
Abstract
Background
Household food insecurity (FI), even at marginal levels, is associated with poor child health outcomes. The Nutrition Screening Tool for Every Preschooler (NutriSTEP®) is a valid and reliable 17-item parent-completed measure of nutrition risk and includes a single item addressing FI which may be a useful child-specific screening tool. We evaluated the diagnostic test properties of the single NutriSTEP® FI question using the 2-item Hunger Vital Sign™ as the criterion measure in a primary care population of healthy children ages 18 months to 5 years.
Results
The sample included 1174 families, 53 (4.5%) of which were marginally food secure. An affirmative response to the single NutriSTEP® question “I have difficulty buying food I want to feed my child because food is expensive” had a sensitivity of 85% and specificity of 91% and demonstrated good construct validity when compared with the Hunger Vital Sign™.
Conclusion
The single NutriSTEP® question may be an effective screening tool in clinical practice to identify marginal food security in families with young children and to link families with community-based services or financial assistance programs including tax benefits.
Trial registration
TARGet Kids! practice-based research network (Registered June 5, 2013 at www.clinicaltrials.gov; NCT01869530); www.targetkids.ca
Similar content being viewed by others

Introduction
Household food insecurity (FI) — a household’s experience of inadequate or insecure access to sufficient, safe and nutritious food because of income or finances — is a major public health problem [1, 2]. Household food insecurity is associated with poor child health outcomes, even at marginal levels [3,4,5]. Previous research also shows that families with marginal food security are more like food-insecure households than food-secure households [6].
Families affirming one or both of the first 2 items of the 18-item U.S. Household Food Security Screening Module (HFSSM), are considered marginally food secure [6, 7]. The first item measures uncertainty about having enough food and the second item measures uncertainty about exhausting their food supply. Developed in the U.S., these items comprise the 2-item Hunger Vital Sign™ (HVS) [8], now advocated for use as a screening tool for marginal food security in clinical practice and embedded into the electronic medical record system along with clinical and billing codes in some areas. However, the 2 items on the HVS™ are from the adult module in the 18-item HFSSM, which may not apply to children [9]. Furthermore, a 1-item child-specific screen for use in paediatric primary care practice may have greater utility in identifying marginal food security in families with young children.
The Nutrition Screening Tool for Every Preschooler (NutriSTEP®) is a valid and reliable 17-item parent-completed questionnaire developed in Canadian children addressing multiple domains of nutrition risk [10, 11]. A single item addressing FI may be a useful child-specific screening tool. The 17-item NutriSTEP® has an area under the curve of 84.6% compared with a dietitian-completed assessment [10, 11]. However, the accuracy of the FI question is unknown. We aimed to examine the diagnostic test properties of the single NutriSTEP® FI question.
Methods
This cross-sectional study enrolled healthy children 18 months to 5 years of age during scheduled health supervision visits at primary care practices in Toronto, Canada participating in a research network called TARGet Kids! (www.targetkids.ca). TARGet Kids! is an ongoing, open, longitudinal cohort enrolling healthy children from birth to age 5 years. The profile of this cohort has been previously described [12]. Study participants were recruited by trained research personnel embedded in participating practices. Informed consent was obtained from parents of participants, who completed standardized questionnaires including the FI screens. For the purpose of this study, children were included if they had complete data on both the HVS™ and NutriSTEP® questionnaires. All methods were performed in accordance with the relevant guidelines and regulations and approved by Research Ethics Boards at the Hospital for Sick Children and St. Michael’s Hospital, Toronto.
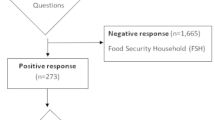
Parents completed the HVS™, the first 2 items of the 18-item HFSSM; this brief 2-item measure has 97% sensitivity and 83% specificity for identifying marginal food security, using the HFSSM as the criterion measure [8]. The HVS™ questions are: “Within the past 12 months, we worried whether our food would run out before we got money to buy more” and “Within the past 12 months, the food we bought just didn’t last and we didn’t have money to buy more” with response options “Was that often true, sometimes true or never true for your household in the past twelve months?” According to convention, both items were coded as an affirmative response if either “often true” or “sometimes true” was selected [7, 8]. By definition, families affirming one or both items were classified as having marginal food security.
Parents also completed the 17-item NutriSTEP® which included the FI question: “I have difficulty buying food I want to feed my child because food is expensive” with response options: “most of the time”; “sometimes”; “rarely”; “never”. Using the same convention as for the HVS™ questions, this single item was coded as an affirmative response if “most of the time”, “sometimes”, or “rarely” was selected. We included “rarely” as an affirmative response as we reasoned that families struggling to meet their needs, may either choose not to disclose or select “rarely” due to stigma or shame [13]. Families affirming this single item were classified as having marginal food security.
We examined the diagnostic test properties (including sensitivity and specificity) of the 1-item NutriSTEP® FI question using the 2-item HVS™ as the criterion measure. We then examined convergent construct validity (the correspondence between the 1-item NutriSTEP® screen and theoretically related variables, e.g. self-report family income) using multiple logistic regression. Convergent construct validity was tested by comparing the multiple logistic regression models for the 1-item NutriSTEP® with those of the 2-item HVS™ evaluating the associations of these FI measures with variables considered predictors of marginal food security (family income, maternal education and parent employment status) adjusting for covariates. Missing covariate data (< 15% missing) were handled using multiple imputation. Statistical significance was defined as p < 0.05, and all statistical tests were 2-sided. Statistical analysis was conducted using SAS version 9.4 (SAS Institute).
Results
Participants
Of 1753 children recruited to the TARGet Kids! cohort, 1174 children had complete data on the HVS™ and NutriSTEP® questionnaires. Of these, 53 (4.5%) children were living in families with marginal food security as determined by the 2-item HVS™. Compared with families not at risk for food insecurity, a higher proportion of children in families at risk for food insecurity had a lower family income, a mother with high school education or less, 1 or both parents were unemployed, and were from a single-parent family (Table 1).
Diagnostic test properties of the 1-item NutriSTEP®
The diagnostic test properties of the single FI NutriSTEP® question, compared with the 2-item HVS™ as the criterion measure were: sensitivity 84.9% (95% CI: 72.4, 93.3), specificity 91.2% (95% CI: 89.4, 92.8), false positive rate 8.8% (95% CI: 7.2, 10.8), positive predictive value 31.3% (95% CI: 26.7, 36.2), negative predictive value 99.2% (95% CI: 98.5, 99.6). An affirmative response indicating marginal food security on the 1-item screen was 9.6 times more likely (LR+ = 9.6; 95% CI: 7.7, 12.0) for those with marginal food security as determined by the 2-item HVS™ (Table 2).
Construct validity
An affirmative response to the single NutriSTEP® FI question was associated with higher odds of family income less than CAD $40,000 (adjusted odds ratio [aOR]: 7.4; 95% CI: 3.4, 16.1; p < 0.001), lower maternal education (high school or less, aOR: 1.8; 95% CI: 0.9, 3.7; p = 0.09; college/trades certificate, aOR: 1.7; 95% CI: 1.0, 2.8; p = 0.049), and both parents being unemployed (aOR: 3.3; 95% CI: 1.1, 10.4; p = 0.04). These associations were similar to (perhaps somewhat weaker than) the corresponding associations for the HVS™ (Table 3).
Discussion
In this large healthy child cohort recruited in urban Canadian primary care practice, the 1-item NutriSTEP® FI question demonstrated strong diagnostic test properties and good construct validity. This single question may be an effective screening tool for identifying young children living in families with marginal food security in primary care settings. Furthermore, increasingly recognized is the importance of nutrition security, defined as ‘having consistent access, availability, and affordability of foods and beverages that promote well-being and prevent disease’ [14]. When using the 17-item NutriSTEP® in healthy toddlers and preschoolers in community settings, this single question provides clinicians with a valid measure of marginal food security, as well as nutrition risk.
Marginal household food security is associated with poor educational outcomes and emotional and behavioural problems in children, as well as maternal major depression and anxiety [3,4,5]. Sociodemographic characteristics of households reporting marginal food security (affirming 1 or 2 items) are more similar to those experiencing more severe food insecurity (affirming > 2 items) than food secure households (affirming 0 items) [3,4,5]. Such evidence of associations of marginal food security and both immediate and long-term adverse health outcomes in young children highlights the importance of screening for social needs in paediatric primary care practice in an empathic and efficient manner.
There are study limitations. First, we did not use the 18-item HFSSM as our criterion measure, so we could not examine associations between the single question and more severe household FI. However, because we were evaluating a brief measure of marginal food security suitable for screening in healthcare settings, the HVS™ is considered the gold standard and therefore is the more appropriate criterion measure. In addition, detection of marginal food security is an appropriate target for a clinical screening tool. Second, our sample had a relatively high family income, which may not be representative of other families. However, because FI screening tools are likely to perform better in low income populations, it is important to evaluate them in an economically diverse population [9].
The 1-item NutriSTEP® FI question is an alternative brief measure of marginal food security and one that is child-specific, which is suitable for screening for marginal food security in families with children in clinical settings. While no previous study has examined this single item on the NutriSTEP® as a food security screen, others have examined the validity of a single item measure of food security. Nolan et al. [15] validated the single question “In the past 12 months, were there any times that you ran out of food and couldn’t afford to buy more?” using the HFSSM as the criterion measure in a random sample of households in three low income regions in Australia, including 56% with children under age 18 years. The question had high specificity (96%) but low sensitivity (56.9%). Urke et al. examined each question in the 18-item HFSSM with the purpose of developing a rapid assessment of food security among Inuit adults and children. They identified one child item (“In the last 12 months, were there times when it was not possible to feed the children a healthy meal because there was not enough money?”) with strong diagnostic test properties using an affirmative response to any 2 HFSSM questions as their criterion measure [9]. Our study differs from Urke et al. in several ways. Our study was conducted in an urban primary care setting, with an anticipated lower prevalence of FI than seen in the remote Arctic setting. In addition, we used the HVS™ as the criterion measure, a measure of marginal food security, rather than the more severe problem of food insecurity. It is possible that the 1-item NutriSTEP® FI question (“I have difficulty buying food I want to feed my child because food is expensive”) may more effectively target marginal food security, which is a more appropriate target for primary care screening efforts. Future research should empirically examine this hypothesis.
While healthcare providers recognize the importance of identifying poverty in clinical settings, they identify time constraints and multiple competing demands as barriers to integrating social needs screening into healthcare [16]. Using a single question to measure marginal food security may be more feasible than using a 2-item tool in a busy practice and would allow clinicians to intervene on unmet social needs by linking families to community-based services or financial assistance programs including tax benefits to which they may be entitled. Despite the clear importance of social determinants to child health, limited research has addressed clinical implementation of social needs screening. However, the importance of identification of caregiver needs and priorities, and referral to appropriate community supports have been highlighted [17, 18]. Furthermore, caregivers experiencing food insecurity report feeling ashamed or embarrassed in reporting FI and that health care provider empathy, concern and empowerment can mitigate these challenges [13]. This single question may be useful for opening a dialogue in the context of a trusting relationship with a health care provider, thus facilitating linkage of families with needed resources.
Conclusion
The single NutriSTEP® question may be an effective screening tool in clinical practice to identify marginal food security in families with young children and to link families with community-based services or financial assistance programs including tax benefits.
Availability of data and materials
Data are available upon request by contacting www.targetkids.ca/contact-us/. The full data are not freely available to respect the confidentiality of our participants, ensure data integrity, and avoid scientific overlap between projects. Once initial contact has been made, we request a short research proposal which will be subject to review by the TARGet Kids! Scientific Committee and approval by institutional IRBs.
Abbreviations
- CI:
-
Confidence Interval
- NHQ:
-
Nutrition and Health Questionnaire
- OR:
-
Odds Ratio
- TARGet Kids!:
-
The Applied Research Group for Kids
References
Council on Community Pediatrics Con. Promoting food security for all children. Pediatrics. 2015;136(5):e1431–e38. https://doi.org/10.1542/peds.2015-3301.
Tarasuk V, Mitchell A, Dachner N. Household Food Insecurity in Canada, 2014. Toronto: Research to identify policy options to reduce food insecurity (PROOF); 2016.
Shankar P, Chung R, Frank DA. Association of food insecurity with children’s behavioral, emotional, and academic outcomes: a systematic review. J Dev Behav Pediatr. 2017;38(2):135–50. https://doi.org/10.1097/DBP.0000000000000383.
Whitaker RC, Phillips SM, Orzol SM. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics. 2006;118(3):e859–w68. https://doi.org/10.1542/peds.2006-0239.
Cook JT, Black M, Chilton M, Cutts D, Ettinger de Cuba S, Heeren TC, et al. Are food Insecurity’s health impacts underestimated in the U.S. population? Marginal food security also predicts adverse health outcomes in young U.S. children and mothers. Adv Nutr. 2013;4(1):51–61. https://doi.org/10.3945/an.112.003228.
Coleman-Jensen A, Rabbitt MP, Gregory CA, et al. Household food security in the United States in 2017. In: ER-256R: U.S. Department of Agriculture, Economic Research Service; 2018.
United States Department of Agriculture. U.S. Household food security survey module: three stage design, with screeners 2012 [Accessed 27 Jun 2019]. Available from: http://www.ers.usda.gov/datafiles/Food_Security_in_the_United_States/Food_Security_Survey_Modules/hh2012.pdf.
Hager ER, Quigg AM, Black MM, Coleman SM, Heeren T, Rose-Jacobs R, et al. Development and validation of a 2-item screen to identify families at risk for food insecurity. Pediatrics. 2010;126(1):e26–32. https://doi.org/10.1542/peds.2009-3146.
Urke HB, Cao ZR, Egeland GM. Validity of a single item food security questionnaire in Arctic Canada. Pediatrics. 2014;133(6):e1616–23. https://doi.org/10.1542/peds.2013-3663 [published Online First: 2014/05/28].
Randall Simpson J, Keller H, Rysdale L, et al. Nutrition screening tool for every preschooler (NutriSTEP): validation and test–retest reliability of a parent-administered questionnaire assessing nutrition risk of preschoolers. Eur J Clin Nutr. 2008;62(6):770–80. https://doi.org/10.1038/sj.ejcn.1602780.
Randall Simpson J, Gumbley J, Whyte K, Lac J, Morra C, Rysdale L, et al. Development, reliability, and validity testing of toddler NutriSTEP: a nutrition risk screening questionnaire for children 18–35 months of age. Appl Physiol Nutr Metab. 2015;40(9):877–86. https://doi.org/10.1139/apnm-2015-0048.
Carsley S, Borkhoff CM, Maguire JL, Birken CS, Khovratovich M, McCrindle B, et al. Cohort profile: the applied research Group for Kids (TARGet Kids!). Int J Epidemiol. 2015;44(3):776–88. https://doi.org/10.1093/ije/dyu123.
Barnidge E, Krupsky K, LaBarge G, Arthur J. Food insecurity screening in pediatric clinical settings: a caregivers’ perspective. Matern Child Health J. 2019;24(1):101–9. https://doi.org/10.1007/s10995-019-02785-6.
Mozaffarian D, Fleischhacker S, Andrés JR. Prioritizing nutrition security in the US. JAMA. 2021. https://doi.org/10.1001/jama.2021.1915.
Nolan M, Williams M, Rikard-Bell G, et al. Food insecurity in three socially disadvantaged localities in Sydney, Australia. Health Promot J Austr. 2006;17(3):247–54. https://doi.org/10.1071/he06247 [published Online First: 2006/12/21].
Bayoumi I, Coo H, Purkey E. et al. Implementing a Clinical Tool to Screen for Poverty in Primary and Pediatric Care Settings. North American Primary Care Research Group Annual Meeting. Montreal; 2017.
Dworkin PH, Garg A. Considering approaches to screening for social determinants of health. Pediatrics. 2019;144(4):e20192395. https://doi.org/10.1542/peds.2019-2395.
Beck AF, Klein MD. Moving from social risk assessment and identification to intervention and treatment. Acad Pediatr. 2016;16(2):97–8. https://doi.org/10.1016/j.acap.2016.01.001.
Acknowledgements
We thank all participating children and families for their time and involvement in TARGet Kids! and are grateful to all practice site physicians, research staff, collaborating investigators, trainees, methodologists, biostatisticians, data management personnel, laboratory management personnel, and advisory committee members who are currently involved in the TARGet Kids! primary care practice-based research network. TARGet Kids! Collaboration details may be found on our website (www.targetkids.ca).
Funding
Funding to support TARGet Kids! was provided by multiple sources including the Canadian Institutes for Health Research (CIHR), namely the Institute of Human Development, Child and Youth Health [No. FRN 114945 to JLM, No. FRN 115059 to PCP] and the Institute of Nutrition, Metabolism and Diabetes [No. FRN 119375 to CSB], as well as, the St. Michael’s Hospital Foundation. The Paediatric Outcomes Research Team (PORT) is supported by a grant from The Hospital for Sick Children Foundation.
Role of Funder: Funding agencies had no role in the design, collection, analyses or interpretation of the results of this study or in the preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
IB, KN and CMB conceptualized and designed the study, performed the statistical analysis, interpreted the data, drafted the manuscript, critically revised and reviewed the manuscript for important intellectual content, and approved the final manuscript. CSB conceptualized and designed the study, designed the data collection instruments, obtained funding, interpreted the data, drafted the manuscript, critically revised and reviewed the manuscript for important intellectual content, and approved the final manuscript. PP and JM designed the data collection instruments, supervised the data collection, critically reviewed the manuscript for important intellectual content, and approved the final version of the manuscript. CM and JRS interpreted the data, critically reviewed the manuscript for important intellectual content, and approved the final version of the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Research Ethics Boards at the Hospital for Sick Children and St. Michael’s Hospital, Toronto approved the study.
Consent for publication
N/A.
Competing interests
Dr. Bayoumi reports receiving unrestricted peer-reviewed grants from the Academic Health Science Centre Alternative Funding Plan Innovation Fund and PSI Foundation, unrelated to this study. Dr. Birken reports receiving an unrestricted grant from Walmart Canada Community Grants, unrelated to this study. Dr. Parkin reports receiving a grant from the Hospital for Sick Children Foundation during the conduct of the study. Dr. Parkin reports receiving the following grants unrelated to this study: a grant from Canadian Institutes of Health Research (FRN # 115059) for an ongoing investigator-initiated trial of iron deficiency in young children, for which Mead Johnson Nutrition provides non-financial support (Fer-In-Sol® liquid iron supplement) (2011–2017); and peer-reviewed grants for completed investigator-initiated studies from Danone Institute of Canada (2002–2004 and 2006–2009), Dairy Farmers of Ontario (2008–2010). Dr. Maguire reports receiving an unrestricted research grant for a completed investigator-initiated study from the Dairy Farmers of Canada (2011–2012). Dr. Randall Simpson reports receiving grants for investigator-initiated studies from the Canadian Institutes for Health Research, the Danone Institute of Canada, and the Canadian Foundation for Dietetic Research for completed NutriSTEP®-related studies. Dr. Borkhoff reports previously receiving a grant for a completed investigator-initiated study from the Sickkids Centre for Health Active Kids (CHAK) (2015–2016) involving the development and validation of a risk stratification tool to identify young asymptomatic children at risk for iron deficiency. These agencies had no role in the design, collection, analyses or interpretation of the results of this study or in the preparation, review, or approval of the manuscript. The remaining authors report no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bayoumi, I., Birken, C.S., Nurse, K.M. et al. Screening for marginal food security in young children in primary care. BMC Pediatr 21, 196 (2021). https://doi.org/10.1186/s12887-021-02674-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-021-02674-4