-hypertensive medication use. The study protocol was approved by the Institutional Review Board of the Korean Centers for Disease Control and Prevention.

Flow chart of study participants.
Measurements and surveys
Height and weight were measured (to the nearest 0.1 cm and 0.1 kg, respectively) using a digital stadiometer and scale. BMI (kg/m2) was calculated by dividing weight by height squared. WC was measured three times at the midpoint between the bottom of the ribcage and the top of the iliac crest using a fiberglass tape measure. Hip circumference was measured three times at the point of maximal protrusion of the buttocks; the mean of the three readings was considered the final hip circumference. WHR was calculated as WC divided by hip circumference and WHtR as WC divided by height. Blood pressure was measured in the sitting position after 5 min of rest using a standard mercury sphygmomanometer. Blood samples were obtained after fasting for at least 8 h. Fasting blood glucose, total cholesterol (TC), triglyceride (TG), and high-density lipoprotein cholesterol (HDL-C) levels were measured in a central, certified laboratory (Seoul Clinical Laboratories, Seoul, Republic of Korea). For subjects with TG levels <400 mg/dl, low-density lipoprotein cholesterol (LDL-C) levels were estimated indirectly using the Friedewald formula [20]. The questionnaire included questions on socio-demographic information, lifestyle, personal and family medical history, smoking status, and alcohol consumption. Smoking and alcohol consumption were defined as current smoker and current drinker, respectively.
Definition of hypertension and diabetes mellitus
In the present study, patients with an SBP of ≥140 mmHg or a DPB of ≥90 mmHg, or who used anti-hypertensive medications, were defined as having hypertension. Diabetes mellitus was defined as a fasting blood glucose level of ≥126 mg/dl, a 2-h post-challenge plasma glucose (2 h-PCPG) level of ≥200 mg/dl, an HbA1c level of ≥6.5%, or use of oral hypoglycemic agents [21].
Statistical analysis
Statistical analyses were performed using the SAS software (version 9.2; SAS Institute, Cary, North Carolina) and MedCalc (MedCalc Software, Mariakerke, Belgium). Continuous variables are expressed as the means ± SD, and discrete variables are expressed as counts and proportions. For comparisons between groups, Student’s t-test was used for continuous data and the chi-square test for categorical data. Receiver operating characteristic (ROC) analysis was used to compare discrimination abilities and to determine optimal cut-off values by sexes. Sensitivity (true-positive rate) and specificity (false-negative rate) based on cut-off values for the various anthropometric measurements and the overall discriminatory power of the diagnostic test were calculated using ROC curves. The cut-off points for hypertension were estimated using the maximized Youden index by sexes. The AUC of each obesity marker was compared those of BMI using the DeLong method [22]. We calculated hazard ratios (HRs) by Cox proportional hazard model with adjustment for age, smoking status, alcohol consumption, diabetes and family history of hypertension by sexes. The adjusted HRs are presented with 95% confidence intervals (CIs). The measurement units are different among obesity measures in the present study, so we compared the HRs according to a 1 standard deviation increase in each obesity parameter and criteria for obesity [10,13,23] by sexes. P < 0.05 was considered to indicate statistical significance.
Results
Baseline characteristics of the study subjects
The baseline characteristics of the study population, stratified by sex, are shown in Table 1. The mean age of the study population was 50.33 years in men and 50.21 years in women. The mean BMI was 23.93 kg/m2 in men and 24.36 kg/m2 in women. The mean WC was 82.45 cm in men and 79.88 cm in women. The mean WHR and WHtR were 0.88 and 0.49, respectively, in men and 0.86 and 0.52, respectively, in women. The prevalence of diabetes mellitus was higher in men than in women (6.67% vs. 5.16%, P < 0.032). Approximately 71.01% of the men were drinkers and about 50.19% were current smokers. 28.50% of women were drinkers and only 3.31% were current smokers.
Incidence of hypertension according to anthropometric index categories
During the 4-year follow up, the overall cumulative incidence of hypertension was 18.05% (384 cases, 50.20 cases/1,000 person-years) in men and 16.08% (374 cases, 43.87 cases/1,000 person-years) in women. As shown in Table 2, the number of cases and incidence rate of hypertension significantly increased with increasing anthropometric index values in both sexes.
Cut-off points for the various anthropometric indices for predicting hypertension
Table 3 shows the AROC values and cut-off points for the anthropometric indices for predicting hypertension. In men, the AROC for WC, WHR, and WHtR was 0.62 while the AROC for BMI was 0.58. In women, the AROCs for BMI, WC, WHR, and WHtR were 0.57, 0.66, 0.68, and 0.68, respectively. In both sexes, the AROC for BMI was smaller than the AROC for the central obesity indices. The AROCs for WC, WHR, and WHtR were significantly different (P < 0.01) compared to the AROC for BMI in both sexes. The optimal cut-off points for predicting hypertension using the Youden index were 23.59 kg/m2, 83.33 cm, 0.88, and 0.49 in men and 25.63 kg/m2, 80.37 cm, 0.86, and 0.51, in women for BMI, WC, WHR, and WHtR, respectively.
HRs for hypertension according to anthropometric index
Table 4 shows that the trends were similar among the HRs for each 1-unit increase in standard deviation for each obesity parameter.
The HR for BMI was lower than those for the central obesity markers WC, WHR, and WHtR in their associations with incident hypertension in both sexes.
After adjustment for age, smoking status, alcohol consumption, diabetes and family history of hypertension, anthropometric indices showed no significant associations, but an increasing trend similar to that for the unadjusted model was maintained. Table 5 shows the HRs for incident hypertension according to obesity status defined by anthropometric indices.
After adjustment for risk factors, the hazard ratios for BMI, WC, WHR and WHtR were 1.39, 1.50, 1.40 and 1.49 in men, 1.31, 1.44, 1.35 and 1.48 in women, respectively. In both sexes, the HRs for hypertension according to BMI were lower than those for the anthropometric indices related to central obesity.
Discussion
We analyzed the usefulness of anthropometric indices as predictors of hypertension. In the present study, the AROC for BMI was smaller than that for WC, WHR, and WHtR, suggesting that anthropometric indices that reflect central obesity are better for predicting hypertension in both sexes. Our results are in accordance with previous comparative studies of the association between obesity measures and hypertension [8,24,25]. The HRs for BMI were also lower than those for central obesity indices, with and without adjustment, in both sexes, similar to the AROC results. The discrimination ability of WHtR was similar to that of WC and WHR in our study, however WHtR is more convenient than other anthropometric indices. The sex differences in cut-off points were smaller for WHR and WHtR than for BMI and WC. The result of WHtR was consistent with our previous study which was cross-sectional using data of the Third Korea National Health and Nutrition Examination Survey (KNHANES III) [25]. Unfortunately however, WHR was not included in our previous study. The small sex difference is based on the same standard, which is easy to memorize and consumer-friendly. Ashwell et al. suggest a public message for adults to prevent hypertension: “keep your WC below your half height” [26]. Tseng et al. assert that these characteristics of WHtR also apply to different ethnic groups, which make it convenient for international research [27]. Moreover, WHtR is useful for children, which makes it suitable for long-term follow-up over the lifetime of an individual. Ashwell et al. investigated the relationship between CVD and anthropometric indices by meta-analysis. Discrimination of hypertension using WHtR was 3–4% better than with BMI [28]. On the other hand, WC and WHR have disadvantages. These anthropometric indices do not reflect the height of the subject [7,8]. Hsieh et al. reported that in Japanese men in the third quartile of WC (84.5– < 89 cm) short individuals had a greater risk of hypertension than those who were taller [29]. Moreover, measuring hip circumference is more difficult than measuring WC, and accurately identifying the point of maximal protrusion of the buttocks in obese people is demanding [27,30]. Previous studies reported that the AROC for WHR for hypertension was the lowest among the anthropometric indices [16,27]. Above all, WHR and WC are not consumer-friendly because of the different cut-off points according to sex [8,26,27]. Considering our results and previous studies, WHtR is an affordable screening tool for predicting hypertension in Korean adults. The present study had a number of strengths. Firstly, it used a large population-based sample and a prospective cohort design. Therefore, the causality between anthropometric indices and incident hypertension is clear. Secondly, interviews were conducted by trained interviewers and anthropometric data were obtained by repeated measurement using a standard protocol. These processes may have helped to reduce bias. The fact that dietary intakes and physical activity were not considered in the analysis is a limitation of the present study. These variables were reported to be risk factors for incident hypertension in previous studies [31,32]. Another limitation in present study is that blood pressure is measured during the visit of each follow-up. Repeated blood pressure measurements during two or more visits are recommended by the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) [33].
Conclusions
In conclusion, WHtR can be recommended as a useful screening tool for predicting hypertension because of its high discrimination ability. Moreover, the cut-off points for WHtR for hypertension were similar in both sexes. WHtR is user-friendly and can be converted into a public message.
Abbreviations
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- WHR:
-
Waist-to-hip ratio
- WHtR:
-
Waist-to-height ratio
- KoGES:
-
Korean Genome and Epidemiology Study
- ROC:
-
Receiver operating characteristic
- AROC:
-
Area under the ROC curve
- KSSO:
-
Korean Society for the Study of Obesity
- CVD:
-
Cardiovascular disease
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- 2 h-PCPG:
-
2-h post-challenge plasma glucose
- HRs:
-
Hazard ratios
- CIs:
-
Confidence intervals
- KNHANES:
-
Korea National Health and Nutrition Examination
References
Wang W, Lee ET, Fabsitz RR, Devereux R, Best L, Welty TK, et al. A longitudinal study of hypertension risk factors and their relation to cardiovascular disease: the Strong Heart Study. Hypertension. 2006;47(3):403–9.
Tuan NT, Adair LS, Stevens J, Popkin BM. Prediction of hypertension by different anthropometric indices in adults: the change in estimate approach. Public Health Nutr. 2010;13(5):639–46.
Panagiotakos DB, Chrysohoou C, Pitsavos C, Skoumas J, Lentzas Y, Katinioti A, et al. Hierarchical analysis of anthropometric indices in the prediction of 5-year incidence of hypertension in apparently healthy adults: the ATTICA study. Atherosclerosis. 2009;206(1):314–20.
Korea Centers for Disease Control and Prevention. Korea Health Statistics 2012: Korea National Health and Nutrition Examination Survey (KNHANESV-3). Seoul, Korea: Korean Ministry of Health and Welfare; 2013.
Zhou Z, Hu D, Chen J. Association between obesity indices and blood pressure or hypertension: which index is the best? Public Health Nutr. 2009;12(8):1061–71.
Ko GT, Chan JC, Woo J, Lau E, Yeung VT, Chow CC, et al. Simple anthropometric indexes and cardiovascular risk factors in Chinese. Int J Obes Relat Metab Disord. 1997;21(11):995–1001.
Browning LM, Hsieh SD, Ashwell M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0.5 could be a suitable global boundary value. Nutr Res Rev. 2010;23(2):247–69.
Li WC, Chen IC, Chang YC, Loke SS, Wang SH, Hsiao KY. Waist-to-height ratio, waist circumference, and body mass index as indices of cardiometabolic risk among 36,642 Taiwanese adults. Eur J Nutr. 2013;52(1):57–65.
Hsieh SD, Yoshinaga H. Waist/height ratio as a simple and useful predictor of coronary heart disease risk factors in women. Intern Med (Tokyo, Japan). 1995;34(12):1147–52.
World health Organization Western Pacific Region (WHO-WPR). The Asia-Pacific Perspective: redefining Obesity and its treatment. Melbourne, Australia: Health Communications; 2000.
Deurenberg P, Yap M, van Staveren WA. Body mass index and percent body fat: a meta analysis among different ethnic groups. Int J Obes Relat Metab Disord. 1998;22(12):1164–71.
Chang CJ, Wu CH, Chang CS, Yao WJ, Yang YC, Wu JS, et al. Low body mass index but high percent body fat in Taiwanese subjects: implications of obesity cutoffs. Int J Obes Relat Metab Disord. 2003;27(2):253–9.
Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007;75(1):72–80.
Zaher ZM, Zambari R, Pheng CS, Muruga V, Ng B, Appannah G, et al. Optimal cut-off levels to define obesity: body mass index and waist circumference, and their relationship to cardiovascular disease, dyslipidaemia, hypertension and diabetes in Malaysia. Asia Pac J Clin Nutr. 2009;18(2):209–16.
Dong X, Liu Y, Yang J, Sun Y, Chen L. Efficiency of anthropometric indicators of obesity for identifying cardiovascular risk factors in a Chinese population. Postgrad Med J. 2011;87(1026):251–6.
Gupta S, Kapoor S. Optimal cut-off values of anthropometric markers to predict hypertension in North Indian population. J Community Health. 2012;37(2):441–7.
Gupta S, Kapoor S. Sex differences in blood pressure levels and its association with obesity indices: who is at greater risk. Ethn Dis. 2010;20(4):370–5.
Baik I, Shin C. Optimal waist circumference for the prevention of cardiovascular disease. Korean J Community Nutr. 2010;15(2):275–83.
Choi SJ, Keam B, Park SH, Park HY. Appropriate waist circumference cut-offs to predict diabetes in the Korean population - the Korean Genome and Epidemiology Study. Circ J. 2010;74(7):1357–63.
Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18(6):499–502.
World Health Organization and International Diabetes Fedaration. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation. Geneva, Switzerland: World Health Organization; 2006.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–45.
World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications: report of WHO consultation. Geneva, Switzerland: World Health Organization; 1999.
Hadaegh F, Zabetian A, Sarbakhsh P, Khalili D, James WP, Azizi F. Appropriate cutoff values of anthropometric variables to predict cardiovascular outcomes: 7.6 years follow-up in an Iranian population. Int J Obes (2005). 2009;33(12):1437–45.
Park SH, Choi SJ, Lee KS, Park HY. Waist circumference and waist-to-height ratio as predictors of cardiovascular disease risk in Korean adults. Circ J. 2009;73(9):1643–50.
Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr. 2005;56(5):303–7.
Tseng CH, Chong CK, Chan TT, Bai CH, You SL, Chiou HY, et al. Optimal anthropometric factor cutoffs for hyperglycemia, hypertension and dyslipidemia for the Taiwanese population. Atherosclerosis. 2010;210(2):585–9.
Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13(3):275–86.
Hsieh SD, Yoshinaga H. Do people with similar waist circumference share similar health risks irrespective of height? Tohoku J Exp Med. 1999;188(1):55–60.
World Health Organization. Waist circumference and waist–hip ratio: report of WHO expert consultation. Geneva, Switzerland: World Health Organization; 2008.
Lim NK, Son KH, Lee KS, Park HY, Cho MC. Predicting the risk of incident hypertension in a Korean middle-aged population: Korean genome and epidemiology study. J Clin Hypertens (Greenwich, Conn). 2013;15(5):344–9.
Dyer AR, Elliott P, Shipley M, Stamler R, Stamler J. Body mass index and associations of sodium and potassium with blood pressure in INTERSALT. Hypertension. 1994;23(6 Pt 1):729–36.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560–72.
Acknowledgements
This study was supported by an intramural grant of the National Institute of Health, Korea 4800-4845-302-210(2011-NG63002).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JWL performed the data analysis and wrote the manuscript. NKL advised statistical analyses and interpreted the data. THB contributed discussion and revising the manuscript. SHP developed the idea and participated in drafting the manuscript. HYP contributed to study design and interpreted the data. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Lee, JW., Lim, NK., Baek, TH. et al. Anthropometric indices as predictors of hypertension among men and women aged 40–69 years in the Korean population: the Korean Genome and Epidemiology Study. BMC Public Health 15, 140 (2015). https://doi.org/10.1186/s12889-015-1471-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-015-1471-5