
Abstract
Background
To determine the association between sleep disorders and Triglyceride glucose index.
Methods
A cross-sectional analysis of the 2005 to 2008 National Health and Nutrition Examination Survey (NHANES) was performed. The 2005 to 2008 NHANES national household survey for adults ≥ 20 years was examined for the sleep disorders.TyG index: ln [triglyceride (mg/ dL) × fasting blood glucose (mg/dL)/2].Multivariable logistic and linear regression models were used to explore the association between the TyG index and sleep disorders.
Results
A total of 4,029 patients were included. Higher TyG index is significantly associated with elevated sleep disorders in U.S. adults. TyG was moderately correlated with HOMA-IR (Spearman r = 0.51). TyG was associated with higher odds of sleep disorders(adjusted OR [aOR],1.896; 95% CI, 1.260 2.854), Sleep apnea (aOR, 1.559; 95% CI, 0.660 3.683), Insomnia(aOR, 1.914;95% CI, 0.531 6.896), and Restless legs (aOR, 7.759; 95% CI,1.446 41.634).
Conclusions
In this study, our result shown that population with higher TyG index are significantly more likely to have sleep disorders in U.S. adults.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Humans spend about one-third of their time sleeping, either to recover or to rest [1]. Sleep disorders are currently considered a public health disease by the Centers for Disease Control (CDC) [2].It cost approximately $3400 to $5200/person/year for health care [3]. Previous studies have shown that sleep disturbances are significantly associated with decreased quality of life and increased metabolic disease, arterial stiffness [4],cardiovascular disease, and mortality [5].
Several observational studies in large populations suggest that insulin resistance (IR) may be a major cause of sleep disturbance [6]. The triglyceride glucose index, which has been reported to be significantly associated with IR, is a simple and reliable surrogate indicator for IR [7,8,9].The association of Triglyceride glucose index (TyG) with cardiovascular outcomes and the onset of diabetes has been demonstrated [10,11,12,13].TyG may also be a risk factor for sleep disorders, and this study aimed to explore the relationship between TyG and sleep disorders.NHANES includes a nationally representative sample of U.S. adults. Therefore, to assess the association of TyG with sleep disorders, this study collected datasets from the National Health and Nutrition Examination Survey (NHANES).
Methods
Study population
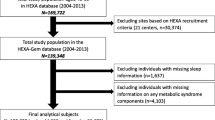
This is a cross-sectional study with data from the National Health and Nutrition Examination Survey (2005–2008). The survey component included diet, questionnaires, and physiological measurements, as well as laboratory tests supervised by trained medical staff. In addition, NHANES employs various modern equipment to make data collection more reliable and efficient. In addition, each participant receives compensation and medical outcome reporting, which increases participant compliance. A total sample size of 20,497 adults was assessed from 2005–2008, Fig. 1 shows the study design and inclusion criteria, and participants who were excluded due to missing information on either covariate(missing data on sleep disorders,TyG index,HOMA-IR,fall asleep time,age, gender, race, smoke, drink,BMI,MVPA, Hypertension,Diabetes, CVD and cancer). The participants' medication information in the past month based on these modules, RXDUSE (Taken prescription medicine, past month),RXDDRUG(Generic drug name).Find the drug code via the RXQ_DRUG module.Only publicly available data were used in the analysis, and the NHANES protocol was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board approval.

Flow chart of subject selection
Data collection and definitions
TyG index was calculated as ln [fasting triglycerides (mg/dL) x fasting glucose (mg/dL)/2] [14]. HOMA-IR index was calculated as [fasting glucose (mmol/L) x fasting insulin (μU/mL)/22.5] [15]. Sleep disorders was self-reported by participants. For each adult, standard demographic data were collected. The sleep disorders module was queried for the NHANES question SLQ060, SLQ050: “Have you ever been told by a doctor or other health professional that you have a sleep disorder?”, “Have you ever told a doctor or other health professional that you have trouble sleeping?”,with those responding “yes” subsequently considered to have a sleep disorder in further analysis and SLQ070:People who self-report having Sleep Apnea,Insomnia,Restless Legs or other sleep disorders.,with those responding “yes” subsequently considered to have a sleep disorder in further analysis.
Assessment of covariates
Age, gender, race (Mexican American, Other Hispanic, non-Hispanic white,non-Hispanic black and other race) were obtained by interviews and physical examinations. Existing smokers were defined as those who smoked 100 or more cigarettes and smoked at the time of the survey. Heavy alcohol consumption was defined as those who had consumed 12 or more glasses of alcohol/for life and who had consumed alcohol at the time of the survey.Leisure levels were calculated as the number of minutes per week during which participants reported participating in moderate to vigorous physical activity (MVPA).Participants with a BMI of 25 kg/m2 were considered overweight in accordance with the limit values.Pre-existing co-morbidities initially included a history of CVD, including coronary artery disease, angina pectoris, myocardial infarction and stroke (yes/no);diabetes (categorised as physician-diagnosed and undiagnosed diabetes); hypertension (categorised as diagnosed hypertension and no hypertension);cancer (categorised as diagnosed cancer and no cancer).
Statistical analysis
Sample weights were used for analysis in order to account for complex survey design and non-response to NHANES.Continuous variables were summarized as mean 95%CI or median (interquartile range) depending on variable distribution, and categorical variables as count (proportion). TyG was compared with HOMA-IR by using Spearman correlation and with sleep disorders. Calculated the area under a receiver-operating characteristic curve generated without covariate adjustment.Multivariate logistic regression and linear analysis was then performed to assess the contribution of TyG index to sleep disorders,Model 1 was unadjusted. Model 2 was adjusted for age, gender, and race.Model 3 was adjusted for age,gender,race,BMI,smoke,drink,MVPA,Hypertension,Diabetes,CVD and cancer.The dose–response association was assessed on a continuous scale with restricted cubic spline curves. The subgroup variable stratified analysis was presented with a fully adjusted Model 3. The log-likelihood test was used to evaluate the interaction effects of the TyG index with subgroup variables.Sensitivity analysis was performed to evaluate which was not affected by taking hypotensive drugs, lipid-lowering drugs or hypoglycemic drugs.All statistical analyses were performed by using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and R version 4.1.3 (R Core Team 2020) with a 2-sided P < 0.05 considered statistically significant.
Results
Baseline data for study participants
Figure 1 presented the study design, sampling and exclusion;and 16,468 participants were excluded due to missing information on either covariate(missing data on sleep disorders,TyG index,HOMA-IR,fall asleep time,age, gender, race, smoke, drink,BMI,MVPA, Hypertension,Diabetes, CVD and cancer).Our final sample included 4,029 NHANES participants, of which 48.61% were female and 71.76% were non-Hispanic whites (table.1). Population-weighted mean age was 46.9 years.Only 25.48% of people do physical activity every week.81.18% consumped at least 12 alcohol drinks/lifetime and drunk at the time of survey. About 50% who smoked at least 100 cigarettes and smoked at the time of survey. One-thirdof the population was hypertensive and obesity.
There were 959 (24.98%) persons with self-reported sleep disorders,4.43% of participants with sleep apnea,1.42% persons suffered from Insomnia.The prevalence of self-reported Restless Legs was 14(0.28%). Average time(mean 95%CI) tofall asleep costed was 21.24(20.28–22.19)minutes.
Comparison of TyG to HOMA-IR and sleep disorders
In the analyzed samples, TyG is Moderately correlated with HOMA-IR, corresponding to The population-weighted Spearman r was 0.51. Figure 2 Display participant-level TyG measurements HOMA-IR for log transformation.

Scatterplot of triglyceride-glucose index against log-transformed homeostatic model assessment of insulin resistance (HOMA-IR). The population-weighted Spearman’s rho was 0.51
Figure 3 exhibited the population-weighted receiver-operating characteristic curve (ROC) of sleep disorders,sleep apnea,Insomnia and Restless Legs.The AUC for TyG to sleep disorders is 0.56, TyG was doing well Differentiation of Restless Legs(AUC = 0.79).

a ROC for TyG to Sleep disorders(AUC = 0.56). b ROC for TyG to Sleep apnea(AUC = 0.61). c ROC for TyG to Insomnia(AUC = 0.53). d ROC for TyG to Restless Legs(AUC = 0.79)
Associations of TyG, HOMA-IR with study outcomes
In Table 2, after adjusting for covariates, higher TyG index was associated with higher relative risks of sleep disorders(OR = 1.87; 95% confidence interval (CI) 1.26, 2.85) and Restless Legs(OR = 7.76; 95% confidence interval (CI) 1.45, 41.63). After adjusting for the same covariates, the HOMA-IR index had an increased risk of sleep disorders (OR = 1.21; 95% confidence interval (CI) 1.05, 1.39) and Sleep Apnea(OR = 2.01; 95% confidence interval (CI) 1.56, 2.59). Higher TyG means longer time to fall asleep(P value for linear trend, < 0.01)(Fig. 4).

Association of triglyceride-glucose index (TyG) with time of fall asleep (minutes). The p-value indicates a test for linear trend with increasing number of symptoms derived by treating symptom count as a continuous variable
As shown in Fig. 5, Restricted cubic spline curves suggested that the relationship between TyG index and sleep disorders,sleep apnea,insomnia and Restless Legs was linear. We analyzed the association of TyG with sleep disorders stratified by age(e_table.1), sex(e_table.2), and race(e_table.3), and we found no interaction effects, the confidence interval was too wide, which precluded meaningful inference.

a Restricted cubic spline fitting for the association between TyG index levels with sleep disorders. b Restricted cubic spline fitting for the association between TyG index levels with sleep apnea. c Restricted cubic spline fitting for the association between TyG index levels with Insomnia. d Restricted cubic spline fitting for the association between TyG index levels with Restless Legs
Sensitivity analysis (e_table.4) was performed to evaluate which was not affected by taking lipid-lowering drugs,hypotensive drugs or hypoglycemic drugs.Since TyG appeared to be more strongly correlated with findings than HOMA-IR, we next tested whether the correlation of TyG with findings was independent of HOMA-IR. With additional adjustment for HOMA-IR,TyG continued to be associated with sleep disorders and Restless Legs.
Discussion
In this nationally representative study, the relationship between TyG and sleep disorders was evaluated.The main finding of this paper is that TyG was associated with sleep disorders in the American adult population.This finding was also validated in adjusting the influence of HOMA-IR and was not affected by the use of lipid-lowering, hypotensive or hypoglycemic medications.We also found that increased exposure to TyG could increase the risk for Restless Legs, and the effect of HOMA-IR on Restless Legs was not significant,associations with Restless Legs seemed largely independent of IR (insulin resistance).
A previous study showed that participants with a higher TyG index had a higher risk of obstructive sleep apnea than the low-level group in Korean adult [16]. It may be related to differences in race or adjusted covariates,we found no positive effect of TyG index on sleep apnea in our study.However,we found the association between HOMA-IR and sleep apnea,similar to those previously published [17].After adjustment for HOMA-IR, changes in sleep disturbances suggesting insulin resistance did not fully explain the potential impact of TyG on the findings. Compared with the HOMA-IR metric, TyG is a lower-cost measure for IR [18, 19].In a large population.TyG index can serve as a practical alternative of IR measurement.In addition, the correlation between IR and sleep disturbances has already been documented [20].
Another significant finding was drawn from our linear trend analysis. This study shown that higher TyG means longer time to fall asleep,Edward etl found that longer periods to fall asleep (> 30 min) were associated with higher fasting insulin only for women [21], it confirmed our results.At the Circadian clocks level,several researchers have explored the interaction of gene behavior and have shown that interactions between diet and clock gene mutations affect fasting blood glucose [22], insulin resistance [23, 24], and T2DM [25].A study shows a correlation between improvements Insulin sensitivity and indicators of increased sleep duration After 40 days of sleep (approximately 45 min extra per night) [26],which partly explained our findings.Bosco D et al. found that IGT (prediabetes) is frequently associated with idiopathic RLS(Restless Legs Syndrome) [27].We also found that association between TyG index and Restless Legs with adjusted HOMA-IR.It suggests that prediction of TyG to sleep disorders is not only related to metabolism, but also genetics.In patients with dysglycemia Metabolic RLS may be due to simultaneous reduction in Inhibitory dopaminergic control of the dorsal horn of the spinal cord Excitatory nociceptive input due to peripheral Neuropathy [28].Basic research is still needed to complete the mechanisms of genetics.
Results from our study shown that a linear dose–response relationship between TyG and various sleep disorders, suggesting that regardless of their causal relationship, the earlier interventions on these two modifiable indicators, the greater the benefit.The American Heart Association proposed to take sleep health as one of Life’s Essential 8 [29], blood lipids and blood glucose are also included.Therefore, the combined improvement of sleep quality and TyG may improve cardiovascular health more than a single improvement,evidence from cohort studies is required.There were numerous cross-sectional and prospective epidemiological studies have shown that insufficient and perhaps excessive sleep time predisposes to systemic and central obesity, the metabolic syndrome, cardiovascular disease and all-cause mortality [5, 30].However,a recent prospective epidemiologic study reported for the first time that fasting hyperinsulinaemia and insulin resistance (as assessed by the HOMA-IR index) preceded incident ‘observed apnoeas’ over a 6-year follow-up period [31].Importantly, this link is bidirectional: on the one hand, the circadian clock regulates energy intake and metabolic pathways throughout the organism, while on the other hand feeding behavior and the nutrient composition of the diet influence the circadian clock itself, especially peripheral metabolic organs and their outputs [4].Our study shows a positive relationship between TyG index and sleep disturbance, but the mechanism of the interaction between metabolism and sleep disturbance remains to be investigated.
Our study was the first to investigate the relationship between TyG and sleep disorders, and the positive relationship has been observed. In this study, the sleep disorders includes several kinds of sleep problems, which could largely reflect people's state of sleep. the findings would serve as a reminder to the public to pay more attention to sleep health.This study provides a foundation for future multi-centre cohort studies on sleep disorders and TyG index.Previous studies showed insulin resistance were associated with sleep disorders [6], which may partly explain the significant relationship of TyG index with sleep disorders.However, our investigation has limitation. it was a study by observation, and causality cannot be demonstrated.
Conclusions
After adjusting for case complexity, a high TyG index was associated with higher odds of individuals with sleep disorders in the general population. Insulin resistance did not fully explain the findings.Our finding suggests that the TyG index may be an independent predictor of the development of sleep disorders.
Availability of data and materials
All data generated or analyzed during this study is included at this URL. https://www.cdc.gov/nchs/nhanes/index.htm.
Abbreviations
- NHANE:
-
National health and nutrition examination survey
- TyG:
-
Triglyceride glucose index
- MVPA:
-
Moderate to vigorous-intensity physical activity
- CVD:
-
Cardiovascular disease
- BMI:
-
Body mass index
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- RLS:
-
Restless legs syndrome
References
Carden KA. Sleep is essential: a new strategic plan for the American Academy of Sleep Medicine. J Clin Sleep Med. 2020;16(1):1–2.
Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, Dinges DF, Gangwisch J, Grandner MA, Kushida C, et al. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. J Clin Sleep Med. 2015;11(8):931–52.
Hui SK, Grandner MA. Trouble Sleeping Associated With Lower Work Performance and Greater Health Care Costs: Longitudinal Data From Kansas State Employee Wellness Program. J Occup Environ Med. 2015;57(10):1031–8.
Summa KC, Turek FW. Chronobiology and obesity: Interactions between circadian rhythms and energy regulation. Adv Nutr. 2014;5(3):312s–9s.
Reutrakul S, Van Cauter E. Sleep influences on obesity, insulin resistance, and risk of type 2 diabetes. Metabolism. 2018;84:56–66.
Brady EM, Bodicoat DH, Hall AP, Khunti K, Yates T, Edwardson C, Davies MJ. Sleep duration, obesity and insulin resistance in a multi-ethnic UK population at high risk of diabetes. Diabetes Res Clin Pract. 2018;139:195–202.
Guerrero-Romero F, Villalobos-Molina R, Jiménez-Flores JR, Simental-Mendia LE, Méndez-Cruz R, Murguía-Romero M, Rodríguez-Morán M. Fasting Triglycerides and Glucose Index as a Diagnostic Test for Insulin Resistance in Young Adults. Arch Med Res. 2016;47(5):382–7.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304.
Vasques AC, Novaes FS, de Oliveira MS, Souza JR, Yamanaka A, Pareja JC, Tambascia MA, Saad MJ, Geloneze B. TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes Res Clin Pract. 2011;93(3):e98–100.
Jin JL, Cao YX, Wu LG, You XD, Guo YL, Wu NQ, Zhu CG, Gao Y, Dong QT, Zhang HW, et al. Triglyceride glucose index for predicting cardiovascular outcomes in patients with coronary artery disease. J Thorac Dis. 2018;10(11):6137–46.
Park B, Lee HS, Lee Y-J. Triglyceride glucose (TyG) index as a predictor of incident type 2 diabetes among nonobese adults: a 12-year longitudinal study of the Korean Genome and Epidemiology Study cohort. Transl Res. 2021;228:42–51.
Navarro-González D, Sánchez-Íñigo L, Pastrana-Delgado J, Fernández-Montero A, Martinez JA. Triglyceride-glucose index (TyG index) in comparison with fasting plasma glucose improved diabetes prediction in patients with normal fasting glucose: The Vascular-Metabolic CUN cohort. Prev Med. 2016;86:99–105.
Zhang M, Wang B, Liu Y, Sun X, Luo X, Wang C, Li L, Zhang L, Ren Y, Zhao Y, et al. Cumulative increased risk of incident type 2 diabetes mellitus with increasing triglyceride glucose index in normal-weight people: The Rural Chinese Cohort Study. Cardiovasc Diabetol. 2017;16(1):30.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, Jacques-Camarena O, Rodríguez-Morán M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–51.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–9.
Kang HH, Kim SW, Lee SH. Association between triglyceride glucose index and obstructive sleep apnea risk in Korean adults: a cross-sectional cohort study. Lipids Health Dis. 2020;19(1):182.
Xu H, Liang C, Zou J, Yi H, Guan J, Gu M, Feng Y, Yin S. Interaction between obstructive sleep apnea and short sleep duration on insulin resistance: a large-scale study : OSA, short sleep duration and insulin resistance. Respir Res. 2020;21(1):151.
Hong S, Han K, Park CY. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: a population-based study. BMC Med. 2020;18(1):361.
Irace C, Carallo C, Scavelli FB, De Franceschi MS, Esposito T, Tripolino C, Gnasso A. Markers of insulin resistance and carotid atherosclerosis A comparison of the homeostasis model assessment and triglyceride glucose index. Int J Clin Pract. 2013;67(7):665–72.
Koren D, Taveras EM. Association of sleep disturbances with obesity, insulin resistance and the metabolic syndrome. Metabolism. 2018;84:67–75.
Suarez EC. Self-reported symptoms of sleep disturbance and inflammation, coagulation, insulin resistance and psychosocial distress: evidence for gender disparity. Brain Behav Immun. 2008;22(6):960–8.
Dashti HS, Follis JL, Smith CE, Tanaka T, Garaulet M, Gottlieb DJ, Hruby A, Jacques PF, Kiefte-de Jong JC, Lamon-Fava S, et al. Gene-Environment Interactions of Circadian-Related Genes for Cardiometabolic Traits. Diabetes Care. 2015;38(8):1456–66.
Dashti HS, Smith CE, Lee YC, Parnell LD, Lai CQ, Arnett DK, Ordovás JM, Garaulet M. CRY1 circadian gene variant interacts with carbohydrate intake for insulin resistance in two independent populations: Mediterranean and North American. Chronobiol Int. 2014;31(5):660–7.
Garcia-Rios A, Gomez-Delgado FJ, Garaulet M, Alcala-Diaz JF, Delgado-Lista FJ, Marin C, Rangel-Zuñiga OA, Rodriguez-Cantalejo F, Gomez-Luna P, Ordovas JM, et al. Beneficial effect of CLOCK gene polymorphism rs1801260 in combination with low-fat diet on insulin metabolism in the patients with metabolic syndrome. Chronobiol Int. 2014;31(3):401–8.
Corella D, Asensio EM, Coltell O, Sorlí JV, Estruch R, Martínez-González M, Salas-Salvadó J, Castañer O, Arós F, Lapetra J, et al. CLOCK gene variation is associated with incidence of type-2 diabetes and cardiovascular diseases in type-2 diabetic subjects: dietary modulation in the PREDIMED randomized trial. Cardiovasc Diabetol. 2016;15:4.
Leproult R, Deliens G, Gilson M, Peigneux P. Beneficial impact of sleep extension on fasting insulin sensitivity in adults with habitual sleep restriction. Sleep. 2015;38(5):707–15.
Bosco D, Plastino M, Fava A, Ettore M, Bosco F, Ermio C, Tallarigo F, Pirritano D, Consoli D. Role of the Oral Glucose Tolerance Test (OGTT) in the idiopathic restless legs syndrome. J Neurol Sci. 2009;287(1–2):60–3.
Handwerker HO, Iggo A, Zimmermann M. Segmental and supraspinal actions on dorsal horn neurons responding to noxious and non-noxious skin stimuli. Pain. 1975;1(2):147–65.
Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, et al. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation. 2022;146(5):e18–43.
Ding X, Wang X, Wu J, Zhang M, Cui M. Triglyceride-glucose index and the incidence of atherosclerotic cardiovascular diseases: a meta-analysis of cohort studies. Cardiovasc Diabetol. 2021;20(1):76.
Balkau B, Vol S, Loko S, Andriamboavonjy T, Lantieri O, Gusto G, Meslier N, Racineux JL, Tichet J. High baseline insulin levels associated with 6-year incident observed sleep apnea. Diabetes Care. 2010;33(5):1044–9.
Acknowledgements
Not applicable.
Funding
This study was supported in part by grants from The Study on the Relationship and Mechanism of RAAS Level, Platelet Activation, Anxiety and Depression in Patients with Hypertension. Tangshan Science and Technology Bureau. Bureau Level. Number: 20130214b. Tangshan Technology Bureau About 2020 Tangshan science and technology research and development Notice of the planned (second batch) project. Relevant (county, district) and development zone administrative departments of science and technology, relevant units: The project of Tangshan Science and Technology Research and Development Plan (the second batch) in 2020 is hereby assigned to you. Please organize the project undertaking unit to sign the assignment book (later subsidy Agreement) with the Municipal Science and Technology Bureau before September 24, 2020, and strengthen the management according to the relevant project and fund management measures and other relevant regulations to ensure the project implementation performance. Item number: 20130214b. Project name: Study on the Relationship and Mechanism of RAAS Level, Platelet Activation, Anxiety and Depression in Patients with Hypertension. Responsible unit: North China University of Science and Technology. Beginning and ending time: 2020.06–2023.06. Project leader: Zhijun Wang. Centralized management of departments: Tangshan Technology Bureau.
Author information
Authors and Affiliations
Contributions
Heng Pei and Xin Su wrote the manuscript. Zhijun Wang, Shuyu Li,Shouling Wu and Yangyang Lu critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
There are no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
e_table.1. Association of triglyceride-glucose index (TyG) with study outcomes, stratified by age.
Additional file 2:
e_table.2. Association of triglyceride-glucose index (TyG) with study outcomes, stratified by gender.
Additional file 3:
e_table.3. Association of triglyceride-glucose index (TyG) with study outcomes, stratified by race
Additional file 4:
e_table.4. Association of triglyceride-glucose index (TyG) with study outcomes
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pei, H., Li, S., Su, X. et al. Association between triglyceride glucose index and sleep disorders: results from the NHANES 2005–2008. BMC Psychiatry 23, 156 (2023). https://doi.org/10.1186/s12888-022-04434-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04434-9