
Abstract
Background
This umbrella review aimed at eliciting good practice characteristics of interventions and policies aiming at healthy diet, increasing physical activity, and lowering sedentary behaviors. Applying the World Health Organization’s framework, we sought for 3 types of characteristics, reflecting: (1) main intervention/policy characteristics, referring to the design, targets, and participants, (2) monitoring and evaluation processes, and (3) implementation issues. This investigation was undertaken by the DEDPIAC Knowledge Hub (the Knowledge Hub on the DEterminants of DIet and Physical ACtivity), which is an action of the European Union’s joint programming initiative.
Methods
A systematic review of reviews and stakeholder documents was conducted. Data from 7 databases was analyzed (99 documents met inclusion criteria). Additionally, resources of 7 major stakeholders (e.g., World Health Organization) were systematically searched (10 documents met inclusion criteria). Overall, the review yielded 74 systematic reviews, 16 position review papers, and 19 stakeholders’ documents. Across characteristics, 25% were supported by ≥ 4 systematic reviews. Further, 25% characteristics were supported by ≥ 3 stakeholders’ documents. If identified characteristics were included in at least 4 systematic reviews or at least 3 stakeholders’ documents, these good practice characteristics were classified as relevant.
Results
We derived a list of 149 potential good practice characteristics, of which 53 were classified as relevant. The main characteristics of intervention/policy (n = 18) fell into 6 categories: the use of theory, participants, target behavior, content development/management, multidimensionality, practitioners/settings. Monitoring and evaluation characteristics (n = 18) were grouped into 6 categories: costs/funding, outcomes, evaluation of effects, time/effect size, reach, the evaluation of participation and generalizability, active components/underlying processes. Implementation characteristics (n = 17) were grouped into eight categories: participation processes, training for practitioners, the use/integration of existing resources, feasibility, maintenance/sustainability, implementation partnerships, implementation consistency/adaptation processes, transferability.
Conclusions
The use of the proposed list of 53 good practice characteristics may foster further development of health promotion sciences, as it would allow for identification of success vectors in the domains of main characteristics of interventions/policies, their implementation, evaluation and monitoring processes.
Similar content being viewed by others


Background
According to the World Health Organization (WHO) low levels of physical activity constitute the fourth leading risk factor for death worldwide and form a key risk factor for non-communicable diseases such as cancer, diabetes, and cardiovascular diseases [1]. Inadequate diet is related to increased likelihood of developing obesity, increased susceptibility to diseases such as diabetes and cardiovascular diseases, reduced immunity, and reduced productivity [1]. Therefore, as suggested by WHO [1] interventions and policies which focus on diet, physical activity, or sedentary behavior are in the main focus of various science disciplines, health organizations, practitioners, and policy makers. Unhealthy diet and physical inactivity are considered among leading causes of the same set the major non-communicable diseases [1], therefore interventions and policies targeting either one of these behaviors or both of them are considered complementary, serving the same overall goals, and they are guided by the same principles for action [1].
Policies constitute of a purposive course of actions to stimulate a healthy diet, physical activity, or to discourage sedentary behavior (defined as the amount of time per day spent sitting, in non-active activities such as watching TV, working at a computer, reading etc.). Policies are formulated in a specific political process; they are adopted, implemented, and enforced by regional, national or international public agencies [2]. In contrast, interventions are actions not yet endorsed, enabled or executed by governments or other public agencies. Interventions may address individuals’ skills, individuals’ beliefs, and contexts such as social systems, physical or build environment, or they may focus on practicing recommended behavior during the intervention sessions. Multilevel and multicomponent interventions may combine these actions and aim at changes at individual, social, and physical environmental levels. Such interventions and policies may have the greatest potential to be effective and thus they may be appealing to practitioners and funding bodies [3]. However, high complexity of interventions and policies hinders identification of the factors responsible for their success.
Good practice characteristics of interventions and polices
Although the number of studies on developing and testing the effects of interventions and policies is growing rapidly, practitioners, policy-makers and researchers indicate difficulties in eliciting factors responsible for a ‘success’ of interventions or policies [4]. ‘Successful’ interventions or policies may be defined as actions that result in significant and sustainable behavior changes and translate behavior change research into real-word settings [5]. Such successful interventions and policies may be characterized by a number of good practice characteristics. These characteristics may include the content of behavior change techniques [6] or aspects of delivery of these techniques [7]. Another line of research stresses that besides the content of an intervention or policy, other characteristics determining ‘successful’ promotion of healthy behaviors may refer to implementation strategies, settings, or integration with local practice [8].
Several conceptual frameworks propose the list of good practice characteristics, defined as characteristics of successful interventions and policies [9,10]. Those lists vary in terms of the range of included characteristics, and in terms of the breadth of the scope. For example, they may focus on specific populations (e.g., children only) [10] or on aspects of implementation (e.g., fidelity to the protocols, consistent delivery) [9]. Although empirical evidence and theoretical developments are accumulating, we found no list of generic characteristics (e.g., non-specific in terms of population, addressing both policies and interventions), which would account for content, evaluation, and implementation aspects.
To identify a good practice characteristic that is typical of ‘successful’ interventions or policies one needs to establish a list of ‘candidate characteristics’ , which have a potential to determine a success. In case of some characteristics, the evidence accumulated in systematic reviews suggests that the presence (or absence) of a characteristic is linked to effects of interventions/policies on diet, physical activity, and sedentary behavior. The development of an evidence-based list of candidate characteristics may serve several aims, namely (1) it may inform the development of new interventions and policies by indicating areas, which should be considered when planning for new interventions/policies; (2) the list may be used as an extended protocol for reporting on interventions and policies; (3) it may promote collection of extended data on characteristics of interventions/policies; collection of these data would enable identifying the essential criteria of successful health promotion.
Reporting and categorizing characteristics of interventions and policies
A progress towards the development and synthesis of interventions and policies is hindered by a lack of widely approved standards of reporting interventions and policies [4]. Existing checklists and protocols for reporting interventions and policies provide some details, but their depth and breadth are limited. The guidelines for reporting are relatively vague, and thus there is not enough information for thorough replications of complex interventions or policies. For example, CONSORT guidelines [11] require reporting “precise details” of the interventions/policies and indicating “how and when they were actually administered”, therefore a very limited description of procedures may fit these standards. To further aid reporting guidelines, Davidson and colleagues [12] suggested that reports of behavior change actions should include details of: (1) the content, (2) characteristics of those delivering the intervention, (3) characteristics of the recipients, (4) settings (e.g., worksite), (5) the mode of delivery, (6) intensity of actions, (7) their duration, and (8) adherence to delivery protocols. Unfortunately, this proposal uses broad constructs; for example it does not specify the type of characteristics of recipients which may be relevant (e.g., minority status, age, beliefs). In sum, these proposals use broad and unspecific characteristics or leave out many characteristics (e.g., implementation, resources [9]) which may determine a success of interventions or polices.
There are several theoretical frameworks which may inform the organization of good practice characteristic. These frameworks tackle the complexity of characteristics, but they usually emphasize either the aspect of content or implementation, or evaluation processes. For example, the Behavior Change Wheel [13] focuses on the content of the interventions or policies, whereas other approaches such as RE-AIM model [9] focus on implementation processes. Another approach to organizing good practice characteristics was recently proposed by WHO [14]. This framework aims at eliciting and classifying good practice characteristics in actions targeting healthy diet and physically active lifestyle. Good practice characteristics were grouped in 3 domains: (1) main intervention/policy characteristics (including the general design, content, main objectives, planned activities, target groups, and stakeholders), (2) monitoring and evaluation (including outcomes, measurement, and process evaluation aspects), and (3) implementation (including performance of implementation, program management, and participation processes). This broad framework was validated in consultations with stakeholders and pilot tests conducted among large-scale program developers [14].
Aims
As the part of the investigation undertaken by the DEDPIAC project (the Knowledge Hub on the DEterminants of DIet and Physical Activity, which is the first Research Action of the European Union’s Joint Programming Initiative on healthy diet for healthy life) [15], the present study aimed at identifying characteristics of interventions and policies promoting healthy diet, physical activity, and a reduction of sedentary behavior. To achieve this target, we performed an umbrella review (i.e., a systematic review of existing reviews) which integrated empirical evidence from existing systematic reviews, position review papers, and stakeholders’ documents. The questions and methods were developed and approved using the rapid review approach [16]. We investigated the presence of attributes of good or recommended practices in policies and interventions targeting the general population, children, and adults. Applying the best practice framework [14], we sought for (1) main intervention/policy characteristics, (2) monitoring and evaluation characteristics, and (3) implementation characteristics.
Methods
Materials and general procedures
We conducted the umbrella review to identify systematic reviews and stakeholders’ documents. In general, systematic reviews and meta-analyses collate empirical evidence that fits pre-specified eligibility criteria, by using explicit, replicable, systematic search, extraction, and evaluation methods that are selected to minimize biases [17]. Umbrella reviews represent a way of synthesizing the evidence accumulated in systematic reviews and making them suitable for a more general audience of healthcare practitioners [18-20]. Although typical umbrella reviews focus on analyzing materials obtained from systematic reviews [17,18], the aim of this study required integrating the evidence presented in reviews (both systematic and non-systematic position reviews) with practice recommendations issued by major stakeholders.
In order to elicit the good practice characteristics 3 types of documents were analyzed. First, we searched for systematic reviews analyzing characteristics of policies/interventions, and forming recommendations about these characteristics. Second, we searched for position papers that offered a comprehensive review of research evidence supporting good practice characteristics, but did not apply methods of systematic reviews. Finally, we searched for peer-reviewed and non-peer-reviewed documents, issued by major national and international stakeholders. We investigated documents aiming at eliciting evidence-based good practice criteria or providing practice recommendations for interventions/policies targeting healthy diet, physical activity, or sedentary behaviors.
Peer-reviewed documents: search strategy, inclusion, and exclusion criteria
The search was conducted in Medline, Cochrane Database of Systematic Reviews, PsycINFO, PsychArticles, Health Source: Nursing/Academic Edition, Academic Premier, and ScienceDirect databases. Documents published between the inception of databases and February 2014 were included. Combinations of 4 groups of keywords were applied, referring to: (1) practice characteristics (“good practic*” or “best practic*” or “recommended practic*” or “recommended strateg*”), (2) the type of action (intervention or polic*), (3) the design (“systematic review” or review or meta-analys*), (4) diet, physical activity, or sedentary behavior-related outcomes (“physical activity” or active or exercise or sedentary or diet or nutrition or fat or snack or fruit or vegetable or fiber or fibre or soda or meal or food or “energy intake” or calorie* or obes*).
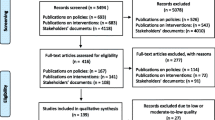
Figure 1 (right panel) presents the stages of the data selection process. The preliminary search yielded 1926 entries, which used a combination of keywords from all 4 categories in either title, or the abstract, or keywords. Identified abstracts were then screened by 2 researchers (KH and AL), and 801 potentially relevant studies were identified.

The flow chart: Selection processes for stakeholders’ documents (left panel) and reviews (right panel).
The researchers (KH and AL) then selected publications that appeared in peer-reviewed English language journals. The following documents were excluded: (a) dissertations, protocols, conference materials, and book chapters; (b) reviews which indicated a need for testing good practice characteristics, but did not investigate such characteristics in the Results sections; (c) documents analyzing interventions or policies focusing on other main outcomes than physical activity, sedentary behaviors or diet. For example, interventions could target prevention or treatment of osteoporosis; such interventions could account for physical activity or diet (listed among multiple behaviors requiring change) but the content, evaluation, and implementation characteristics of such interventions were specific for their respective main outcomes (e.g., focusing on characteristics of prior treatment, current medication, health maintenance organizations); (d) publications aiming at eliciting practice characteristics in multi-behavior interventions/polices, which did not distinguish characteristics specific for either dietary or physical activity or sedentary behaviors; (e) documents which were reviewing guidelines for diet/physical activity/sedentary behaviors, but did not indicate characteristics of interventions/policies; (f) publications which discussed only one example of a policy or intervention.
In case of systematic reviews we included systematic reviews of quantitative studies (criteria for systematic reviews: clearly defined study aims, search strategy, inclusion and exclusion criteria, design of original studies, a suitable synthesis given the heterogeneity of findings [17]). In case of non-systematic position reviews, papers focusing on eliciting evidence-based good practices were included. Regarding peer-reviewed stakeholder’s documents, we included papers indicating a major professional organization (e.g., American Dietetic Association) among the authors or in the title. If several position review papers were prepared by the same authors and dealt with the same original trials, we included the most recent document, and sought for other (distinct) characteristics in earlier documents. Further, manual searches of the reference lists were conducted.
Quality assessment of each systematic review was conducted using the Methodological Quality Checklist (MQC) [18]. It is a 7-item scale with total scores ranging from 0 to 7. MQC evaluates strategies applied in original reviews and accounts for 7 quality criteria: (1) well-defined study participants, intervention, and outcomes; (2) search strategy is defined, combining several databases and other strategies of reference checking; (3) transparent inclusion and exclusion criteria; (4) designs of original studies and the number of studies are clarified; (5) quality assessment of original studies is included; (6) methods of data synthesis is specified and it accounts for data heterogeneity; and (7) at least 2 researchers are involved at each stage of review process. Two researchers (KH and AL) rated all systematic reviews independently. Previous umbrella reviews using MQC applied the cutoff of 4 as representing moderate or high quality [19,20] and included research which scored ≥ 4 in MQC. Therefore, only systematic reviews scoring ≥ 4, were included into the final analyses.
Because there are no widely used measures of quality evaluation of stakeholders’ documents or non-systematic reviews, we have developed a tool serving this purpose (the Methodological Quality Checklist for Stakeholder Documents and Position Papers, MQC-SP; see Additional file 1). It was based on criteria applied in MQC [18], with a 6-item scale and total scores ranging from 0 to 6. Two researchers (KH and AL) independently rated all peer-reviewed stakeholders’ documents and position review papers. Only papers scoring ≥ 4, representing moderate or high quality, were included into analyses.
For all 3 types of analyzed documents the concordance of quality evaluations was high. The values of kappa coefficient were ranging from .89 (p < .01) to 1.00 (p < .001).
Overall, 99 peer reviewed papers met all inclusion and exclusion criteria. They included 74 systematic reviews, 16 position papers based on a review of empirical evidence, and 9 stakeholders’ documents, published in peer-reviewed journals.
Stakeholders’ documents (other than peer-reviewed): search strategy, inclusion criteria, exclusion criteria, and quality evaluation
Besides identifying the stakeholders’ documents that were published in peer-reviewed journals, we searched for documents published directly by the stakeholders. To obtain major stakeholders’ documents aiming at good practice recommendations, a group of 5 experts used the consensus method [17] to select the stakeholders. The inclusion criteria were: (1) the international or national stakeholder using English language to issue the documents (i.e., developing documents available to researchers, policy makers, and practitioners around the world); (2) the stakeholder issues documents that provide evidence-based good practice recommendations for policies and interventions targeting any populations; (3) the stakeholder develops documents which refer to diet, physical activity, or sedentary behavior as the main outcome of the interventions/policies. Similar inclusion criteria were used in previous reviews of stakeholders’ documents [21]. The following stakeholders were included: European Commission (EC), National Institute for Health and Clinical Excellence (NICE; United Kingdom), World Health Organization, Regional Office for Europe (WHO), Centers for Disease Control and Prevention (CDC; USA), Institute of Medicine (IOM; USA), Australian Department of Health (ADH), and National Health and Medical Research Council (NHMRC; Australia). All websites of respective stakeholders were searched using the same keywords as in the search of the databases. Using a search engine (Google) further attempts to elicit potential documents were undertaken. The sets of keywords used in the databases search were applied, accompanied by the names of the stakeholder organization (or its acronym). Only documents that were available for downloading were included. The initial search resulted in identifying 8279 links to potentially relevant documents (see Figure 1, left panel).
In the next step, the titles of these potentially relevant documents were screened and the documents with titles that appeared relevant for the present umbrella review were further reviewed. We included documents which aimed at (1) reviewing good practices or (2) providing an overview of characteristics of good practices, or (3) formulating practice recommendations in interventions or policies promoting healthy diet, physical activity, or a reduction of sedentary behavior. Only documents developed (or officially endorsed) by a respective stakeholder were included. Documents were excluded if they presented selected examples of good practice in interventions/policies or if they did not focus on the characteristics of interventions/policies. Moreover, we excluded documents aiming at interventions or policies focusing on other main outcomes than physical activity, sedentary behaviors or diet (e.g., osteoporosis prevention). These steps were conducted by 2 researchers (MH and MvdB).
Next, the quality of the documents was evaluated. The quality criteria were based on MQC criteria [18], with a 6-item scale and total scores ranging from 0 to 6 (see Additional file 1). Two researchers (MH, MvdB) independently rated all stakeholders’ documents. Papers scoring ≥ 4, that is representing high or moderate quality, were included into the further analyses. The concordance of the quality evaluation was very high, with κ = 1.00, p < .001.
Overall, we obtained 15 non-peer-reviewed stakeholder documents, meeting all inclusion criteria. However, 5 out of 15 documents presented a major overlap with another document issued by the same stakeholder; such documents were excluded (i.e., the excluded document did not report any additional practices compared to the included document). Thus, 10 documents were used for further analyses.
Data extraction, coding, and synthesis
To ensure accuracy and consistency of data extraction and coding at least 2 researchers extracted and coded data independently. Any disagreements in the processes of data selection and abstraction were resolved by the consensus method (searching for possible rating errors, followed by a discussion and arbitration by a third researcher) [17].
Descriptive data was extracted by one researcher (KH or MH) and then verified by the second researcher (AL). Extracted data included: (1) the descriptive characteristics of the original studies (e.g., participants, target behavior), synthesized in the analyzed reviews and stakeholders’ documents; (2) data necessary for quality evaluation. These descriptive characteristics and quality evaluations are presented in Additional file 1.
Next, the intervention and policy characteristics were extracted. Each document was searched for good practice characteristics. In particular, we retrieved the names of characteristics (as documented by authors of original documents) and their operationalization or definition (e.g., an explanation of the function of a characteristic within the context of development, implementation, and evaluation of policies and interventions). In case of systematic reviews these characteristic had to be included in the original analysis (as a significant determinant or as a moderator) as well as into original conclusions of the review. In case of stakeholders’ documents and position review papers, attributes of intervention/policies listed in the respective documents were coded as good practice characteristics if they were indicated as crucial for the development, implementation, and evaluation of any interventions or policies targeting healthy diet and physically active lifestyle.
The good practice characteristics that had an equivalent operationalization but different original names were considered to represent the same construct (e.g., accounting for cultural customs and addressing ethnic minority values). If an original document used a broad name for a characteristic (e.g., costs) we elicited a functional definition applied in the original document (e.g., total costs, cost per participants, cost per a unit of behavior change), and the broader characteristic was divided into separate units, reflecting its functional definition. The findings are presented using definitions as presented by the authors of the original documents (see Additional file 1). Interventions and policies aiming at any type of physical activity (general levels of physical activity or its specific types, such as walking) or a reduction of sedentary behavior were coded as referring to physical activity. Only 4 documents addressed sedentary behaviors, therefore these behaviors and physical activity were combined into one category. Similarly, interventions and policies targeting narrowly defined dietary behaviors (e.g., a reduction of snacking) as well as addressing more complex dietary changes (e.g., a meal composition) were coded as referring to dietary behavior.
The characteristics were allocated into 3 domains proposed by the WHO [14]. They were considered as representing (1) main intervention/policy characteristics, (2) monitoring and evaluation processes, or (3) implementation issues. The allocation was conducted by 2 researchers (KH, MH) and verified by a third researcher (AL).
Next, characteristics within each domain were combined into broader categories. Two researchers (KH, AL) independently clustered all identified characteristics into categories. The names of categories and characteristics were then independently evaluated by the 3 researchers (MH, MvdB, GR) who searched for flaws in categorization and evaluated the meaningfulness of categories and characteristics.
Finally, the characteristic was categorized as a good practice characteristic if the respective characteristic was indicated in either at least 4 systematic reviews or in at least 3 stakeholders’ documents. This threshold is based on the number of documents supporting each characteristic and it represents the top quartile in the number of the supporting systematic reviews and stakeholders’ documents, respectively. To reach this threshold, the number of documents supporting a characteristic had to fall into the respective upper quartile: across characteristics, 75% were supported by 0–3 systematic reviews, whereas 25% were supported by at least 4 systematic reviews. Further, 75% characteristics were indicated in 0–2 stakeholder documents, whereas only 25% were indicated in at least 3 stakeholders’ documents (see Additional file 1). This arbitrary inclusion threshold was obtained in a consensus meeting by 3 research groups, represented by the researchers from 3 countries, involved in DEDIPAC project. The upper quartile-based thresholds are used in health promotion research eliciting good practice examples [22]. The threshold applied in the present study was considered as indicating strong support in analyzed data.
All good practice characteristic listed in Tables 1, 2, 3, 4 met this threshold (was supported by either at least 4 systematic reviews or by at least 3 stakeholders’ documents); 96 remaining characteristics (see Additional file 1) fell below the threshold and therefore were not included into the final list of best practice characteristics. For example, a good practice characteristic referring to the identification of environmental barriers and resources for participation was supported by 2 documents and therefore it was excluded from the final list.
Results
Description of analyzed material
The final selection included 74 systematic reviews (67.9%), 19 stakeholders’ documents (17.4%) and 16 position review papers (14.7%). Systematic reviews investigated a total of 2989 original studies. Populations analyzed in original papers included: general population samples (k = 31, 28.4%), children (k = 21, 19.4%), adolescents (k = 2, 1.8%), children and adolescents (k = 13, 11.9%), adults (k = 14, 12.8%), adults with a chronic disease, including cardiovascular or neurological diseases, diabetes, depression, obesity (k = 15, 13.8%), pregnant women (k = 1, 0.9%), adults at workplace (k = 6, 5.5%), older adults (k = 5, 4.7%), and vulnerable populations, such as ethnic minorities (k = 1, 0.8%). Three documents focused on women only. The majority of documents (k = 64, 58.7%) provided recommendations which could be applied both in policies and interventions, 39 (35.8%) formulated recommendations for interventions only; 6 (5.5%) focused on policy only. The majority referred to both physical activity and dietary behaviors (k = 62, 56.9%), whereas 36 (33%) analyzed dietary behaviors only and 11 (10.1%) addressed physical activity/sedentary behaviors only. The majority of documents (k = 97; 89%) referred to multi-level interventions and policies (i.e., using techniques aiming at a change at individual and social/environmental levels). Additional file 1 yields a description of original documents.
Quality of papers included into analysis ranged from moderate to minimal flaws (see Additional file 1). For systematic reviews, MQC scores ranged from 4 to 7, M = 5.50, SD = 0.93. In case of stakeholders’ documents and position review papers the scores for MQC-based measure ranged from 4 to 6, M = 4.68, SD = 0.60.
Good practice attributes
Regarding main intervention/policy characteristics, we identified 40 good practice characteristics that were reported in at least one document (see Additional file 1). The characteristics were grouped into 6 distinct categories: the use of theory (n = 1), participants, (n = 6), target behavior (n = 6), content development and content management (n = 16), multidimensionality of interventions/ policies (n = 4), practitioner and setting contexts (n = 7).
Strong support was found for 18 good practice characteristics. They were reported in at least 4 systematic reviews or at least 3 stakeholders’ documents and thus coded as good practice characteristics (Table 1). The list of main intervention/policy characteristics includes: 1 attribute referring to the use of theory, 3 for participants, 1 for target behavior, 9 for content development and content management, 2 for multidimensionality of intervention/policy, and 2 for practitioner and setting contexts (Table 1). The majority of good practice characteristics (17 out of 18) were generic, that is they were indicated in documents referring to both diet and physical activity/sedentary behavior, referred to different age groups, interventions, and policies (see Additional file 1). The exception is ‘family involvement’, a characteristic referring to interventions and policies targeting children and adolescents only.
The analysis of original documents yielded 37 monitoring and evaluation characteristics of good practice (see Additional file 1). The characteristics were grouped into 6 categories: costs and funding (n = 5), outcomes (n = 11), the evaluation of effects: time and effect size (n = 6), reach (n = 5), the evaluation of participation and generalizability (n = 6), underlying processes and active components (n = 4).
Strong support was found for 18 good practice characteristics (Table 2), which represent the attributes of good practice referring to processes of monitoring and evaluation. They were indicated in at least 3 stakeholders’ documents or 4 systematic reviews. The list of good practice characteristics referring to monitoring and evaluation includes: 3 attributes referring to costs and funding, 5 for outcomes, 3 for the evaluation of effects: time and effect size, 3 for reach, 2 for the evaluation of participation and generalizability, and 2 for processes and active components. All 18 characteristics in the monitoring/evaluation domain were generic: they were found in documents referring to diet and physical activity/sedentary behavior, different age groups, interventions, and policies.
Finally, we identified 72 implementation good practice characteristics (see Additional file 1). They included: participation processes (n = 13), training for practitioners (n = 4), the use/integration of existing resources (n = 18), feasibility (n = 4), maintenance and sustainability (n = 8), partnership for implementation (n = 7), implementation consistency and adaptation processes (n = 13), and transferability (n = 5).
In contrast to findings for other domains (main characteristics and evaluations/processes), the majority of implementation characteristics (72%) was endorsed by less than 3 documents (Additional file 1). Only 17 met the threshold of strong support; only these characteristics were included into the final list of good practice characteristics. The final list includes: 3 attributes for participation processes, 1 for training for practitioners, 3 for use/integration of existing resources, 2 for feasibility, 2 for maintenance and sustainability, 2 for partnership for implementation, 2 for implementation consistency and adaptation processes, and 2 for transferability (see Table 3). The vast majority of good practice characteristics referring to implementation (16 out of 17) were generic. The exception was ‘adherence to protocol/protocol fidelity monitoring’ characteristic which was indicated in documents analyzing interventions, but not policies.
In sum, data synthesis yielded 149 good practice characteristics, referring to policies and interventions aiming at healthy diet and physical activity/sedentary behaviors. We found stronger support for 53 good practice characteristics, of which 51 are generic. The list of good practice characteristics was combined into a checklist (Table 4), which may be used for developing practice and reporting research on interventions and policies.
Discussion and conclusions
This study provides an insight into good practice characteristic in interventions and policies targeting healthy diet, physical activity, and sedentary behavior in various populations. We identified 53 good practice attributes (51 generic), falling into 3 broad domains proposed by WHO [14]: main characteristics, monitoring/evaluations, and implementation. Across these domains, a similar number of characteristics of good practice was identified (18, 18, and 17, respectively), which may be an indicator of equivalent relevance of 3 domains.
Our efforts to identify characteristics which are evidenced and practice-based characteristics were undertaken in a response to concerns and appeals of practitioners, researchers, and editors which indicate difficulties in replicating and applying interventions/policies in various populations, because research reports present limited detail [4,7]. Compared to other lists [4,12] which serve similar purposes, the list of good practice characteristics developed in the present umbrella review was not restricted to the one domain of main descriptive intervention or policy characteristics, but also emphasizes the important domains of implementation and evaluation.
The list of 53 potentially crucial practice characteristics may be seen as a point of departure for further syntheses. The list might be shortened if future research would provide evidence for a lack of relevance of some characteristics for the success of interventions/policies. Until then, this broad list has a potential to inspire accumulating more detailed data and, in consequence, it would allow for identifying characteristics responsible for a success of interventions/policies.
The findings indicated that the majority of the 53 characteristics were endorsed by researchers as well as stakeholders, responsible for issuing practice recommendations. So far research on practice attributes reviewed either peer-reviewed studies [20,23] or stakeholders’ guidelines [21]. Combining 2 types of sources reinforces the conclusions. The list proposed in the present study integrates findings and concerns of researchers, practitioners, and those responsible for developing practice guidelines.
In sum, the list of good practice characteristics provides a comprehensive overview of specific aspects of potentially successful interventions and policies. Researchers, practitioners and policy makers may account for those characteristics when planning, developing, and reporting interventions and policies promoting healthy diet and physical activity. Compared to other lists of guidelines for reporting interventions/policies, the present list is based on a systematic review of empirical evidence and stakeholders’ proposals, therefore it may be feasible not only for researchers, but also for practitioners who need to apply the guidelines formed by major national stakeholders. Further, compared to other proposals, our list does not focus on broad categories e.g. [8], which may be difficult to translate into practice, but on specific, narrowly defined characteristic. Based on existing evidence it may be assumed that accounting for these characteristics increases the likelihood of developing a successful policy or intervention.
We analyzed characteristics indicated in position papers, which presented attributes of practice based on non-systematic reviews of literature. Although those papers were of relatively high quality, the support for a practice characteristic found in this type of documents was not used as a criterion for including the characteristic into the final list of attributes of good practice. A relatively small number of characteristics from the preliminary list (18 out of 149) was supported solely by position papers. It has to be noted, that in the domain of implementation the number of characteristics indicated in position papers only was twice as high as in 2 remaining domains. Therefore, future research investigating implementation practices should explore evidence accumulated in systematic and non-systematic reviews.
Our study has several limitations. The proposed list of good practice characteristics is based on an umbrella review of reviews and stakeholders’ documents. Thus, some recent studies on good practice characteristics were not included. Furthermore, the present study did not differentiate between target groups (e.g., adults versus children) and it is possible that some good practice characteristics are more relevant for some target groups than for others. Additionally, we combined evidence for good practice characteristics for policies and interventions. Although 52 out of 53 characteristics were supported in documents referring to both interventions and policies, future research should investigate if attributes of good practices are different for policies and for interventions. The decision to define characteristics as the attributes of good practice was based on an arbitrary criterion (i.e. the number of documents supporting the characteristic had to fall into the upper quartile for the number of either systematic reviews or stakeholders’ documents), which was chosen by a consensus method [17]. As indicated, the quartile-based thresholds are used in health promotion research eliciting good practice examples [22]. The main limitation of this approach refers to the fast progress in accumulation of the evidence: as new systematic reviews and stakeholders’ documents are published every year, the characteristic that just missed the threshold may fit the criteria of good practice characteristics very soon. Further, with growing evidence the threshold may need to be changed as a different number of documents would represent the upper quartile. Therefore, as new evidence is accumulating, this list should be updated regularly. Finally, the evaluation of the quality of the material included in the present study was based on criteria which were relatively lenient. In sum, all conclusions should be treated with caution and the proposed list of characteristics is preliminary.
In conclusion, our study provides a broad list of good practice characteristics in interventions and policies targeting healthy diet and physical activity. Research aiming at defining successful interventions and policies may need to report the presence (and, where feasible, the content) of those characteristics. The use of the proposed list of good practice characteristics may foster further development of health promotion sciences, as it would allow for identification of success vectors in the domains of main characteristics of interventions/policies, their implementation, evaluation and monitoring processes.
Abbreviations
- DEDIPAC:
-
The Knowledge Hub on the DEterminants of DIet and Physical ACtivity
- MQC:
-
Methodological Quality Checklist
References
World Health Organization: Global strategy on diet, physical activity and Health: Physical activity. WHO 2014. [http://www.who.int/dietphysicalactivity/pa/en/]
European Union: White Paper: A Strategy for Europe on Nutrition, Overweight and Obesity related health issues. COM279 final. EU 2007. [http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=COM:2007:0279:FIN:EN:PDF]
Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet. 2012;380(9838):272–81.
Abraham C, Johnson BT, de Bruin M, Luszczynska A. Enhancing reporting of behavior change intervention evaluation. J Acquir Immune Defic Syndr. 2014;66 Suppl 3:S293–299.
Ory MG, Jordan PJ, Bazzarre T. The Behavior Change Consortium: setting the stage for a new century of health behavior-change research. Health Educ Res. 2002;17(5):500–11.
Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28(6):690–701.
Peters GJP, de Bruin M, Crutzen R: Everything should be as simple as possible, but no simpler: towards a protocol for accumulating evidence regarding the active content of health behaviour change interventions, Health Psych Rev 2013. doi:10.1080/17437199.2013.848409.
Glasgow RE, Emmons KM. How can we increase translation of research into practice? Types of evidence needed. Annu Rev Public Health. 2007;28(1):413–33.
Green LW, Glasgow RE. Evaluating the relevance, generalization, and applicability of research: issues in external validation and translation methodology. Eval Health Prof. 2006;29(1):126–53.
Khan LK, Sobush K, Keener D, Goodman K, Lowry A, Kakietek J, et al. Recommended community strategies and measurements to prevent obesity in the United States. MMWR Recomm Rep. 2009;58(RR-7):1–26.
Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, the CONSORT Group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Ann Intern Med. 2008;148(4):295–309.
Davidson KW, Goldstein M, Kaplan RM, Kaufmann PG, Knatterud GL, Orleans CT, et al. Evidence-based behavioral medicine: what is it and how do we achieve it? Ann Behav Med. 2003;26(3):161–71.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
World Health Organization. Good practice appraisal tool for obesity prevention programmes, projects, initiatives and interventions. Copenhagen, Denmark: World Health Organization; 2011. EUR/10/ EUDHP1003966/ 3.
Lakerveld J, van der Ploeg HP, Kroeze W, Ahrens W, Allais O, Andersen LF, et al. Towards the integration and development of a cross European research network and infrastructure: The DEterminats of Diet and Physical Activity (DEDIPAC) Knowledge Hub. 2014. Int J of Behav Nutr Phys Act. 2014;11:143.
Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: the evolution of a rapid review approach. Syst Rev. 2012;1:10.
Higgins J, Green S. Cochrane Handbook For Systematic Reviews Of Interventions. Chichester, UK: Wiley; 2008.
Bambra C, Gibson M, Sowden AJ, Wright K, Whitehead M, Petticrew M. Working for health? Evidence from systematic reviews on the effects of health and health inequalities of organizational changes to the psychosocial work environment. Prev Med. 2009;48(5):454–61.
Cislak A, Safron M, Pratt M, Gaspar T, Luszczynska A. Family-related predictors of body weight and weight-related behaviors among children and adolescents: a systematic umbrella review. Child Care Health Dev. 2012;38(3):321–31.
Safron M, Cislak A, Gaspar T, Luszczynska A. Micro-environmental characteristics related to body weight, diet, and physical activity of children and adolescents: a systematic umbrella review. Int J Environ Health Res. 2011;21(5):317–30.
Richardson L, Paulis WD, van Middelkoop M, Koes BW. An overview of national clinical guidelines for the management of childhood obesity in primary care. Prev Med. 2013;57(5):448–55.
Brener ND, Wechsler H, McManus T. How school healthy is your state? A state-by-state comparison of school health practices related to a healthy school environment and health eductation. J Sch Health. 2013;83(10):743–9.
Dombrowski SU, Sniehotta FF, Avenell A, Johnston M, MacLennan G, Araújo-Soares V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychol Rev. 2012;6:7–32.
Ajie WN, Chapman-Novakofski KM. Impact of computer-mediated, obesity-related nutrition education interventions or adolescents: a systematic review. J Adolesc Health. 2014;54(6):631–45.
Avery KN, Donovan JL, Horwood J, Lane JA. Behavior theory for dietary interventions for cancer prevention: a systematic review of utilization and effectiveness in creating behavior change. Cancer Causes Control. 2013;24(3):409–20.
Besculides M, Zaveri H, Hanson C, Farris R, Gregory-Mercado K, Will J. Best practices in implementing lifestyle interventions in the WISEWOMAN program: adaptable strategies for public health programs. Am J Health Promot. 2008;22(5):322–8.
Bock C, Jarczok MN, Litaker D. Community-based efforts to promote physical activity: a systematic review of interventions considering mode of delivery, study quality and population subgroups. J Sci Med Sport. 2013;17(3):276–82.
Bossen D, Veenhof C, Dekker J, de Bakker D. The effectiveness of self-guided web-based physical activity interventions among patients with a chronic disease: a systematic review. J Phys Act Health. 2014;11(3):665–77.
Flynn MA, McNeil DA, Maloff B, Mutasingwa D, Wu M, Ford C, et al. Reducing obesity and related chronic disease risk in children and youth: a synthesis of evidence with 'best practice' recommendations. Obes Rev. 2006;7 Suppl 1:7–66.
Golley RK, Hendrie GA, Slater A, Corsini N. Interventions that involve parents to improve children's weight-related nutrition intake and activity patterns - what nutrition and activity targets and behaviour change techniques are associated with intervention. Obes Rev. 2011;12(2):114–30.
Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health. 2011;11:119.
Hamel LM, Robbins LB. Computer‐ and web‐based interventions to promote healthy eating among children and adolescents: a systematic review. J Adv Nurs. 2013;69(1):16–30.
Hardeman W, Griffin S, Johnston M, Kinmonth AL, Wareham NJ. Interventions to prevent weight gain: a systematic review of psychological models and behaviour change methods. Int J Obes Relat Metab Disord. 2000;24(2):131–43.
Hendrie GA, Brindal E, Corsini N, Gardner C, Baird D, Golley RK. Combined home and school obesity prevention interventions for children: what behavior change strategies and intervention characteristics are associated with effectiveness? Health Educ Behav. 2012;39(2):159–71.
Husebø AM, Dyrstad SM, Søreide JA, Bru E. Predicting exercise adherence in cancer patients and survivors: a systematic review and meta-analysis of motivational and behavioural factors. J Clin Nurs. 2013;22(1–2):4–21.
Lee LL, Watson MC, Mulvaney CA, Tsai CC, Lo SF. The effect of walking intervention on blood pressure control: a systematic review. Int J Nurs Stud. 2010;47(12):1545–61.
Nixon CA, Moore HJ, Douthwaite W, Gibson EL, Vogele C, Kreichauf S, et al. Identifying effective behavioural models and behaviour change strategies underpinning preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: a systematic review. Obes Rev. 2012;13 Suppl 1:106–17.
Prestwich A, Sniehotta FF, Whittington C, Dombrowski SU, Rogers L, Michie S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014;33(5):465–74.
Rabin BA, Glasgow RE, Kerner JF, Klump MP, Brownson RC. Dissemination and implementation research on community-based cancer prevention: a systematic review. Am J Prev Med. 2010;38(4):443–56.
Thomson CA, Ravia J. A systematic review of behavioral interventions to promote intake of fruit and vegetables. J Am Diet Assoc. 2011;111(10):1523–35.
Tierney S, Mamas M, Woods S, Rutter MK, Gibson M, Neyses L, et al. What strategies are effective for exercise adherence in heart failure? A systematic review of controlled studies. Heart Fail Rev. 2012;17(1):107–15.
Webb TL, Joseph J, Yardley L, Michie S. Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res. 2010;12(1):e4.
American Dietetic Association, Society for Nutrition Education, American School Food Service Association. Position of the American Dietetic Association, Society for Nutrition Education, and American School Food Service Association—Nutrition services: an essential component of comprehensive school health programs. J Am Diet Assoc. 2003;103(4):505–14.
Dubois N, Jetha N, Robinson K, Szuto I, Wan G, Wilkerson T: Canadian best practices initiative methodology background paper. 2008. [http://seniorspolicylens.ca/Root/Materials/Adobe%20Acrobat%20Materials/CBPI-methodology.pdf]
Netherlands Centre Youth Health (NCJ), Netherlands Institute for Sport and Physical Activity (NISB), Netherlands Youth Institute (NJi), RIVM Centre for Healthy Living (CGL): Dutch Recognition System for Interventions criteria for joint quality assessment 2013–2018. 2013. [http://loketgezondleven.nl/object_binary/o16954_Recognition-system-Criteria-2013-2018.pdf]
Stockley L. Toward public health nutrition strategies in the European Union to implement food based dietary guidelines and to enhance healthier lifestyles. Public Health Nutr. 2001;4(2A):307–24.
Gillison F, Greaves C, Stathi A, Ramsay R, Bennett P, Taylor G, et al. Waste the waist’: the development of an intervention to promote changes in diet and physical activity for people with high cardiovascular risk. Br J Health Psychol. 2012;17(2):327–45.
McNeil DA, Flynn MA. Methods of defining best practice for population health approaches with obesity prevention as an example. Proc Nutr Soc. 2006;65(4):403–11.
Summerbell CD, Moore HJ, Vögele C, Kreichauf S, Wildgruber A, Manios Y, et al. Evidence-based recommendations for the development of obesity prevention programs targeted at preschool children. Obes Rev. 2012;13 Suppl 1:129–32.
Biddle SJ, Petrolini I, Pearson N. Interventions designed to reduce sedentary behaviours in young people: a review of reviews. Br J Sports Med. 2014;48(3):182–6.
Brown DR, Soares J, Epping JM, Lankford TJ, Wallace JS, Hopkins D, et al. Stand-alone mass media campaigns to increase physical activity: a Community Guide updated review. Am J Prev Med. 2012;43(5):551–61.
Ghisi GL, Abdallah F, Grace SL, Thomas S, Oh P. A systematic review of patient education in cardiac patients: Do they increase knowledge and promote health behavior change? Patient Educ Couns. 2014;95(2):160–74.
Klesges LM, Williams NA, Davis KS, Buscemi J, Kitzmann KM. External validity reporting in behavioral treatment of childhood obesity: a systematic review. Am J Prev Med. 2012;42(2):185–92.
Latimer AE, Brawley LR, Bassett RL. A systematic review of three approaches for constructing physical activity messages: What messages work and what improvements are needed? Int J Behav Nutr Phys Act. 2010;7:36.
Marsh S, Foley LS, Wilks DC, Maddison R. Family-based interventions for reducing sedentary time in youth: a systematic review of randomized controlled trials. Obes Rev. 2014;15(2):117–33.
Salmon J, Booth ML, Phongsavan P, Murphy N, Timperio A. Promoting physical activity participation among children and adolescents. Epidemiol Rev. 2007;29:144–59.
Taylor NF, Dodd KJ, Shields N, Bruder A. Therapeutic exercise in physiotherapy practice is beneficial: a summary of systematic reviews 2002–2005. Aust J Physiother. 2007;53(1):7–16.
van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. 2007;335(7622):703.
Vuillemin A, Rostami C, Maes L, Van Cauwenberghe E, Van Lenthe FJ, Brug J, et al. Worksite physical activity interventions and obesity: a review of European studies (the HOPE project). Obes Facts. 2011;4(6):479–88.
Christiansen NV, Kahlmeier S, Racioppi F. Sport promotion policies in the European Union: results of a contents analysis. Scand J Med Sci Sports. 2014;24(2):428–38.
King L, Gill T, Allender S, Swinburn B. Best practice principles for community-based obesity prevention: development, content and application. Obes Rev. 2011;12(5):329–38.
Dixey R, Heindl I, Loureiro I, Pérez-Rodrigo, Snel J, Warnking P: Healthy eating for young people in Europe. A school-based nutrition education guide.1999. [http://www.euro.who.int/__data/assets/pdf_file/0005/119921/E69846.pdf]
World Health Organization: Physical activity promotion in socially disadvantaged groups: principles for action. PHAN Work Package 4 Final Report. WHO, 2013. [http://www.euro.who.int/__data/assets/pdf_file/0005/185954/E96817eng.pdf]
Ayliffe B, Glanville NT. Achieving healthy body weight in teenagers: evidence-based practice guidelines for community nutrition interventions. Can J Diet Pract Res. 2010;71(4):205.
De Meester F, van Lenthe FJ, Spittaels H, Lien N, De Bourdeaudhuij I. Interventions for promoting physical activity among European teenagers: a systematic review. Int J Behav Nutr Phys Ac. 2009;6:82.
Edwardson CL, Gorely T. Parental influences on different types and intensities of physical activity in youth: a systematic review. Psychol Sport Exerc. 2010;11(6):522–35.
Katz DL, O'Connell M, Njike VY, Yeh MC, Nawaz H. Strategies for the prevention and control of obesity in the school setting: systematic review and meta-analysis. Int J Obes. 2008;32(12):1780–9.
Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. 2011;45(11):923–30.
Niemeier BS, Hektner JM, Enger KB. Parent participation in weight-related health interventions for children and adolescents: a systematic review and meta-analysis. Prev Med. 2012;55(1):3–13.
American Dietetic Association (ADA). Position of The American Dietetic Association: dietary guidance for healthy children aged 2 to 11 years. J Am Diet Assoc. 1999;99(1):93–101.
American Dietetic Association (ADA). Position of the American Dietetic Association: individual-, family-, school-, and community-based interventions for pediatric overweight. J Am Diet Assoc. 2006;106(6):925–45.
Trudnak T, Melton ST, Simpson L, Baldwin J. The childhood obesity response in Florida: where do we stand? Child Obes. 2012;8(3):237–42.
Burrows T, Golley RK, Khambalia A, McNaughton SA, Magarey A, Rosenkranz RR, et al. The quality of dietary intake methodology and reporting in child and adolescent obesity intervention trials: a systematic review. Obes Rev. 2012;13(12):1125–38.
Kirk SF, Penney TL, McHugh TL, Sharma AM. Effective weight management practice: a review of the lifestyle intervention evidence. Int J Obes. 2012;36(2):178–85.
Robertson R, Robertson A, Jepson J, Maxwell M. Walking for depression or depressive symptoms: a systematic review and meta-analysis. Ment Health Phys Act. 2012;5(1):66–75.
Pratt CA, Stevens J, Daniels S. Childhood obesity prevention and treatment: recommendations for future research. Am J Prev Med. 2008;35(3):249–52.
Cress ME, Buchner DM, Prohaska T, Rimmer J, Brown M, Macera C, et al. Best practices for physical activity programs and behavior counseling in older adult populations. Eur Rev Aging Phys Act. 2006;3(1):34–42.
Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity. A systematic review. Am J Prev Med. 2002;22 Suppl 4:73–107.
Weaver RG, Beets MW, Webster C, Beighle A, Huberty J. A conceptual model for training after-school program staffers to promote physical activity and nutrition. J Sch Health. 2012;82(4):186–95.
Carroll JK, Yancey AK, Spring B, Figueroa-Moseley C, Mohr DC, Mustian KM, et al. What are successful recruitment and retention strategies for underserved populations? Examining physical activity interventions in primary care and community settings. Transl Behav Med. 2011;1(2):234–51.
Schröer S, Haupt J, Pieper C. Evidence-based lifestyle interventions in the workplace–an overview. Occup Med. 2014;64(1):8–12.
Walton-Moss B, Samuel L, Nguyen TH, Commodore-Mensah Y, Hayat MJ, Szanton SL. Community-based cardiovascular health interventions in vulnerable populations: a systematic review. J Cardiovasc Nurs. 2013;29:293–307.
Haughton B, Stang J. Population risk factors and trends in health care and public policy. J Acad Nutr Diet. 2012;112 Suppl 1:S35–46.
Hoelscher DM, Kirk S, Ritchie L, Cunningham-Sabo L, Academy Positions Committee. Position of the Academy of Nutrition and Dietetics: interventions for the prevention and treatment of pediatric overweight and obesity. J Acad Nutr Diet. 2013;113(10):1375–94.
Simovska V, Dadaczynski K, Viig NG, Tjomsland HE, Bowker S, Woynarowska, B, de Ruiter S, Buijs, G: HEPS Tool for Schools: A guide for school policy development on healthy eating and physical activity. 2010. [http://pure.au.dk//portal/files/760/ToolforschoolsLRes_website.pdf]
Bellew B, Schöeppe S, Bull FC, Bauman A. The rise and fall of Australian physical activity policy 1996–2006: a national review framed in an international context. Aust New Zealand Health Policy. 2008;31;5:18.
Foltz JL, May AL, Belay B, Nihiser AJ, Dooyema CA, Blanck HM. Population-level intervention strategies and examples for obesity prevention in children. Annu Rev Nutr. 2012;21;32:391–415.
Swinburn B, Gill T, Kumanyika S. Obesity prevention: a proposed framework for translating evidence into action. Obes Rev. 2005;6(1):23–33.
Brennan Ramirez LK, Hoehner CM, Brownson RC, Cook R, Orleans CT, Hollander M, et al. Indicators of Activity-Friendly Communities: an evidence-based consensus process. Am J Prev Med. 2006;31(6):515–24.
Aalbers T, Baars MA, Rikkert MG. Characteristics of effective internet-mediated interventions to change lifestyle in people aged 50 and older: a systematic review. Ageing Res Rev. 2011;10(4):487–97.
Choi J, Fukuoka Y, Lee JH. The effects of physical activity and physical activity plus diet interventions on body weight in overweight or obese women who are pregnant or in postpartum: a systematic review and meta-analysis of randomized controlled trials. Prev Med. 2013;56(6):351–64.
Geraedts H, Zijlstra A, Bulstra SK, Stevens M, Zijlstra W. Effects of remote feedback in home-based physical activity interventions for older adults: a systematic review. Patient Educ Couns. 2013;91(1):14–24.
Müller-Riemenschneider F, Reinhold T, Nocon M, Willich SN. Long-term effectiveness of interventions promoting physical activity: a systematic review. Prev Med. 2008;47(4):354–68.
Brennan LK, Brownson RC, Orleans CT. Childhood obesity policy research and practice: evidence for policy and environmental strategies. Am J Prev Med. 2014;46(1):e1–16.
Goode AD, Reeves MM, Eakin EG. Telephone-delivered interventions for physical activity and dietary behavior change: an updated systematic review. Am J Prev Med. 2012;42(1):81–8.
Lombard CB, Deeks AA, Teede HJ. A systematic review of interventions aimed at the prevention of weight gain in adults. Public Health Nutr. 2009;12(11):2236–46.
Morris JH, Macgillivray S, McFarlane S. Interventions to promote long-term participation in physical activity after stroke: a systematic review of the literature. Arch Phys Med Rehabil. 2014;95(5):956–67.
van Achterberg T, Huisman-de Waal GG, Ketelaar NA, Oostendorp RA, Jacobs JE, Wollersheim HC. How to promote healthy behaviours in patients? An overview of evidence for behaviour change techniques. Health Promot Int. 2011;26(2):148–62.
Broekhuizen K, Kroeze W, van Poppel MN, Oenema A, Brug J. A systematic review of randomized controlled trials on the effectiveness of computer-tailored physical activity and dietary behavior promotion programs: an update. Ann Behav Med. 2012;44(2):259–86.
Kohl LF, Crutzen R, de Vries NK. Online prevention aimed at lifestyle behaviors: a systematic review of reviews. J Med Internet Res. 2013;15(7):e146.
Ogilvie D, Foster CE, Rothnie H, Cavill N, Hamilton V, Fitzsimons CF, et al. Interventions to promote walking: systematic review. BMJ. 2007;334(7605):1204.
Paul-Ebhohimhen V, Avenell A. A systematic review of the effectiveness of group versus individual treatments for adult obesity. Obes Facts. 2009;2(1):17–24.
Stephens SK, Cobiac LJ, Veerman JL. Improving diet and physical activity to reduce population prevalence of overweight and obesity: An overview of current evidence. Prev Med. 2014;62:167–78.
Aldcroft SA, Taylor NF, Blackstock FC, O'Halloran PD. Psychoeducational rehabilitation for health behavior change in coronary artery disease: a systematic review of controlled trials. J Cardiopulm Rehabil Prev. 2011;31(5):273–81.
Martin J, Chater A, Lorencatto F. Effective behaviour change techniques in the prevention and management of childhood obesity. Int J Obes. 2013;37(10):1287–94.
Nawaz H, Katz DL. American College of Preventive Medicine Practice Policy statement: weight management counseling of overweight. Am J Prev Med. 2001;21(1):73–8.
Heath GW, Brownson RC, Kruger J, Miles R, Powell KE, Ramsey LT. The effectiveness of urban design and land use and transport policies and practices to increase physical activity: a systematic review. J Phys Act Health. 2006;3 Suppl 1:S55–76.
Pearson ES. Goal setting as a health behavior change strategy in overweight and obese adults: a systematic literature review examining intervention components. Patient Educ Couns. 2012;87(1):32–42.
Sumlin LL, Garcia AA. Effects of food-related interventions for African American Women with type 2 diabetes. Diabetes Educ. 2012;38(2):236–49.
Campbell KJ, Hesketh KD. Strategies which aim to positively impact on weight, physical activity, diet and sedentary behaviours in children from zero to five years. A systematic review of the literature. Obes Rev. 2007;8(4):327–38.
Anderson LM, Quinn TA, Glanz K, Ramirez G, Kahwati LC, Johnson DB, et al. The effectiveness of worksite nutrition and physical activity interventions for controlling employee overweight and obesity: a systematic review. Am J Prev Med. 2009;37(4):340–57.
Hoehner CM, Ribeiro IC, Parra DC, Reis RS, Azevedo MR, Hino AA, et al. Physical activity interventions in Latin America: expanding and classifying the evidence. Am J Prev Med. 2013;44(3):e31–40.
Roux L, Pratt M, Tengs TO, Yore MM, Yanagawa TL, Van Den Bos J, et al. Cost effectiveness of community-based physical activity interventions. Am J Prev Med. 2008;35(6):578–88.
Weightman A, Ellis S, Cullum A, Sander L, Turley R: Grading evidence and recommendations for public health interventions: developing and piloting a framework. Health Development Agency 2005. [http://www.gserve.nice.org.uk/nicemedia/docs/grading_evidence.pdf]
Wu S, Cohen D, Shi Y, Pearson M, Sturm R. Economic analysis of physical activity interventions. Am J Prev Med. 2011;40(2):149–58.
Katz DL, O'Connell M, Yeh MC, Nawaz H, Njike V, Anderson LM, et al. Public health strategies for preventing and controlling overweight and obesity in school and worksite settings: a report on recommendations of the Task Force on Community Preventive Services. MMWR Recomm Rep. 2005;54(RR-10):1–12.
Klesges LM, Dzewaltowski DA, Glasgow RE. Review of external validity reporting in childhood obesity prevention research. Am J Prev Med. 2008;34(3):216–23.
National Cancer Institute, Division of Cancer Control and Population Sciences (NCI): Measuring the Use of the RE-AIM Model Dimension Items Checklist. 2012. [http://www.re-aim.hnfe.vt.edu/resources_and_tools/measures/checklistdimensions.pdf]
Spencer LM, Schooley MW, Anderson LA, Kochtitzky CS, DeGroff AS, Devlin HM, et al. Seeking best practices: a conceptual framework for planning and improving evidence-based practices. Prev Chronic Dis. 2013;10:130186.
Gudzune K, Hutfless S, Maruthur N, Wilson R, Segal J. Strategies to prevent weight gain in workplace and college settings: a systematic review. Prev Med. 2013;57(4):268–77.
De Bourdeaudhuij I, Van Cauwenberghe E, Spittaels H, Oppert JM, Rostami C, Brug J, et al. School-based interventions promoting both physical activity and healthy eating in Europe: a systematic review within the HOPE project. Obes Rev. 2011;12(3):205–16.
Geaney F, Kelly C, Greiner BA, Harrington JM, Perry IJ, Beirne P. The effectiveness of workplace dietary modification interventions: a systematic review. Prev Med. 2013;57(5):438–47.
Wilding MJ, Seegert L, Rupcic S, Griffin M, Kachnowski S, Parasuraman S. Falling short: recruiting elderly individuals for a fall study. Ageing Res Rev. 2013;12(2):552–60.
IMPALA: Proposed European Guidelines improving infrastructures for leisure-time physical activity in the local arena towards social equity, inter-sectoral collaboration and participation. Final Draft. 2011. [http://www.impala-eu.org/fileadmin/user_upload/2011_IMPALA_guideline_web.pdf]
Hearn LA, Miller MR, Campbell-Pope R. Review of evidence to guide primary health care policy and practice to prevent childhood obesity. Med J Aust. 2008;188 Suppl 8:S87–91.
Acknowledgements
The preparation of this paper was supported by the DEDIPAC Knowledge Hub. The DEDIPAC project is funded under the Joint Programming Initiative (JPI) a Healthy Diet for a Healthy Life, a research and innovation initiative of European Union member states and associated countries. The content of this article reflects only the authors’ views and the Joint Programming Initiative (JPI) a Healthy Diet for a Healthy Life is not liable for any use that may be made of the information contained therein. This article is supported by the following funding agencies (in alphabetical order of participating Member State): Belgium: Research Foundation – Flanders; The Netherlands: The Netherlands Organisation for Health Research and Development (ZonMw); Norway: The Research Council of Norway; Poland: The National Centre for Research and Development.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contribution
KH contributed to the conception of the study and its design, conducted data search, data extraction, data analysis and synthesis, drafted and revised the manuscript. AL contributed to the conception of the study and its design, conducted data extraction, data analysis and synthesis, drafted and revised the manuscript. MvdB participated in the conception of the study and its design, data analysis, and revised the draft of the manuscript. MH conceived of the study and its design, participated in data extraction and revised the draft of the manuscript. GR conceived of the study and its design, participated in data synthesis, and revised the draft of the manuscript. IDB contributed to conception of the study and revised the manuscript. HB contributed to conception of the study and revised the manuscript. All authors read and approved the final manuscript.
Additional file
Additional file 1:
Quality evaluation criteria for stakeholders’ documents, descriptive data for all reviewed documents and the list of 149 elicited characteristics (with supporting documents). Additional file includes: (a) the quality evaluation criteria for stakeholders’ documents Methodological Quality Checklist for Stakeholders’ Documents and Position Papers; (MQC-SP); (b) descriptive data retrieved from systematic reviews, stakeholder documents and position review papers included into the umbrella review, (c) the list of 149 best practice characteristics and references to the documents supporting the characteristics.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Horodyska, K., Luszczynska, A., van den Berg, M. et al. Good practice characteristics of diet and physical activity interventions and policies: an umbrella review. BMC Public Health 15, 19 (2015). https://doi.org/10.1186/s12889-015-1354-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-015-1354-9