
Abstract
Background
The association between diet, symptoms and health related quality of life in children and young people with Juvenile idiopathic arthritis (JIA) is not clearly understood. The objectives of this systematic review and meta-analysis were to explore the evidence for a relationship between nutritional status, dietary intake, arthritis symptoms, disease activity and health-related quality of life in children and young people with JIA considering both observational and interventional studies separately.
Method
The databases PubMed, CINAHL, PsycINFO, Web of Science and Cochrane were searched in October 2019, updated in September 2020 and October 2021. Searches were restricted to English language, human and age (2–18 years old). Studies were included if they measured the effect of dietary supplements, vitamins or minerals, or diet in general, on quality of life and/ or arthritis symptom management. Two researchers independently screened titles and abstracts. Full texts were sourced for relevant articles. PRISMA guidelines were used for extracting data. For variables (vitamin D and disease activity), a random-effects meta-analysis model was performed. Two authors using a standardized data extraction form, extracted data independently.
Results
11,793 papers were identified through database searching, 26 studies met our inclusion criteria with 1621 participants. Overall studies quality were fair to good. Results from controlled trial and case control studies with total 146 JIA patients, found that Ɯ-3 PUFA improved the mean active joint count (p < 0.001), Juvenile Arthritis Disease Activity Score (JADAS-27) (p < 0.001) and immune system (≤ 0.05). Furthermore, n-3 and n-6 PUFAs have a negative correlation with CRP (C-reactive protein) and ESR (erythrocyte sedimentation rate) (p < 0.05). Improvement in JIA symptoms were observed in one case, one pilot and one exploratory study with overall 9 JIA patients after receiving Exclusive Enteral Nutrition (EEN) which contains protein and what is required for a complete nutrition, A clinical trial study found Kre-Celazine nutrition (composed of a proprietary alkali buffered, creatine monohydrate and fatty acids mixture) in 16 JIA patients improved symptoms of JIA. No association was found between vitamin D and disease activity from three studies. Height and weight values in relation to healthy controls varied across studies (p = 0.029).
Conclusions
We were only able to include small studies, of lower design hierarchy, mainly pilot studies. We found some evidence of lower height and weight across studies in JIA, but were unable to confirm an association between diet, symptoms and health-related quality of life in children and young people with JIA. Well-designed, carefully measured and controlled interventional studies of dietary patterns in combination with important contributing factors such as medication and lifestyle behaviours, including physical activity, are required to determine the impact of diet in improving symptoms and growth patterns in children and young people with JIA, with an aim to improve the quality of their life.
Trial registration
PROSPERO [CRD42019145587].
Similar content being viewed by others


Introduction
Juvenile idiopathic arthritis (JIA) is the most prevalent autoimmune rheumatic disease in the paediatric population, with a prevalence of approximately one in 1000 [1, 2] and a significant cause of short and long-term disabilities [3]. Young people with JIA have a poorer Health-related quality of life (HRQOL) as compared with healthy peers related to the chronic relapsing nature of the condition, unpredictable disease course, symptom management and long-term treatments [4,5,6,7]. The cause of JIA is still unknown, yet it is likely to involve both genetic susceptibility and environmental factors [8]. Lifestyle factors, including diet, are important determinants of health and wellbeing in young people living with JIA, with the implementation of nutrition interventions including vitamin D suggested to potentially regulate disease severity and associated symptoms through an effect on the immune system [9]. Recently it has also been suggested that vitamin D is an environmental factor that, affects the prevalence of autoimmune diseases by modulating the immune system [10]. Whilst, the potential mechanism has been highlighted, the influence of vitamin D dosage in both the development of JIA and disease activity is still unclear [11]. The impact of diet and nutrition is difficult to interpret in the paediatric population, particularly those with rheumatic disease, due to family influence, dietary regulation and data collection in children [12, 13]. Suboptimal nutrition is suggested to adversely affect the long-term outcome of this group of children and is a source of considerable concern to parents and patients alike [11]. Nutritional deficits affect the general well-being of the child, may adversely affect disease control and contribute to growth disturbance. Considering the potential benefits of diet on short and long-term health and wellbeing, a better understanding of optimal dietary approaches is of value and could inform the development of management strategies. Despite the importance of diet and its potential impact on the HRQOL in children and young adults with JIA, the dietary factors associated with better outcomes are not clearly understood, with the literature varying in quality and including heterogeneous outcomes. The overall aim of this systematic review and meta-analysis is to assess the quality and extent of the evidence of the relationship between nutritional status, dietary intake, arthritis symptoms, disease activity and health-related quality of life in children and young people with JIA considering both observational and interventional studies separately.
Methods
This study was performed following Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines [14]. The protocol for this review was registered with PROSPERO [CRD42019145587].
Data sources and searches
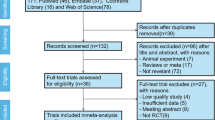
The following databases were used from inception to October 2019 to conduct searches: PubMed, CINAHL, Cochrane, PsycINFO and Web of Science. Search was updated in September 2020 and October 2021. The full search strategy is included in Fig. 1. Six researchers were involved in this systematic review. Two researchers independently screened titles and abstracts. Full texts were sourced for relevant articles. Inclusion criteria were assessed independently.

Study selection flow diagram
Eligibility criteria
Observational research, including baseline intervention or control arm data, longitudinal, control trial, randomised controlled trial and case studies were included in this systematic review and meta-analysis. Studies were included that measured the effect of dietary patterns, vitamin/mineral levels or supplements on disease activity, symptoms such as fatigue, pain, inflammation and quality of life in JIA. Searches were restricted to English language publications, human and age (2–18 years old) but no date restrictions were imposed. These criteria are derived from the literature review and consensus opinion of experts.
Data extraction
Two authors using a standardized data extraction form extracted data independently. Extracted data included study characteristics, baseline demographics of participants, description of the intervention, subtypes of arthritis, measurement, interventions, primary and secondary outcomes.
Outcomes. The primary outcome of this systematic review and meta-analysis was to assess the evidence of the extent of the relationship of dietary intake (patterns, vitamins/mineral levels or supplements) on the quality of life in children and adolescents with JIA. The additional outcome was to assess the evidence of the extent of the effect of dietary supplements or diet on disease activity and symptoms of arthritis, including pain, fatigue, joint stiffness, inflammation, weight and height.
Assessment of risk of bias and quality of evidence. Two researchers independently assessed the quality of all included trials by using the Cochrane Collaboration risk of bias tool [15]. If two of the domains were rated as high, the study was considered to be at high risk of bias. The NIH quality assessment tool was applied to assess the quality of observational cohorts, case–control, case series and cross-sectional studies [16]. For the case report, JBI critical appraisal checklist was used [17]. Any discrepancy was resolved over the discussion by another reviewer.
Data synthesis and analysis
A descriptive analysis of each study is provided in Fig. 2. Where four studies reported on a variable, forest plots were used to show the point estimate (95% CIs) for each study. For variables (vitamin D and disease activity), correlation, number of participants, 95%CIs and data weight were calculated using a random-effects meta-analysis model. Standard errors were calculated by converting 95% CIs using the following formula: SD = N × (upper bound of the CI − lower bound of the CI)/3.92 [18].

Association Vitamin D and disease activity
Results
Identification and selection of relevant studies
An overview of the study identification process is provided in Fig. 1. The initial search yielded 11,793 records; after the removal of duplicates and based on title and abstract, 380 papers were retrieved for more detailed evaluation. The full texts of the remaining 355 articles were reviewed against the study selection criteria, and 26 studies that met our inclusion criteria were included.
Study characteristics
A summary of the characteristics of the selected studies is listed in Tables 1 and 2. Of the 26 selected articles, there were five from the United States, three from Brazil and Sweden, two from Ukraine, Turkey and Finland, and one from Egypt, Bulgaria, Poland, Italy, Norway, United Kingdom, Australia, Morocco and China. Seven were cross-sectional (601participants), seven were case controls (526 participants), three were randomised control trials (153 participants), one case study, one pilot study with one participant, one cross-sectional cohort with 80 participants, one clinical trial with 16 participants, two control trials with 69 participants, two cross-sectional studies with control group with 167 participants and one exploratory study with seven participants. The most recent classification system International League of Associations for Rheumatology (ILAR) was used in 15(57.6%) studies to identify arthritis, while three studies used the American college of rheumatology (ACR), and the remaining studies did not mention their classification. In the majority of patient populations, there were greater numbers of females. Oligoarticular JIA was the most common disease category reported across all the studies.
Risk of bias
From the randomised trials, one study [20] had an overall low risk of bias, and two had some concern [19, 23], while the remaining trials [12, 21, 22] had an overall high concern. For the cross-sectional studies, overall, four studies had good quality [9, 33, 36, 38] while others were fair [10, 32, 34, 35, 37, 39]. In assessing the risk of bias for case–control studies, two out of six studies had fair quality [28, 30], four were in a good category [26, 27, 29, 31] and one in poor [25]. The pilot and exploratory studies were of good quality [40, 41], and the case study was fair [24] (Table 3).
Results from observational studies
Nutritional status, vitamin and mineral levels and energy intake in JIA
According to Mortensen [36], mean energy intakes were significantly below the recommended dietary intake (RDI) in the systemic group (p = 0.01), and in the polyarticular group mean energy intake, calcium, and zinc were below the RDI (p = 0.001). Vitamin C, A and zinc levels for both systemic and polyarticular groups were significantly lower than the control group (p ≤ 0.01, p ≤ 0.05, p ≤ 0.05 respectively) [31], while copper was higher (p ≤ 0.05) [36]. There were no significant differences for copper and zinc between juvenile chronic arthritis (JCA) and the control group (p = 0.644, p = 0.938, respectively), yet in both groups, the mean copper and zinc intakes were below the RDI [36]. Regarding protein–energy malnutrition (PEM), 28% of JIA patients had nutritional abnormalities, which is more prevalent among polyarticular types [34].
Gonçalves and colleagues [33] evaluated plasma homocysteine (Hcy), vitamin B12 and folate in 51 JIA patients and 52 healthy controls. Results were not significant; however, higher average plasma Hcy and folate levels were observed in participants with JIA compared to controls (p = 0.615, p < 0.001, respectively), whilst there was no difference in vitamin B12 concentration in patients and controls (p = 0.341).
Honkanen and others [28], in a case–control study with 137 participants, assessed vitamin A and E levels in juvenile chronic arthritis (JCA). Only vitamin E levels were significantly lower in JCA compared to the control group (p < 0.001).
Juvenile idiopathic arthritis and body mass indexes.
Bacon et al. [31] showed a positive correlation between height for age and weight for height (p = + 0.6, P ≤ 0.02) in 14 children with polyarticular arthritis. A negative correlation was found between weight and height in eight patients with systemic arthritis (r =—0.8, P < 0.015), yet no correlation was found between these variables in the pauciarticular group with 12 patients.
Haugen and colleagues [26] reported that eight children with polyarticular arthritis had a significantly lower weight compared to both 17 healthy controls (p = 0.01) and seven children with pauciarticular arthritis (p = 0.02). Similarly, Lofthouse et al. [27] found that in 22 patients with JIA, height and weight were lower compared to healthy control; however, the observed differences were not significant (p = 0.096, 0.075, respectively). 15 polyarticular patients had significantly lower weight and height compared with 22 healthy participants (p = 0.047 and 0.045 respectively), while the results were not significant in seven pauciarticular JIA (p = 0.389, 0.605 respectively).
Mortensen et al. [36] reported that mean height and weight Z scores were significantly below the Z scores in the general population, in the systemic and polyarticular (p = 0.009, p = 0.02, P = 0.001 respectively) groups (n = 25). There was no significant difference in the mean weight for height index between the systemic, polyarticular and pauciarticular groups.
Pelajo et al. [9] found in their cross-sectional study that only 28 out of 154 patients with JIA were obese, while Caetano [39] mentioned all 42 girls with JIA had higher median Z-BMI scores (p = 0.034) compared with 35 healthy controls. According to Grönlund [33], 40 JIA patients were overweight when compared to 40 matched controls (p = 0.029), however, there was no significant difference for height between groups (p = 0.11). There were no significant differences in weight and height between 66 JIA patients and 42 healthy controls (p = 0.26, p = 0.38 respectively) reported by Gorczyca [30].
Disease activity and health-related quality of life in relation to dietary patterns and supplements in JIA.
Gorczyca and colleagues [30] in a case–control study with 110 participants found that omega 3 and omega 6 PUFAs negatively correlated with inflammatory markers ESR and CRP (p < 0.05).
According to Çakır et al. [37], serum 25(OH) vitamin D levels of the 100 healthy subjects were significantly higher compared to the vitamin D levels of the patient group with 117 participants (p < 0.01). There was no statistically significant correlation between vitamin D levels and the number of joints with active arthritis (r = 0.1, p = 0.4). In a retrospective study by Çomak et al. [38] with 47 participants, no significant difference was found between disease activity and 25(OH) D levels in children who consumed vitamin D supplements compared those who did not (p = 0.053 and p = 0.021, respectively), whereas there was a significant negative correlation between 25(OH) D levels and disease activity as described by JADAS-27(p = 0.01, r = -0.37, d = -0.7965). Pelajo et al. [9] in a cross-sectional study with 154 participants reported serum 25(OH) D levels were not associated with JADAS-27 (beta coefficient = 0.002; 95%CI = -0.1, 0.1; p = 0.97), although in new-onset patients there was a negative correlation (r = -029 and d = -0.60) and positive correlation with long term JIA patients (r = 0.06, d = 0.12). Shevchenko et al. [25] in a case control study with 84 participants found no relationship between vitamin D and disease activity (r = -0.11, p > 0.05). In another cross-sectional study by Bouaddi et al. [10] with 40 participants Serum 25(OH)D levels were associated with disease activity (p = 0.04, β: − 3.87) (Fig. 2).
Results from interventional studies
Disease activity and health-related quality of life in relation to dietary patterns and supplements in JIA.
Gheita and colleagues [22] in a controlled trial study with 47 participants, evaluated the effect of dietary supplements of Ɯ-3 PUFA for 12 weeks intervention, with an improvement in the mean active joint count (p < 0.001) and Juvenile Arthritis Disease Activity Score 27(JADAS-27) (p < 0.001) in JIA group. However, there is a high risk of bias in the study based on the Cochrane tool for randomised trials. Similarly, Yareman et al. [23] in a randomised controlled trial with 68 participants, demonstrated the ω-3 PUFA over three months of intervention had a positive effect on the comprehensive treatment of inflammatory diseases (p = 0.05) even though there are some concerns in the study.
According to Tang et al. [19] disease activity did not improve after receiving vitamin D supplements for 24 weeks in 18 children with JIA (P > 0.05). Berntson et al. [24, 40, 41], in one case and one pilot study with one participant, and one exploratory study with seven participants, reported that inflammation, pain and disease activity improved after full nutrition with EEN (which contains protein and what is required for complete nutrition). Furthermore, EEN reduced inflammatory proteins such as MCP-2, MCP-3 and MCP-4 (monocyte chemoattractant protein), resulting in clinical improvement in 7 patients with JIA. Golini, in a clinical trial study with 16 participants, showed that Kre-Celazine nutritional supplement (composed of a proprietary alkali buffered, creatine, monohydrate and fatty acids mixture) have improved pain and decreased inflammatory indexes (ESR and CRP). [21].
Dilandro et al. [12] in a control trial study including 22 participants showed biscuit supplementation enriched with an iron over the 4-month period, decreased the inflammatory indexes particularly ESR (p = 0.002).
Discussion
To our knowledge, this is the first systematic review and meta-analysis to look at the evidence for the impact of diet interventions, supplements and other nutritional factors in children and young people with JIA. Importantly there were no studies assessing particular dietary patterns on symptoms in JIA.
Overall, based on the findings from interventional non-controlled studies, there was some evidence that dietary supplements Kre-Celazine and full nutrition by EEN may have potential for a beneficial effect on symptoms such as pain, inflammatory markers and disease activity in patients with JIA. However, this should be interpreted with caution as controlled studies with larger sample sizes in children are required to confirm the results. Although, observations from the research in adults should be considered where an association between disease severity in arthritis and food intake has been demonstrated [42] and the role of the gastrointestinal mucosal immune system in the pathogenesis of rheumatoid arthritis has been strongly evidenced [42].
We further observed that in two controlled trial and one case control studies, ω-3 FAs reduced pain, joint tenderness, morning stiffness, inflammatory markers, and over time, the NSAIDs dose needed by JIA patients in addition to improvement of the JADAS-27, CHAQ scores and improved immune system [20, 21, 26]. This is similar to most studies on ω-3 FAs in RA adults. However, findings in those with JIA should be interpreted with caution, as studies covered a relatively small group of patients with a high dropout rate and thus prone to bias. It may be beneficial to do high-quality research with a larger sample size to clarify the efficacy of ω-3 FAs in children and young people with JIA.
Research is conflicting in regards to the impact of vitamin D on rheumatic symptoms in both children and adults. With respect to vitamin D levels in children and young adults with JIA, two out of six studies [10, 38] reported a significant negative correlation between disease activity and 25(OH) vitamin D levels independent of age, gender, JIA subtype, disease duration, medications and BMI. In addition, patients with higher disease activity levels have vitamin D deficiency. These results are consistent with similar studies in adults [43,44,45,46]. Other studies in children with JIA have yielded contradictory results [9, 19, 37, 45] and did not observe a relationship between 25(OH) D level and disease activity, which is consistent with the findings by Braun-Moscovici et al. [47] in adults. Despite being of fair to high quality, future studies with larger sample sizes that consider and adapt analysis for other contributing factors, and importantly studies in new-onset and long-term JIA patients are required to confirm the results of the above studies.
There was some evidence from observational studies for the relationship of dietary supplements and blood markers of vitamins and minerals to growth rate, weight and disease activity and life quality with overall poorer diet relating to worse health. However, the data was variable and difficult to interpret in relation to today's cohort of children due to the study designs, studies span a significant time, through which there have been substantial developments in the treatment of JIA specifically the widespread use of biologic medications. Well-designed interventional studies required.
Regarding nutrient status [35], disease activity and subtype of the disease, there are no significant differences when compared to plasma copper and zinc levels. Bacon et al. [31] confirmed the results of this study. However, children with JIA as well as healthy children presented lower RDI of copper and zinc [35]. For those with JIA, this may signify a greater deficit, as there may be an increase in the requirements caused by the inflammatory process [26]. On the other hand, the study by Stark reported that [20] in taking calcium from food in children with JIA was increased by behavioural change interventions, while previous intervention studies on calcium have used calcium supplements, calcium-enriched foods, to achieve increases in calcium intake.
Considering anthropometric measurements, one study [32] found that children with JIA had more total body fat compared with healthy children. These findings agreed with studies by Knops [48] and Summers [49]. These results are inconsistent with the studies by Haugen, Lofthouse and Mortensen (26, 34, 36) who showed that weight and height were reduced in JIA patients, although differences in measurements between the JIA patients and controls were not statistically significant. Lack of significance could be due to the small number of participants in the study; studies with a greater sample size are required to assess the anthropometric measures in JIA patients.
To its strength, a comprehensive and inclusive search strategy were used and composed with input from a literature-searching specialist and implemented across multiple databases.
The main limitation of this review is bias due to heterogeneity, in which individual studies varied in their inclusion/exclusion of specific JIA subtypes. Due to resource constraints, only studies in English were included; however, we felt it unlikely that this led to omission of major relevant studies.
Conclusion
To our knowledge and based on the results of this systematic review and meta-analysis, there is no study to date that assesses the relationship between dietary intake, symptoms and health-related quality of life in children and young people with JIA. The findings of this systematic review indicate that supplements such as Ɯ-3 FAs and full nutrition by EEN may show potential for improving JIA symptoms, while other supplements, including vitamin D, were found not to be associated with improvement of JIA symptoms nor a better quality of life. In addition, the reporting of weight and height, in some studies indicates children with arthritis had a significantly lower weight than healthy controls, while in other studies, obesity was reported to be greater in children and young people with JIA. Different countries with different nutritional norms, routines and supplementation might justify the differences. It is not clearly understood to what extent diet causes low levels of different nutrient components. It could as well be the disease itself, caused by aberrations in the gastrointestinal function, the possibility to absorb nutritional components, or caused by medication etc. Well-designed, carefully measured interventional studies of dietary patterns in combination with important contributing factors such as medication and life style behaviours including physical activity are required to determine the impact of diet in improving symptoms and growth patterns in children and young people with JIA, with an aim to improve the quality of their life.
References
Thierry S, Fautrel B, Lemelle I, Guillemin F. Prevalence and incidence of juvenile idiopathic arthritis: A systematic review. Joint Bone Spine. 2014;81(2):112–7.
Costello R, McDonagh J, Hyrich KL, Humphreys JH. Incidence and prevalence of juvenile idiopathic arthritis in the United Kingdom, 2000–2018: results from the Clinical Practice Research Datalink. Rheumatology. 2021;61(6):2548–54.
Minden K. Adult Outcomes of Patients with Juvenile Idiopathic Arthritis. Horm Res. 2009;72(suppl 1):20–5. https://doi.org/10.1159/000229759.
Shaw KL, Southwood TR, Duffy CM, McDonagh JE. Health-related quality of life in adolescents with juvenile idiopathic arthritis. Arthritis Rheum. 2006;55(2):199–207. https://doi.org/10.1002/art.21852. PMID: 16583399.
Gutiérrez-Suárez R, Pistorio A, Cespedes Cruz A, Norambuena X, Flato B, Rumba I, Harjacek M, Nielsen S, Susic G, Mihaylova D, Huemer C, Melo-Gomes J, Andersson-Gare B, Balogh Z, De Cunto C, Vesely R, Pagava K, Romicka AM, Burgos-Vargas R, Martini A, Ruperto N; Pediatric Rheumatology International Trials Organisation (PRINTO). Health-related quality of life of patients with juvenile idiopathic arthritis coming from 3 different geographic areas. The PRINTO multinational quality of life cohort study. Rheumatology (Oxford). 2007 Feb;46(2):314–20. doi: https://doi.org/10.1093/rheumatology/kel218. Epub 2006 Jul 28. PMID: 16877459.
Oliveira S, Ravelli A, Pistorio A, Castell E, Malattia C, Prieur AM, Saad-Magalhães C, Murray KJ, Bae SC, Joos R, Foeldvari I. Proxy-reported health-related quality of life of patients with juvenile idiopathic arthritis: the Pediatric Rheumatology International Trials Organization multinational quality of life cohort study. Arthritis Rheum. 2007;57(1):35–43.
Amine B, Rostom S, Benbouazza K, et al. Health related quality of life survey about children and adolescents with juvenile idiopathic arthritis. Rheumatol Int. 2009;29:275–9. https://doi.org/10.1007/s00296-008-0672-y.
Weiss JE, Ilowite NT. Juvenile idiopathic arthritis. Rheumatic Disease Clinics of North America. 2007;33(3):441–70.
Pelajo CF, Lopez-Benitez JM, Kent DM, Price LL, Miller LC, Dawson-Hughes B. 25-hydroxyvitamin D levels and juvenile idiopathic arthritis: is there an association with disease activity? Rheum Int. 2012;32(12):3923–9.
Bouaddi I, Rostom S, El Badri D, Hassani A, Chkirate B, Abouqal R, Amine B, Hajjaj-Hassouni N. Vitamin D concentrations and disease activity in Moroccan children with juvenile idiopathic arthritis. BMC Musculoskelet Disord. 2014;15(1):1–5.
Lovell DJ, Henderson CJ, Warady B, et al. Role of nutrition in juvenile rheumatoid arthritis. In: Ekvall S, Wheby E, editors., et al., Nutritional needs of the child with a handicap or a chronic illness. Cincinnati (OH) Cincinnati University Affiliated Center for Developmental Disorders; 1987. p. 105–19.
Dilandro G, De Cosmi V, Corona F, Torcoletti M, Petaccia A, Filocamo G, et al. May biscuits contribute to iron balance? An observation in children with juvenile idiopathic arthritis. Int J Food Sci Nutr. 2015;66(7):811–4.
Magni-Manzoni S, Pistorio A, Labo E, Viola S, Garcia-Munitis P, Panigada S, et al. A longitudinal analysis of physical functional disability over the course of juvenile idiopathic arthritis. Ann Rheum Dis. 2008;67(8):1159–64.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151:W65-94. https://doi.org/10.7326/0003-4819-151-4-200908180-00136.
Shinichi A. Cochrane Handbook for Systematic Reviews of Interventions. Online Kensaku. 2014;35:154–5.
Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016;6(12):e011458.
Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Lisy K, Qureshi R, Mattis P, Mu P. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z (Editors). JBI Manual for Evidence Synthesis. JBI, 2020.
Higgins JPT. Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0 (updated March 2011). Cochrane Collaboration website. http://training.cochrane.org/handbook. 2011. Accessed November 22, 2017.
Tang T, Zhang Y, Luo C, Liu M, Xu L, Tang X. Adjunctive vitamin D for the treatment of active juvenile idiopathic arthritis: An open-label, prospective, randomized controlled trial. Exp Ther Med. 2019 Dec;18(6):4921–4926. doi: https://doi.org/10.3892/etm.2019.8133. Epub 2019 Oct 25. PMID: 31798713; PMCID: PMC6880388.
Stark LJ, Janicke DM, McGrath AM, Mackner LM, Hommel KA, Lovell D. Prevention of Osteoporosis: A Randomized Clinical Trial to Increase Calcium Intake in Children with Juvenile Rheumatoid Arthritis. J Pediatr Psychol. 2006;30(5):377–86.
Golini J, Jones WL. Kre-Celazine((R)) as a viable treatment for juvenile rheumatoid arthritis/juvenile idiopathic arthritis - a pilot study. J Med Food. 2014;17(9):1022–6.
Gheita T, Kamel S, Helmy N, El-Laithy N, Monir A. Omega-3 fatty acids in juvenile idiopathic arthritis: effect on cytokines (IL-1 and TNF-alpha), disease activity and response criteria. Clin rheum. 2012;31(2):363–6.
Yarema N, Fedortsiv O, Palasiuk B. Influence of ω-3 polyunsaturated fatty acids on the structure of immunocompetent cell membranes and the parameters of cellular and humoral immunity in children with rheumatoid arthritis. Fam Med Primary Care Rev. 2018;20(1):78–82.
Berntson L. Anti-inflammatory effect by exclusive enteral nutrition (EEN) in a patient with juvenile idiopathic arthritis (JIA): brief report. Clin Rheumatol. 2014;33(8):1173–5.
Shevchenko N, Khadzhynova Y. Juvenile idiopathic arthritis and vitamin d status in ukrainian patients. Georgian Med News. 2019;294:88–91 PMID: 31687956.
Haugen MA, Hoyeraal HM, Larsen S, Gilboe IM, Trygg K. Nutrient intake and nutritional status in children with juvenile chronic arthritis. Scand J Rheumatol. 1992;21(4):165–70.
Lofthouse CM, Azad F, Baildam EM, Akobeng AK. Measuring the nutritional status of children with juvenile idiopathic arthritis using the bioelectrical impedance method. Rheumatology Oxford. 2002;41(10):1172–7.
Honkanen VE, Pelkonen P, Konttinen YT, Mussalo-Rauhamaa H, Lehto J, Westermarck T. Serum cholesterol and vitamins A and E in juvenile chronic arthritis. Clin Exp Rheumatol. 1990;8(2):187–91.
Harper RP, Brown CM, Triplett MM, Villasenor A, Gatchel RJ. Masticatory function in patients with juvenile rheumatoid arthritis. Pediatr Dent. 2000;22(3):200–6.
Gorczyca D, Postepski J, Czajkowska A, Pasciak M, Prescha A, Olesinska E, et al. The profile of polyunsaturated fatty acids in juvenile idiopathic arthritis and association with disease activity. Clin Rheumatol. 2017;36(6):1269–79.
Bacon MC, White PH, Raiten DJ, Craft N, Margolis S, Levander OA, et al. Nutritional status and growth in juvenile rheumatoid arthritis. Sem Arthritis Rheum. 1990;20(2):97–106.
Gronlund MM, Kaartoaho M, Putto-Laurila A, Laitinen K. Juvenile idiopathic arthritis patients with low inflammatory activity have increased adiposity. Scand J Rheumatol. 2014;43(6):488–92.
Goncalves M, D’Almeida V, Guerra-Shinohara EM, Galdieri LC, Len CA, Hilario MO. Homocysteine and lipid profile in children with Juvenile Idiopathic Arthritis. Pediatr Rheumatol Online J. 2007;5:2.
Henderson CJ, Lovell DJ. Assessment of protein-energy malnutrition in children and adolescents with juvenile rheumatoid arthritis. Arthritis Care Research. 1989;2(4):108–13.
SilverioAmancio OM, Alves Chaud DM, Yanaguibashi G, Esteves Hilario MO. Copper and zinc intake and serum levels in patients with juvenile rheumatoid arthritis. Eur J Clin Nutr. 2003;57(5):706–12.
Mortensen AL, Allen JR, Allen RC. Nutritional assessment of children with juvenile chronic arthritis. J Paediatr Child health. 1990;26(6):335–8.
Dagdeviren-Cakir A, Arvas A, Barut K, Gur E, Kasapcopur O. Serum vitamin D levels during activation and remission periods of patients with juvenile idiopathic arthritis and familial Mediterranean fever. Turk J Pediatr. 2016;58(2):125–31.
Comak E, Dogan CS, Uslu-Gokceoglu A, Akbas H, Ozdem S, Koyun M, et al. Association between vitamin D deficiency and disease activity in juvenile idiopathic arthritis. Turk J Pediatr. 2014;56(6):626–31.
Caetano MC, Sarni RO, Terreri MT, Ortiz TT, Pinheiro M, de Souza FI, et al. Excess of adiposity in female children and adolescents with juvenile idiopathic arthritis. Clin Rheumatol. 2012;31(6):967–71.
Berntson L, Agback P, Dicksved J. Changes in fecal microbiota and metabolomics in a child with juvenile idiopathic arthritis (JIA) responding to two treatment periods with exclusive enteral nutrition (EEN). Clin Rheumatol. 2016;35(6):1501–6.
Berntson L, Hedlund-Treutiger I, Alving K. Anti-inflammatory effect of exclusive enteral nutrition in patients with juvenile idiopathic arthritis. Clin Exp Rheumatol. 2016;34(5):941–5.
Hvatum M, Kanerud L, Hallgren R, Brandtzaeg P. The gut– joint axis: cross reactive food antibodies in rheumatoid arthritis. Gut. 2006;55:1240–7.
Craig SM, Yu F, Curtis JR, et al. Vitamin D status and its associations with disease activity and severity in African Americans with recent-onset rheumatoid arthritis. J Rheumatol. 2010;37:275–81.
Patel S, Farragher T, Berry J, Bunn D, Silman A, Symmons D. Association between serum vitamin D metabolite levels and disease activity in patients with early inflammatory polyarthritis. Arthritis Rheum. 2007;56:2143–9.
Heidari B, Hajian-Tilaki K, Heidari P. The status of serum vitamin D in patients with rheumatoid arthritis and undifferentiated inflammatory arthritis compared with controls. Rheumatol Int. 2012;32:991–5.
Rossini M, MaddaliBongi S, La Montagna G, et al. Vitamin D deficiency in rheumatoid arthritis: prevalence, determinants and associations with disease activity and disability. Arthritis Res Ther. 2010;12:R216.
Braun-Moscovici Y, Toledano K, Markovits D, Rozin A, Nahir AM, Balbir-Gurman A. Vitamin D level: is it related to disease activity in inflammatory joint disease? Rheumatol Int. 2011;31:493–9.
Knops N, Wulffraat N, Lodder S, Houwen R, de Meer K. Resting energy expenditure and nutritional status in children with juvenile rheumatoid arthritis. J Rheumatol. 1999;26:2039–43.
Summers GD, Metsios GS, Stavropoulos-Kalinoglou A, Kitas GD. Rheumatoid cachexia and cardiovascular disease. Nat Rev Rheumatol. 2010;6:445–51.
Acknowledgment
We would like to acknowledge the collaboration of the Nuffield Orthopaedic Centre, Oxford, United Kingdom and Birmingham woman’s children’s foundation trust for contributions to this project.
Funding
There is no financial support for this review.
Author information
Authors and Affiliations
Contributions
NZ, HD, MM, SC and KB designed the study.NZ conducted the literature search, screened articles, performed data extraction, quality assessment, writing and drafting the manuscript. HD and NZ interpreted the data. AN independently screened the titles and abstract. SC independently assessed the quality of all included studies. All authors critically reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Ethics approval and consent to participate
Not applicable for this systematic review and meta-analysis.
Consent for publication is not applicable for this systematic review and meta-analysis.
Competing interests
The review authors have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 3:
Table 1. Characteristics of the selected studies (trials, exploratory, case and pilot studies).
Additional file 4: Table 2.
Characteristics of the selected studies (case-control, cross-sectional, cross-sectional with control and cross-sectional cohort).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zare, N., Mansoubi, M., Coe, S. et al. An investigation into the relationship between nutritional status, dietary intake, symptoms and health-related quality of life in children and young people with juvenile idiopathic arthritis: a systematic review and meta-analysis. BMC Pediatr 23, 3 (2023). https://doi.org/10.1186/s12887-022-03810-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03810-4