
Abstract
Background
Deep transcranial magnetic stimulation (DTMS) is a non-invasive method of stimulating widespread cortical areas and, presumably, deeper neural networks. The current study assessed the effects of DTMS in the treatment of substance use disorders (SUD) using a systematic review.
Methods
Electronic literature search (PsycInfo, Medline until April 2017) identified k = 9 studies (k = 4 randomized-controlled trials, RCTs, with inactive sham and k = 5 open-label studies). DTMS was most commonly applied using high frequency/intensity (10–20 Hz/100–120% of the resting motor threshold, MT) protocols for 10–20 daily sessions in cases with alcohol, nicotine or cocaine use disorders. The outcome measures were craving and dependence (according to standardized scales) or consumption (frequency, abstinence or results of biological assays) at the end of the daily treatment phases and at the last follow-up.
Results
Acute and longer-term (6–12 months) reductions in alcohol craving were observed after 20 sessions (20 Hz, 120% MT) relative to baseline in k = 4 open-label studies with comorbid SUD and major depressive disorder (MDD). In k = 2 RCTs without MDD, alcohol consumption acutely decreased after 10–12 sessions (10–20 Hz, 100–120% MT) relative to baseline or to sham. Alcohol craving was reduced only after higher frequency/intensity DTMS (20 Hz, 120% MT) relative to sham in k = 1 RCT. Nicotine consumption was reduced and abstinence was increased after 13 sessions (10 Hz, 120% MT) and at the 6-month follow-up relative to sham in k = 1 RCT. Cocaine craving was reduced after 12 sessions (15 Hz, 100% MT) and at the 2-month follow-up relative to baseline in k = 1 open-label study while consumption was reduced after 12 sessions (10 Hz, 100% MT) relative to baseline but not to sham in k = 1 RCT.
Conclusions
High-frequency DTMS may be effective at treating some SUD both acutely and in the longer-term. Large RCTs with inactive sham are required to determine the efficacy and the optimal stimulation parameters of DTMS for the treatment of SUD.
Similar content being viewed by others

Background
Deep transcranial magnetic stimulation (DTMS) with the H-coil system is a relatively novel non-invasive brain stimulation method [1]. Since 2013 DTMS is approved by the US Food and Drug Administration (FDA) for treatment-resistant unipolar major depression (MDD). The most commonly utilized DTMS protocol involves high-frequency (18–20 Hz) and high intensity (120% of the resting motor threshold, MT) stimulation delivered for 20 days. Such protocol has acute antidepressant [2, 3] as well as anxiolytic [4] properties in MDD, and tends to improve working memory and executive functioning in MDD and schizophrenia [5, 6].
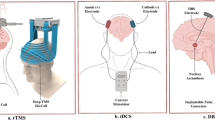
The current focus in the field is to test other therapeutic applications of DTMS beyond MDD [7, 8]. One such application involves the use of DTMS for treatment of substance use disorders (SUD). Since SUD are difficult to treat with only modest responses to available therapies [9], they increase the burden of disease, in particular in comorbid conditions [10]. The evidence to date suggests that depending on the protocols and the coils, the non-invasive, repetitive brain stimulation methods appear to affect the neuroplasticity around the coil as well as throughout the brain [9, 11]. The functional reorganization could affect behaviors related to addiction, including reduction in craving and a better regulation of the compulsive desire to consume the substances [9, 11]. The unique structure of the H-coils is of particular interest because it allows to repetitively stimulate the entire cortex in contrast to other systems offering a more focal stimulation (for example, the figure of eight, F8-coil, used for repetitive transcranial magnetic stimulation, rTMS). Such a broad stimulation with H-coils could increase the electrical field in deeper, subcortical brain regions [12, 13]. Therefore, DTMS with H-coils is a promising candidate for treatment of various SUD that affect similar neural circuitry (deeper cortico-striatal pathways) [14] and share numerous molecular targets [15].
The aim of the current study was to systematically assess the effects of DTMS in the treatment of SUD.
Methods
The current review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16].
Systematic search strategy and study selection
An electronic search of PsycInfo, Medline, and Google Scholar (until April 2017) identified k = 133 studies (Table 1).
Nine studies [17,18,19,20,21,22,23,24,25] met the following inclusion criteria:
-
1)
DTMS applied in cases with any SUD using any type of H-coil,
-
2)
any study designs including double-blind randomized controlled trials (RCTs) with inactive sham groups or open-label designs,
-
3)
parallel designs in case of RCTs (to prevent any carry-over effects),
-
4)
any number of cases/study (including single case studies),
-
5)
SUD assessed at baseline and after DTMS using any method (standardized scales or biological assays).
Studies were excluded if they did not assess SUD (k = 55/83), did not include human data (k = 10/83) or were reviews (k = 9/83; Fig. 1).

Study selection procedure (PRISMA flowchart). Note. Abbreviations: k, number of studies; SUD, substance use disorders
Data coding and outcome measures
Data from k = 9 studies were coded by the authors independently and any inconsistencies were resolved by consensus. Study details (participant characteristics, study designs, SUD assessment methods, and stimulation parameters) are shown in Tables 2, 3 and 4.
The primary outcome measures were craving and dependence (assessed with standardized scales listed in Table 3) or consumption (use frequency, abstinence rate or results of urine, blood or hair analysis; Table 3) at the end of the acute (daily) treatment with DTMS and at the last follow-up. Since some studies included samples with comorbid MDD, the secondary outcome measure was depression severity according to the Hamilton Depression Rating Scale (HDRS).
Risk of bias assessment (RCTs)
The risk of bias in RCTs was assessed using the criteria proposed by Cochrane [26]. The outcomes of this assessment for each individual study are shown in Table 5.
Results
Study details (Tables 2 and 3)
Our review comprises k = 9 studies including k = 5 studies with open-label designs and k = 4 double-blind RCTs with sham control groups. Of all 148 participants, n = 84 received active high-frequency (10–20 Hz) DTMS, n = 50 sham treatment, and n = 14 low-frequency (1 Hz) DTMS. Most participants in all studies were middle-aged and male. Substance-related diagnoses included alcohol use disorders (AUD) in k = 6 studies (n = 39 DTMS, n = 15 sham), nicotine dependence (k = 1; n = 32 high-frequency DTMS, n = 14 low-frequency DTMS, n = 31 sham), and cocaine use disorders (CUD; k = 2, n = 13 DTMS, n = 4 sham). The participants in all studies were seeking treatment for their SUD and were recruited from the general population or from clinics specializing in SUD. Most were heavy, long-term users of alcohol, nicotine or cocaine (average use of 10–46 years) who either did not successfully respond to or relapsed after other treatments. DTMS was administered either as an add-on therapy to antidepressants and/or to mood stabilizers in k = 5 open-label studies or as a monotherapy in k = 4 RCTs.
The last follow-up assessments were conducted at 2–12 months after the last acute DTMS sessions. Once the course of daily stimulation ended, there was no maintenance DTMS treatment in any of the studies. Substance-related cues were presented before DTMS in two studies with AUD or nicotine use disorders, respectively [18, 20].
Stimulation parameters (Table 4)
The majority of studies utilized H1 coil (k = 7) and a high frequency/intensity (10–20 Hz/100–120% of the resting motor threshold, MT) stimulation protocol applied for 10–20 acute (daily or almost daily) sessions. One study [18] also included a low-frequency (1 Hz) stimulation protocol with 120% MT and 13 sessions.
Risk of bias in the RCTs (Table 5)
The quality of the k = 4 RCTs was acceptable in terms of randomization, blinding, and reporting of results. However, the outcome assessment was problematic (underpowered) in three RCTs due to small sample sizes and high attrition. Furthermore, two of the four RCTs were industry-sponsored.
DTMS and SUD (Table 6)
The results synthesized from all k = 9 studies suggest that overall the high-frequency DTMS was effective at treating various symptoms of different SUD, both acutely and in the longer term (Table 6).
Alcohol outcomes
DTMS with H1-coil consistently alleviated AUD symptoms, particularly in k = 4 open-label studies with comorbid AUD and MDD. Specifically, alcohol craving and/or urge was acutely reduced after DTMS (20 sessions/18–20 Hz/120% MT) relative to baseline and at follow-up (6–12 months) relative to baseline. In addition, depression severity was also alleviated, both acutely and at follow-up (6–12 months) relative to baseline in all k = 4 studies.
The acute effects of DTMS were also reported in k = 2 RCTs with inactive sham that included AUD cases without MDD [20, 25]. Daily use was reduced in both RCTs after DTMS relative to baseline or to sham. However, alcohol craving was acutely reduced in only one of the RCTs [20] with a higher frequency/intensity protocol (10 sessions/20 Hz/120% MT) relative to baseline or to sham. The effects of active DTMS relative to sham were not computed and no change in craving was acutely observed after DTMS with lower frequency/intensity (12 sessions/10 Hz/100% MT) relative to baseline in the other RCT [25]. Although the longer-term effects of DTMS on AUD could not be reliably established due to a high drop-out rate in one RCT [20], craving and consumption tended to remain lower in the active DTMS group at follow-up (2–3 months) relative to baseline or to sham.
In addition to the subjective assessment of SUD symptoms (with scales or self-reported frequency of use), both RCTs also reported acutely reduced dopamine activity using biological measures. Specifically, blood cortisol and prolactin levels (markers of dopamine activity) were reduced after DTMS relative to baseline or to sham [20] and striatal dopamine transporter (DAT) availability (measured with the single photon emission computed tomography, SPECT) was reduced after DTMS relative to baseline [25].
Nicotine outcomes
Only one study (RCT with inactive sham) [18] assessed the effects of DTMS with HADD-coil on nicotine use. Although nicotine craving did not differ acutely after DTMS relative to sham, acute nicotine consumption and dependence were reduced and abstinence increased in the high-frequency DTMS groups (13 sessions/10 Hz/120% MT), in particular when DTMS was preceded by a smoking-related cue, relative to sham [18]. The reduction in nicotine consumption and continuous abstinence were also observed in the high-frequency DTMS groups at follow-up (6 months) relative to sham [18]. In contrast, low-frequency DTMS (1 Hz) had poor efficacy and was discontinued [18].
Cocaine outcomes
The effects of DTMS with H1-coil on CUD were assessed in k = 2 studies (one RCT [24] and one open-label study [23]). Cocaine consumption (detected in hair) and craving were acutely reduced after DTMS (12 sessions/10–15 Hz/100% MT) relative to baseline and at follow-up (2–6 months) relative to baseline. However, there was no difference in cocaine consumption between the active DTMS relative to sham in the RCT [24].
Safety
All patients completed the treatment with DTMS in six out of k = 9 studies included in this review. However, high drop-out rates were reported in k = 3 studies (Table 2). The authors of these studies claimed that DTMS is safe because no severe side-effects occurred. Mild adverse reactions to DTMS (headaches, nausea, discomfort) were reported in nine participants in k = 2 studies [18, 24]. Others dropped out due to relapse in SUD or other factors unrelated to treatment, such as inconvenience and other personal reasons.
Discussion
Our review summarizes the preliminary evidence suggesting that high-frequency DTMS might be a promising treatment for cases with SUD who failed to respond to other available treatments. According to data from nine studies, craving, dependence, and consumption of alcohol, nicotine, and cocaine were reduced after daily treatment with DTMS and some of these effects lasted for up to 12 months without maintenance treatment. Although highly interesting, the evidence to date should be interpreted with caution because it is based on studies with open-label designs or RCTs with small sample sizes. Furthermore, the interpretation of results in these studies is difficult due to heterogeneous stimulation protocols, different SUD and SUD outcomes, and high drop-out rates especially after cessation of daily treatment.
While the most optimal stimulation parameters for the treatment of SUD remain unknown [14, 27], the current review shows that various SUD symptoms were alleviated following the high-frequency stimulation protocols. In particular, protocols with higher frequencies/intensities (18–20 Hz, 120% MT) reduced alcohol craving and depression severity in comorbid AUD and MDD, both acutely (after 20 sessions) and at follow-up (6–12 months). Since such protocols produce consistent acute antidepressant effects in MDD with AUD [10] but also in MDD alone [2, 3], the acute reduction in AUD symptoms might have been secondary to the alleviation of MDD symptoms. However, the effects of DTMS cannot be secondary alone because two RCTs without comorbid MDD [20, 25] also reported acute reductions in AUD symptoms after high-frequency DTMS. Thus, high-frequency protocols may acutely reduce the severity of both conditions (MDD and AUD). Protocols with lower frequencies/intensities (10–15 Hz/100% MT) and less daily sessions (10–13) also acutely reduced some aspects of nicotine use and CUD symptoms although the longer-term durability of these effects remains unclear due to the low volume of data. In contrast to high-frequency, low-frequency DTMS (1 Hz) was ineffective at reducing nicotine use [18]. Similar to evidence from rTMS studies [9, 11, 28], the efficacy of DTMS in the treatment of SUD is likely to depend on the length of stimulation in combination with frequency, intensity as well as other stimulation parameters. For example, DTMS outcomes in SUD may depend on the number of stimuli that have been shown to influence the antidepressant outcomes of rTMS with F8-coil [29, 30]. Furthermore, craving for some substances may be reduced based on a complex mechanism requiring both excitation with the high-frequency stimulation (10 Hz) and inhibition with the low-frequency stimulation (1 Hz) according to preliminary evidence from an rTMS study with F8-coil in methamphetamine users [28]. A higher volume of primary data is required to investigate the most optimal parameters of DTMS required for the acute treatment of SUD using multivariate statistical methods. It is also necessary to test the longer-term efficacy of DTMS to improve treatment compliance and reduce relapse after daily treatment.
Although the general idea of applying non-invasive brain stimulation to treat SUD symptoms is not new [9, 11, 27, 31, 32], the mechanism of action of these methods, including DTMS, is still unclear. Past reviews have shown that the high-frequency rTMS with F8-coil is able to transiently reduce craving for various substances [9, 14, 32,33,34,35], possibly due to changes in the dopamine and glutamate activity in the cortico-striato-limbic systems implicated in SUD [9, 14, 15]. These changes may include increased dopaminergic release and/or improved dopaminergic binding in the striatum, although multiple networks and neurotransmitter systems are likely to be involved depending on the type of SUD [36]. In general, although various SUD affect common neural pathways, share common molecular targets, and have similar reinforcing effects, they may access the reward system via different mechanisms [15]. Advancing efficient translational research is required to find new pharmacological treatments for SUD [15]. The non-invasive brain stimulation could be a viable alternative to pharmacotherapy in the short-term and/or could offer a longer-term relief from SUD although it may require some individualization of protocols and/or stimulation sites rather than the ‘one-size-fits-all’ approach [11]. In fact, the unique shape of the H-coil that delivers a broad cortical and presumably deeper, subcortical stimulation [12, 37] may be particularly useful in the longer-term treatment of SUD [38]. Indeed, the current review shows that the effects of DTMS may last for up to 12 months after daily stimulation phases despite the absence of maintenance treatment. It has been suggested that repetitive stimulation is required for persistent and enduring plastic neuroadaptations [11, 31]. In fact, the most consistent and longer-lasting plastic changes in SUD may result from a combination of repetitive, broad, and (presumably) deep stimulation achieved using H-coils with high frequencies (18–20 Hz) and delivered for at least 20 sessions. Such broad and deep stimulation could affect both the multiple nodes of the executive control network and the limbic network implicated in craving [27]. The enhanced cognitive control could also contribute to efficacy of DTMS in comorbid conditions, such as MDD and SUD [36]. If DTMS improves cognition first [5], the recovery of executive functioning could allow patients to subsequently regain cognitive control over their substance craving, as well as their negative mood states [22]. Future research is required to investigate the neurobiological mechanisms and the interaction between the cognitive outcomes and the alleviation of SUD symptoms following DTMS. Furthermore, head-to-head studies directly comparing the effects of various coils (for example, F8-coil and H1-coil) in the treatment of SUD are required to investigate which approach is more effective.
While there is interest in finding new treatments for SUD, the quality of evidence from DTMS studies is only preliminary so far, similar to the evidence from rTMS studies [9, 11]. The current review suggests that apart from assessing various stimulation protocols and the durability of the acute effects, other issues should also be considered in the future DTMS research in SUD. First, large, double-blind RCTs with inactive sham are required to determine the efficacy of DTMS in the treatment of various SUD. The studies reviewed here used open-label designs (k = 5) while the four RCTs with sham groups had only moderate quality at best. All studies reported a relatively low volume of data (only up to 11 cases received active DTMS treatment in eight out of the nine studies) and/or high drop-out rates (33–50% in three out of the nine studies). Therefore, the majority of studies were underpowered and placebo and expectancy effects were not controlled for. A preliminary meta-analysis of the acute effects in studies included in the current review showed a large pooled reduction in craving and dependence after active DTMS relative to baseline (Hedges’ g = 2.65, 95% confidence interval: 1.28–4.02, k = 5 studies [39]). However, this pooled effect was not controlled for sham and there was a trend towards higher effects in open-label studies relative to the RCTs [39]. The effects of DTMS on SUD cannot be explained by placebo/expectancy effects alone for a number of reasons. Trends in the data suggest that DTMS was more effective than sham for some symptoms of alcohol and nicotine use disorders according to three RCTs reviewed here. Furthermore, the subjective reports regarding the reductions in SUD symptom severity after DTMS were confirmed with biological changes, including reductions in either dopamine activity or concentrations of nicotine and cocaine metabolites. Finally, despite the absence of maintenance treatment, eight studies reported that some acute effects of DTMS on SUD tended to last for 2–12 months after the last daily DTMS session. Second, future DTMS studies need to carefully choose the outcome measures. Most studies report the effects of non-invasive brain stimulation on craving rather than the actual use [32]. The subjective self-reports of substance use should also be verified with biological assays. Although substance use tends to be reliably and validly reported in anonymous research contexts [40], it may be underreported in the clinical practice. Third, the clinical characteristics of patients could affect the outcomes of DTMS studies in SUD. The efficacy of DTMS may depend on SUD severity, concurrent pharmacotherapy, and polysubstance use. Our review suggests that DTMS may be most effective in combination with pharmacotherapy for comorbid MDD and AUD or for cases with higher severity of SUD. In contrast, DTMS as a monotherapy or for cases with lower severity of SUD may produce less satisfactory outcomes, possibly leading to higher dropout rates. Polysubstance use also needs to be carefully controlled for because H-coils targeting different neural regions may be required for best efficacy depending on the substance and/or the type of SUD. Finally, although no severe reactions to DTMS were reported, a systematic assessment of DTMS safety in SUD is necessary in future research.
There are a number of other limitations in the current review. First, eight out of nine studies were conducted in Italy. The clinical outcomes of DTMS on SUD symptoms need to be tested in other institutions/countries. Second, the current review considered only published literature from two academic databases. Although it is unlikely that other published studies on the topic exist, currently ongoing studies may provide higher-quality evidence regarding the use of DTMS in the treatment of SUD. Third, the current review is descriptive only and does not report any effect sizes. We conducted a preliminary meta-analysis based on craving and dependence outcomes using data from k = 5 studies [39]. The effect sizes were based on highly heterogeneous data, including different study designs (open-label vs. RCT), SUD types, outcome measures, and stimulation parameters. Therefore, a larger volume of data is required for a more reliable meta-analysis of the effects of DTMS on SUD.
Conclusions
In conclusion, the current review provides preliminary evidence that high-frequency DTMS may be effective at treating some SUD symptoms both acutely and in the longer-term (for 2–12 months after daily treatment). Large RCTs with inactive sham are required to determine the efficacy and the optimal stimulation parameters of DTMS for the treatment of different SUD.
Abbreviations
- AUD:
-
Alcohol use disorder
- CUD:
-
Cocaine use disorder
- DTMS:
-
Deep transcranial magnetic stimulation
- FTND:
-
Fagerstrom test for nicotine dependence
- HDRS:
-
Hamilton Depression Rating Scale
- k :
-
Number of studies
- MT:
-
Resting motor threshold
- n :
-
Sample size at baseline in DTMS groups
- OCDS:
-
Obsessive compulsive drinking scale
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- RCT:
-
Double-blind randomized controlled trial with inactive sham control group
- rTMS:
-
Repetitive transcranial magnetic stimulation
- SPECT:
-
Single photon emission computed tomography
- sTCQ:
-
The short tobacco craving questionnaire
- SUD:
-
Substance use disorder (dependence and/or abuse)
- VAS:
-
Visual analogue scale for craving
References
Zangen A, Roth Y, Voller B, Hallett M. Transcranial magnetic stimulation of deep brain regions: evidence for efficacy of the H-coil. Clin Neurophysiol. 2005;116:775–9.
Kedzior KK, Gellersen H, Brachetti A, Berlim MT. Deep transcranial magnetic stimulation (DTMS) in the treatment of major depression: an exploratory systematic review and meta-analysis. J Affect Disord. 2015;187:73–83.
Levkovitz Y, Isserles M, Padberg F, Lisanby SH, Bystritsky A, Xia G, Tendler A, Daskalakis ZJ, Winston JL, Dannon P, Hafez HM, Reti IM, Morales OG, Schlaepfer TE, Hollander E, Berman JA, Husain MM, Sofer U, Stein A, Adler S, Deutsch L, Deutsch F, Roth Y, George MS, Zangen A. Efficacy and safety of deep transcranial magnetic stimulation for major depression: a prospective multicenter randomized controlled trial. World Psychiatry. 2015;14:64–73.
Kedzior KK, Gellersen H, Roth Y, Zangen A. Acute reduction in anxiety after deep transcranial magnetic stimulation (DTMS) in unipolar major depression- a systematic review and meta-analysis. Psychiatry Res. 2015;230:971–4.
Kedzior KK, Gierke L, Gellersen HM, Berlim MT. Cognitive functioning and deep transcranial magnetic stimulation (DTMS) in major psychiatric disorders: a systematic review. J Psychiatr Res. 2016;75:107–15.
Levkovitz Y, Harel EV, Roth Y, Braw Y, Most D, Katz LN, Sheer A, Gersner R, Zangen A. Deep transcranial magnetic stimulation over the prefrontal cortex: evaluation of antidepressant and cognitive effects in depressive patients. Brain Stimul. 2009;2:188–200.
Kedzior KK, Gellersen HM. Clinical application of deep transcranial magnetic stimulation (DTMS) in neuropsychiatric disorders: a systematic literature review and meta-analysis. Eur Arch Psychiatry Clin Neurosci. 2017;267:34.
Tendler A, Barnea Ygael N, Roth Y, Zangen A. Deep transcranial magnetic stimulation (dTMS) - beyond depression. Expert Rev Med Devices. 2016;13:987–1000.
Hadar A, Zangen A. Brain stimulation as a novel technique for craving management and the treatment of addiction. In: Wilson SJ, editor. The Wiley handbook on the cognitive neuroscience of addiction. USA: Wiley & Sons, Ltd.; 2015.
Rapinesi C, Kotzalidis GD, Ferracuti S, Girardi N, Zangen A, Sani G, Raccah RN, Girardi P, Pompili M, Del Casale A. Add-on high frequency deep transcranial magnetic stimulation (dTMS) to bilateral prefrontal cortex in depressive episodes of patients with major depressive disorder, bipolar disorder I, and major depressive with alcohol use disorders. Neurosci Lett. 2018;671:128–32.
Diana M, Raij T, Melis M, Nummenmaa A, Leggio L, Bonci A. Rehabilitating the addicted brain with transcranial magnetic stimulation. Nat Rev Neurosci. 2017;18:685–93.
Parazzini M, Fiocchi S, Chiaramello E, Roth Y, Zangen A, Ravazzani P. Electric field estimation of deep transcranial magnetic stimulation clinically used for the treatment of neuropsychiatric disorders in anatomical head models. Med Eng Phys. 2017;43:30–8.
Roth Y, Pell GS, Chistyakov AV, Sinai A, Zangen A, Zaaroor M. Motor cortex activation by H-coil and figure-8 coil at different depths. Combined motor threshold and electric field distribution study. Clin Neurophysiol. 2014;125:336–43.
Gorelick DA, Zangen A, George MS. Transcranial magnetic stimulation (TMS) in the treatment of substance addiction. Ann N Y Acad Sci. 2014;1327:79–93.
Karoly HC, YorkWilliams SL, Hutchison KE. Clinical neuroscience of addiction: similarities and differences between alcohol and other drugs. Alcohol Clin Exp Res. 2015;39:2073–84.
Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Rapinesi C, Kotzalidis GD, Serata D, Del Casale A, Bersani FS, Solfanelli A, Scatena P, Raccah RN, Brugnoli R, Digiacomantonio V, Carbonetti P, Fensore C, Tatarelli R, Angeletti G, Ferracuti S, Girardi P. Efficacy of add-on deep transcranial magnetic stimulation in comorbid alcohol dependence and dysthymic disorder: three case reports. Prim Care Companion CNS Disord. 2013;15 https://doi.org/10.4088/PCC.4012m01438.
Dinur-Klein L, Dannon P, Hadar A, Rosenberg O, Roth Y, Kotler M, Zangen A. Smoking cessation induced by deep repetitive transcranial magnetic stimulation of the prefrontal and insular cortices: a prospective, randomized controlled trial. Biol Psychiatry. 2014;76:742–9.
Rapinesi C, Kotzalidis GD, Scatena P, Del Casale A, Janiri D, Callovini G, Piacentino D, Serata D, Raccah RN, Brugnoli R, Digiacomantonio V, Mascioli F, Ferri VR, Ferracuti S, Pompili M, De Pisa E, Di Pietro S, Zangen A, Angeletti G, Girardi P. Alcohol and suicidality: could deep transcranial magnetic stimulation (dTMS) be a possible treatment? Psychiatr Danub. 2014;26:281–4.
Ceccanti M, Inghilleri M, Attilia ML, Raccah R, Fiore M, Zangen A, Ceccanti M. Deep TMS on alcoholics: effects on cortisolemia and dopamine pathway modulation. A pilot study. Can J Physiol Pharmacol. 2015;93:283–90.
Girardi P, Rapinesi C, Chiarotti F, Kotzalidis GD, Piacentino D, Serata D, Del Casale A, Scatena P, Mascioli F, Raccah RN, Brugnoli R, Digiacomantonio V, Ferri VR, Ferracuti S, Zangen A, Angeletti G. Add-on deep transcranial magnetic stimulation (dTMS) in patients with dysthymic disorder comorbid with alcohol use disorder: a comparison with standard treatment. World J Biol Psychiatry. 2015;16:66–73.
Rapinesi C, Curto M, Kotzalidis GD, Del Casale A, Serata D, Ferri VR, Di Pietro S, Scatena P, Bersani FS, Raccah RN, Digiacomantonio V, Ferracuti S, Bersani G, Zangen A, Angeletti G, Girardi P. Antidepressant effectiveness of deep transcranial magnetic stimulation (dTMS) in patients with major depressive disorder (MDD) with or without alcohol use disorders (AUDs): a 6-month, open label, follow-up study. J Affect Disord. 2015;174:57–63.
Rapinesi C, Del Casale A, Di Pietro S, Ferri V, Piacentino D, Sani G, Raccah R, Zangen A, Ferracuti S, Vento A, Angeletti G, Brugnoli R, Kotzalidis G, Girardi P. Add-on high frequency deep transcranial magnetic stimulation (dTMS) to bilateral prefrontal cortex reduces cocaine craving in patients with cocaine use disorder. Neurosci Lett. 2016;629:43–7.
Bolloni C, Panella R, Pedetti M, Frascella AG, Gambelunghe C, Piccoli T, Maniaci G, Brancato A, Cannizzaro C, Diana M. Bilateral transcranial magnetic stimulation of the prefrontal cortex reduces cocaine intake: a pilot study. Front Psychiatry. 2016;7:133.
Addolorato G, Antonelli M, Cocciolillo F, Vassallo GA, Tarli C, Sestito L, Mirijello A, Ferrulli A, Pizzuto DA, Camardese G, Miceli A, Diana M, Giordano A, Gasbarrini A, Di Giuda D. Deep transcranial magnetic stimulation of the dorsolateral prefrontal cortex in alcohol use disorder patients: effects on dopamine transporter availability and alcohol intake. Eur Neuropsychopharmacol. 2017;27:450–61.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savović J, Schulz KF, Weeks L, Sterne JAC. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343 https://doi.org/10.1136/bmj.d5928.
Hanlon CA, Dowdle LT, Austelle CW, DeVries W, Mithoefer O, Badran BW, George MS. What goes up, can come down: novel brain stimulation paradigms may attenuate craving and craving-related neural circuitry in substance dependent individuals. Brain Res. 2015;1628:199–209.
Liu Q, Shen Y, Cao X, Li Y, Chen Y, Yang W, Yuan T-F. Either at left or right, both high and low frequency rTMS of dorsolateral prefrontal cortex decreases cue induced craving for methamphetamine. Am J Addict. 2017;26:776–9.
Fitzgerald P. rTMS in depression: is more always better? Clin Neurophysiol. 2017;128:e3.
Kedzior KK, Azorina V, Reitz SK. More female patients and fewer stimuli per session are associated with the short-term antidepressant properties of repetitive transcranial magnetic stimulation (rTMS): a meta-analysis of 54 sham-controlled studies published between 1997-2013. Neuropsychiatr Dis Treat. 2014;10:727–56.
Feil J, Zangen A. Brain stimulation in the study and treatment of addiction. Neurosci Biobehav Rev. 2010;34:559–74.
Salling, MC, Martinez, D. Brain stimulation in addiction. Neuropsychopharmacology. 2016;41:2798–2809.
Grall-Bronnec M, Sauvaget A. The use of repetitive transcranial magnetic stimulation for modulating craving and addictive behaviours: a critical literature review of efficacy, technical and methodological considerations. Neurosci Biobehav Rev. 2014;47:592–613.
Hone-Blanchet A, Ciraulo DA, Pascual-Leone A, Fecteau S. Noninvasive brain stimulation to suppress craving in substance use disorders: review of human evidence and methodological considerations for future work. Neurosci Biobehav Rev. 2015;59:184–200.
Jansen JM, Daams JG, Koeter MW, Veltman DJ, van den Brink W, Goudriaan AE. Effects of non-invasive neurostimulation on craving: a meta-analysis. Neurosci Biobehav Rev. 2013;37:2472–80.
Dunlop K, Hanlon CA, Downar J. Noninvasive brain stimulation treatments for addiction and major depression. Ann N Y Acad Sci. 2016; https://doi.org/10.1111/nyas.12985.
Schmittwilken L, Schuchinsky M, Kedzior K. Neurobiological mechanisms of deep transcranial magnetic stimulation (DTMS): a systematic review. Brain Stimul. 2017;10:379.
Barr MS, George TP. Deep repetitive transcranial magnetic stimulation for smoking cessation: is going deeper better? Biol Psychiatry. 2014;76:678–80.
Kedzior K, Gerkensmeier I, Schuchinsky M. How deep is the deep transcranial magnetic stimulation (DTMS)? Putative stimulation of reward pathways in substance use disorders: a systematic review and meta-analysis. Brain Stimul. 2017;10:355.
Kedzior K, Badcock J, Martin-Iverson M. Validity and consistency of self-reports regarding substance use in general research volunteers, including regular cannabis users and schizophrenia patients. Subst Use Misuse. 2006;41:743–50.
Ross HE, Gavin DR, Skinner HA. Diagnostic validity of the MAST and the alcohol dependence scale in the assessment of DSM-III alcohol disorders. J Stud Alcohol. 1990;51:506–13.
Fagerström KO, Schneider NG. Measuring nicotine dependence: a review of the Fagerstrom tolerance questionnaire. J Behav Med. 1989;12:159–82.
Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62.
Anton RF, Moak DH, Latham P. The obsessive compulsive drinking scale: a self-rated instrument for the quantification of thoughts about alcohol and drinking behavior. Alcohol Clin Exp Res. 1995;19:92–9.
Heishman SJ, Singleton EG, Pickworth WB. Reliability and validity of a short form of the tobacco craving questionnaire. Nicotine Tob Res. 2008;10:643–51.
Vakili S, Sobell LC, Sobell MB, Simco ER, Agrawal S. Using the timeline Followback to determine time windows representative of annual alcohol consumption with problem drinkers. Addict Behav. 2008;33:1123–30.
McMillan DE, Gilmore-Thomas K. Stability of opioid craving over time as measured by visual analog scales. Drug Alcohol Depend. 1996;40:235–9.
Acknowledgements
Some data reported in this article were presented by the first author at the 2nd International Brain Stimulation Conference, Barcelona (March 2017).
Funding
There was no funding for the research reported in this article.
Availability of data and materials
All data generated or analysed during this study are included in this article.
Author information
Authors and Affiliations
Contributions
KKK conceptualized the study and performed the literature search; all authors coded the data; KKK wrote the manuscript, all authors critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kedzior, K.K., Gerkensmeier, I. & Schuchinsky, M. Can deep transcranial magnetic stimulation (DTMS) be used to treat substance use disorders (SUD)? A systematic review. BMC Psychiatry 18, 137 (2018). https://doi.org/10.1186/s12888-018-1704-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-018-1704-0