
Abstract
Background
Malnutrition is the most common cause of mortality and morbidity of children in low and middle income countries including Ethiopia and household wealth index shares the highest contribution. Thus, in this study it is aimed to conduct bivariate binary logistic regression analysis by accounting the possible dependency of child composite index anthropometric failure and household wealth index.
Methods
In this study the data from Ethiopian Demographic and Health Survey (EDHS) 2016 involved 9411 under five children was considered. Child Composite Index Anthropometric Failure (CIAF) measures the aggregate child undernourished derived from the conventional anthropometric indices (stunting, underweight and wasting). The correlation between CIAF and wealth index was checked and significant correlation found. To address the dependency between the two outcome variables bivariate binary logistic regression was used to analyze the determinants of child CAIF and household wealth index jointly.
Results
Study results show that region, place of residence, religion, education level of women and husband/partner, sex of child, source of drinking water, household size and number of under five children in the household, mothers body mass index, multiple birth and anemia level of child had significant association with child CIAF. Female children were 0.82 times less likely to be CIAF compared to male and multiple birth children were more likely to be CIAF compared to single birth. Children from Oromia, Somalie, Gambela, SNNPR, Harari and Addis Ababa region were 0.6, 0.56, 0.67, 0.52, 0.6 and 0.44 times less likely to be CIAF compared to Tigray. A household from rural area were 15.49 times more likely poor compared to a household. The estimated odds of children whose mothers attended primary, and secondary and higher education was 0.82, and 0.52 times respectively the estimated odds of children from mothers who had never attended formal education.
Conclusion
The prevalence of children with composite index anthropometric failure was high and closely tied with the household wealth index. Among the determinants, region, religion, family education level, and anemia level of child were statistically significant determinants of both CIAF and household wealth index. Thus, the authors recommend to concerned bodies and policymakers work on household wealth index to reduce the prevalence of child composite anthropometric failure.
Similar content being viewed by others

Background
Malnutrition is a relative or absolute deficiency or excess of one or more essential nutrients, and it is still a crucial problem, in particular, of children aged under five in the world [1]. It is the most common cause of mortality and morbidity, and responsible for more than half of death in children in low and middle income countries such as Ethiopia [2, 3]. Child malnutrition is the major public health problems in the world, with estimate of 45% of all death among under five children [4]. In Africa, the prevalence of chronic malnutrition is about 39% among under five children, and in Ethiopia it is worse higher than other African countries [4], revealed that more than one third of child death is associated with malnutrition [5]. Because, children are most vulnerable to malnutrition due to low dietary intakes, inequitable distribution of food within the household, improper food storage and preparation [6].
Malnutrition is devastating problems, particularly low-economic countries like Ethiopia as half of the Ethiopian population is living below the food poverty line and there is difficulty to meet their daily minimum nutritional requirement [6]. The anthropometric indicators involve wasting (weight-for-height), stunting (height-for-age), and underweight (weight-for-age) are among those commonly used to measure malnutrition in a population of childhood [4, 7]. Children whose measurements fall below 2 standard deviations from the reference median are generally considered malnourished and each indicator captures different aspects of malnutrition [7]. Based on these three indices the total malnourished of children can be detected using composite index of anthropometric failure (CIAF) [8]. In this study the composite index of stunting, wasting and underweight as composite index of anthropometric failure (CIAF) was employed for better description of malnutrition [8, 9]. Despite some improvements and remarkable efforts done to reduce child malnutrition rates, nearly half of under five children in Ethiopia are still malnourished [7].
Several socio-economic, demographic, and biological factors contribute to malnutrition. Of these, household wealth index shares the highest contribution and a key determinant of malnutrition which influence dietary intake and health cares of children and mothers. Household wealth index is an indicator of access to adequate food supplies, use of health services, availability of improved water sources, and sanitation facilities [6]. Several studies in Ethiopia [5,6,7] showed that higher household wealth index leads to lower levels of child malnutrition and it is indicated that low-income areas need consideration for prioritization and design of interventions to prevent and reduce malnutrition [10]. As researchers’ knowledge concerned, several studies of malnutrition [4, 5, 11], the anthropometric indicator wasting, stunting, and underweight were analyzed separately as malnutrition. However, in this study all the three anthropometric indicators incorporated and valued as Composite Index Anthropometric Failure (CIAF) for better description of malnutrition over other studies. Besides to this, the risk factors of child malnutrition and household wealth index studies conducted using univariate binary analysis, and a little attention is given for bivariate binary analysis in order to assess the association between child malnutrition and household wealth index with effects of socio-economic, demographic and biological factors. Thus, in this study it is aimed to conduct bivariate binary logistic regression analysis on the association between child CIAF and household wealth index relying on other socio-economic, demographic, and biological characteristics of children and households.
Methods
Data Source
The data for this analysis was obtained from 2016 Ethiopia Demographic and Health Survey (EDHS). The 2016 EDHS sample was stratified in to urban and rural areas and selected in two stages. In the first and second stages, a total of 645 enumeration areas (EAs) and 28 households per EA were selected with probability proportional to EA size and using systematic sampling, respectively. Based on the household and womens’ questionnaire, the children’s data including its height and weight measures was analyzed from 9411 children aged below 59 months [12].
The household and women’s survey questionnaire are two questionnaires among the five (the Household Questionnaire, the Woman’s Questionnaire, the Men’s Questionnaire, the Biomarker Questionnaire, and the Health Facility Questionnaire) that developed by Ethiopian Central Statistical Agency to reflect the population and health issues relevant to Ethiopia [12].
Variables
Dependent Variables
The outcome variables for this study were child composite index anthropometric failure (CIAF) and household wealth index. The first outcome variable, child CIAF measures the aggregate child undernourished derived from the conventional anthropometric indices (stunting, underweight and wasting) that classifies into seven groups (no failure; stunted only; underweight only; wasted only; stunted and underweight; wasted and underweight; wasted, stunted, and underweight) [8, 13]. Stunting, underweight and wasting are defined using Z-score as Z \(i=\frac{AI_i-\mu }{\sigma }\), where, AIi is the individual (child) anthropometric indicator, and refer respectively to median and standard deviation of the reference [14]. The CIAF is a better index for assessing the overall prevalence of undernourished and for identifying children with multiple anthropometric failures in a population [9, 13, 14]. For this study a single child CIAF was computed and re-coded into binary outcome as:” 1 = yes” if a child is either stunted only; underweight only; wasted only; stunted and underweight; wasted and underweight; or wasted, stunted and underweight; and” 0 = no” if a child is neither of them (no failure) [7].
The second outcome variable, household wealth index was computed according to national level wealth index/quantiles by Ethiopian Statistical Agency from poorest to richest utilizing family unit resource data by means of a principal components’ analysis [12, 15], where the twenty, forty, sixty, eighty and hundred percentiles are assigned to poorest, poorer, medium, rich, and richest. For the purpose of this study, household wealth index was categorized as poor = 1 and rich = 0 by merging poorest and poor as poor, and middle, rich and richest as rich.
Explanatory Variables
The selection of explanatory variables are theoretically driven that draw support from prior research with regard to factors affecting children’s nutritional status and household wealth index. Previous studies are referenced in creating categories for naturally continuous and discrete variables [16].
Statistical Analysis
Ordinary Binary Logistic Regression Model
Ordinary binary logistic regression model is considered only single response variable with binary outcome given other covariates. Let Yi = (Yi1,Yi2) be a vector of binary responses indicating whether the ith child is CIAF (Yi1 = 1) and a household is poor (Yi2 = 1) while Xi is the vector of covariates for the ith child. Then the ordinary binary logistic regression model is given by:
and the probability that the ith child will be malnourished (Yi1 = 1) or poor household (Yi2 = 1) is [17]:
The X’s are p-explanatory variables that may affect the outcomes and β’s are the coefficients of X’s that estimated from the data. The coefficients β’s allows researchers to rank the relative significance of explanatory variables and to understand their impact [15].
Bivariate Binary logistic Regression Model
We can perform separate analysis for the two outcomes CIAF and household wealth index (HHWI) by fitting ordinary binary logistic regression. This, however, would ignore the dependency between the two outcomes. To address this problem and take into account the dependency between two outcomes bivariate logistic regression model was used. Bivariate binary logistic regression analysis is a statistical method used to modeling two binary dependent variables jointly as a function of covariates [18]. In this study, the two outcomes of interests are child CIAF (yes = 1, no = 0) and household wealth index (poor = 1, rich = 0). In case of bivariate binary logistic regression analysis two binary outcomes (Y1, Y2) has four possible joint probabilities as:

Therefore, the joint probabilities expressed as a function of explanatory variables (xi) is given by [18]:
Alternatively, these can be articulated as logit function as:
In the Eq. (3, 4, 5) β11 and β10 refers to the parameters of the conditional logit model for Y2 = 1 and Y2 = 0, respectively in a function of predictors, X. These parameters used to express the nature of dependency between the outcome variables Y1 and Y2 in the presence of explanatory variables. A regression model for the odds ratio (OR) [18], which describes the dependence of child CIAF and household wealth index is fitted as:
The dependence between Y1 and Y2, can measure in terms of odds ratio and any departure from odds ratio = 1 will indicate the extent of dependence. The null hypothesis H0: β11 = β10 can be tested for independence in the presence of covariates between the two binary outcome variables Y1 and Y2.
Parameter Estimation and Model Diagnosis
All the logistic models of the parameters are estimated by the maximum likelihood techniques using Newton-Raphson algorithm iterative procedure and individual parameter estimates are tested based on the H0: β1j = 0 versus H1: β1j 6 = 0 using the Wald statistic \(W=\frac{{\hat{\beta}}_{1 ji}}{\hat{s}e\left({\hat{\beta}}_{1 ji}\right)}\) [17]. The goodness-of-fit test of the model was checked using correct classification rate (CCR). CCR is the ratio of number of correct predictions to number of observations. When the number of correct predictions is high, the CCR is high which indicates that higher accuracy and hence, the estimated model is good fit of the data [17].
The data was coded and entered to Statistical package for social science (SPSS) version 26 for Windows. The SPSS version 26 and R version 4.0.0 with VGLM package were used for the data analysis [19].
Results
Exploratory Analysis
In this study, a total of 9411 under five children were involved. The exploratory analysis was presented in four tables. Tables 1 and 2 revealed the description and frequency of dependent and independent variables, respectively. Nearly half of the children involved in this study had CIAF (46.7%) and from poor household (46.4%) (Table 1).
Twenty percent of children was between aged 24–35 months, 51.2% of the children were males and 89.1% lived in rural areas. The majority of mothers (65.0%) were aged less than 20 and 44.7% of households were used unimproved drinking water. Mothers and their parents who didn’t attend education were 65.8 and 45.0% respectively. Nearly one fifth (20.2%), one tenth (11.9%), and one seventh (14.7%) of children had cough, diarrhea, and fever symptoms two months before the survey respectively and more than one third of children (37.3%) have anemia (Table 2).
Table 3 shows the association of covariates with CIAF and household wealth index using chi-square (χ2) test. The CIAF was statistically associated with age of child, sex of child, region, place of residence, birth order, number of under five children in the household, source of drinking water of the household, multiple birth, age mother at first birth, mothers body mass index, anemia complication, diarrhea and fever symptoms, and husbands and mothers education level as they have p-value less than 0.05.
The maximum prevalence of CIAF for children under 5 years of age is observed within the age groups of 24 to 47 months. As mothers’ age at first birth increases the prevalence of child CIAF fairly decreases. Whereas the prevalence of child CIAF decreases as educational level of mothers and their parents increase. For instance, the prevalence of anthropometric failure for children under 5 years of age whose mothers had never attended formal education, attended primary, and secondary and above education were 70.8, 25.5, and 8.7% respectively. Nearly half of child CIAF (47.8%) was from households who had two children under five years of age. Compared to child lived in urban area, child CIAF lived in rural area was higher (7.8% vs.92.2%). The prevalence of child CIAF and poor household was vary from region to region. For instance, the highest prevalence of CIAF (42.9%) and poor household (44.0%) was found in Oromia region whereas, the smallest prevalence of CIAF(0.2%) was found in Harari and Gambela region, and poor household(0.0%) was found in Addis Ababa. The prevalence of poor household was fairy decreases as the education level of mothers and their parents increases. That is, the prevalence of poor household with mothers who didn’t attend formal education, attended primary and secondary education and higher was 78.0, 21.0 and 1.0% respectively while the prevalence of poor household with parents had not education, attend primary school and secondary education and higher was 61.1, 35.4 and 3.5% respectively (Table 3).
Table 4 revealed the frequency distribution of each covariate over child CIAF conditioned on household wealth index. The proportion of child CIAF from poor household was equal with child CIAF from rich households at early age of child while child CIAF from poor household were higher compared to child CIAF from rich households and both were increased between age 6 and 35 months. Whereas, as the education level of mothers and their parents increase the child CIAF from poor household was decreased rapidly. The prevalence of male CIAF from poor household was higher compared to female CIAF from poor household (53.1% vs. 46.9%). Similarly, the proportion of child CIAF from poor household who used unimproved drinking water was higher compared to poor household who used improved drinking water (62.2% vs. 37.8%).
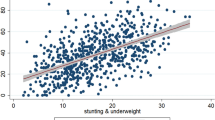
Table 5 shows the joint and marginal probabilities of child CIAF and household wealth index (HHWI) as well as the odds ratio. The odds ratio (OR) is a natural measure used to describe the association between the two binary responses and a value of unity denotes statistical independence [19, 20]. The OR is differed from unity (1.649). Thus, to fit the joint probability of child CIAF and household wealth index as a set of covariates while accounting for the possible dependency between the two responses using bivariate binary logistic regression model is very natural. Therefore, the bivariate logistic regression analysis of CIAF and household wealth index with other covariates was presented in Table 6.
Parameter Estimates
Table 6 revealed that the effect of covariates on child CAIF and household wealth index by taking into account the dependency of child CIAF and household wealth index using bivariate binary logistic regression model. The dependency between child CIAF and household wealth index was measured using odds ratio (OR) equals 1.498 and a value differ from one indicates significant dependency between child CIAF and household wealth index. After the dependency between child CIAF and household wealth index checked the effect of each covariate on CAIF and household wealth index was identified. Among covariates region, religion, education level of women and husband, sex of child, number of under five children, mothers body mass index, multiple birth, birth order, and anemia level of children were found as significantly associated factors for child CIAF. Whereas, region, place of residence, religion, education level of women and husband, household size, source of drinking water, anemia level of children e and number of under five children had significant association with household wealth index.
Table 7 revealed the predicted and observed counts for a combination of CIAF and household wealth index based on the estimated bivariate binary logistic regression model. The ratio of the number of correct predictions to number of observation, i.e. the correct classification rate (CCR) equals to 80.0% which is very high. This indicates that the estimated model was a good fit of the data.
Discussion
In this study, attempt was made to demonstrate the effects of children and households’ characteristics on children composite index anthropometric failure (CIAF) by considering its dependency with household wealth index (HHWI). A single CIAF was computed from the three classical anthropometric indices and recoded into binary outcome as they have a multidimensional nature [14]. Bivariate binary logistic regression model was employed to determine the effects of covariates on CIAF and HHWI. Based on this model and exploratory data analysis, significant dependency between CIAF and HHWI was noticed. This study demonstrated that child CIAF has significant association with household wealth index given other children’s and households’ characteristics.
This study reveals that the prevalence of child CIAF in Ethiopia was high (46.7%) and which has been also discussed in previous studies [3, 5, 14, 21]. This study found that region in Ethiopia has significant effect on child CIAF and household wealth index. The risk of child CIAF in Tigray was higher than Oromia (OR = 0.60), Somalie (OR = 56), Gambela (OR = 0.67), SNNPR (OR = 0.52), Hararie (OR = 0.60) and Addis Ababa (OR = 0.44). This finding of the study was consistent with different domestic research [5, 22], that reported children who are living in Tigray region have a higher risk of child CIAF compared to children living in Oromia, Somalie, Gambela, SNNPR, Harari, and Addis Ababa. Place of residence has significantly associated with household wealth index. Studies done by Tekile et al., Talukder, and Silveira et al. [4, 5, 21] states that compared to children from middle class and rich households, the likelihood of switching status from malnourished to nourished nutritional status was lower for children from poor household. This indicates that children who were living in rural area is more likely to be CIAF than children living in urban area. This is because of limited infrastructure that enables to affect a family to access food, health-care facility, exchange desired commodities, and so on. This finding was also in line with studies done in Bangladesh and Ethiopia [4].
As education level of mothers and husbands/partners getting higher, the likelihood of child exposed to CIAF was lower. Children whose mothers and husband/partners had never attended education were more likely to exposed to CIAF compared to children whose mothers and husband/partners had primary, and secondary and higher education which was consistent with studies conducted in Ethiopia [5, 22]. These studies reported that children whose mothers had never attended education were significantly more likely to be stunted, underweight, and/or under nutrition as compared to children whose mothers had primary, and secondary and above education level. Moreover, religion of the household was also an important determinate that significantly associated with child CIAF.
The result showed that a child whose household religion orthodox was less likely to be CIAF and more likely to be rich compared to its counterpart. Whereas the reality in Ethiopia shows that the majority Muslim and protestant households were lived in urban area whereas the majority orthodox households are living in rural area where health care facilities, child feeding practice, access to improved water, and so on are less accessible and poverty is very high (OR for urban versus rural is 15.49). Mostly mothers in rural area are participated in farming activities and giving less attention to feed and care of their child. Beyond to this, orthodox mothers are commonly fasting during their prenatal and postnatal period. Therefore, the pre-specified and other issues may be responsible for child CIAF whose household beliefs orthodox than other religious in contrast of this study. In addition, the household who drank improved water were more likely to be rich compared to the household who drank unimproved water.
The existence of CIAF was significantly differ within sex of child and multiple of birth i.e., males were more likely to be CIAF compared to females and multiple birth children were more likely to be CIAF compared to single birth. This result is in line with studies done at Ethiopia and Favelas Brazil [5, 11]. On the other hand, compared to children who drank unimproved water, children who drank improved water were less likely to belonging in poor household and this led to less likely to be CIAF, which is supported by previous study findings [11, 14]. Like a study done in Ethiopia [5], number of under five children in the household was an important determinant effect on child CIAF. Children from a household having two under five children were 1.21 times more likely to be CIAF compared to a household having one under five children.
Unlike a study in Ethiopia and Brazil [5, 11], mothers age at first birth and child age were insignificantly associated with child CIAF in this study. This may because of the methodology difference, i.e., in this study a bivariate binary logistic regression accounting the dependency of a single CIAF and household wealth index was employed whereas the previous studies were used binary and ordinal univariate logistic regression.
Mothers’ body mass index was significantly associated with child CIAF which in line with a study done by Silveira et al. [21] and they stated that short height and poor weight of mothers were associated with child malnutrition. Moreover, this study found that anemic children were more exposed to CIAF compared to non-anemic children that in line with a study done in Ethiopia [22].
Conclusion
The prevalence of children with composite index anthropometric failure was high and closely tied with the household wealth index. Among covariates region, religion, residence, education level of women and husband, sex of child, number of under five children, household size, source of drinking water, mothers body mass index, multiple birth, birth order, and anemia level of children were found as significantly associated factors for child composite index anthropometric failure and household wealth index. This means that children from poor households are more likely to be underfed, get sick, least likely to access safe water and receive sufficient health-care facilities, and exposed to composite index anthropometric failure. Thus, the authors recommend to concerned bodies and policymakers work on household wealth index to reduce the prevalence of child composite anthropometric failure.
Availability of data and materials
The datasets for generated analyses during the study is available in Ethiopian Demographic and Health Survey data if unique request sent via their site EDHS 2016.
Abbreviations
- CIAF:
-
Composite index anthropometric index
- HHWI:
-
Household wealth index
- BMI:
-
Body mass index
- EDHS:
-
Ethiopian demographic and health survey
- OR:
-
Odds ratio
- CCR:
-
Correct classification rate
- SNNPR:
-
South Nations Nationalities and Peoples Representatives
References
WHO. World Health Organization. Global nutrition reports; 2018.
Mengistu K, Alemu K, Destaw B. Prevalence of malnutrition and associated factors among children aged 6-59 months at Hidabu Abote District, north Shewa, Oromia regional state. J nutr disorders ther. 2013;1:1–5.
Tsedeke W, Tefera B, Debebe M. Prevalence of acute malnutrition (wasting) and associated factors among preschool children aged 3660 months at Hawassa Zuria, South Ethiopia: a community based cross sectional study. J Nutr Food Sci. 2016;6(466):2.
Talukder A. Factors associated with malnutrition among under-five children: illustration using Bangladesh demographic and health survey, 2014 data. Children. 2017;4(10):88. https://doi.org/10.3390/children4100088.
Tekile AK, Woya AA, Basha GW. Prevalence of malnutrition and associated factors among under-five children in Ethiopia: evidence from the 2016 Ethiopia demographic and health survey. BMC Res Notes. 2019;12(1):391. https://doi.org/10.1186/s13104-019-4444-4.
Girma W, Genebo T. Determinants of nutritional status of women and children in Ethiopia; 2002
Silva P. Environmental factors and childrens malnutrition in Ethiopia. Washington, DC: The World Bank; 2005.
Svedberg P. Poverty and undernutrition: theory, measurement, and policy. Oxford: Clarendon Press; 2000.
Bose K. The concept of composite index of anthropometric failure (CIAF): Revisited and Revised; 2018
Dominguez-Salas P, Alarcón P, Häsler B, Dohoo IR, Colverson K, Kimani-Murage EW, et al. Nutritional characterisation of low-income households of Nairobi: socioeconomic, livestock and gender considerations and predictors of malnutrition from a cross-sectional survey. BMC Nutrition. 2016;2(1):47. https://doi.org/10.1186/s40795-016-0086-2.
Zeray A, Kibret GD, Leshargie CT. Prevalence and associated factors of undernutrition among under-five children from model and non-model households in east Gojjam zone, Northwest Ethiopia: a comparative cross-sectional study. BMC Nutrition. 2019 Dec 1;5(1):27.
EDHS. Ethiopian Demographic and health survey report; 2016.
Nandy S, Irving M, Gordon D, Subramanian SV, Smith GD. Poverty, child undernutrition and morbidity: new evidence from India. Bull World Health Organ. 2005;83:210–6.
Kassie GW, Workie DL. Exploring the association of anthropometric indicators for underfive children in Ethiopia. BMC Public Health. 2019;19(1):1–6.
Lakew D, Tesfaye D, Mekonnen H. Determinants of stillbirth among women deliveries at Amhara region, Ethiopia. BMC Pregnancy and Childbirth. 2017;17(1):375.
Lakew D, Tesfaye D, Mekonnen H. Determinants of stillbirth among women deliveries at Amhara region, Ethiopia. BMC Pregnancy and Childbirth. 2017;17(1):375. https://doi.org/10.1186/s12884-017-1573-4.
Agresti A. An introduction to categorical data analysis. Hoboken: John Wiley and Sons; 2016.
Islam MA, Chowdhury RI, Briollais L. A bivariate binary model for testing dependence in outcomes. Bull Malays Math Sci Soc (2). 2012;35(4):845–58.
Yee T. VGAM: vector generalized linear and additive models; 2017.
Montgomery DC, Runger GC. Applied statistics and probability for engineers. Hoboken: John Wiley and Sons; 2010.
Silveira KB, Alves JF, Ferreira HS, Sawaya AL, Florncio TM. Association between malnutrition in children living in favelas, maternal nutritional status, and environmental factors. J Pediatr. 2010;86(3):215–20. https://doi.org/10.1590/S0021-75572010000300009.
Kassie GW, Workie DL. Determinants of under-nutrition among children under five years of age in Ethiopia. BMC Public Health. 2020;20:1–1.
Acknowledgments
The authors are thank full to Ethiopian Demographic and Health survey for data availability.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
DLW had the idea of the study. DLW and LMT proposed the first draft, conducted data analysis, interpretation and wrote the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethical clearance for 2016 EDHS was approved by Ethical Review Board of Ethiopia Central Statistical Agency (ECSA) and all participants who agreed to take part in the survey signed a consent form. Hence, author asked the permission to use data via online form and the data manager has given permission to use the data for this study.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Workie, D.L., Tesfaw, L.M. Bivariate binary analysis on composite index of anthropometric failure of under-five children and household wealth-index. BMC Pediatr 21, 332 (2021). https://doi.org/10.1186/s12887-021-02770-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-021-02770-5