
Abstract
Background
Previous studies have suggested that choline and betaine are associated with improved anthropometric measures including, BMI and waist circumference however, results are largely inconsistent and limited studies exist in children. Our objective was to investigate the relationship between dietary choline and betaine, and anthropometric measurements among Iranian children.
Methods
In this cross-sectional study, dietary information was collected for 788 six-year-old children, who attended Tehran health centers in 2018. We measured dietary intakes using a valid and reliable semi-quantitative food frequency questionnaire. The USDA database was used to calculate dietary choline and betaine. We assessed anthropometric characteristics, physical activity, and socio-demographic status based on a reliable and valid protocol. Logistic regression adjusted for energy, physical activity, socio-economic status, and maternal age, physical activity, BMI, and HEI2015 was used to assess this association.
Results
Free choline, glycero-phospho-choline, phospho-choline, phosphatidyl-choline, total choline, and total betaine, and choline were not related to overweight, obesity, underweight and wasting in the crude and adjusted model after controlling for children’s energy intake, children’s physical activity, socio-economic status, maternal physical activity, and BMI. Betaine intake was associated with mid-arm circumference and risk of overweight.
Conclusions
We did not find any evidence to support the association between dietary choline with anthropometric measurements among Iranian children. Further prospective studies with a large sample size in different populations are needed.
Similar content being viewed by others


Background
Epidemiological studies suggest that well-nourished children have healthier growth and development patterns, which may lead to a lower risk of chronic disease later in life [1]. Still, childhood overweight and obesity have become significant public health issues [2]. The number of overweight or obese infants and young children (aged 0 to 5 years) increased from 32 million globally in 1990 to 41 million in 2016 [3]. In Iran, reports have shown that childhood obesity has risen from 5% to 15% between 2000 to 2018 [4]. Furthermore, based on a national study, six-year-old girls are at double the risk of being categorized as overweight compared to boys in Iran [5]. Childhood overweight is associated with an increased risk for obesity, insulin resistance, diabetes, dyslipidemia, fatty liver disease, and cardiovascular diseases in adulthood [6]. According to previous studies, various factors impact childhood obesity, such as diet [7, 8], physical activity, and socio-economic status (SES) [9, 10]. Notably, a double burden exists which suggests children who experience underweight or wasting are similarly at a higher risk for developing non-communicable diseases later in life, or suffering from undernutrition or nutrition deficiency, which can also lead to the development of infectious disease [11]. On a global scale, approximately 16% of children are considered underweight, and 9% are considered wasted [12]. In Iran, poor nutrition status impacted approximately 15.5% of children in 2017, with higher rates observed among girls [13, 14]. Interestingly, a meta-analysis showed a distinct parent-child resemblance in anthropometric measurements [15] and a different umbrella review reported that family-based interventions were helpful for obesity and weight management [16]. Together, this suggests that maternal influence and characteristics are important considerations for weight management programs and research.
Several studies have explored the association between individual foods, nutrients [17,18,19], and dietary patterns [20,21,22,23] and anthropometric measurements in children. However, there is limited evidence regarding the association between other dietary components such as choline and betaine, as methyl donor compounds, and anthropometric measurements. Choline and betaine are quaternary ammonium compounds synthesized from diet or de novo synthesis in tissues [24, 25]. Choline is the primary source of methyl groups in the diet, and is found in dietary sources including eggs, beef, liver, seafood, and milk [25]. Various esterified forms of choline exist with different metabolic impacts, bioavailability, and dietary sources, including phospho-choline, glycero-phospho-choline, and phosphatidyl-choline [26]. For example, phosphatidyl-choline has a role in gene expression, glucose homeostasis, and membrane structure, phospho-choline is the main form of choline in human breast milk and modulates immune function, and glycero-phospho-choline maintains osmotic regulation [27,28,29]. Betaine is abundant in marine invertebrates, wheat germ, spinach, and sugar beets [24]. Betaine supplementation has been shown to increase muscle mass, decrease body fat percentage and fat mass [30, 31]. Previous work in adults has shown that supplementation of dietary choline and betaine led to decreased visceral fat accumulation, waist circumference, and body weight which suggests they may contribute to the development of chronic disease [32, 33]. However, limited studies exist in children investigating their role, and findings in adults remain inconsistent [32, 34,35,36]. Children get ready to enter the school environment at six years of age and experience more independence to self-select and manage their own food menu choices [37]. Various esterified forms of choline have different metabolic impacts, bioavailability, and dietary sources, and no other study has investigated their role. Taken together with the higher rates of underweight and wasting observed in girls, it is critical to delineate the role that diet plays in the development of chronic disease in this age category. Therefore, we aimed to investigate the association between dietary choline forms and betaine and anthromopometric measures among Irainian six-year-old girls.
Methods and materials
Study population
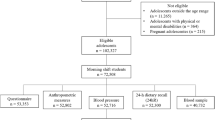
This cross-sectional study was performed on 788 children who attended Tehran health centers with their mothers for preschool vaccination from October 2017 to March 2018. Obesity and overweight prevalence was used to calculate sample size [5], on P1 = 0.22, P2 = 0.32, β = 0.2, α = 0.05 with the following formula: \( n=\frac{{\left[\left({z}_{1-\frac{\alpha }{2}}\right)+\left({z}_{1-\beta}\right)\right]}^2\times \left({p}_1\left(1-{p}_1\right)+{p}_2\left(1-{p}_2\right)\right)}{{\left({p}_2-{p}_1\right)}^2} \). We interviewed 788 six-year-old girls to account for missing data. Participants were selected using a cluster random sampling method from 10 health and treatment centers. Parents provided written and informed consent for their child’s participation. Inclusion criteria information was collected from parents and included six-year-old girls without any history of acute or chronic disease, or specific diet. Participants were excluded in the final analysis stage if their estimated energy intake (calculated using NUTRITIONIST 4; version 7.0; NSquared Computing, Salem, OR) was not between 235 and 1735 kcal/d [38] (n = 0).
Dietary intake assessment and choline calculation
Participants dietary intake was assessed using a reliable semi-quantitative food frequency questionnaire (FFQ) with 168 food items over the past year; validated in children [39, 40]. Dietary intakes were recorded based on face-to-face interviews with participant mothers. The FFQ collected the number of daily (e.g. bread), weekly (e.g. rice), or monthly (e.g. fish) standard servings using household measures of common food items consumed in Iran in the previous 12 months by a trained nutritionist. Reported food intakes were converted into grams per day (g/d), and entered into the NUTRITIONIST 4 (version 7.0; NSquared Computing, Salem, OR) software, modified for Iranian food items, and total calorie (kcal/day) and nutrient intakes were computed for each food item. Choline, glycero-phospho-choline, phospho-choline, phosphatidyl-choline, and betaine were calculated by multiplying each food item based on the United States Department of Agriculture (USDA) food content databases [41,42,43,44,45]. Total choline intake was calculated as the sum of choline intake from free choline, glycero-phospho-choline, phospho-choline, and phosphatidyl-choline. The sum of total choline and betaine together was used to calculate total betaine and choline.
Anthropometric, socio-demographic, and physical activity measurement
Subjects were weighed (to the nearest 0.1 kg) with minimum coverage using an electronic scale (Seca 753E; Seca Weighing and Measuring Systems, Hamburg, Germany). Standing height was measured (to the nearest 0.1 cm) in a fixed position without shoes, and body mass index (BMI) was calculated (kg/m2). Mid-arm circumference was measured based on the length between the mid-point of the elbow and the shoulder (at 0.1 mm) precision. World Health Organization (WHO) diagnostic criteria was used to diagnose overweight or obesity in children: obese (BMI-for-age ≥ 2SD), overweight (BMI-for-age ≥ 1SD), normal (BMI-for-age ≥ −1SD and < 1SD), underweight (BMI-for-age < −1SD) and wasting (BMI-for-age < −2SD) [46]. Physical activity levels were recorded based on self-reported measures by the mothers of participants based on the average time of indoor and outdoor physical activity over a 24 h period, according to light, moderate, high, and very high intensity. These values were multiplied by their corresponding metabolic equivalent, stated as metabolic equivalent hours per week (MET h/wk) [47], and total physical activity was calculated using the International Physical Activity Questionnaire. We categorized participants socioeconomic status (SES) according to a validated Persian questionnaire, which included questions related to the information about the parent’s occupation and education, number of children under 18 years, number of family members, income level, health care insurance, food assistance, dwelling ownership, neighborhood, vehicle ownership, number of cars and number of rooms in the house [48]. A standardized SES score was calculated using factor analysis and a summary index, and compliance using a Kappa test. The correlation of these parameters with the standardized SES score was reported at 0.87.
Statistical analysis
A Kolmogorov-Smirnov test and histogram curve was used to test the normality of quantitative variables. A one-way analysis of variance (ANOVA) was used to compare quantitative variables across total dietary to choline, total betaine, and total choline and betaine tertiles based on population distribution. An analysis of covariance (ANCOVA) adjusted for daily energy intake using the residual method and Healthy Eating Index (HEI) was used to compare dietary intake of macro and micronutrients across tertiles of total choline, total betaine, and total choline and betaine [49]. Statistical interaction between dietary choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, total betaine, and total betaine and choline with participant height-for-age and mid-arm circumference was analyzed using linear regression. Multivariable binary logistic regressions were used to assess the association between participants’ anthropometric measurements and dietary choline, glycero-phospho-choline, phospho-choline, phosphatidyl-choline, total choline, total betaine, and total betaine and choline. Participant energy intake, physical activity, SES, maternal age, physical activity, BMI, and Healthy Eating Index 2015 score (HEI2015) were adjusted for. Partial correlation analysis controlling for energy and HEI was used to evaluate the correlation of dietary choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, total betaine, and total betaine and choline with participants characteristics. Statistical analyses were performed using SPSS software (version 26, SPSS Inc., Chicago, IL, USA). A P < 0.05 was considered statistically significant.
Ethical consideration
The National Institute for Medical Research Development of Tehran University of Medical Science, Tehran, Iran (IR. TUMS. VCR.REC.94–04–161-31,112) was granted ethical approval from the Ethics Commission of Tehran University of Medical Science. Verbal and written informed consent was obtained from parents for the participation of their children in the study.
Results
Demographic characteristics of the 788 participants and mothers are shown in Table 1. All participants remained in the study for the entire study duration. The mean age, BMI, physical activity, and energy intake of mothers was: 32 years, 24.88, 30 MET/h, and 2267 kcal. Participants mean intake of free choline (57 mg/day), glycerol-phospho-choline (54 mg/day), phospho-choline (12 mg/day), phosphatidyl choline (140 mg/day), total choline (263 mg/day), total betaine (71 mg/day), and total choline and betaine (334 mg/day) are reported in Table 1.
Table 2 represents general characteristics of participants across dietary total choline, betaine, and total choline and betaine tertiles. Accordingly, participants with a greater total betaine intake had lower energy intake (985 kcal, P = 0.013) and estimated SES (32, P = 0.035).
Energy and HEI2015 adjusted dietary intakes across tertiles of dietary choline and betaine intakes are shown in Table 3. Accordingly, participants with a higher intake of total choline and betaine had a greater intake of macronutrients and micronutrients (P < 0.05) however this significant association was not observed for vitamin E and total fiber.
Crude and multivariable odds ratio (OR) and 95% confidence intervals (CI) for overweight, obesity, underweight, and wasting across free choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, total betaine, and total betaine and choline tertiles are shown in Table 4. After adjusting for potential confounders, including participant energy intake, physical activity, SES, maternal age, physical activity, BMI, and HEI2015, there was no significant association between total choline, and risk of wasting (OR: 1.00; 95% CI 0.35–2.89), obesity (OR: 0.94; 95% CI 0.33–2.71), overweight/obesity (OR: 1.08; 95% CI 0.74–1.56), and underweight/wasting (OR: 1.04; 95% CI 0.63–1.73). Participants in the lowest tertiles of total betaine intake were not associated with a higher risk of wasting (OR: 1.00; 95% CI 0.32–3.14), obesity (OR: 1.30; 95% CI 0.42–4.09), and underweight/wasting (OR: 0.90; 95% CI 0.53–1.51). Similarly, a higher intake of total choline and betaine was not associated with risk of wasting (OR: 1.05; 95% CI 0.36–3.03), obesity (OR: 0.77; 95% CI 0.28–2.13), overweight/obesity (OR: 1.01; 95% CI 0.69–1.47), and underweight/wasting (OR: 1.13; 95% CI 0.68–1.87). Participants in the highest dietary betaine intake group had a significantly higher risk of overweight/obesity (OR: 1.49; 95% CI 1.02–2.18).
Multiple linear regression was used to assess the potential relationship between free choline, glycero-l phospho-choline, phospho-choline, phosphatidyl choline, total choline, total betaine, and total betaine and choline, and height-for-age, and mid-arm circumference, adjusted for participant energy intake, physical activity, SES (Model 1), and maternal age, BMI, physical activity, and HEI2015 (Model 2, Table 5). Total betaine intake was positively associated with mid-arm circumference (β = 0.087, P = 0.018). There was no significant relationship between free choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, and total choline and betaine.
Table 6 demonstrates the adjusted Pearson correlations between participants’ characteristics and dietary free choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, total betaine, and total choline and betaine intake among participants. There was a correlation between the mid-arm circumference (r = 0.093, P = 0.009) and age (r = − 0.072, P = 0.044) with total betaine intake. With the exception of vitamin E, the dietary intake of children was correlated with free choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, and total betaine and choline. There was no significant correlation observed between dietary free choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, and total choline and betaine intake, and maternal age, BMI, physical activity, participant physical activity, BMI-for-age, height-for-age, or mid-arm circumference.
Discussion
To our knowledge, no other studies exist that investigate the relationship between dietary choline and betaine and risk of overweight/obesity and underweight/wasting in a sample of children in Iran. Our findings demonstrate that free choline, glycero-phospho-choline, phospho-choline, phosphatidyl choline, total choline, total betaine, and total betaine and choline were not related to overweight/obesity and underweight/wasting in Iranian six-year-old girls. However, we did observe total betaine intake was associated with mid-arm circumference.
Previous work exploring the association between dietary choline and betaine and anthropometric measures in children is largely inconsistent, and the relationship remains unclear. For example, betaine supplementation did not affect body composition in 42 obese adults following a hypo-energetic diet [50] or 42 untrained men [51]. Additionally, no significant difference in fat mass or fat-free mass was observed following six weeks of betaine supplementation in 29 trained CrossFit© athletes [52]. This was further supported by Long et al. who demonstrated, no significant differences in body weight or waist circumference across tertiles of participant betaine intake [53]. However, Cholewa et al. reported that betaine supplementation was related to improved body composition [30, 34]. On a similar note, no significant differences in anthropometric measures including weight, BMI, body fat percentage, waist circumference, hip circumference, and waist-to-hip ratio were observed in 96 diabetic patients following a two-month choline supplementation trial [31]. In contrast, a previous study reported improved body composition metrics following dietary choline and betaine supplementation, including total body fat percentage, trunk fat percentage, android fat percentage, gynoid fat percentage, body weight, BMI, waist circumference, and waist-to-hip ratio in 3214 participants across different age and sex categories [32].
These findings suggest that dietary choline and betaine may impact anthropometric measurements. Yet, the lack of consistent findings may be a reflection of several factors. First, different methods such as dual-energy x-ray absorptiometry (DXA), Bioelectric impedance analysis (BIA), BodPod, underwater weighing, and skin-fold calipers were used to assess anthropometric measurements in the literature. Although each measure has its own validity and reliability in context, the comparability of these measures should be considered. Second, men and women have different sex hormones, metabolites, and growth patterns that confound anthropometric measures, which were not considered in all studies. Lastly, to date, most of the literature has been conducted on adults, however, children engage in different dietary habits that influence their choline and betaine dietary intakes. As it stands, more research is required to expand our current understanding of the higher prevalence of obesity/overweight in girls and how dietary intake affects body composition in children.
Although choline and betaine’s mechanisms are not fully understood, a couple of theories have been suggested. Choline’s beneficial effect might be due to its capacity to reduce carnitine, which ultimately plays a role in fat mobilization and oxidation [54]. Further, choline, as a precursor for acetylcholine, may induce glucose uptake and lipolysis by activating m3 receptors in the brain [55]. However, due to the relationship between choline and other one-carbon metabolism components, the relationship is complex and still needs to be explored. Only one potential mechanism has been suggested for the relationship between betaine dietary intake and anthropometric measurements. It has been suggested that betaine can decrease acetyl-CoA carboxylase and lipoprotein lipase [34] and increase hormone-sensitive lipase and growth hormone [56].
Our study was the first to examine the association between different forms of dietary choline and betaine with anthropometric measurements among children. The cross-sectional design is the main limitation of the present study, as we are unable to determine causation. Although we controlled for multiple potential confounders, including SES and physical activity, our findings may be influenced by unknown residual confounders. Further, while FFQ is the best dietary assessment tool for large populations, recall bias could have influenced our results, and our study relied on self-reported measures by participant’s mothers. Finally, as our study sample was homogenous, we were unable to stratify our analysis based on sex or age.
Conclusions
In conclusion, our cross-sectional study did not demonstrate an association between various forms of dietary choline intake and anthropometric measurements among six-year-old girls in Iran, but total betaine intake was associated with mid-arm circumference. Future prospective studies with a larger sample size in different populations are needed to delineate this relationship more clearly and explore potential mechanisms.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ANCOVA:
-
Analysis of covariance
- ANOVA:
-
Analysis of variance
- BIA:
-
Bioelectric impedance analysis
- BMI:
-
Body mass index
- CVD:
-
Cardiovascular disease
- DXA:
-
Dual-energy x-ray absorptiometry
- FFQ:
-
Food frequency questionnaire
- HC:
-
Hip circumference
- PA:
-
Physical activity
- SES:
-
Socio-economic status
- SFA:
-
Saturated fatty acid
- WHO:
-
World Health Organization
- WC:
-
Waist circumference
- WHR:
-
Waist to hip ratio
References
Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B. Developmental potential in the first 5 years for children in developing countries. Lancet (London, England). 2007;369(9555):60–70. https://doi.org/10.1016/s0140-6736(07)60032-4.
Gies I, AlSaleem B, Olang B, Karima B, Samy G, Husain K, et al. Early childhood obesity: a survey of knowledge and practices of physicians from the Middle East and North Africa. BMC Pediatr. 2017;17(1):115. https://doi.org/10.1186/s12887-017-0865-1.
Organization WH. Childhood overweight and obesity. World Health Organization. 2020. Available from: https://www.who.int/dietphysicalactivity/childhood/en/. Accessed 19 Oct 2020.
Agha-Alinejad H, Farzad B, Salari M, Kamjoo S, Harbaugh BL, Peeri M. Prevalence of overweight and obesity among Iranian preschoolers: interrelationship with physical fitness. J Res Med Sci. 2015;20(4):334–41.
Pouraram H, Djazayery A, Mohammad K, Parsaeian M, Abdollahi Z, Dorosty Motlagh A, et al. Second National Integrated Micronutrient Survey in Iran: study design and preliminary findings. Arch Iran Med. 2018;21(4):137–44.
Hajian-Tilaki K, Heidari B. Childhood obesity, overweight, socio-demographic and life style determinants among preschool children in Babol, northern Iran. Iran J Public Health. 2013;42(11):1283–91.
Ahadi Z, Qorbani M, Kelishadi R, Ardalan G, Motlagh ME, Asayesh H, et al. Association between breakfast intake with anthropometric measurements, blood pressure and food consumption behaviors among Iranian children and adolescents: the CASPIAN-IV study. Public Health. 2015;129(6):740–7. https://doi.org/10.1016/j.puhe.2015.03.019.
Payab M, Kelishadi R, Qorbani M, Motlagh ME, Ranjbar SH, Ardalan G, et al. Association of junk food consumption with high blood pressure and obesity in Iranian children and adolescents: the CASPIAN-IV Study. Jornal de pediatria. 2015;91(2):196–205. https://doi.org/10.1016/j.jped.2014.07.006.
Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. 2011;35(7):891–8. https://doi.org/10.1038/ijo.2010.222.
Zhang LL, Huang MY, Yang Y, Huang MQ, Shi JJ, Zou L, et al. Bioactive platycodins from Platycodonis Radix: Phytochemistry, pharmacological activities, toxicology and pharmacokinetics. Food Chem. 2020;327. https://doi.org/10.1016/j.foodchem.2020.127029.
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet (London, England). 2013;382(9890):427–51. https://doi.org/10.1016/s0140-6736(13)60937-x.
Organization WH. Malnutrition. World Health Organization. 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/malnutrition. Accessed 1 Apr 2020.
Mohammadi M, Vaisi Raiegan AA, Mirzaei M, Zahednezhad H, Jalali R, Abbasi P. Prevalence of underweight in Iranian children: a systematic review and meta-analysis. Tehran Univ Med J TUMS Publications. 2018;76(4):241–9.
Nouri Saeidlou S, Babaei F, Ayremlou P. Children malnutrition in northwestern, central and southern regions of Iran: does geographic location matter? Glob J Health Sci. 2014;6(4):36–41. https://doi.org/10.5539/gjhs.v6n4p36.
Wang Y, Min J, Khuri J, Li M. A Systematic Examination of the Association between Parental and Child Obesity across Countries. Adv Nutr. 2017;8(3):436–48. https://doi.org/10.3945/an.116.013235
Chai LK, Collins C, May C, Brain K, Wong See D, Burrows T. Effectiveness of family-based weight management interventions for children with overweight and obesity: an umbrella review. JBI Database System Rev Implement Rep. 2019;17(7):1341–427. https://doi.org/10.11124/jbisrir-2017-003695.
Chong KH, Lee ST, Ng SA, Khouw I, Poh BK. Fruit and Vegetable Intake Patterns and Their Associations with Sociodemographic Characteristics, Anthropometric Status and Nutrient Intake Profiles among Malaysian Children Aged 1–6 Years. Nutrients. 2017;9(8). https://doi.org/10.3390/nu9080723.
Moschonis G, van den Heuvel EG, Mavrogianni C, Singh-Povel CM, Leotsinidis M, Manios Y. Associations of Milk Consumption and Vitamin B2 and Β(12) Derived from Milk with Fitness, Anthropometric and Biochemical Indices in Children. The Healthy Growth Study. Nutrients. 2016;8(10). https://doi.org/10.3390/nu8100634.
Rienks J, Penczynski KJ, Schmitting S, Buyken AE, Nöthlings U. Dietary flavonoids among children and adolescents in the Dortmund Nutritional and Anthropometric Longitudinally Designed (DONALD) study: intake, food sources and trends from 1985 until 2016. Br J Nutr. 2020:1–9. https://doi.org/10.1017/s000711452000183x.
Delgado Floody PA, Caamaño Navarrete F, Jerez Mayorga D, Cofré-Lizama A, Guzmán-Guzmán IP. The association between children's food habits, anthropometric parameters and health-related quality of life in Chilean school-age children. Nutricion Hospitalaria. 2019;36(5):1061–6. https://doi.org/10.20960/nh.02643.
Liu D, Zhao LY, Yu DM, Ju LH, Zhang J, Wang JZ, et al. Dietary Patterns and Association with Obesity of Children Aged 6−17 Years in Medium and Small Cities in China: Findings from the CNHS 2010−2012. Nutrients. 2018;11(1). https://doi.org/10.3390/nu11010003.
Mehranfar S, Jalilpiran Y, Surkan PJ, Azadbakht L. Association between protein-rich dietary patterns and anthropometric measurements among children aged 6 years. Nutr Dietetic 2020;77(3):359-67.https://doi.org/10.1111/1747-0080.12609, 367.
Vinciguerra F, Tumminia A, Roppolo F, Romeo LC, La Spina N, Baratta R, et al. Impact of unhealthy childhood and unfavorable parents' characteristics on adiposity in schoolchildren. Diabetes Metabol Res Rev. 2019;35(8):e3199. https://doi.org/10.1002/dmrr.3199.
Craig SA. Betaine in human nutrition. Am J Clin Nutr. 2004;80(3):539–49. https://doi.org/10.1093/ajcn/80.3.539.
Zeisel SH, Blusztajn JK. Choline and human nutrition. Ann Rev Nutr. 1994;14:269–96. https://doi.org/10.1146/annurev.nu.14.070194.001413.
Zeisel SH. Choline: critical role during fetal development and dietary requirements in adults. Ann Rev Nutr. 2006;26:229–50. https://doi.org/10.1146/annurev.nutr.26.061505.111156.
Gallazzini M, Burg MB. What's new about osmotic regulation of glycerophosphocholine. Physiology (Bethesda). 2009;24:245–9. https://doi.org/10.1152/physiol.00009.2009.
Parchim NF, Wang W, Iriyama T, Ashimi OA, Siddiqui AH, Blackwell S, et al. Neurokinin 3 receptor and phosphocholine transferase: missing factors for pathogenesis of C-reactive protein in preeclampsia. Hypertension. 2015;65(2):430–9. https://doi.org/10.1161/hypertensionaha.114.04439.
Ridgway ND. The role of phosphatidylcholine and choline metabolites to cell proliferation and survival. Crit Rev Biochem Mol Biol. 2013;48(1):20–38. https://doi.org/10.3109/10409238.2012.735643.
Cholewa JM, Hudson A, Cicholski T, Cervenka A, Barreno K, Broom K, et al. The effects of chronic betaine supplementation on body composition and performance in collegiate females: a double-blind, randomized, placebo controlled trial. J Int Soc Sport Nutr. 2018;15(1):37. https://doi.org/10.1186/s12970-018-0243-x.
Rashvand S, Mobasseri M, Tarighat-Esfanjani A. The Effects of Choline and Magnesium Co-Supplementation on Metabolic Parameters, Inflammation, and Endothelial Dysfunction in Patients With Type 2 Diabetes Mellitus: A Randomized, Double-Blind, Placebo-Controlled Trial. J Am Col Nutr. 2019;38(8):714–21. https://doi.org/10.1080/07315724.2019.1599745.
Gao X, Wang Y, Randell E, Pedram P, Yi Y, Gulliver W, et al. Higher Dietary Choline and Betaine Intakes Are Associated with Better Body Composition in the Adult Population of Newfoundland, Canada. PloS one. 2016;11(5):e0155403. https://doi.org/10.1371/journal.pone.0155403.
Ueland PM. Choline and betaine in health and disease. J Inherited Metabol Dis. 2011;34(1):3–15. https://doi.org/10.1007/s10545-010-9088-4.
Cholewa JM, Wyszczelska-Rokiel M, Glowacki R, Jakubowski H, Matthews T, Wood R, et al. Effects of betaine on body composition, performance, and homocysteine thiolactone. J Int Soc Sport Nutr. 2013;10(1):39. https://doi.org/10.1186/1550-2783-10-39.
Lecorguillé M, Lioret S, de Lauzon-Guillain B, de Gavelle E, Forhan A, Mariotti F, et al. Association between Dietary Intake of One-Carbon Metabolism Nutrients in the Year before Pregnancy and Birth Anthropometry. Nutrients. 2020;12(3). https://doi.org/10.3390/nu12030838.
Mazidi M, Katsiki N, Mikhailidis DP, Banach M. Dietary choline is positively related to overall and cause-specific mortality: results from individuals of the National Health and Nutrition Examination Survey and pooling prospective data. Br J Nutr. 2019;122(11):1262–70.https://doi.org/10.1017/s0007114519001065
Merkiel S. Dietary intake in 6-year-old children from southern Poland: part 1--energy and macronutrient intakes. BMC Pediatr. 2014;14:197. https://doi.org/10.1186/1471-2431-14-197.
Willett W, Stampfer MJ. Total energy intake: implications for epidemiologic analyses. Am J Epidemiol. 1986;124(1):17–27. https://doi.org/10.1093/oxfordjournals.aje.a114366.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62. https://doi.org/10.1017/s1368980009991698.
Esmaillzadeh A. Final report of "relative validity and reproducibility of a semi-quantitative food frequency questionnaire to assess long-term dietary intakes in children". Deputy for Research; 2012.
USDA Database for the Choline Content of Common Foods, Release 2 (2008) 2020 [Available from: https://data.nal.usda.gov/dataset/usda-database-choline-content-common-foods-release-2-2008.
Zeisel SH, Mar MH, Howe JC, Holden JM. Concentrations of choline-containing compounds and betaine in common foods. J Nutr. 2003;133(5):1302–7. https://doi.org/10.1093/jn/133.5.1302.
Haytowitz D, Ahuja J, Wu X, Khan M, Somanchi M, Nickle M, et al. USDA National Nutrient Database for standard reference, legacy. USDA National Nutrient Database for Standard Reference 2018.
Howe JC, Williams JR, Holden JM, Zeisel SH, Mar M-H. USDA database for the choline content of common foods. Release One; 2004.
Patterson KY, Bhagwat SA, Williams JR, Howe JC, Holden J, Zeisel S, et al. USDA database for the choline content of common foods, release two. Nutrient Data Laboratory, Beltsville Human Nutrition Research Center, ARS, USDA. 2008.
Organization WH. WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development: World Health Organization; 2006.
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32(9 Suppl):S498-504.https://doi.org/10.1097/00005768-200009001-00009, S516.
Saraf-Bank S, Haghighatdoost F, Esmaillzadeh A, Larijani B, Azadbakht L. Adherence to Healthy Eating Index-2010 is inversely associated with metabolic syndrome and its features among Iranian adult women. Eur J Clin Nutr. 2017;71(3):425–30. https://doi.org/10.1038/ejcn.2016.173.
Willett WC, Howe GR, Kushi LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. 1997;65(4 Suppl):1220S–8S; discussion 9S–31S. https://doi.org/10.1093/ajcn/65.4.1220S.
Schwab U, Törrönen A, Toppinen L, Alfthan G, Saarinen M, Aro A, et al. Betaine supplementation decreases plasma homocysteine concentrations but does not affect body weight, body composition, or resting energy expenditure in human subjects. Am J Clin Nutr. 2002;76(5):961–7. https://doi.org/10.1093/ajcn/76.5.961.
del Favero S, Roschel H, Artioli G, Ugrinowitsch C, Tricoli V, Costa A, et al. Creatine but not betaine supplementation increases muscle phosphorylcreatine content and strength performance. Amino Acids. 2012;42(6):2299–305. https://doi.org/10.1007/s00726-011-0972-5.
Moro T, Badiali F, Fabbri I, Paoli A. Betaine Supplementation Does Not Improve Muscle Hypertrophy or Strength Following 6 Weeks of Cross-Fit Training. Nutrients. 2020;12(6). https://doi.org/10.3390/nu12061688.
Long JA, Zhong RH, Chen S, Wang F, Luo Y, Lu XT, et al. Dietary betaine intake is associated with skeletal muscle mass change over three years in middle-aged adults: the Guangzhou Nutrition and Health Study. Br J Nutr. 2020:1–21. https://doi.org/10.1017/s0007114520002433.
Hongu N, Sachan DS. Supplemented with Carnitine, choline and caffeine regardless of exercise. J Med Sci. 2002;2(2):59–64. https://doi.org/10.3923/jms.2002.59.64.
Yang TT, Chang CK, Tsao CW, Hsu YM, Hsu CT, Cheng JT. Activation of muscarinic M-3 receptor may decrease glucose uptake and lipolysis in adipose tissue of rats. Neurosci Lett. 2009;451(1):57–9. https://doi.org/10.1016/j.neulet.2008.12.029.
Huang Q-C, Xu Z-R, Han X-Y, Li W-F. Changes in hormones, growth factor and lipid metabolism in finishing pigs fed betaine. Livest Sci. 2006;105(1):78–85. https://doi.org/10.1016/j.livsci.2006.04.031.
Acknowledgments
The authors thank the subjects who participated in the study. We want to acknowledge the contribution of Hossein Shahinfar from Tehran university of medical science for assistance.
Funding
This study was funded by the National Institute for Medical Research Development (Grant Number: 94–04–161-31112).
Author information
Authors and Affiliations
Contributions
AJ, YJ, and LA contributed to the design of the study. AJ contributed to the acquisition and analysis of the data. AJ drafted the manuscript. YJ revised the manuscript. KS and NB edited the english and commented on the manuscript. LA supervised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in this study in accordance with the Declaration of Helsinki and ethically approved by the National Institute for Medical Research Development of Tehran University of medical science, Tehran, Iran (IR. TUMS. VCR.REC.94–04–161-31 112). Their mothers provided written and informed consent for participation of their children after informing them of the study objective, procedures, and their full right to participate or withdraw their consent at any time in the study.
Consent for publication
Not applicable.
Competing interests
The author declared no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jafari, A., Jalilpiran, Y., Suitor, K. et al. The association of dietary choline and betaine and anthropometric measurements among Iranian children: a cross-sectional study. BMC Pediatr 21, 213 (2021). https://doi.org/10.1186/s12887-021-02677-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-021-02677-1