
Abstract
Background
Non-suicidal self-injury (NSSI) is an important symptom of bipolar disorder (BD) and other mental disorders and has attracted the attention of researchers lately. It is of great significance to study the characteristic markers of NSSI. Metabolomics is a relatively new field that can provide complementary insights into data obtained from genomic, transcriptomic, and proteomic analyses of psychiatric disorders. The aim of this study was to identify the metabolic pathways associated with BD with NSSI and assess important diagnostic and predictive indices of NSSI in BD.
Method
Nuclear magnetic resonance spectrometry was performed to evaluate the serum metabolic profiles of patients with BD with NSSI (n = 31), patients with BD without NSSI (n = 46), and healthy controls (n = 10). Data were analyzed using an Orthogonal Partial Least Square Discriminant Analysis and a t-test. Differential metabolites were identified (VIP > 1 and p < 0.05), and further analyzed using Metabo Analyst 3.0 to identify associated metabolic pathways.
Results
Eight metabolites in the serum and two important metabolic pathways, the urea and glutamate metabolism cycles, were found to distinguish patients with BD with NSSI from healthy controls. Eight metabolites in the serum, glycine and serine metabolism pathway, and the glucose-alanine cycle were found to distinguish patients with BD without NSSI from healthy controls. Five metabolites in the serum and the purine metabolism pathway were found to distinguish patients with BD with NSSI from those with BD without NSSI.
Conclusions
Abnormalities in the urea cycle, glutamate metabolism, and purine metabolism played important roles in the pathogenesis of BD with NSSI.
Similar content being viewed by others


Background
BD represents a chronic and recurrent disorder that affects approximately 1% of the global population [1, 2], resulting in a number of disabilities in young people, such as cognitive and functional impairment, in addition to increased mortality, particularly from suicide and cardiovascular disease [3, 4]. Bipolar disorder (BD) is characterized by biphasic moods that include depression and mania (in some cases, hypomania), which alternate throughout the course of the disease. Depressive episodes are more common in patients with BD, as a characteristic symptom, the incidence of NSSI is increasing gradually [5], which has important research significance.
Non-suicidal self-injury (NSSI), defined as the direct and deliberate destruction of one’s own bodily tissue (e.g., cutting, burning, and hitting oneself) in the absence of suicidal intent [6], has recently seen a sharp rise among young people [5]. As NSSI is the strongest predictor of future suicidal behavior [7, 8], it is important to probe its pathogenesis in patients with BD with NSSI. Following decades of progressive increase and growing scientific interest in the incidence of NSSI among adolescents and adults [5], NSSI is listed separately in the Diagnostic and Statistical Manual of Mental Disorders (fifth edition). However, there is little relevant research on the pathogenesis of NSSI. Studies suggested that the amygdala and nucleus accumbens may be potential treatment targets in persons who engage in NSSI [9, 10]. Meanwhile, Zahid, et al. have reported an association between neural activity across the dorsolateral prefrontal cortex and suicidal ideation and self-injury risk [11]. Related studies have also pointed to a relationship between abnormal gene methylation and NSSI [12, 13]. Studies have shown that increased inflammation may change major neurotransmitter metabolism, thereby affecting frontal function and decreasing response inhibition, which is associated with increased behavioral impulsivity. This may explain the neurobiological basis of NSSI. However, little is known about the neurobiological mechanisms and biomarkers of NSSI.
Metabolomics is a promising approach for the identification of potential diagnostic and treatment response biomarkers of psychiatric disorders [14, 15]. As blood samples are easier to obtain, it is possible to assess peripheral biomarkers. BD biomarkers in blood, serum, urine, and plasma have been probed using proton nuclear magnetic resonance (1H NMR) [16,17,18], gas chromatography-mass spectrometry [19], and in vivo brain imaging experiments [20, 21]. Significant metabolic markers, such as α-hydroxybutyrate, choline, and isobutyrate, among others, can differentiate patients with BD from healthy individuals [22,23,24,25]. However, little information on the biomarkers associated with NSSI is available. Therefore, a metabolomics study of blood samples may provide insightful information on the pathophysiology of BD. Thus, this study sought to assess the biomarkers of NSSI in patients with BD using metabolomics technologies.
Methods
Participants
This study was conducted at the Department of Psychiatry in Shanxi Bethune Hospital from January 2018 to August 2020. Inpatients and outpatients aged 15 to 45 years and diagnosed with BD during a depressive episode using the Diagnostic and Statistical Manual of Mental Disorders (fifth edition) were recruited. Participants were classified into two groups based on their history of NSSI: BD with NSSI (n = 31) and BD without NSSI (non-NSSI) (n = 46). Patients were directly interviewed, their medical records examined and medical information obtained. The Inventory of Statements About Self-injury (ISAS) assessment was conducted on all patients. Participants were asked if they had any self-injurious behaviors. Exclusion criteria: patients with suicidal ideation and behavior, cerebral trauma, other serious mental illness, and alcohol or substance abuse. The patients were diagnosed by at least two psychiatrists. The normal control group had no family history of psychiatric disorders. All participants were of Han Chinese origin.
Collection of clinical data and assessment of patients
Demographic and clinical information of the participants was collected by a self-designed case data form, which include the following information: age, sex, onset age, family history, life events, sleep time, working pressure, and the presence or absence of NSSI and its specific situation.
The ISAS [26] comprehensively evaluates the characteristics and functions of NSSI. It consists of two parts. The first part evaluates the frequency of NSSI behavior, age at onset, pain experience, and resistance to NSSI behavior. Individuals with NSSI behavior were assessed in part II, including 13 potential functions: affect-regulation, anti-dissociation, anti-suicide, autonomy, interpersonal boundaries, interpersonal influence, marking distress, peer-bonding, self-care, self-punishment, revenge, sensation seeking, and toughness. The ISAS has high reliability and validity in measuring the frequency and function of NSSI. Patients who attempted NSSI more than 5 times in one year were classified into the NSSI group.
The HAMD-24 was used to measure the level of depression and changes in its severity. Patients with bipolar disorder was in a depressed state, as HAMD-24 score was > 17. The statistical results of related information are shown in Table 1.
Collection of NMR metabolomics data
Serum collection
Participants were not allowed to eat or drink after 10 pm, then, serum samples were collected between 8:00 am and 9:00 am the next day.
1H-NMR spectrum and data analysis
We used Bruker 600 MHz AVANCE III NMR spectrometer and Carr-Purcell-Meiboom-Gill (CPMG) pulse sequence. Parameter Settings are as follows: free induction attenuation (64 K data points), self-axonal relaxation delay (320 ms), 64 scans. In order to determine the related pathways of biomarkers, biomarkers will further import MetaboAnalyst 5.0 [27] (http://www.metaboanalyst.ca/), then, the pathway was screened by p-values of pathway enrichment analysis and Impact values of pathway topology analysis.
Data processing and statistical analyses
SIMCA-P14.0 software was used to centralize and normalize the integral data collected and processed by NMR. Partial least squares discriminant analysis (PLS-DA) and orthogonal partial least squares discriminant analysis (OPLS-DA) were performed. Data are presented as mean ± standard deviation (SD). Statistical analyses comparing the two groups were performed using a two-tailed unpaired t-test, whereas two or more groups were compared using one-way ANOVA. P < 0.05 indicated a statistically significant difference.
Results
Demographic data of the participants
There were no significant differences in age (F = 0.139, p = 0.870), sex (χ2 = 1.288, p = 0.525), marital status (χ2 = 11.185, p = 0.083), or family history (χ2 = 6.943, p = 0.139) among the BD (NSSI), BD (non-NSSI), and HC (healthy control) groups. The BD (NSSI) group had a younger age at onset and higher total HAMD-24 scores than the BD (non-NSSI) group (F = 0.153, p = 0.046; and F = 0.040, p = 0.001, respectively). There were significant differences in life events (χ2 = 8.830, p = 0.012), sleep time (χ2 = 19.389, p = 0.001), and work pressure (χ2 = 10.877, p = 0.028) between the BD (NSSI) and BD (non-NSSI) groups (Table 1).
In the BD (NSSI) group, 61.3% of patients had frequent NSSI. The most common method of inflicting NSSI was cutting (54.8%), scratching (25.8%), hitting (9.7%), and biting (9.7%) (Table 1). Eight patients had previously used antidepressants and antipsychotic drugs––4 cases in NSSI group and 4 cases in non-NSSI group (Table 1); none of the other patients had taken any psychotropic drugs.
Analysis of 1H NMR spectroscopy data
Figure 1 shows the typical 1H NMR spectrum profiles of the BD and HC groups. Twenty-eight small-molecule compounds were identified on the 1H NMR spectrum profiles of participants in the two groups based on the findings of the assessment of the human metabolome database (http://www.hmdb.ca/) and related articles published previously (Table 2).

Proton nuclear magnetic resonance spectra of blood samples from patients with bipolar disorder and healthy controls
Discriminative model construction
Partial least-squares discriminant analysis (PLS-DA) was used for 1H NMR metabolic profile analysis of all serum samples. The results were shown in Fig. 2a, indicating that the healthy control group was significantly separated from BD (NSSI) group and the BD (non-NSSI) group. Model verification results are shown in Fig. 2b. The results show that the PLS-DA model is effective.

Proton nuclear magnetic resonance spectra of the partial least-squares discriminant analysis of the serum of patients in the three groups (circle: bipolar disorder with non-suicidal self-injury (NSSI) group; square: bipolar disorder without NSSI; triangle: healthy control group)
Differences in the plasma metabolite and metabolic pathways associated with the BD (NSSI) and HC groups
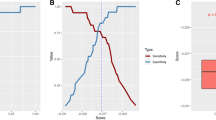
The corresponding OPLS-DA loading plot was further established between BD (NSSI) and HC groups (Fig. 3). A total of eight endogenous differential metabolites were detected (variable importance in projection [VIP] > 1, P < 0.05)—high-density lipoprotein (HDL), 3-hydroxybutyric acid, pyruvic acid, citrulline, and creatinine were significantly increased (*P < 0.05, **P < 0.01), while oxidized glutathione, glyceryl, and β-glucose were significantly decreased (*P < 0.05, **P < 0.01) in the BD (NSSI) group compared with that in the HC group (Table 3). Multiple differential metabolic pathways were identified, using an impact value above 0.05 (Fig. 4), including the urea cycle, the glutamate metabolism pathway, and the pyruvaldehyde degradation pathway.

PCA plots of the OPLS-DA of the healthy control group and BD (NSSI) group, which were validated using S-plots

Metabolic pathways associated with bipolar disorder with non-suicidal self-injury
Differences in the plasma metabolite and metabolic pathways associated with the BD (non-NSSI) and HC groups
The OPLS-DA loading plot between BD (non-NSSI) and HC groups (Fig. 5) detected differences in a total of eight endogenous metabolites (VIP > 1 and P < 0.05)—HDL, pantothenate, alanine, glyceryl, dimethylglycine, and valine were significantly increased (*P < 0.05, **P < 0.01), and N-acetyl glycoproteins and ascorbate were significantly decreased (*P < 0.05, **P < 0.01) in the BD (non-NSSI) group compared with that in the HC group (Table 4). Through analysis of metabolic pathways, we found that the main metabolic pathways consisted of the glycine and serine metabolism pathway and the glucose-alanine cycle (Fig. 6).

PCA plots of the OPLS-DA of the healthy control group and BD (non-NSSI) group, which were validated using S-plots

Metabolic pathways associated with bipolar disorder without non-suicidal self-injury
Differences between the plasma metabolites and metabolic pathways in the BD (non-NSSI) and BD (NSSI) groups
A total of five endogenous differential metabolites between the BD (non-NSSI) and the BD (NSSI) groups was identified (VIP > 1, P < 0.05)—xanthine, niacinamide, adenosine, hypoxanthine, and histidine were significantly higher in the BD (NSSI) group (P < 0.05, P < 0.01) (Table 5). Analysis of metabolic pathways revealed that the main differential metabolic pathways was the purine metabolism (Fig. 7).

Comparison of metabolic pathways associated with bipolar disorder with and without non-suicidal self-injury
Discussion
This study identified the metabolic pathways associated with BD (NSSI) and assessed the important diagnostic and predictive indices of NSSI in BD. To the best of our knowledge, this is the first study to identify the differential metabolites of BD (NSSI) and BD (non-NSSI).
NSSI is a characteristic manifestation of BD, due to its rapidly increasing prevalence, NSSI requires more clinical attention [28]. In a previous study, 5.1% to 24% of people who inflict self-injury reported that they had initiated this behavior before age 11–13 years [29]. In this study, we observed that the onset age of patients in the BD (NSSI) group was lower than that of those in the BD (non-NSSI) group, which is consistent with previous results. Cutting, scratching, burning, hitting, and biting are some of the most commonly used methods of inflicting NSSI. Most self-injurers cut themselves using a sharp object, such as a knife or blade, mainly on the forearms, legs, and/or abdomen [30], which was consistent with our research. Studies confirmed that life stressors and adverse interpersonal experiences are associated with an increased risk of NSSI [31, 32], which is consistent with the present result. In the present study, we also found that sleep problems were most common in the BD (NSSI) group than in the BD (non-NSSI) group or healthy group. Previous research suggests that multiple sleep variables, including poor sleep quality and frequent nightmares, are associated with and are independent risk factors for NSSI [33, 34]. Therefore, we suspect that interventions that improve sleep quality and sleep duration or reduce life stress may concomitantly decrease the risk of NSSI.
A series of studies of BD demonstrated abnormalities of energy metabolism in patients with BD [35]. Several studies have confirmed that lipid metabolic disorders or abnormalities is concerned with neuropsychiatric disorders, such as BD, schizophrenia, and major depressive disorder. Previous studies confirm that there is a high prevalence of elevated triglycerides, cholesterol, low-density lipoprotein, and glucose levels and low high-density lipoprotein (HDL) level in patients with BD [36]. In this study, we found that HDL is a common differential metabolite in the BD (NSSI) and BD (non-NSSI) groups, which suggested the importance of lipid metabolism in BD, that is consistent with previous studies [36, 37]. Results showed that sphingolipids and glycerolipids were increased, whereas glycerophospholipids were decreased, in serum samples from patients with BD. Moreover, studies also showed that elevated lipid level is associated with smaller brain structures in patients with BD [38]. Future research is needed to verify the changes in the HDL levels of BD patients compared with those of healthy individuals and the specific mechanisms of lipid changes in the pathogenesis of BD.
The results of the present study indicate that 3-hydroxybutyric acid, pyruvic acid, oxidized glutathione, glyceryl, citrulline, creatinine, and β-glucose are characteristic markers of bipolar NSSI. Patients in the BD (NSSI) group showed higher lipid, 3-hydroxybutyric acid, pyruvic acid, citrulline, and creatinine levels and lower oxidized glutathione, glyceryl, and β-glucose levels than the healthy controls. Kamonwad et al. reported that patients with BD have increased salivary levels of glutathione and oxidized glutathione compared to controls [39]. Rosa et al. [40] documented decreased levels of glutathione and increased levels of glutathione disulfide in the plasma of patients with BD. Previous studies have also revealed higher serum levels of pyruvate and N-acetyl glutamate in patients with BD than in healthy controls [35, 41], which is consistent with the findings of this study. However, previous studies have insufficiently focused on correlation between the abovementioned metabolites and NSSI in patients with BD.
This study showed that the urea cycle and the glutamate metabolism pathway are significant metabolic pathways in BD (NSSI). For the urea cycle, also known as the ornithine cycle, when amino acids are metabolized in the body, ammonia is produced and subsequently synthesized into urea through. Studies have suggested that an abnormality in the urea cycle (or arginine metabolism) is associated with BD [42, 43]. The results of this study indicated that an abnormal urea cycle is associated with BD (NSSI). Xu et al. reported that state-related abnormalities in oxidative and glutamate metabolism are associated with BD [44, 45]. Increasing evidence suggests that changes in inflammatory mediators are involved in the pathogenesis of mood disorders [46, 47]. Meanwhile, studies have demonstrated links between alterations in inflammation and glutamate metabolism in mood disorders [48, 49]. This indicates that inflammatory mediators, glutamate metabolism and oxidative stress are closely related to the pathogenesis of BD(NSSI). Thus, therapeutic strategies targeting amino acid metabolism such as glutamate may be effective in patients with BD (NSSI), and increased inflammation as reflected in C-reactive protein levels may be helpful in the diagnosis of BD (NSSI).
In clinical practice, identifying specific diagnostic markers of NSSI in patients with BD will provide a strong basis for the recognition and treatment of NSSI. Thus, we also compared the metabolic differences between BD (NSSI) and BD (non-NSSI) groups. Five endogenous differential metabolites, including xanthine, niacinamide, adenosine, hypoxanthine, and histidine, were significantly higher in the BD (NSSI) group than in the BD (non-NSSI) group. Adenosine, a purine nucleoside, may contribute to the pathophysiology of mental disease by interacting with dopamine and glutamate receptors through A1 and A2A receptors; thus, modulating dopaminergic and glutamatergic neurotransmission [50, 51]. Zhang et al. reported that levels of the purines guanine and guanosine are decreased in the brains of patients with BD [52]. However, assessments of changes in purine and adenosine metabolism levels are lacking. This study shows that the important metabolic pathways associated with BD (NSSI) are the purine and methylhistidine metabolism pathways. The purinergic system is a critical neurotransmitter system with uric acid (UA) as its end-product. Recent studies have shown that the patients with BD have the highest UA levels among healthy controls and those with other mental disorders [53, 54], which is involved in the occurrence and development of mental illnesses such as BD and MDD [55, 56]. The purinergic system is involved in the neurodevelopment and pathophysiological processes of psychotic disorders, such as the genesis, differentiation of neurocytes and inflammation of neuroglial cells [57, 58]. Growing evidence suggests that oxidative stress and the purine/adenosine system play key roles in the development and progression of mental diseases, such as BD [59, 60]. We suggest that NSSI in patients with BD is related to an increase in oxidative stress levels. Post-mortem and imaging studies showed an increasingly complex interaction between the mitochondrial, purinergic, and oxidative systems, which are associated with psychiatric disorders [61]. These results suggest that an increase in purinergic-UA metabolism and oxidative stress levels may be a significant mechanism underpinning BD (NSSI), which may be related to mitochondrial dysfunction.
It has been hypothesized that gout and BD may share similar pathophysiological mechanisms, such as purinergic dysfunction. Previous research has shown that patients with BD have an increased risk of gout [62, 63]. We observed increased purine synthesis in the BD (NSSI) group in this study, indicating that the incidence of gout was higher in patients with BD (NSSI). This suggests that purine-UA metabolism is a potential therapeutic target in the treatment of BD (NSSI). As xanthine and hypoxanthine levels are elevated in BD (NSSI), allopurinol, an inhibitor of xanthine oxidase, is used to treat and prevent gout. Allopurinol and febuxostat [64], two potent inhibitors of UA accumulation, have demonstrated antimanic and antidepressant effects in clinical and preclinical studies, and may be used as add-on therapy for BD (NSSI) to reduce rates of self-injury. Hirota et al. suggested that adenosine modulator adjuvant therapy is more beneficial than a placebo in treating manic episodes of BD [65]. As adenosine levels were altered in this study, we suspect that adenosine modulator adjuvant therapy may be effective for BD (NSSI). These drugs can be used as potential therapeutic options for patients with BD (NSSI).
In this study, purine and amino acid metabolism were found to be altered in patients with BD (NSSI) compared to that in healthy controls, which is consistent with the findings of a previous study [66]. As the final metabolite of purine, UA acts on neurons presynaptically and postsynaptically, and on specific receptors in the glial cell membrane that can affect activities of other neurotransmitters involved in the pathophysiological process of mood disorders, including dopamine, GABA, glutamate, and serotonin [67]. It has been suggested that purinergic-UA metabolism is associated with glutamate metabolism, further affecting oxidative stress and is involved in the pathogenesis of NSSI, all of which are related to mitochondrial dysfunction [68,69,70]. This provides important evidence for the diagnosis and treatment of BD (NSSI). These findings provide a basis for further research on the pathogenesis of NSSI, and are highly significant with regard to the diagnosis, recognition, and treatment of NSSI.
Limitations
This study has some limitations. First, the previous use of antidepressants and antipsychotic drugs may be a confounding factor for those eight participants with medication history. We did not control for the effects of psychotropic medications, which may affect plasma metabolite profiling. Second, the sample size was limited. Adequately powered studies are warranted in the future to confirm our preliminary conclusions. Therefore, further studies using a larger sample size of medication-free patients are required. Third, as the difference in metabolomics between the NSSI and non-NSSI groups can be attributed to various factors, such as the relationship between depressive symptom severity and outcome, we need to further evaluate this aspect in subsequent studies.
Conclusion
This study demonstrated that purine and amino acid metabolism are greatly enhanced in BD with NSSI than that in BD without NSSI, providing evidence of the relationship between the purinergic system, glutamate metabolism, and the pathogenesis of NSSI in patients with BD. In addition, the results of this study indicate that xanthine, hypoxanthine, and adenosine may be potential biomarkers of NSSI in patients with BD. These findings suggest that abnormalities in the purinergic system, urea cycle, and glutamate metabolism play important roles in the pathogenesis of BD. Further investigations are needed to elucidate the relationship between purinergic-UA metabolism, amino acid cycling, and oxidative stress. In addition, future studies which are stringently designed with larger samples are required to validate our results and confirm our conclusions.
Availability of data and materials
All data used during the study appear in the submitted article.
Abbreviations
- BD:
-
Bipolar disorder
- NSSI:
-
Non-suicidal self-injury
- UA:
-
Uric acid
- HAMD:
-
Hamilton Depression Scale
- 1H NMR:
-
Proton nuclear magnetic resonance
- PCA:
-
Principal Component Analysis
- iPCA:
-
Interval principal component analysis
- PLS-DA:
-
Partial least-squares discriminant analysis
- OPLS-DA:
-
Orthogonal projections to latent structures discriminant analysis
- OSC:
-
Orthogonal signal correction
- HDL:
-
High-density lipoprotein
- HC:
-
Healthy control
References
Merikangas KR, Jin R, He JP, Kessler RC, Lee S, Sampson NA, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–51.
Sagar R, Pattanayak RD. Potential biomarkers for bipolar disorder: Where do we stand? Indian J Med Res. 2017;145(1):7–16.
Hilty DM, Leamon MH, Lim RF, Kelly RH, Hales RE. A review of bipolar disorder in adults. Psychiatry (Edgmont). 2006;3(9):43–55.
Vieta E, Berk M, Schulze TG, Carvalho AF, Suppes T, Calabrese JR, et al. Bipolar disorders Nat Rev Dis Primers. 2018;4:18008.
Swannell SV, Martin GE, Page A, Hasking P, St John NJ. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression. Suicide Life Threat Behav. 2014;44(3):273–303.
Nonsuicidal self-injury: definition and classification. Washington, DC: American Psychological Association. 2009.
You J, Leung F, Fu K, Lai CM. The prevalence of nonsuicidal self-injury and different subgroups of self-injurers in Chinese adolescents. Arch Suicide Res. 2011;15(1):75–86.
Chesin MS, Galfavy H, Sonmez CC, Wong A, Oquendo MA, Mann JJ, et al. Nonsuicidal Self-Injury Is Predictive of Suicide Attempts Among Individuals with Mood Disorders. Suicide Life Threat Behav. 2017;47(5):567–79.
Westlund Schreiner M, Klimes-Dougan B, Mueller BA, Eberly LE, Reigstad KM, Carstedt PA, et al. Multi-modal neuroimaging of adolescents with non-suicidal self-injury: Amygdala functional connectivity. J Affect Disord. 2017;221:47–55.
Cullen KR, Schreiner MW, Klimes-Dougan B, Eberly LE, LaRiviere LL, Lim KO, et al. Neural correlates of clinical improvement in response to N-acetylcysteine in adolescents with non-suicidal self-injury. Prog Neuropsychopharmacol Biol Psychiatry. 2020;99: 109778.
Zahid Z, McMahon L, Lynch M. Neural Activity Across the Dorsolateral Prefrontal Cortex and Risk for Suicidal Ideation and Self-Injury. Arch Suicide Res. 2022;26(1):187-207.
Zheng D, Bi X, Zhang T, Han C, Ma T, Wang L, et al. Epigenetic Alterations of the Promoter Region of the POMC Gene in Adolescent Depressive Disorder Patients with Nonsuicidal Self-injury Behaviors. Psychol Res Behav Manag. 2020;13:997–1008.
Wang L, Zheng D, Liu L, Zhong G, Bi X, Hu S, et al. Relationship between SIRT1 gene and adolescent depressive disorder with nonsuicidal self-injury behavior: Based on gene methylation and mRNA expression. Medicine (Baltimore). 2021;100(31): e26747.
Tomita M, Kami K. Cancer. Systems biology, metabolomics, and cancer metabolism. Science. 2012;336(6084):990–1.
Zhang A, Sun H, Yan G, Wang P, Wang X. Metabolomics for Biomarker Discovery: Moving to the Clinic. Biomed Res Int. 2015;2015: 354671.
Sethi S, Pedrini M, Rizzo LB, Zeni-Graiff M, Mas CD, Cassinelli AC, et al. (1)H-NMR, (1)H-NMR T2-edited, and 2D-NMR in bipolar disorder metabolic profiling. Int J Bipolar Disord. 2017;5(1):23.
Sussulini A, Prando A, Maretto DA, Poppi RJ, Tasic L, Banzato CE, et al. Metabolic profiling of human blood serum from treated patients with bipolar disorder employing 1H NMR spectroscopy and chemometrics. Anal Chem. 2009;81(23):9755–63.
Chen JJ, Zhou CJ, Liu Z, Fu YY, Zheng P, Yang DY, et al. Divergent Urinary Metabolic Phenotypes between Major Depressive Disorder and Bipolar Disorder Identified by a Combined GC-MS and NMR Spectroscopic Metabonomic Approach. J Proteome Res. 2015;14(8):3382–9.
Liu ML, Zheng P, Liu Z, Xu Y, Mu J, Guo J, et al. GC-MS based metabolomics identification of possible novel biomarkers for schizophrenia in peripheral blood mononuclear cells. Mol BioSyst. 2014;10(9):2398-406.
Soeiro-de-Souza MG, Otaduy MCG, Machado-Vieira R, Moreno RA, Nery FG, Leite C, et al. Anterior Cingulate Cortex Glutamatergic Metabolites and Mood Stabilizers in Euthymic Bipolar I Disorder Patients: A Proton Magnetic Resonance Spectroscopy Study. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3(12):985–91.
Atagun MI, Sikoglu EM, Can SS, Ugurlu GK, Kaymak SU, Caykoylu A, et al. Neurochemical differences between bipolar disorder type I and II in superior temporal cortices: A proton magnetic resonance spectroscopy study. J Affect Disord. 2018;235:15–9.
Zheng P, Wei YD, Yao GE, Ren GP, Guo J, Zhou CJ, et al. Novel urinary biomarkers for diagnosing bipolar disorder. Metabolomics. 2013;9:800-808.
Xu XJ, Zheng P, Ren GP, Liu ML, Mu J, Guo J, et al. 2,4-Dihydroxypyrimidine is a potential urinary metabolite biomarker for diagnosing bipolar disorder. Mol Biosyst. 2014;10(4):813-9.
Ren Y, Chen ZZ, Sun XL, Duan HJ, Tian JS, Wang JY, et al. Metabolomic analysis to detect urinary molecular changes associated with bipolar depression. Neurosci Lett. 2021;742: 135515.
Ren Y, Bao S, Jia Y, Sun XL, Cao XX, Bai XY, et al. Metabolic Profiling in Bipolar Disorder Patients During Depressive Episodes. Front Psychiatry. 2020;11: 569612.
Klonsky ED, Glenn CR. Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS). J Psychopathol Behav Assess. 2009;31(3):215–9.
Pang Z, Chong J, Zhou G, de Lima Morais DA, Chang L, Barrette M, et al. MetaboAnalyst 5.0: narrowing the gap between raw spectra and functional insights. Nucleic Acids Res. 2021;49(W1):W388–96.
Guérin-Marion C, Bureau JF, Lafontaine MF, Gaudreau P, Martin J. Profiles of Emotion Dysregulation Among University Students Who Self-Injure: Associations with Parent-Child Relationships and Non-Suicidal Self-Injury Characteristics. J Youth Adolesc. 2021;50(4):767-787.
Whitlock J SM. The Oxford Handbook of Suicide and Self-injury. 2014.
Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6:339–63.
Wang L, Liu J, Yang Y, Zou H. Prevalence and risk factors for non-suicidal self-injury among patients with depression or bipolar disorder in China. BMC Psychiatry. 2021;21(1):389.
Baiden P, Stewart SL, Fallon B. The role of adverse childhood experiences as determinants of non-suicidal self-injury among children and adolescents referred to community and inpatient mental health settings. Child Abuse Negl. 2017;69:163–76.
Liu X, Chen H, Bo QG, Fan F, Jia CX. Poor sleep quality and nightmares are associated with non-suicidal self-injury in adolescents. Eur Child Adolesc Psychiatry. 2017;26(3):271–9.
Asarnow JR, Bai S, Babeva KN, Adrian M, Berk MS, Asarnow LD, et al. Sleep in youth with repeated self-harm and high suicidality: Does sleep predict self-harm risk? Suicide Life Threat Behav. 2020;50(6):1189–97.
Yoshimi N, Futamura T, Kakumoto K, Salehi AM, Sellgren CM, Holmen-Larsson J, et al. Blood metabolomics analysis identifies abnormalities in the citric acid cycle, urea cycle, and amino acid metabolism in bipolar disorder. BBA Clin. 2016;5:151–8.
Wysokinski A, Strzelecki D, Kloszewska I. Levels of triglycerides, cholesterol, LDL, HDL and glucose in patients with schizophrenia, unipolar depression and bipolar disorder. Diabetes Metab Syndr. 2015;9(3):168–76.
Schwarz E, Prabakaran S, Whitfield P, Major H, Leweke FM, Koethe D, et al. High throughput lipidomic profiling of schizophrenia and bipolar disorder brain tissue reveals alterations of free fatty acids, phosphatidylcholines, and ceramides. J Proteome Res. 2008;7(10):4266–77.
Kennedy KG, Islam AH, Grigorian A, Fiksenbaum L, Mitchell RHB, McCrindle BW, et al. Elevated lipids are associated with reduced regional brain structure in youth with bipolar disorder. Acta Psychiatr Scand. 2021;143(6):513–25.
Ngamchuea K, Batchelor-McAuley C, Williams C, Godlewska BR, Sharpley AL, Cowen PJ, et al. Salivary glutathione in bipolar disorder: A pilot study. J Affect Disord. 2018;238:277–80.
Rosa AR, Singh N, Whitaker E, de Brito M, Lewis AM, Vieta E, et al. Altered plasma glutathione levels in bipolar disorder indicates higher oxidative stress; a possible risk factor for illness onset despite normal brain-derived neurotrophic factor (BDNF) levels. Psychol Med. 2014;44(11):2409–18.
Yoshimi N, Futamura T, Kakumoto K, Salehi AM, Sellgren CM, Holmén-Larsson J, et al. Blood metabolomics analysis identifies abnormalities in the citric acid cycle, urea cycle, and amino acid metabolism in bipolar disorder. BBA Clin. 2016;5:151-8.
Klonsky ED, Oltmanns TF, Turkheimer E. Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am J Psychiatry. 2003;160(8):1501–8.
Yanik M, Vural H, Tutkun H, Zoroglu SS, Savas HA, Herken H, et al. The role of the arginine-nitric oxide pathway in the pathogenesis of bipolar affective disorder. Eur Arch Psychiatry Clin Neurosci. 2004;254(1):43–7.
Lan MJ, McLoughlin GA, Griffin JL, Tsang TM, Huang JT, Yuan P, et al. Metabonomic analysis identifies molecular changes associated with the pathophysiology and drug treatment of bipolar disorder. Mol Psychiatry. 2009;14(3):269–79.
Xu J, Dydak U, Harezlak J, Nixon J, Dzemidzic M, Gunn AD, et al. Neurochemical abnormalities in unmedicated bipolar depression and mania: a 2D 1H MRS investigation. Psychiatry Res. 2013;213(3):235–41.
Isgren A, Jakobsson J, Palsson E, Ekman CJ, Johansson AG, Sellgren C, et al. Increased cerebrospinal fluid interleukin-8 in bipolar disorder patients associated with lithium and antipsychotic treatment. Brain Behav Immun. 2015;43:198–204.
Jakobsson J, Bjerke M, Sahebi S, Isgren A, Ekman CJ, Sellgren C, et al. Monocyte and microglial activation in patients with mood-stabilized bipolar disorder. J Psychiatry Neurosci. 2015;40(4):250–8.
Tilleux S, Hermans E. Neuroinflammation and regulation of glial glutamate uptake in neurological disorders. J Neurosci Res. 2007;85(10):2059–70.
Haroon E, Fleischer CC, Felger JC, Chen X, Woolwine BJ, Patel T, et al. Conceptual convergence: increased inflammation is associated with increased basal ganglia glutamate in patients with major depression. Mol Psychiatry. 2016;21(10):1351–7.
Boison D, Singer P, Shen HY, Feldon J, Yee BK. Adenosine hypothesis of schizophrenia–opportunities for pharmacotherapy. Neuropharmacology. 2012;62(3):1527–43.
Lara DR, Dall’Igna OP, Ghisolfi ES, Brunstein MG. Involvement of adenosine in the neurobiology of schizophrenia and its therapeutic implications. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(4):617–29.
Zhang R, Zhang T, Ali AM, Al Washih M, Pickard B, Watson DG. Metabolomic Profiling of Post-Mortem Brain Reveals Changes in Amino Acid and Glucose Metabolism in Mental Illness Compared with Controls. Comput Struct Biotechnol J. 2016;14:106–16.
Bartoli F, Crocamo C, Mazza MG, Clerici M, Carra G. Uric acid levels in subjects with bipolar disorder: A comparative meta-analysis. J Psychiatr Res. 2016;81:133–9.
Lu Z, Wang Y, Xun G. Individuals with bipolar disorder have a higher level of uric acid than major depressive disorder: a case-control study. Sci Rep. 2021;11(1):18307.
Cheffer A, Castillo ARG, Correa-Velloso J, Goncalves MCB, Naaldijk Y, Nascimento IC, et al. Purinergic system in psychiatric diseases. Mol Psychiatry. 2018;23(1):94–106.
Kesebir S, Tatlidil Yaylaci E, Suner O, Gultekin BK. Uric acid levels may be a biological marker for the differentiation of unipolar and bipolar disorder: the role of affective temperament. J Affect Disord. 2014;165:131–4.
Burnstock G, Krugel U, Abbracchio MP, Illes P. Purinergic signalling: from normal behaviour to pathological brain function. Prog Neurobiol. 2011;95(2):229–74.
Burnstock G. Introductory overview of purinergic signalling. Front Biosci (Elite Ed). 2011;3:896–900.
de Sousa RT, Machado-Vieira R, Zarate CA Jr, Manji HK. Targeting mitochondrially mediated plasticity to develop improved therapeutics for bipolar disorder. Expert Opin Ther Targets. 2014;18(10):1131–47.
Goldstein BI, Young LT. Toward clinically applicable biomarkers in bipolar disorder: focus on BDNF, inflammatory markers, and endothelial function. Curr Psychiatry Rep. 2013;15(12):425.
Andreazza AC, Wang JF, Salmasi F, Shao L, Young LT. Specific subcellular changes in oxidative stress in prefrontal cortex from patients with bipolar disorder. J Neurochem. 2013;127(4):552–61.
Chung KH, Huang CC, Lin HC. Increased risk of gout among patients with bipolar disorder: a nationwide population-based study. Psychiatry Res. 2010;180(2–3):147–50.
Chen J, Chen H, Feng J, Zhang L, Li J, Li R, et al. Association between hyperuricemia and metabolic syndrome in patients suffering from bipolar disorder. BMC Psychiatry. 2018;18(1):390.
Komoriya K, Hoshide S, Takeda K, Kobayashi H, Kubo J, Tsuchimoto M, et al. Pharmacokinetics and pharmacodynamics of febuxostat (TMX-67), a non-purine selective inhibitor of xanthine oxidase/xanthine dehydrogenase (NPSIXO) in patients with gout and/or hyperuricemia. Nucleosides Nucleotides Nucleic Acids. 2004;23(8–9):1119–22.
Hirota T, Kishi T. Adenosine hypothesis in schizophrenia and bipolar disorder: a systematic review and meta-analysis of randomized controlled trial of adjuvant purinergic modulators. Schizophr Res. 2013;149(1–3):88–95.
Wei J, Zhao L, Du Y, Tian Y, Ni P, Ni R, et al. A plasma metabolomics study suggests alteration of multiple metabolic pathways in patients with bipolar disorder. Psychiatry Res. 2021;299: 113880.
Machado-Vieira R, Lara DR, Souza DO, Kapczinski F. Purinergic dysfunction in mania: an integrative model. Med Hypotheses. 2002;58(4):297–304.
Popoli M, Yan Z, McEwen BS, Sanacora G. The stressed synapse: the impact of stress and glucocorticoids on glutamate transmission. Nat Rev Neurosci. 2011;13(1):22–37.
Manji H, Kato T, Di Prospero NA, Ness S, Beal MF, Krams M, et al. Impaired mitochondrial function in psychiatric disorders. Nat Rev Neurosci. 2012;13(5):293–307.
Luykx JJ, Laban KG, van den Heuvel MP, Boks MP, Mandl RC, Kahn RS, et al. Region and state specific glutamate downregulation in major depressive disorder: a meta-analysis of (1)H-MRS findings. Neurosci Biobehav Rev. 2012;36(1):198–205.
Acknowledgements
The authors sincerely thank the research staff and the patients, their families, and healthy volunteers for their participation.
Funding
This work was supported by the National Natural Science Foundation of China (8210053813), Applied Basic Research Projects of Shanxi Province (201901D111418), Research Project Supported by Shanxi Scholarship Council of China (2021–167) and Basic Research Priorities Program of Shanxi Province (20210302123314).
Author information
Authors and Affiliations
Contributions
Y Ren designed and performed the study and modified the manuscript. XJ Guo and J Jia collected and analyzed the data and wrote the manuscript. ZY Zhang, YT Miao, P Wu and YQ Bai performed or contributed to the experiments. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors state that they have obtained approval from The Medical Research Ethics Committee of Shanxi Bethune Hospital (the Approval Notice Number: YXLL-2020–001) and have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, X., Jia, J., Zhang, Z. et al. Metabolomic biomarkers related to non-suicidal self-injury in patients with bipolar disorder. BMC Psychiatry 22, 491 (2022). https://doi.org/10.1186/s12888-022-04079-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04079-8