
Abstract
Background
Several studies have investigated the cognitive profile in patients with Anorexia Nervosa (AN) and Bulimia Nervosa (BN); on the contrary few studies have evaluated it in patients with Binge Eating Disorder (BED). The purpose of this study was to compare decision making, central coherence and set-shifting between BED and AN patients.
Methods
A battery of neuropsychological tests including the Iowa Gambling Task (IGT), the Rey-Osterrieth Complex Figure Test (RCFT), the Wisconsin Card Sorting Test (WCST), the Trial Making Task (TMT) and the Hayling Sentence Completion Task (HSCT) were administered in a sample of 135 women (45 AN, 45 BED, 45 Healthy Controls [HC]). Furthermore, Beck Depression Inventory (BDI) was administered to evaluate depressive symptoms. Years of education, age, Body Mass Index (BMI) and depression severity were considered as covariates in statistical analyses.
Results
BED and AN patients showed high rates of cognitive impairment compared to HC on the domains investigated; furthermore, the cognitive profile of BED patients was characterised by poorer decision making and cognitive flexibility compared to patients with AN. Cognitive performance was strongly associated with depressive symptoms.
Conclusions
In the present sample, two different neurocognitive profiles emerged: a strong cognitive rigidity and a central coherence based on the details was predominant in patients with AN, while a lack of attention and difficulty in adapting to changes in a new situation seemed to better describe patients with BED. The knowledge of the different cognitive profiles of EDs patients may be important for the planning their psychotherapeutic intervention.
Similar content being viewed by others


Background
Cognitive flexibility (i.e., the mental ability to adjust thinking or attention in response to changing goals and/or environmental stimuli) has been widely studied in patients with Eating Disorders (EDs) [1,2]. Most of these studies were conducted with female patients with Anorexia Nervosa (AN) or Bulimia Nervosa (BN) demonstrating strong cognitive rigidity [3,4]. Inflexibility is a typical feature of AN [5] and is evident in ED related thoughts (e.g., categorising food as good or bad, thinking about calories, fat or sugar content, etc.), behaviours (e.g., calculating calories consumed and/or burned, continuous body shape and weight control, ritualised exercise pattern, etc.) and difficulties in finding alternative ways of dealing with a problem. Interestingly, extreme weight condition (EWC) groups like AN patients and obese subjects (OB) have shown similar dysfunctional executive profiles [6,7].
Binge Eating Disorder (BED) is an ED characterised by recurring episodes of over eating associated with lack of control during which patients eat large amounts of food [8]. In contrast to BN, recurrent inappropriate compensatory behaviours to counterbalance the consequences of bingeing are absent, for this reason patients with BED are frequently obese. Several studies have shown that BED patients have a higher lifetime prevalence of other psychiatric disorders such as personality [9], anxiety and mood disorders [10]. Few studies have assessed cognitive flexibility among patients with BED; in all cases BED patients were compared to OB [11-16].
A recent functional MRI study has shown neurocognitive impairment in BED, particularly in the reward circuitry of the brain [17]. More specifically, BED patients showed diminished recruitment of the ventral striatum and the inferior frontal gyrus during the anticipatory phase of reward processing and reduced activity in the medial prefrontal cortex during the outcome phase of reward processing. In three studies [12,15,16], obese individuals with BED showed impaired decision-making compared with people without BED [12], and BED overweight women performed more poorly on neuropsychological testing than people without BED [15,16]. However, in other studies [13,14] no significant differences emerged between people with and without BED on cognitive testing.
Studies have shown that people with cognitive impulsivity (i.e., the inability to weigh the consequences of immediate and future events and, consequently, inability to delay gratification) like BED patients, found themselves in trouble in certain situations because their decision-making pattern was influenced by immediate rewards [13,18]; furthermore attentional/executive deficit played an important role in the development and maintenance of obesity and EDs [19,20]. In fact, the possible comorbidity between BED and Attention Deficit Hyperactivity Disorder (ADHD) - characterised by symptoms of impulsivity, hyperactivity and inattention - has been highlighted [21,22].
Based on the above, the purpose of the present study was to assess and compare BED and AN patients on the three most widely studied domains of cognition (i.e., set-shifting, central coherence and decision-making) through neuropsychological testing. We hypothesised that, similarly to AN patients, BED patients might also exhibit a pathological but different pattern of cognition in the following way: BED patients would exhibit more errors in the decision-making task, more non-perseverative errors in the set-shifting domain and poorer central coherence than AN patients.
Methods
Patients and procedures
The sample for this study consisted of 135 female participants: 45 patients with AN Restrictive type, 45 patients diagnosed with BED and 45 healthy controls (HC). Patients were consecutively recruited at an Ambulatory for Treatment of EDs and were diagnosed by experienced clinicians according to DSM-IV-TR [8] diagnostic criteria, using the structured clinical interview for DSM IV Axis I disorders (SCID-I) [23].
The interviewers were clinicians who worked in the field of EDs who were trained in the administration of SCID and neuropsychological tests and used these tools in their daily clinical practice. An expert psychologist in this field supervised the interviewers during the data collection.
HC participants were recruited at the local University and the Socio-Psycho-Pedagogical High School of the city. Prior to assessment, they were all interviewed and asked about the lifetime presence of an ED or other axis I diagnosis (i.e. mood disorder, anxiety disorder, psychotic disorder, impulse-control disorder), history of being underweight [Body Mass Index (BMI) <17.5] and obesity (BMI ≥30) and were excluded if so. Patients and HC were all Caucasian.
Inclusion criteria in the clinical groups were: AN Restrictive type or BED diagnosis according to DSM-IV TR. All participants were subject to the following exclusion criteria: a) male gender, b) drug dependence, c) use of psycho-active medications, d) cognitive deficits as indicated by Mini Mental State Examination score <24 [24], e) history of chronic medical illness or neurological condition that might affect cognitive function, f) head trauma with loss of consciousness for more than 2 minutes, g) other severe medical comorbidity (e.g., epilepsy or diabetes), h) BMI < 14 for AN patients. Furthermore, following the indications of other researchers, individuals older than 45 years were excluded [13,14].
Participants were informed about the aim of the study, that participation was voluntary, that personal data would be kept confidential and that no extra credit would be given to students for their participation. All partakers, or their parents on behalf of those younger than eighteen, signed a written informed consent according to the Ethical Committee, before entering the study. The study, approved by the Ethical Committee of Azienda Ospedaliera Universitaria Mater Domini, was conducted from July 2013 to June 2014.
Measures
Neuropsychiatric assessment
ED psychopathology was assessed by means of the Eating Disorder Inventory-2 (EDI-2) [25] and the Binge Eating Scale (BES) [26] and depression severity was evaluated with the Beck Depression Inventory (BDI) [27].
EDI-2
The EDI-2 is a self-report questionnaire that assesses the psychopathology of EDs using 91 items on a six-point Likert-type scale from 0 ‘never’ to 6 ‘always’ coded with a 3-point system where ‘sometimes’ , ‘rarely’ and ‘never’ were assigned zeros while ‘often’ , ‘usually’, and ‘always’ were assigned a score of 1, 2 and 3, respectively. Subscales measured by the test were: Drive for Thinness (DT), Bulimia (B), and Body Dissatisfaction (BD), Perfectionism (P), Interoceptive Awareness (IA), Maturity Fears (MF), Ineffectiveness (I), and Interpersonal Distrust (ID), Asceticism (A), Social insecurity (SI), and Impulse Regulation (IR). Cronbach’s alpha in the present study was 0.91.
BES
The BES is an easily administered test with adequate internal consistency and validity that has been widely used in research either to measure binge eating severity in the non-purge binge eating population or to determine whether potential research participants meet the inclusion criteria of binge eating. It is made up of 16 items describing the behavioural manifestations, feelings and cognitions associated with binge eating. Each item consisted of four statements that reflected a range of severity from which subjects chose the one that best described perceptions and feelings about their own eating behaviour. Total BES score <17 indicated unlikely BED, 17–27 score possible BED and values >27 probable BED. BES was only administered to BED patients in order to further corroborate the diagnosis. Cronbach’s alpha in this study was 0.89.
BDI
The BDI self-report questionnaire is widely used to assess the severity of depressive symptoms and consisted of 21 items. The first thirteen items assessed the cognitive-affective sphere and the remaining eight converged into the performance-somatic symptoms scale. The clinical cut-off has been set at 16; scores between 0–9, 10–16, 17–29 and ≥30 indicated minimum, mild, moderate and severe depression respectively. Cronbach’s alpha in this study was 0.91.
Anthropometric measures
Participants, wearing light indoor clothing and no shoes, were measured using a portable stadiometer (Seca 220, GmbH & Co., Hamburg, Germany) and a balance scale (Seca 761, GmbH & Co., Hamburg, Germany); their standing height to the nearest 0.1 cm and body weight to the nearest 0.1 kg were taken the morning of the assessment. Then the individual’s BMI (= kg.m−2) was calculated.
Neuropsychological assessment
All participants were assessed with the following neuropsychological tests: a) Iowa Gambling Task (IGT) [28]; b) Rey-Osterrieth Complex Figure Test (RCFT) [29]; c) Trial Making Task (TMT) [30]; d) Wisconsin Card Sorting Test (WCST) [31]; e) Hayling Sentence Completion Test (HSCT) [32].
IGT
The computerised version of the original IGT was used to assess decision making. The subject was given a virtual amount of money to play with; the task required selecting one hundred cards from four decks. By selecting one card over another, the participant can either gain or gain-and-lose virtual money. Decks A and B were disadvantageous in the long run because the total gain was lower than the total loss, whereas decks C and D were advantageous because although the gains were lower, the penalties were also lower. The goal of the task was to make the most profit. Decision-making ability was determined by examining IGT performance over time; this was done by dividing the 100 card choices in five blocks of 20 trials. Performance was measured by calculating a ‘net score’ for each block; this was obtained by counting card picks from advantageous decks (C + D) minus the number from disadvantageous decks (A + B) in each block [i.e., (C + D) - (A + B)]. Higher results indicated better performance, while negative results indicated a preference for the disadvantageous decks.
RCFT
The RCFT is a test used to assess visual organisation, short-term visual memory and visuospatial abilities. The subject must copy and recall, after an interval of 3 minutes, a complex geometric figure. The accuracy of the reproduction of all the details of the figure was a measure of visuospatial and visual memory abilities. In addition, the RCFT can be used to examine organisational strategies used during the copy condition. It is possible to calculate a Central Coherence Index (CCI) that results from the order of construction index (drawing of global or local elements in the first stage of the copy task) and the Style Index (the degree of continuity in the drawing process). The CCI ranges from 0 (detailed) to 2 (global). Drawing style was assessed using both Savage’s [33] and Booth’s [34] scoring systems.
TMT
Cognitive flexibility was measured using a pencil-and-paper version of the TMT. The test was divided into two parts: in Part A, the subject must join with a continuous line the circles containing the numbers from 1 to 25 in ascending order; in Part B the subject must alternately join, always with a continuous line, a number (1 to 13) and a letter (A to N) that are found in circles in a random order on the page. The first part assessed visuospatial and motor skills of the subject; the second part assessed cognitive flexibility; more specifically, the time taken to carry out Part B of the task and the subtraction of time A from time B was considered a measure of cognitive flexibility.
WCST
The WCST was administered according to the Italian normative data [35]. It was used to assess the executive function deficits and required participants to match stimulus cards that vary in geometric shapes, colour and number of items per card. In the standard administration, the examiner does not inform the participant of the rule for correct matching (e.g., colour, shape, number of items on card) but simply responds ‘right’ or ‘wrong’ after each guess. In addition, the rule for correct matching changes without warning after the participant correctly matches 10 consecutive cards. The global score [number of trials – (number of achieved categories × 10)], Perseverative Errors, Non-Perseverative Errors, and Failures to maintain set were scored.
HSCT
The HSCT is a measure of response initiation and response suppression. We used the Italian adapted version of the HSCT [36] that consisted of 20 sentences in which the final word was missing; in Part A the examiner reads 10 sentences aloud and the participant has to simply complete each one, yielding a simple measure of response initiation speed. Part B requires subject to complete 10 sentences with a nonsense ending word (and suppress a sensible one), giving measures of response suppression ability and thinking time. Two practice sentences are read to the participants before each section. Participants are encouraged to respond as fast as they can. Other indexes provided by Part B are the type of answers: Type C Answer for sentence completion, Type S for semantic-related answers and Type U for semantic-unrelated answers. The sum of the Answers S and C provided the error score. The last index was the Average time of Type U answers.
All the neuropsychological measures were administered in the same session in this order: TMT, WCST, IGT, RCFT (copy), HSCT, RCFT (recall).
Statistical analyses
Data were analysed using the Statistical Package for Social Sciences Version 21 (SPSS, Chicago, Illinois, USA). Anova followed by Bonferroni post hoc test was used to evaluate significant differences between AN, BED and HC. A univariate general linear model (UGLM) was used to check the influence of age, years of education, BMI and depressive symptoms (BDI score) on neuropsychological test performances. The first step was to evaluate differences in the neuropsychological tests for diagnosis and the second step was to evaluate the influence of age, education, BMI and BDI score as covariates. The level of statistical significance was set at p ≤ 0.05.
Results
The sample consisted of 135 female participants, 45 per group.
Clinical and demographic features of the sample
Table 1 describes the main characteristics of the sample, the scores of BDI and EDI-2 and the comparisons between groups. Significant differences were evident regarding age (F = 11.412; p < .001), years of education (F = 15.159; p < .001) and BMI (F = 289.725; p < .001) between groups and thus were included in the UGLM as covariates.
Significant differences were also evident with regard to BDI (F = 70.543; p < .001): BED patients exhibited the highest scores in BDI corresponding to a moderate degree of depression, AN patients reported mild depression whereas HC reported minimum depression. Thus the BDI score was also included in the UGLM as covariate.
Regarding EDI-2, BED patients had significantly higher means in B and BD and lower P than AN patients and higher scores for all subscales of EDI-2 except for P compared to HC. Finally, AN patients had significantly higher means than HC in all EDI-2 subscales with the only exception of B.
Table 2 shows the results of the neuropsychological assessment and the comparison between groups.
Decision making
-
IGT. Total Score was significantly lower for BED and AN patients compared to HC participants. Furthermore, BED performed significantly lower than HC on Blocks 3 and 5 while AN performed significantly lower than HC in Blocks 2 and 3 (Figure 1).
Figure 1 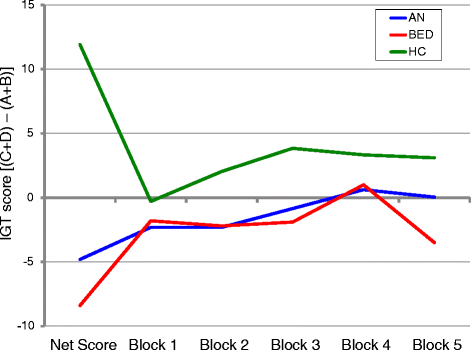
Iowa Gambling Task:performance in Eating Disorder groups and Healthy Controls. Mean net score and net number of chosen cards [(C + D) – (A + B)] across the five blocks each consisting of 20 trials by AN, BED and HC groups. Positive scores reflect advantageous performance whereas negative scores indicate the opposite.

Cognitive flexibility
-
HCST. BED performed better than AN and HC in Part A of HCST; contrarily BED had a significantly lower performance in Average time of Type U answers compared to both AN and HC. They also had poorer performance than HC in Part B, Part B-Part A and provided more type S and U answers. Interestingly no significant differences were found between AN and HC on HSCT. Differences between groups remained significant in Part B-Part A when correcting for age, and in Average time Type U answers when correcting for age and BDI scores.
-
TMT. Significant differences emerged between AN and BED patients compared to HC in the number of errors in Part B. Moreover, BED patients performed worse than AN and HC in Part B and Part B-Part A. These last differences remained significant between groups when correcting for age and years of education.
-
WCST. BED patients also had the worst performance in all indexes except on perseverative errors compared to AN and HC; AN performed significantly worse than HC in all subscales. Differences between groups remained significant in Global score, Non perseverative errors and Failure to maintain the set when correcting for diagnosis; when analysis were corrected for BMI, the differences in Global score and Non perseverative errors remained significant.
Central coherence
-
RCFT. BED had the lowest score on Rey-Accuracy Index compared to AN and HC in the copy condition of the RCFT; furthermore they had a significantly poorer performance on RCFT Percentage of recall than HC. The differences between groups remained significant after controlling for age, BMI, BDI score, years of education and diagnosis.
Discussion
The aim of this study was to assess and compare BED and AN patients on the three most widely studied domains of cognition through neuropsychological testing. BED and AN patients showed high rates of cognitive impairment compared to HC on the domains investigated; furthermore the profile of BED patients was characterised by a poorer performance in decision making along the test, poorer cognitive flexibility and lower accuracy during the RCFT compared to patients with AN.
To our knowledge this is the first study to compare BED and AN patients on a wide range of neuropsychological tests (i.e., decision-making, set-shifting and central coherence).
Regarding decision-making strategies, our results were in line with recent literature on the performance of BED [12,14] and AN [3,37] patients. In fact, our data showed that BED had lower Total Score and lower values in the 3rd and the 5th Block (and thus worse results), indicating a difficulty in finding a correct strategy for the test. In agreement with other authors [12], BED patients often made more risky decisions than HC, showing impaired capacities to advantageously utilise feedback processing. Instead AN patients compared to HC group had lower Total Score and lower values in the second and third blocks of IGT, denoting greater insensitivity to feedback in early stages of the test.
HSCT was previously used only twice in the field of EDs [3,38] and BED patients were not involved. In our study, the most interesting results were those regarding BED who did Part A faster than AN and HC, yet they provided more Type S answers and took longer to give Type U answers in Part B. The results in Part A may be explained by their higher impulsivity, a typical trait associated with BED [39,40]; instead, the lower performance in Part B reflected more severe cognitive flexibility impairment. Furthermore, although no significant differences emerged between AN and HC, AN performed worse in all indexes. Significantly worse performance compared to HC in Type S and U answers have been described among AN patients [3].
Regarding TMT, BED patients were significantly slower than AN and HC in TMT Part B and proportional score Part B-Part A, according to another study [12], that indicated lower executive functioning among BED. Duchesne et al. [14] pointed out that BED obese hardly reached significant differences from non-BED obese; others found no differences on cognitive functioning performances between morbidly obese individuals with and without BED [15] so authors concluded that ‘obesity rather than binge eating, may be directly related to cognition’. In our study, AN patients had a worse performance in the number of errors on Part B compared to HC. Even if TMT is widely used in the literature, it provides controversial results [3,41-43] so another explanation may be given. Perfectionism, a characteristic psychological AN trait, leads to cognitive rigidity; nevertheless it can be of advantageous help for AN patients as it furthers the drive for good performance through a higher cognitive effort [44] which was not found among other ED patients.
Interesting results emerged in WCST. Research has demonstrated a worse performance by AN patients compared to HC [3,45,46]; our results were in accordance with those findings. In fact AN patients performed worse than HC group in all subscales. Nevertheless BED group was revealed to be the most impaired: they failed to find an appropriate strategy, as demonstrated by the high number of non-perseverative errors and the number of failures to maintain set. It could be read as if BED followed a trial-and-error strategy. On the other hand, AN patients committed more perseverative errors demonstrating more cognitive rigidity. Other authors [14] found not only a greater difficulty to maintain the set but also more perseverative errors in obese with BED than in obese controls; this last result should be better addressed comparing BED obese patients with AN and normal-weight HC in order to ascertain if this is a real or a relative increment of perseverative errors.
Finally, significant differences emerged on RCFT. Although this test was previously used with AN patients [41,47-50], this was the first time it was applied in the context of BED. BED patients showed a lower score on Rey-Accuracy index compared to AN and HC in the copy condition; furthermore BED had a significantly poorer performance on RCFT percentage of recall than HC. Even if our results were not statistically significant they showed a trend towards significance and thus they seem to be in line with previous studies [41,43,47,48] confirming that AN patients have lower central coherence (e.g., low order, style and central coherence) than HC. It was as if they drew their copy based on the details of the picture rather than oriented to it globally.
Thus, poor central coherence seems to be the characteristic feature of AN patients while poor attention, rather than lack of central coherence, is the distinctive trait of BED patients.
In this study depression interfered with cognitive performance as it negatively correlated with cognitive flexibility; in our case BED patients showed longer average time of Type U answers in HCST that could be explained by slowed thinking - a characteristic symptom of patients with depression. Cognitive impairments are common in Major Depression [51] and reflect the general inability to concentrate [8,52]. An inverse correlation between depression severity and cognitive performance in domains of executive function among others has been reported [53] and studies have demonstrated how depression also interferes with cognitive performance among ED patients [3,54-57]. The present results confirmed this influence in patients with BED. Possible explanations can be different. On the one hand, BED patients were more severely depressed, and depression is a frequently comorbid disorder in this ED [10,58-60]; on the other hand, BED participants were older and had less education. Age is related to lower cognitive flexibility and slower information processing that might explain a longer reaction time to TMT and HCST [61,62]. Education may reflect the skill level that patients acquired through the school years [63]. Further, people with depression are less attentive to details and the low RCFT Accuracy among BED patients could support it.
Body weight (BMI) was significantly associated with poor cognitive flexibility (WCST) in the sense that extreme weight conditions performed worse than HC. More specifically BED performed worse than AN, and AN worse than HC. Fagundo et al. [6] also found that AN and OB made significantly more errors than controls and had significantly fewer correct responses in WCST.
Although our findings provided a pattern of cognitive impairment for AN and BED, the present study was limited in several ways. The first limit could be the lack of an obese non-BED control group to better assess the cognitive profile across the extreme eating/weight conditions, and in greater detail between obese BED and non-BED [11-16]. Second, ours was a cross-sectional study, and results could change in the long term after therapy. Third, nutritional indexes (i.e., glycemia, hypertension, level of serotonin and dopamine) were not provided but there is evidence of their involvement in human cognition [64-66]. Finally, although contrasting data exist about the influence of anxious symptomatology on neurocognitive performance of ED patients [43,67-69], the present research did not take this variable into consideration; therefore future studies should include measures of anxiety symptoms to better clarify its effects, if any, on these domains.
Conclusions
BED patients, and likewise other subjects with EDs, exhibited a pathological cognitive pattern. AN patients showed impaired cognitive flexibility, decision making and central coherence. Compared to patients with AN, the cognitive profile of BED was characterised by poorer decision making and cognitive flexibility. Thus, two different neurocognitive profiles emerged: a strong cognitive rigidity and a central coherence based on the details appeared predominant in patients with AN, while a lack of attention and difficulty in adapting to changes in a new situation seemed to better describe patients with BED. The knowledge of the different cognitive profiles of EDs patients may be important for the planning their psychotherapeutic intervention.
Abbreviations
- ED:
-
Eating Disorder
- AN:
-
Anorexia Nervosa
- BN:
-
Bulimia Nervosa
- EWC:
-
Extreme weight condition
- OB:
-
Obese subjects
- BED:
-
Binge Eating Disorder
- ADHD:
-
Attention Deficit Hyperactivity Disorder
- HC:
-
Healthy controls
- BMI:
-
Body mass index
- EDI-2:
-
Eating Disorder Inventory 2
- DT:
-
Drive for thinness
- B:
-
Bulimia
- BD:
-
Body dissatisfaction
- IA:
-
Interoceptive awareness
- ASC:
-
Asceticism
- P:
-
Perfectionism
- MF:
-
Maturity fears
- IR:
-
Impulse regulation
- IN:
-
Ineffectiveness
- SI:
-
Social insecurity
- ID:
-
Interpersonal distrust
- BES:
-
Binge Eating Scale
- BDI:
-
Beck Depression Inventory
- IGT:
-
Iowa Gambling Task
- HCST:
-
Hayling Sentence Completion Test
- TMT:
-
Trial Making Task
- WCST:
-
Wisconsin Card Sorting Test
- RCFT:
-
Rey-Osterrieth Complex Figure Test
- UGLM:
-
Univariate General Linear Model
References
Roberts ME, Tchanturia K, Stahl D, Southgate L, Treasure J. A systematic review and meta-analysis of set-shifting ability in eating disorders. Psychol Med. 2007;37:1075–84.
Stedal K, Frampton I, Landrø NI, Lask B. An examination of the ravello profile–a neuropsychological test battery for anorexia nervosa. Eur Eat Disord Rev. 2012;20:175–81.
Abbate-Daga G, Buzzichelli S, Amianto F, Rocca G, Marzola E, McClintock SM, et al. Cognitive flexibility in verbal and nonverbal domains and decision making in anorexia nervosa patients: a pilot study. BMC Psychiatry. 2011;11:162.
Stedal K, Rose M, Frampton I, Landrø NI, Lask B. The neuropsychological profile of children, adolescents, and young adults with anorexia nervosa. Arch Clin Neuropsychol. 2012;27:329–37.
Merwin RM, Timko CA, Moskovich AA, Ingle KK, Bulik CM, Zucker NL. Psychological inflexibility and symptom expression in anorexia nervosa. Eat Disord. 2011;19:62–82.
Fagundo AB, de la Torre R, Jiménez-Murcia S, Agüera Z, Granero R, Tárrega S, et al. Executive functions profile in extreme eating/weight conditions: from anorexia nervosa to obesity. PLoS One. 2012;7:e43382.
Wu M, Brockmeyer T, Hartmann M, Skunde M, Herzog W, Friederich HC. Set-shifting ability across the spectrum of eating disorders and in overweight and obesity: a systematic review and meta-analysis. Psychol Med. 2014;44:3365–85.
American Psychiatric Association: DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Revised. Washington, DC:American Psychiatric Association; 2000.
Friborg O, Martinussen M, Kaiser S, Øvergård KT, Martinsen EW, Schmierer P, et al. Personality disorders in eating disorder not otherwise specified and binge eating disorder: a meta-analysis of comorbidity studies. J Nerv Ment Dis. 2014;202:119–25.
Grilo CM, White MA, Masheb RM. DSM-IV psychiatric disorder comorbidity and its correlates in binge eating disorder. Int J Eat Disord. 2009;42:228–34.
Danner UN, Ouwehand C, van Haastert NL, Hornsveld H, de Ridder DT. Decision-making impairments in women with binge eating disorder in comparison with obese and normal weight women. Eur Eat Disord Rev. 2012;20:e56–62.
Svaldi J, Brand M, Tuschen-Caffier B. Decision-making impairments in women with binge eating disorder. Appetite. 2010;54:84–92.
Davis C, Patte K, Curtis C, Reid C. Immediate pleasures and future consequences. A neuropsychological study of binge eating and obesity. Appetite. 2010;54:208–13.
Duchesne M, Mattos P, Appolinário JC, de Freitas SR, Coutinho G, Santos C, et al. Assessment of executive functions in obese individuals with binge eating disorder. Rev Bras Psiquiatr. 2010;32:381–8.
Galioto R, Spitznagel MB, Strain G, Devlin M, Cohen R, Paul R, et al. Cognitive function in morbidly obese individuals with and without binge eating disorder. Compr Psychiatry. 2012;53:490–5.
Manasse SM, Juarascio AS, Forman EM, Berner LA, Butryn ML, Ruocco AC. Executive functioning in overweight individuals with and without loss-of-control eating. Eur Eat Disord Rev. 2014;22:373–7.
Balodis IM, Grilo CM, Kober H, Worhunsky PD, White MA, Stevens MC, et al. A pilot study linking reduced fronto-Striatal recruitment during reward processing to persistent bingeing following treatment for binge-eating disorder. Int J Eat Disord. 2014;47:376–84.
Nederkoorn C, Smulders FT, Havermans RC, Roefs A, Jansen A. Impulsivity in obese women. Appetite. 2006;47:253–6.
Smith E, Hay P, Campbell L, Trollor JN. A review of the association between obesity and cognitive function across the lifespan: implications for novel approaches to prevention and treatment. Obes Rev. 2011;12:740–55.
Raman J, Smith E, Hay P. The clinical obesity maintenance model: an integration of psychological constructs including mood, emotional regulation, disordered overeating, habitual cluster behaviours, health literacy and cognitive function. J Obes. 2013;2013:240128. doi:10.1155/2013/240128.
Mattos P, Saboya E, Ayrão V, Segenreich D, Duchesne M, Coutinho G. Comorbid eating disorders in a Brazilian attention deficit/hyperactivity disorder adult clinical sample. Rev Bras Psiquiatr. 2004;26:248–50.
Fernández-Aranda F, Agüera Z, Castro R, Jiménez-Murcia S, Ramos-Quiroga JA, Bosch R, et al. ADHD symptomatology in eating disorders: a secondary psychopathological measure of severity? BMC Psychiatry. 2013;13:166.
First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM IV Axis I Disorders (SCID-I), Clinician Version, Administration Booklet. Washington: American Psychiatric Publishing Inc; 1997.
Folstein MF, Folstein SE, McHugh PR. Mini-Mental State. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98.
Garner DM. Eating Disorder Inventory 2: Professional manual. Odessa: Psychological Assessment Resources; 1991.
Gormally J, Black S, Daston S, Rardin D. The assessment of binge eating severity among obese persons. Addict Behav. 1982;7:47–55.
Beck A, Ward C, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–71.
Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50:7–15.
Rey A. L'examen psychologique dans les cas d'encéphalopathie traumatique. Archives de Psychologie. 1941;28:215–85.
Reitan RM. Validity of the Trail Making test as an indicator of organic brain damage. Percept Mot Skills. 1958;8:271–6.
Berg EA. A simple objective technique for measuring flexibility in thinking. J Gen Psychol. 1948;39:15–22.
Burgess P, Shallice T. The Hayling and Brixton Tests. Test manual. Bury St Edmunds: Thames Valley Test Company; 1997.
Savage CR, Baer L, Keuthen N, Brown HD, Rauch SL, Jenike MA. Organizational strategies mediate nonverbal memory impairment in obsessive-compulsive disorder. Biol Psychiatry. 1999;45:905–16.
Booth R. Local–global Processing and Cognitive Style in Autism Spectrum Disorders and Typical Development. London: King’s College London; 2006.
Laiacona M, Inzaghi MG, De Tanti A, Capitani E. Wisconsin card sorting test: a new global score, with Italian norms, and its relationship with the Weigl sorting test. Neurol Sci. 2000;21:279–91.
Shallice T, Marzocchi GM, Coser S, Del Savio M, Meuter RF, Rumiati RI. Executive function profile of children with attention deficit hyperactivity disorder. Dev Neuropsychol. 2002;21:43–71.
Galimberti E, Fadda E, Cavallini MC, Martoni RM, Erzegovesi S, Bellodi L. Executive functioning in anorexia nervosa patients and their unaffected relatives. Psychiatry Res. 2013;208:238–44.
Pignatti R, Bernasconi V. Personality, clinical features, and test instructions can affect executive functions in Eating Disorders. Eat Behav. 2013;14:233–6.
Hege MA, Stingl KT, Kullmann S, Schag K, Giel KE, Zipfel S, et al. Attentional impulsivity in binge eating disorder modulates response inhibition performance and frontal brain networks. Int J Obes (Lond). 2014. doi:10.1038/ijo.2014.99.
Schag K, Teufel M, Junne F, Preissl H, Hautzinger M, Zipfel S, et al. Impulsivity in binge eating disorder: food cues elicit increased reward responses and disinhibition. PLoS One. 2013;16:e76542.
Tenconi E, Santonastaso P, Degortes D, Bosello R, Titton F, Mapelli D, et al. Set-shifting abilities, central coherence, and handedness in anorexia nervosa patients, their unaffected siblings and healthy controls: Exploring putative endophenotypes. World J Biol Psychiatry. 2010;11:813–23.
Konstantakopoulos G, Tchanturia K, Surguladze SA, David AS. Insight in eating disorders: clinical and cognitive correlates. Psychol Med. 2011;41:1951–61.
Roberts ME, Tchanturia K, Treasure J. Exploring the neurocognitive signature of poor set-shifting in anorexia and bulimia nervosa. J Psychiat Res. 2010;44:964–70.
Fassino S, Daga GA, Pierò A, Delsedime N. Psychological factors affecting eating disorders. Adv Psychosom Med. 2007;28:141–68.
Danner UN, Sanders N, Smeets PA, van Meer F, Adan RA, Hoek HW, et al. Neuropsychological weaknesses in anorexia nervosa: set-shifting, central coherence, and decision making in currently ill and recovered women. Int J Eat Disord. 2012;45:685–94.
Tchanturia K, Davies H, Roberts M, Harrison A, Nakazato M, Schmidt U, et al. Poor cognitive flexibility in eating disorders: examining the evidence using the Wisconsin Card Sorting Task. PLoS One. 2012;7:e28331.
Favaro A, Santonastaso P, Manara R, Bosello R, Bommarito G, Tenconi E, et al. Disruption of visuospatial and somatosensory functional connectivity in anorexia nervosa. Biol Psychiatry. 2012;72:864–70.
Lopez C, Tchanturia K, Stahl D, Booth R, Holliday J, Treasure J. An examination of the concept of central coherence in women with anorexia nervosa. Int J Eat Disord. 2008;41:143–52.
Lopez C, Tchanturia K, Stahl D, Treasure J. Weak central coherence in eating disorders: A step towards looking for an endophenotype of eating disorders. J Clin Exp Neuropsychol. 2009;31:117–25.
Lindner SE, Fichter MM, Quadflieg N. Central coherence in full recovery of anorexia nervosa. Eur Eat Disord Rev. 2013;21:115–20.
Castaneda AE, Tuulio-Henriksson A, Marttunen M, Suvisaari J, Lönnqvist J. A review on cognitive impairments in depressive and anxiety disorders with a focus on young adults. J Affect Disord. 2008;106:1–27.
Marazziti D, Consoli G, Picchetti M, Carlini M, Faravelli L. Cognitive impairment in major depression. Eur J Pharmacol. 2010;626:83–6.
McDermott LM, Ebmeier KP. A meta-analysis of depression severity and cognitive function. J Affect Disord. 2009;119:1–8.
Galderisi S, Bucci P, Mucci A, Bellodi L, Cassano GB, Santonastaso P, et al. Neurocognitive functioning in bulimia nervosa: the role of neuroendocrine, personality and clinical aspects. Psychol Med. 2011;41:839–48.
Weider S, Indredavik MS, Lydersen S, Hestad K. Neuropsychological function in patients with anorexia nervosa or bulimia nervosa. Int J Eat Disord. 2014. doi:10.1002/eat.22283.
Giel KE, Wittorf A, Wolkenstein L, Klingberg S, Drimmer E, Schönenberg M, et al. Is impaired set-shifting a feature of "pure" anorexia nervosa? Investigating the role of depression in set-shifting ability in anorexia nervosa and unipolar depression. Psychiatry Res. 2012;200:538–43.
Tchanturia K, Liao PC, Uher R, Lawrence N, Treasure J, Campbell IC. An investigation of decision making in anorexia nervosa using the Iowa Gambling Task and skin conductance measurements. J Int Neuropsychol Soc. 2007;13:635–41.
Javaras KN, Pope HG, Lalonde JK, Roberts JL, Nillni YI, Laird NM, et al. Co-occurrence of binge eating disorder with psychiatric and medical disorders. J Clin Psychiatry. 2008;69:266–73.
American Psychiatric Association Workgroup on Eating Disorders. Practice guideline for the treatment of patients with eating disorders (revision). Am J Psychiat. 2006;163:1–39.
Faulconbridge LF, Bechtel CF. Depression and disordered eating in the obese person. Curr Obes Rep. 2014;3:127–36.
Ferreira D, Molina Y, Machado A, Westman E, Wahlund LO, Nieto A, et al. Cognitive decline is mediated by gray matter changes during middle age. Neurobiol Aging. 2014;35:1086–94.
Salthouse TA. When does age-related cognitive decline begin? Neurobiol Aging. 2009;30:507–14.
Guerrero-Berroa E, Ravona-Springer R, Schmeidler J, Silverman JM, Sano M, Koifmann K, et al. Age, gender, and education are associated with cognitive performance in an older Israeli sample with type 2 diabetes. Int J Geriatr Psychiatry. 2014;29:299–309.
Klanker M, Feenstra M, Denys D. Dopaminergic control of cognitive flexibility in human and animals. Front Neurosci. 2013;7:201.
Lakhan SE, Kirchgessner A. The emerging role of dietary fructose in obesity and cognitive decline. Nutr J. 2013;12:114.
Schmitt JA, Wingen M, Ramaekers JG, Evers EA, Riedel WJ. Serotonin and human cognitive performance. Curr Pharm Des. 2006;12:2473–86.
Talbot A, Hay P, Buckett G, Touyz S: Cognitive deficits as an endophenotype for anorexia nervosa: An accepted fact or a need for re-examination? Int J Eat Disord 2014, Jul 21. doi:10.1002/eat.22332. [Epub ahead of print]
Billingsley-Marshall RL, Basso MR, Lund BC, Hernandez ER, Johnson CL, Drevets WC, et al. Executive function in eating disorders: the role of state anxiety. Int J Eat Disord. 2013;46:316–21.
Friederich HC, Wu M, Simon JJ, Herzog W. Neurocircuit function in eating disorders. Int J Eat Disord. 2013;46:425–32.
Acknowledgements
Authors are grateful to Prof. Maria Pavia from Università degli Studi Magna Graecia di Catanzaro (Italy) and Prof. Isabelle Durand-Zaleski from Université Paris Est Créteil (France) for their help to resolve the statistical dilemmas. Authors are also grateful to the Department of Culture, Education and Research of the Region Calabria for the financial support to this research. Finally, authors thank participants for the time they have given to this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
All authors declare that they have no competing interests.
Author’s contributions
CSG designed the study. MA, AB, MC, AP and MR collected the data. CSG and MA performed the statistical analyses. CSG and MA wrote the first draft of the manuscript. PDF and MAC made the first critical review and participated to write the final manuscript. All authors commented on and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Aloi, M., Rania, M., Caroleo, M. et al. Decision making, central coherence and set-shifting: a comparison between Binge Eating Disorder, Anorexia Nervosa and Healthy Controls. BMC Psychiatry 15, 6 (2015). https://doi.org/10.1186/s12888-015-0395-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-015-0395-z