
Abstract
Background
work alienation is receiving increasing attention as a psychological risk at work, and little is known about the mechanisms of role ambiguity and work alienation in nurses in the context of the COVID-19 pandemic. This article aims to examine how role ambiguity affects work alienation among Chinese nurses during the two years after COVID-19 pandemic and verify emotional exhaustion as mediators.
Methods
A cross-sectional study design was used to recruit 281 Chinese nurses. Nurses completed online questionnaires containing demographic characteristics, role ambiguity, emotional exhaustion, and work alienation, and SPSS 26.0 and AMOS 24.0 were used for data analysis and structural equation modelling.
Results
work alienation scores were (34.64 ± 10.09), work alienation was correlated with role ambiguity and emotional exhaustion (r1 = 0.521, r2 = 0.755; p < .01), and role ambiguity was positively correlated with emotional exhaustion (r = 0.512; p < .01). A mediating effect of emotional exhaustion between role ambiguity and work alienation held (mediating effect of 0.288, 95% CI: 0.221–0.369, accounting for 74.8% of the total effect).
Conclusion
Role ambiguity has a significant direct effect on nurses’ feelings of alienation and exacerbates alienation through emotional exhaustion. Clarifying roles at work and being less emotionally drained are effective ways to reduce nurses’ feelings of alienation.
Similar content being viewed by others

Introduction
As the population grows and ages, the demand for health care services rises, promoting the development of the nursing profession while placing increasing demands on nurses [1]. However, the shortage of nurses is a key challenge for global health systems [2]. The World Health Organization reported 9 million nurses shortage by 2030 and the severely understaffed situation in nursing profession, which was made worse by the advent of COVID-19 [3]. People have become more connected as a result of advancements in transportation and lifestyle changes, and in the future, the appearance of novel infectious diseases won’t be as surprising [4]. During the pandemic, nurses played a pivotal role in the prevention, treatment and care of infected patients, creating a safer health care organization [5]. The literature points to increased risk of skin damage from wearing uncomfortable protective gear for long periods of time in a closed environment, increased workload and reversed sleep rhythms, leading to physical and mental fatigue, periodic emotional outbursts and increased fear among nurses [6]. They are very careful in their work to prevent themselves from becoming infected and in turn infecting their family and friends [7]. In addition, they suffer discrimination and prejudice from the public because of their close contact with infected patients, but their sense of mission and responsibility as health care professionals makes them conflicted and tormented inside [8]. The imbalance between what they give and what they get in return, the difficulty in obtaining satisfaction from their work and the sense of disparity in expectations, reinforce the desire to leave the nursing profession and a sense of work alienation emerges [9].
Work alienation is a negative state in which one’s needs and expectations are not met at work, resulting in reduced behavioural engagement and psychological alienation [10, 11]. There are three core dimensions of work alienation: (a) sense of helplessness, which refers to the fact that individuals do not have control and control over the content of their work and that they do not have the right to make decisions about it; (b) sense of friendlessness, where the individual do not consider themselves a member of the organization, thus having no sense of identity or not appreciating the ideas, goals and values of the organization; (c) sense of meaninglessness means that individuals do not have a plan to achieve their personal career goals, are not motivated to achieve organizational goals, do not appreciate the importance of their work, and do not feel the value of their work [12]. This concept has been explored extensively over the last 10 years and in Turkey over 80% of nurses feel alienated at work [12]. In China, nurses reported a medium to high level of alienation [13]. In the Netherlands, alienation midwives were less engaged in their work [10]. Studies in Spain, Italy and Pakistan showed high rates of work alienation [14,15,16]. Research also noted that nurses are prone to experience work alienation because of work overload and occupational risks [17]. More importantly, the study pointed out that employees performed poorly at work or even showed anti-productive behaviour when they had stronger feelings of alienation [18]. Therefore, in the context of major public health emergencies, it is necessary to investigate the potential influencing factors of nurses’ work alienation, and strategies need to be tapped to effectively alleviate nurses’ alienation, which would subsequently protect patients safety, reduce nurse turnover and promote the development of nursing.
Role ambiguity is a lack of clarity related to the absence of job information such as role responsibilities or expectations [19]. The current changes in the health care system have expanded and complicated the scope of nurses’ roles. As a result, nurses found themselves doing overlapping tasks, receiving missing and receiving confusing treatment information (e.g. COVID-19 patient treatment and care information, roles in multidisciplinary teams, unclear instructions from managers) [20,21,22]. Previous research has found that role ambiguity has a negative impact on an individual’s physical and psychological well-being and is negatively associated with work attitudes and behaviours (such as work alienation, organizational commitment), while being positively associated with job dissatisfaction [23,24,25,26]. Lacking clear information about the job match, role ambiguity makes it difficult for individuals to perform their jobs, lose confidence in their ability to do the job, become frustrated and feel incompetent due to their inability to control the job, and gradually show alienation from the work and develop feelings of work alienation [27]. Previous research has explored the relationship between role ambiguity and work alienation, but this relationship is not yet clear in the nurse population.
Emotional exhaustion is the depletion of psychological and emotional resources caused by the demands of work and is one of the core factors of burnout [28]. Numerous studies have found that emotional exhaustion has a negative impact on an individual’s physical and mental health and reduces employee motivation and engagement, psychological withdrawal, avoidance of work and ultimately leads to a sense of alienation from work [29, 30]. Marx argues that workers experience alienation followed by physical exhaustion and a lack of mental strength [31]. Based on this, some studies have found that emotional exhaustion increases the occurrence of work alienation, and that work alienation also exacerbates emotional exhaustion in employees [14]. According to the Theory of Limited Self-Control Resource, emotional exhaustion occurs when individuals are under the influence of stressors (role ambiguity) and need to continuously consume psychological resources to make adjustments to their behaviour and cognition in order to exhibit rational work behaviour, with a long-term depletion of intrinsic resources [32]. According to Chiara Panari’s research [33], role ambiguity decreases the motivation of health care workers, and health care workers feel exhausted and depressed in response to role ambiguity, leading to emotional exhaustion. Anita Padmanabhanunni’s study of university teachers during the COVID-19 epidemic found that role ambiguity increased teacher stress, impairs mental health, and was a significant predictor of teacher emotional exhaustion [34].
As role ambiguity increases emotional exhaustion, which is negatively associated with work alienation, emotional exhaustion may mediate the relationship between role ambiguity and work alienation. However, to date, to our knowledge, this mechanism has been under-researched in the nurse population, both in China and in other countries.
Study aims
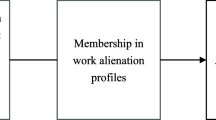
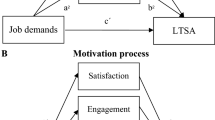
The study is designed (1) to identify the current state of role ambiguity, emotional exhaustion and work alienation among nurses; (2) to investigate the mechanisms by which role ambiguity affects job alienation among nurses and to validate the mediating role of emotional exhaustion. The theoretical model is shown in Fig. 1.

The hypothesized model
Methods
Design and sampling
The study was a cross-sectional design, using a questionnaire to collect data. A convenience sampling method was used to select four grade 3 A hospitals in Shandong Province and Shaanxi Province from October 2022 to January 2023. With the help and support of hospital administrators, a link to an anonymous version of the electronic questionnaire was sent to clinical nurses. Inclusion criteria: (1) nurses who had obtained the professional qualification certificate of the People’s Republic of China; (2) nurses who had been working in the hospital for more than 1 year; (3) informed consent and voluntary participation. Exclusion criteria: (1) those who were not in their posts during the survey period (due to sick leave, maternity leave, etc.); (2) rotating nurses or trainee nurses.
We have set each IP address to be filled in only once in the backend of the questionnaire software in order to prevent receiving duplicate questionnaires. In addition, intelligent logic recognition was set in the backend to check for invalid (all questions answered the same, does not correspond to reality, “Age 2000”, etc.) questionnaires. Finally, valid questionnaires were checked by two researchers to ensure the accuracy of the data.
Sample size
We calculated the sample size according to Kendall (1975) [35]. The total number of questionnaire entries used in this study was 27, which was then expanded by a further 20% given the potential loss of sample size due to incomplete completion.
The sample size was therefore calculated as N = [27 × 5 × (1 + 20%)] = 162, indicating that a minimum of 162 participants were required for this study. According to the Muelle [36], the proposed structural equation model (SEM) requests a sample size of no less than 200 for the framework, and, ultimately a total of 281 nurses met the inclusion and exclusion criteria to take part in our study.
Measurements
Covariables: social-demographic characteristics
Sociodemographic variables include mainly gender, age, degree (college, bachelor, master and above), marital status (married, unmarried), job title, years of work (0 ~ 2,3 ~ 5,6 ~ 10, > 10).
Dependent variable: work alienation
Work alienation was measured using the Work Alienation Questionnaire for Nurses developed by Ren [37], which is widely used in China and has good reliability and validity [38]. The questionnaire consisted of 12 items from 3 dimensions: feelings of helplessness (4 items), feelings of hopelessness (4 items) and feelings of meaninglessness (4 items). Scoring was based on a 5-point Likert scale from 1 (not conforming) to 5 (very conforming), with total scores of 12–27, 28–43 and 44–60 representing low, medium and high levels of work alienation among nurses respectively. The Cronbach’s alpha for the scale was.841.
Independent variable: role ambiguity
Role ambiguity was measured using five entries from the Role Stress Scale developed by Pteterson [39]. (for example, “I know what my job responsibilities are”, “I know exactly what the organization expects of me”), the scale has been translated into a Chinese version and is widely used by scholars in China [27]. Each entry was scored from 1 (strongly disagree) to 5 (strongly agree) and all entries were reversely coded to calculate a total questionnaire score, with higher scores associated with higher levels of role ambiguity. The Cronbach’s alpha for the scale was 0.932.
Mediator: emotional exhaustion
Emotional exhaustion was measured using the Maslach scale [40]. We used five items from the Maslach Burnout Inventory (MBI) (for example, “Work makes me feel physically and mentally exhausted”, “The thought of facing the day ahead makes me very tired”), it has high reliability and validity and is widely used in China [41]. The scale is scored on a five-point Likert scale from 1 (never) to 5 (always), with higher total scores indicating higher levels of emotional exhaustion. The scale’s Cronbach’s alpha for the scale was 0.957.
Ethical approval
This study was conducted in accordance with the ethical standards required in the Declaration of Helsinki. This study is not related to human clinical trials or animal experiments. All participants were provided with anonymous written informed consent and informed that they could refuse or withdraw from the study at any time before the study was conducted, and this study was approved by the Independent Ethics Committee of the Second Affiliated Hospital of the Fourth Military Medical University.
Data analysis
For the data analysis, IBM SPSS Statistics 26.0 was employed. Initially, we examined demographic characteristics by descriptive statistics and analyzed the correlation between role ambiguity, emotional exhaustion, and work alienation by Pearson correlations. Finally, we used IBM AMOS 24.0 to build and measure structural equation models with 2000 bootstrapping resamples to calculate the mediating effect of emotional exhaustion, with 95% CI not including 0, representing a significant mediating effect.
Results
Sociodemographic characteristics
A total of 281 nurses participated in this study, of whom 243 (86.5%) were female, with a mean age of 32.88 years (SD = 6.93), a mean length of service of 10.15 years (SD = 7.63), and 204 (72.6%) were married, and most nurses had obtained a bachelor’s degree199 (70.8%), as shown in Table 1.
Means, standard deviations, and correlations among variables
As shown in Table 2, the total scores for role ambiguity, emotional exhaustion, and work alienation were 12.22 ± 4.74, 16.37 ± 4.75, and 34.64 ± 10.09, respectively. Correlation analyses revealed positive correlations between role ambiguity, emotional exhaustion and work alienation (r = .521, 0.755, p < .01) and positive correlations between role ambiguity and emotional exhaustion (r = .512, p < .01).
Model test
Independent variable role ambiguity, the dependent variable work alienation, and the intermediate variable emotional exhaustion were included in the equation by AMOS 24.0 to model the structural equations. We then used maximum likelihood to fit and correct the initial model. The model fit results were: χ2/df = 2.155, CFI = 0.983, TLI = 0.978, SRMR = 0.040, RMSEA = 0.064 (Table 3). As shown in Table 4, the mediation analysis revealed a significant total effect of role ambiguity on work alienation (β = 0.385, p < .01). In addition, role ambiguity was directly and positively related to work alienation (β = 0.098, p < .01), positively related to emotional exhaustion (β = 0.432, p < .01), and emotional exhaustion was positively related to work alienation (β = 0.666, p < .01). The mediating effect of emotional exhaustion in role ambiguity and work alienation (2 indirect paths multiplied) was 0.288 with 95% CI not including 0 (0.221 to 0.369), indicating a significant indirect effect of role ambiguity on work alienation through emotional exhaustion, with the mediating effect accounting for 74.8% of the total effect. Our findings explain the hypothesis. Figure 2 depicts the mediating effect model.

Mediation Model. RA, role ambiguity; e9-e13, manifest variables of role ambiguity; EE, emotional exhaustion; e1-e5, manifest variables of emotional exhaustion; WA, work alienation; e6-e8, manifest variables of the three dimensions of work alienation
Discussion
Levels of role ambiguity, emotional exhaustion, and work alienation
Our research results demonstrate that Chinese clinical nurses had a moderate level of work alienation, with an overall score of 34.64 ± 10.09, similar to Xia’s findings [17], But higher than Cui’s study of nurses in northwest China [42]. We believe that a number of reasons account for this: (1) Although all were in the context of a pandemic, differences in the timing of the survey, the region studied, the intensity of the epidemic, the strains of infection, and the preventive and control measures taken may have led to differences in the number of infections, psychological stress and nurses’ workload, resulting in heterogeneity in the nurses’ sense of alienation from their work. During the period of our study, China implements the " Category B, B Control” programme (Isolation measures are not being implemented for COVID-19 patients), and the number of new coronary pneumonia cases was on the rise, with many nurses reporting COVID positive. Nurses face a dramatic increase in workload, the risk of their own infections, and work with illness, making a huge contribution and dedication to safeguarding people’s lives. However, low pay and benefits, few opportunities for advancement and limited career development make nurses experience a reduced sense of professional value, which may lead to nurses seeing their work as meaningless [38]; (2) Nurses had limited control and autonomy over their work, which constrained their enthusiasm for their work and they became less-motivated to achieve professional success, as they worked under the direction of medical advice, constantly repeated the implementation of medical advice and were responsible for checking for omissions. a sense of helplessness at not being able to choose what to do with your work [10]; (3) The lack of humanistic care for nurses in the organization, the lack of improvement in the psychosocial working environment for nurses. Particularly during the COVID-19 epidemic, the needs of patients and families increase and nurses are not supported and cared for while performing overloads, demands for quality care, and potential infection risks. Their needs are not taken into account and they are constantly exposed to psychosocial risks, leaving nurses physically and mentally exhausted and with a sense of friendlessness [38]. This may also be the reason for the prolonged work alienation among the group of nurses.
Our study reported nurses’ role ambiguity at a moderate level, higher than that in the Jing’s findings which consisted of 227 nurses from two public hospitals in northern China [43], but lower than the results of Saad A. Alyahya’s study of nurses in primary health care centres in Saudi Arabia [21]. Our findings suggest that nurses are affected by role ambiguity psychological stressors at work, which we speculate may be related to the following: (1) There are differences in guidelines and management protocols related to the treatment and care of COVID-19 patients, which are constantly and dynamically adjusted to the actual situation and, for nurses, require adaptation to organizational changes. These differences and organizational changes may lead to a lack of clarity in the delineation of job-related content, responsibilities, etc., leading to the occurrence of nurse role ambiguity [44]; (2) Today there is a high and diverse demand for healthcare. As medical professionals, nurses undertake multiple roles such as educators, caregivers, consultants, change agents, managers [45, 46]. Nurses need to use knowledge from different disciplines to perform these roles and when there is a lack of relevant knowledge, it leads to nurses being ambiguity about the role [45].
In our study, nurses’ emotional exhaustion was at a moderately high level, slightly higher than in Yang’s findings [47]. It may be caused by the following: (1) The 72.6% of married nurses in this study, during the COVID-19 epidemic, had high job demands, worked long hours in a cordoned off environment, worked endless shifts and had difficulty balancing work-family and may have been highly emotionally internalized, leading to emotional exhaustion [48]; (2) Inadequate staffing, cancellation of breaks or coming to work even when sick, unsafe working environment, lack of support from work resources, resulted in the nurses’ frustration and disillusion with their work [49]; (3) Related research points out that COVID-19-related fear, panic, misinformation and misdirected anger can all lead to workplace violence, and that workplace violence damages nurses’ mental health with negative emotions such as anxiety and depression, increasing ego depletion and causing nurses to experience emotional exhaustion [50, 51] .
The correlations of role ambiguity, emotional exhaustion, and work alienation
The results of the correlation study showed that nurses’ work alienation and its three dimensions were positively correlated with role ambiguity, which is consistent with previous research findings [52]. Lack of clarity in job-related knowledge, responsibilities, instructions and information can prevent nurses from performing their clinical work correctly. Especially during a pandemic, when the increased scope of roles, differences in treatment policies, inadequate protective equipment support, as well as fear and dread, lack of information and lack of clarity about the job lead to nurses feeling difficult to control their work, feeling that it is meaningless and creating a sense of helplessness and friendlessness that they have no way to cope with the problem feelings. This leads to an acceleration of their alienation from their work [27]. This suggests that managers should rationalize tasks and time and make timely adjustments to changes in the work environment to reduce role ambiguity.
Work alienation was positively correlated with emotional exhaustion, meaning that nurses’ emotional exhaustion increased with the severity of work alienation, which is consistent with previous research findings [29]. The study noted that emotional exhaustion negatively affects an individual’s cognition, thinking, attention, work planning and ability to switch tasks and solve problems, depleting the individual’s internal resources, reducing work ethic and creating feelings of alienation [53, 54]. According to Marx’s theory [55], alienated employees manifest themselves as exhausted and mentally drained. During the COVID-19 epidemic, health care workers were involved in epidemic prevention, but also in completing their own work and demonstrating professionalism in their ongoing interactions with patients and families, this led to health care workers being physically overworked and suppressing themselves [56]. According to resource conservation theory, when resources are depleted, nurses are more likely to choose to reduce their commitment to patients to protect themselves from distress, become apathetic to their work and gradually alienation from it [38].
Role ambiguity was positively correlated with, indicating that increased role ambiguity was associated with higher emotional exhaustion [57]. Role ambiguity is a psychosocial risk factor for well-being [58]. Research has found that role ambiguity creates uncertainty and doubt about job goals, and how to accomplish tasks, and that employees exert effort to cope with role stress, experiences that increase occupational stress and manifest as physical exhaustion and emotional draining [59]. The need for nurses to constantly adapt to an uncertain environment, role ambiguity and lack of clear goals deplete nurses’ psychological resources [60]. During the pandemic, high role ambiguity and low personal resources had a greater impact on the mental health of nurses, who were more likely to be exhausted, emotionally disturbed, with inadequate resource support, experiencing emotional exhaustion [33].
The mediating role of emotional exhaustion between role ambiguity and work alienation
The results of the mediating effects we analyzed showed that role ambiguity was a positive direct predictor of feelings of work alienation (0.098) and that emotional exhaustion partially mediated the relationship between role ambiguity and work alienation (0.288). Specifically, higher role ambiguity was associated with greater severity of emotional exhaustion, thereby increasing the occurrence and development of work alienation in nurses. Clear job roles help individuals to engage in their work and enhance their intellectual and emotional energy, whereas role ambiguity prevents individuals from choosing coping resources and strategies to solve problems and leads to burnout and negative emotions, reduced motivation and feelings of work alienation [27]. During a pandemic, nurses face uncertainty at work (e.g. treatment options, unclear instructions) which increases job insecurity, prevents nurses from adopting protective measures and strategies for problem solving, makes it difficult to perform clinical tasks correctly and effectively, creates stress and emotional distress from feeling unable to perform and complete their work, depletes nurses’ physical and mental resources, increases job dissatisfaction and leads to emotional exhaustion [33, 58]. These problems lead to feelings of helplessness and friendlessness, negative job evaluations, a sense of the meaninglessness of work and increase the level of work alienation among nurses.
Conclusion
This study examines the impact of role ambiguity on nurses’ work alienation two years after the COVID-19 epidemic, and the mechanisms mediating emotional exhaustion. It fills a gap in current research and has significant reference value for improving the psychosocial working environment of nurses during major public health emergency events. Our findings indicate that nurses have moderate levels of role ambiguity and work alienation, have moderately high levels of emotional exhaustion, and that measures should be taken to improve this situation. In addition, we found that role ambiguity directly or indirectly affects nurses’ sense of work alienation through emotional exhaustion. Therefore, by reducing role ambiguity at work and improving emotional exhaustion, nurses’ sense of work alienation can be reduced, this helps to increase nurses’ enthusiasm and commitment to their work, which in turn improves the quality of care.
Limitation
There are several limitations to this study. First, we used a cross-sectional research design and did not infer a causal relationship between the variables. Secondly, data were distributed and collected using a questionnaire platform, and the number of questionnaires distributed and the differences between nurses who participated and those who declined to participate in the study are unclear. In addition, the results may be somewhat subjective based on the self-reported questionnaire format, and these factors may limit the generalisability of the findings. Finally, our study was conducted in only two provinces in China and the findings may not be applicable to other regions and countries and have limitations. In future studies, we will expand the scope of the survey, increase the sample size, include more influencing factors and enrich the research mechanism of work alienation.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Awosoga OA, Odole AC, Onyeso OK, Doan J, Nord C, Nwosu IB, Steinke C, Ojo JO, Ekediegwu EC, Murphy S. Well-being of professional older adults’ caregivers in Alberta’s assisted living and long-term care facilities: a cross-sectional study. BMC Geriatr. 2023;23(1):85. https://doi.org/10.1186/s12877-023-03801-9
Estephan L, Pu C, Bermudez S, Waits A. Burnout, mental health, physical symptoms, and coping behaviors in healthcare workers in Belize amidst COVID-19 pandemic: a nationwide cross-sectional study. Int J Soc Psychiatry 2023:207640231152209. https://doi.org/10.1177/00207640231152209
Organization WH. Global strategy on human resources for health: workforce 2030. 2016.
Fei Y, Fu W, Zhang Z, Jiang N, Yin X. The effects of effort-reward imbalance on emergency nurses’ turnover intention: the mediating role of depressive symptoms. J Clin Nurs. 2022. https://doi.org/10.1111/jocn.16518
McCauley L, Hayes R. Taking responsibility for front-line health-care workers. The Lancet Public health. 2020;5(9):e461. https://doi.org/10.1016/s2468-2667(20)30179-1
Zhang R, Lai J, Wang Y, Huang J, Hu S, Wang H. Mental health outcome and resilience among aiding Wuhan nurses: one year after the COVID-19 outbreak in China. J Affect Disord. 2022;297:348–52. https://doi.org/10.1016/j.jad.2021.10.050
Cipolletta S, Previdi S, Martucci S. The Healthcare Relationship during the Second Wave of the COVID-19 pandemic: a qualitative study in the Emergency Department of an italian hospital. Int J Environ Res Public Health. 2023;20(3). https://doi.org/10.3390/ijerph20032072
Sun T, Zhang SE, Yin HY, Li QL, Li Y, Li L, Gao YF, Huang XH, Liu B. Can resilience promote calling among chinese nurses in intensive care units during the COVID-19 pandemic? The mediating role of thriving at work and moderating role of ethical leadership. Front Psychol. 2022;13:847536. https://doi.org/10.3389/fpsyg.2022.847536
Alfuqaha OA, Shunnar OF, Khalil RA, Alhalaiqa FN, Thaher YA, Al-Masarwah UM, Al Amad TZ. Work alienation influences nurses’ readiness for professional development and willingness to learn: a cross-sectional correlation study. PLoS ONE. 2023;18(5):e0284963. https://doi.org/10.1371/journal.pone.0284963
Tummers LG, Den Dulk L. The effects of work alienation on organisational commitment, work effort and work-to-family enrichment. J Nurs Adm Manag. 2013;21(6):850–9. https://doi.org/10.1111/jonm.12159
Marx, KJTTBIMsCoM. by Erich Fromm: 1961.“Economic and Philosophical Manuscripts.”. 1844:85–196.
Amarat M, Akbolat M, Ünal Ö, Güneş Karakaya B. The mediating role of work alienation in the effect of workplace loneliness on nurses’ performance. J Nurs Adm Manag. 2019;27(3):553–9. https://doi.org/10.1111/jonm.12710
You Q, Bai D, Wu C, Gao J, Hou C. Status of work alienation among nurses in China: a systematic review. Front Psychiatry. 2022;13:986139. https://doi.org/10.3389/fpsyt.2022.986139
Khan MAS, Jianguo D, Mann A, Saleem S, Boamah KB, Javed U, Usman M. Rejuvenating the Concept of Work Alienation through Job Demands-Resources Model and examining its relationship with emotional exhaustion and explorative and exploitative learning. Psychol Res Behav Manage. 2019;12:931–41. https://doi.org/10.2147/prbm.S204193
Lagios C, Lagios N, Stinglhamber F, Caesens G. Predictors and consequences of work alienation in Times of Crisis: evidence from two longitudinal studies during the COVID-19 pandemic. Curr Psychol (New Brunsw NJ). 2022;1–15. https://doi.org/10.1007/s12144-022-03372-9
Delgado Bolton RC, San-Martín M, Vivanco L. Role of Empathy and lifelong Learning Abilities in Physicians and Nurses who work in direct contact with patients in adverse Working Conditions. Int J Environ Res Public Health. 2022;19(5). https://doi.org/10.3390/ijerph19053012
Xia B, Wang X, Li Q, He Y, Wang W. How workplace incivility leads to work alienation: a moderated mediation model. Front Psychol. 2022;13:921161. https://doi.org/10.3389/fpsyg.2022.921161
Amzulescu G, Butucescu AJPRU. The role of work alienation in the Relationship between Perceived Organizational injustice and counterproductive work behaviors. 2021, 19(1)
Shin Y, Hur WM, Park K, Hwang H. How managers’ job crafting reduces turnover intention: the mediating roles of role ambiguity and emotional exhaustion. Int J Environ Res Public Health. 2020;17(11). https://doi.org/10.3390/ijerph17113972
Carbone R, Ferrari S, Belperio S, Bravi S, Mancinelli C, Soave E, Di Bartolomeo M, Andreassi L, Perondi L, Tamba M, et al. Advanced competence in intensive care unit: expectations, role ambiguity between physicians and nurses in intensive care units. Multi - method survey. Acta Biomed. 2022;92(S2):e2021332. https://doi.org/10.23750/abm.v92iS2.12670
Alyahya SA, Al-Mansour KA, Alkohaiz MA, Almalki MA. Association between role conflict and ambiguity and stress among nurses in primary health care centers in Saudi Arabia during the coronavirus disease 2019 pandemic: a cross-sectional study. Med (Baltim). 2021;100(37):e27294. https://doi.org/10.1097/md.0000000000027294
Smits MAA, Boezeman EJ, Nieuwenhuijsen K, de Boer A, van Nieveen EJM, Eskes AM. Family involvement on nursing wards and the role conflicts experienced by surgical nurses: a multicentre cross-sectional study. Scand J Caring Sci. 2022;36(3):706–16. https://doi.org/10.1111/scs.13032
Stavropoulou A, Rovithis M, Sigala E, Moudatsou M, Fasoi G, Papageorgiou D, Koukouli S. Exploring nurses’ Working Experiences during the First Wave of COVID-19 outbreak. Healthc (Basel). 2022;10(8). https://doi.org/10.3390/healthcare10081406
Hoy WKJI. Dimensions of student alienation and characteristics of public high schools. 1972, 3(4):38–52.
Orgambídez A, Almeida H, Borrego Y. Social support and job satisfaction in nursing staff: understanding the link through role ambiguity. J Nurs Adm Manag. 2022;30(7):2937–44. https://doi.org/10.1111/jonm.13675
Alblihed M, Alzghaibi HA. The impact of job stress, role ambiguity and work-life imbalance on turnover intention during COVID-19: a case study of Frontline Health Workers in Saudi Arabia. Int J Environ Res Public Health. 2022;19(20). https://doi.org/10.3390/ijerph192013132
Min Y. The Influence of Role Ambiguity on Employees’ Time Banditry Behavior Master’s thesis Zhongnan University of Economics and Law; 2021.
Wang A, Tang C, Zhou L, Lv H, Song J, Chen Z, Yin W. How surface acting affects turnover intention among family doctors in rural China: the mediating role of emotional exhaustion and the moderating role of occupational commitment. Hum Resour health. 2023;21(1):3. https://doi.org/10.1186/s12960-023-00791-y
Matiz-Moya E, Delgado Bolton RC, García-Gómez E, Vivanco L. Empathy and Occupational Health and Well-Being in ecuadorian Physicians Working with COVID-19 patients: a mixed-method study. Healthc (Basel). 2023;11(8). https://doi.org/10.3390/healthcare11081177
Zanatta AB, Lucca SR. [Prevalence of burnout syndrome in health professionals of an onco-hematological pediatric hospital]. Revista da Escola de Enfermagem da U S P. 2015;49(2):253–60. https://doi.org/10.1590/s0080-623420150000200010
Marx KJFLPH. Economic and philosophical manuscripts of 1844. 1975.
Baumeister RF. Ego depletion and self-regulation failure: a resource model of self-control. Alcohol Clin Exp Res. 2003;27(2):281–4. https://doi.org/10.1097/01.Alc.0000060879.61384.A4
Panari C, Caricati L, Pelosi A, Rossi C. Emotional exhaustion among healthcare professionals: the effects of role ambiguity, work engagement and professional commitment. Acta Biomed. 2019;90(6–s):60–7. https://doi.org/10.23750/abm.v90i6-S.8481
Padmanabhanunni A, Pretorius TB. Teacher burnout in the Time of COVID-19: antecedents and psychological consequences. Int J Environ Res Public Health. 2023;20(5). https://doi.org/10.3390/ijerph20054204
Ni P, Chen J-l, Liu NJCJN. The sample size estimation in quantitative nursing research. 2010, 45(4):378e380.
Mueller ROJSEMAMJ. Structural equation modeling: Back to basics. 1997, 4(4):353–369.
Ren X. The Research on the structure of nurse’s work alienation and related research. Henan: Henan University; 2012. Master’s thesis.
Cui Y, Yang T, Gao H, Ren L, Liu N, Liu X, Zhang Y. The relationship between ego depletion and work alienation in chinese nurses: a network analysis. Front Psychol. 2022;13:915959. https://doi.org/10.3389/fpsyg.2022.915959
Peterson MF, Smith PB, Akande A, Ayestaran S, Bochner S, Callan V, Cho NG, Jesuino JC. D’amorim M, Francois P-HJAoMJ: role conflict, ambiguity, and overload: a 21-nation study. 1995, 38(2):429–52.
Maslach C, Jackson SE, Leiter MP. Maslach burnout inventory: Scarecrow Education; 1997.
Wu L, Ren L, Wang Y, Zhang K, Fang P, Liu X, Yang Q, Wang X, Wu S, Peng J. The item network and domain network of burnout in chinese nurses. BMC Nurs. 2021;20(1):147. https://doi.org/10.1186/s12912-021-00670-8
Cui Y, Yang T, Zhang M, Liu N, Liu Q, Zhang L, Zhang L, Yang H, Zhang Y. Influence of empathy on work alienation among chinese nurses during the COVID-19 pandemic: the mediating effect of ego depletion. Front Psychol. 2023;14:1057460. https://doi.org/10.3389/fpsyg.2023.1057460
Qian J, Wang H, Han ZR, Wang J, Wang H. Mental health risks among nurses under abusive supervision: the moderating roles of job role ambiguity and patients’ lack of reciprocity. Int J mental health Syst. 2015;9:22. https://doi.org/10.1186/s13033-015-0014-x
Xu Z, Ye Y, Wang Y, Qian Y, Pan J, Lu Y, Fang L. Primary care practitioners’ barriers to and experience of COVID-19 Epidemic Control in China: a qualitative study. J Gen Intern Med. 2020;35(11):3278–84. https://doi.org/10.1007/s11606-020-06107-3
Martin D, Weeres A. Building nursing role clarity on a foundation of knowledge and knowledge application. Healthc Manage forum. 2016;29(3):107–10. https://doi.org/10.1177/0840470416633237
Lankshear S, Rush J, Weeres A, Martin D. Enhancing role clarity for the practical nurse: a Leadership Imperative. J Nurs Adm. 2016;46(6):300–7. https://doi.org/10.1097/nna.0000000000000349
Song Y, Yang F, Sznajder K, Yang X. Sleep quality as a Mediator in the relationship between perceived stress and job burnout among chinese nurses: a structural equation modeling analysis. Front Psychiatry. 2020;11:566196. https://doi.org/10.3389/fpsyt.2020.566196
Yarifard K, Abravesh A, Sokhanvar M, Mehrtak M, Mousazadeh Y. Work-family conflict, burnout, and related factors among nurses during the COVID-19 pandemic in the Northwest of Iran. Work (Reading Mass). 2023. https://doi.org/10.3233/wor-220210
Hajebi A, Abbasinejad M, Zafar M, Hajebi A, Taremian F. Mental Health, Burnout, and Job Stressors among Healthcare Workers during the COVID-19 pandemic in Iran: a cross-sectional survey. Front Psychiatry. 2022;13:891430. https://doi.org/10.3389/fpsyt.2022.891430
Yang Y, Wang P, Kelifa MO, Wang B, Liu M, Lu L, Wang W. How workplace violence correlates turnover intention among chinese health care workers in COVID-19 context: the mediating role of perceived social support and mental health. J Nurs Adm Manag. 2022;30(6):1407–14. https://doi.org/10.1111/jonm.13325
Cao Y, Gao L, Fan L, Zhang Z, Liu X, Jiao M, Li Y, Zhang S. Effects of verbal violence on job satisfaction, work engagement and the mediating role of emotional exhaustion among healthcare workers: a cross-sectional survey conducted in chinese tertiary public hospitals. BMJ open. 2023;13(3):e065918. https://doi.org/10.1136/bmjopen-2022-065918
Dan SC, Thundiyil T, Wang JJEMJ. Alienation and its correlates: A meta-analysis. 2014, 32(1):24–36.
Oosterholt BG, Van der Linden D, Maes JH, Verbraak MJ, Kompier MA. Burned out cognition–cognitive functioning of burnout patients before and after a period with psychological treatment. Scand J Work Environ Health. 2012;38(4):358–69. https://doi.org/10.5271/sjweh.3256
Conway E, Monks K, Fu N, Alfes K, Bailey KJIJoHRM. Reimagining alienation within a relational framework: evidence from the public sector in Ireland and the UK. 2020.
Shantz A, Alfes K, Truss CJIJoHRM. Alienation from work: marxist ideologies and twenty-first-century practice. 2014, 25(18):2529–50.
Wen J, Zou L, Wang Y, Liu Y, Li W, Liu Z, Ma Q, Fei Y, Mao J, Fu W. The relationship between personal-job fit and physical and mental health among medical staff during the two years after COVID-19 pandemic: emotional labor and burnout as mediators. J Affect Disord. 2023;327:416–24. https://doi.org/10.1016/j.jad.2023.02.029
Stan R, Ciobanu C. The Mediation Chain Effect of Cognitive Crafting and Personal Resources on the relationship between Role Ambiguity and Dentists’ emotional exhaustion. Int J Environ Res Public Health. 2022;19(24). https://doi.org/10.3390/ijerph192416617
Orgambídez A, Almeida H. Exploring the link between structural empowerment and job satisfaction through the mediating effect of role stress: a cross-sectional questionnaire study. Int J Nurs Stud. 2020;109:103672. https://doi.org/10.1016/j.ijnurstu.2020.103672
Hazeen Fathima M, Umarani C. A study on the impact of role stress on engineer intention to leave in indian construction firms. Sci Rep. 2022;12(1):17576. https://doi.org/10.1038/s41598-022-21730-2
Meng H, Bai S, Cao Q. Risk factors of role stress and professional burnout among nurse anesthetists: a multicenter cross-sectional study. Japan J Nurs science: JJNS. 2021;e12413. https://doi.org/10.1111/jjns.12413
Acknowledgements
We are grateful for the support of the hospital management and the participation and cooperation of all the nurses.
Funding
This works was supported by Research on the Development Mechanism of Emotional Exhaustion among Nursing Personnel in the Post Epidemic Era (2023KXKT081).
Author information
Authors and Affiliations
Contributions
H-lZ, CW, and J-rY designed the study and were responsible for analyzing the data and writing the article. J-hL was responsible for collecting the data. PW and M-yH were responsible for checking the data, FL gives guidance in statistics. H-jl and H-mQ directed the study design and interpretation. All authors approved the final paper.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the ethical standards required in the Declaration of Helsinki. This study is not related to human clinical trials or animal experiments. All participants were provided with anonymous written informed consent and informed that they could refuse or withdraw from the study at any time before the study was conducted, and this study was approved by the Independent Ethics Committee of the Second Affiliated Hospital of the Fourth Military Medical University.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Hl., Wu, C., Yan, Jr. et al. The relationship between role ambiguity, emotional exhaustion and work alienation among chinese nurses two years after COVID-19 pandemic: a cross-sectional study. BMC Psychiatry 23, 516 (2023). https://doi.org/10.1186/s12888-023-04923-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-04923-5