
Abstract
Background
Anaemia is one of the major causes of death among children under five years in Africa, with a prevalence of 64.6% among pre-school children. In 2014, we conducted a cross-sectional study in Namutumba district in East-central Uganda to determine the prevalence and factors associated with anaemia among children aged 6 to 59 months.
Methods
We conducted a household survey in 376 randomly selected households. One child aged 6 to 59 months was randomly sampled from each selected household. A structured questionnaire administered to an adult caregiver was used to collect household data. Blood was collected by finger or heel prick to estimate the haemoglobin level using a portable haemocue analyser. Anthropometric data including age, weight and height was collected for each child. A modified poisson regression model was used to determine the correlates of anaemia, prevalence ratios and their 95% confidence intervals (CI).
Results
The prevalence of anaemia was high (58.8%) and was highest among children aged 12 to 23 months (68.5%) and males (61.3%). About 27.7% children were stunted. Children aged 6–11 and 12–23 months were more likely to be anaemic (APR = 1.12; 95% CI: 1.05–1.19 and APR = 1.12; 95% CI: 1.00–1.24 respectively), Resident of Magada and Namutumba (urban areas) were less likely to be anaemic (APR = 0.89; 95% CI: 0.87–0.91and APR = 0.86; 95% CI: 0. 85–0.88 respectively). Children of caretakers of a big family size (seven or more children) and with any formal education were less likely to be anaemic (APR = 0.94; 95% CI: 0.89–0.99 and APR = 0.93; 95% CI: 0.87–0.99). Stunting (HAZ scores) was a predictor of anaemia (APR = 1.07; 95% CI: 1.02–1.12).
Conclusion
Anaemia is highly prevalent among children and there is need to invest in measures to prevent anaemia, especially among children in the rural areas.
Similar content being viewed by others


Background
Anaemia is a global public health threat especially in the developing countries [1–4]. In Africa, the prevalence of anaemia among preschool children is estimated at 64.6% [4], however, community-based estimates of anaemia prevalence among children in settings where malaria is endemic range from 49 to 76% [5]. Childhood anaemia is a preventable condition, which has serious consequences including growth retardation, poor immune system and increased susceptibility to diseases [6], and death [7–9] and has severe socio-economic consequences for families and communities.
Despite several interventions like de-worming, malarial presumptive treatment, provision of fortified complimentary foods or enriched foods [9, 10] that have been put in place to increase the iron status of children less than five years, anaemia remains a challenge in Uganda. It is estimated that 50% of children under five years in Uganda have anaemia. The prevalence of anaemia among children in the East Central region of Uganda, the setting for this study is even higher at 67.5% [11].
Namutumba district has had frequent episodes of malnutrition over the past five years, an indication of potentially high micronutrient deficiencies and anaemia. Estimating the prevalence of anaemia and especially understanding its determinants is critical in designing effective anaemia interventions. This study assessed the prevalence, nutritional and non-infectious disease factors associated with anaemia among children aged 6 to 59 months in Namutumba district, in East-central Uganda.
Methods
This was a quantitative cross-sectional household survey.
Study settings
This study was conducted in Namutumba district, in the east-central region of Uganda, a district that has suffered frequent episodes of malnutrition [12]. The main occupation of people in Namutumba district, across all sub-counties, is largely farming and major crops include; rice, groundnuts, sorghum, millet and cassava.
Sample size calculation
The sample size was estimated using Bennett’s cluster survey sampling formula, assuming prevalence of anaemia of 67.5% among children aged 6 to 59 months, a design effect of 1.12, and standard error of 0.0255 [11]. Seven respondents were selected per cluster. A total of 376 children were recruited for the study and their mothers/caregivers were interviewed.
Sampling procedure
Multi-stage sampling procedure was used. Three (50%) of the six sub-counties in the district were randomly selected. In each sub-county two parishes were randomly selected by ballot method and all villages within the selected parishes were selected. Overall, 54 villages were selected out of 348 villages within the district. Within each village (cluster) seven households were selected, using systematic random sampling. Household lists (sample frame) were obtained from Village Health Teams (VHTs). The sampling interval was determined by dividing the total number of households in the village by seven. In case the selected household did not have an eligible child, the next household was selected. Within each household one child aged 6 to 59 months was selected. In households with more than one child, one was selected randomly by the ballot method from the list of household members. All children aged 6 to 59 months who had stayed for at least 6 months in Namutumba district by the time of the study were eligible for enrollment.
Data collection methods
Data collection was conducted from April to May 2014. Trained research assistants conducted face-to-face interviews with caregivers of the children using structured questionnaires. A caregiver was defined as the person who looks after or was in charge of the children’s well-being in the household.
Measures
Some questions were adapted from the Uganda Demographic and Health Survey (socio demographic characteristics including; number of children in the household, number of people living in the household, respondents’ relationship with the child, age of caregiver and age of the child), while others were developed based on the study objectives. The pretested questionnaire was used to collect data on the non-nutritional factors which included; socio demographic characteristics and nutritional related factors such as household dietary diversity, food consumption, age at cessation of breast feeding and child health history.
Haemoglobin level determination
Haemoglobin (Hb) levels were measured using the HaemoCue method (HaemoCue Hb® 301, Sweden) [13]. Hb determination was done within the homes by a team of trained health personnel. Blood was obtained from children by a heel or finger prick. The first drop of blood was wiped off and the next drop was collected into a disposable microcuvette. Blood was drawn carefully to avoid introducing bubbles. The Hb levels were displayed on a digital register on the HaemoCue 301 and recorded to the nearest 0.1 g/dl. To ensure hygiene and safety of the procedure, each set of accessory (lancet, microcuvette, gloves, and alcohol swabs) was used once. To ensure accuracy of the HaemoCue, a controlled cuvette was used on a daily basis [13]. Anaemia was classified into severe, moderate and mild according to the WHO/United Nations University/UNICEF cut –offs [14].
Nutrition status assessment
The weight of each child was measured using a Seca weighing scale, which was calibrated to zero. Caregivers were asked to remove the child’s clothes or dress them in light clothes. The child was then told to stand on the weighing scale and the weight of the child was recorded. In case the child was not able to stand the caregiver of the child was told to stand on the weighing scale, his or her measurement was taken first then both child and caregiver were weighed. To obtain the weight of the child, the weight of the caregiver was subtracted from the measurement of both child and the mother. The weight was recorded to the nearest 0.1 kg.
To measure the height, the height board was placed either horizontally or vertically on a flat ground surface. The child’s caregiver was requested to remove the child’s foot wear and headgear then the child was assisted to stand against the height board. Children who were less than 2 years or less than 87 cm were measured while lying down (recumbent). The research assistant held the child’s body (head and legs) in the appropriate position to ensure accuracy. The height/length readings were recorded to the nearest 0.1 cm. The nutrition status of the children was determined using weight, height and age of the children. The WHO nutrition indices were used to classify the nutritional status as underweight (Weight for Age Z score, < −2.0 standard deviations), stunting (Height for Age Z score or Length for Age, < −2.0 standard deviations), wasting (Weight for Height Z score, < −2.0 standard deviations, or normal [15].
Study variables
The dependent variable was anaemia (Haemoglobin levels <11 g/l). Independent variables included; socio-demographic factors, (number of children and number of household members) and other factors included; history of child health, child nutritional status, dietary diversity and age at cessation of breastfeeding, Maternal factors (education, age, and occupation), area of residence and Food consumption.
Data analysis
Data were analysed using STATA version 12.0. Anaemia was categorized using the WHO [14] classification into; severe anaemia (Hb <7.0 g/dl), moderate anaemia (Hb level 7.0–9.9 g/dl), mild anaemia (Hb level 10.0–10.9 g/dl), and no anaemia (Hb levels ≥11 g/dl). Univariable analysis was conducted to describe the background characteristics of the households. Continuous variables, which included haemoglobin levels and age were summarized using proportions, means and standard deviations.
At bivariable analysis, the association between independent variables and anaemia was examined. The outcome variable was categorized into two; anaemia (Hb levels < 11 g/dl) and no anaemia (Hb levels ≥ 11 g/dl). A modified Poisson regression model with robust error variance was used to estimate prevalence ratios (PR) as a measure of association for the relationship between independent variables (maternal education, maternal occupation, maternal age , child’s sex, child’s age, and feeding practices, area of residence and history of child morbidity) and anaemia as the primary outcome. PR was used as a measure of association because of the high prevalence of the outcome (>10%), thus providing a better estimate of risk than the odds ratio (OR) [16, 17]. Adequacy of food consumption was categorized as; acceptable (score > 35), borderline (score 21.5–≤ 35) and poor (score <21.5), based on the UNWFP food consumption score [18]. The Food Consumption Score (FCS) is a composite score based on dietary diversity, food frequency, and relative nutritional importance of different food groups. The respondent is asked about frequency of consumption over a recall period of the past 7 days.
Nutrition status data was analysed using ENA for SMART (Version 2011). The WHO cutoff points were used to categorize the nutrition status of children including weight for height (WHZ) scores to determine whether the child was wasted, weight for age (WAZ) scores to determine whether the child was underweight, and height for age (HAZ) scores to determine whether child was stunted. The WHZ, WAZ and HAZ scores were categorized into malnutrition or normal nutrition status. The categorized nutrition status data was then exported into STATA 12.0 for further analysis. Prevalence ratios and their 95% confidence intervals were used to investigate associations between malnutrition indices (underweight, wasting and stunting) with anaemia. Statistical significance was established when the p – value was less than 0.05.
At multivariable analysis, a modified Poisson regression model with robust error variance was used to estimate adjusted prevalence ratios and their 95% confidence interval [17]. Variables, with p < 0.20 at bivariable analysis or potential confounders were considered for the multivariable analysis. The final multivariable model was selected by adding variables to the model using the forward selection method Adjustment for correlation within sub-counties was done at multivariable analysis.
Results
A total of 378 children aged 6 to 59 months were identified for the study from Magada, Namutumba and Bulange sub-counties. Two eligible individuals declined participation. A total of 376 children participated in the study: 49.5% (186) were males while 50.5% (190) were females (Table 1). The mean age of the children was 24.9 months with a standard deviation (SD) of +/−13.8. Most of the children were residing in Magada sub-county 52.7% (198), followed by Namutumba subcounty 25.8% (97) (Table 1).
Nutrition status of the children aged 6 to 59 months
The prevalence of wasting (WHZ < −2 SD) was 5.3% (n = 20), higher among males (7.5%) than females (3.2%). The prevalence of underweight (WAZ < −2SD) was 12.8% (48) while the prevalence of stunting (HAZ < −2SD) was 27.7% (104).
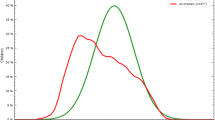
Prevalence of anaemia among children aged 6 to 59 months in Namutumba District
Overall, 58.8% (221) of the children had anaemia (haemoglobin level below 11 g/dl). The haemoglobin levels ranged from 4.4 to 13.5 g/dl with mean haemoglobin level of 10.5 g/dl (SD 1.42). The proportion of children who had severe anaemia (Hb < 7 g.dl) was 1.3% (5), while those with moderate anaemia was 27.7% (104), and mild anaemia was 29.8% (112) (Fig. 1).

Recruitment Flow chart
Factors associated with child anaemia
At bivariable analysis, factors that were associated with anaemia included; child age, number of household members, number of children in a household, respondents education level, area of residence, child having suffered from fever in the past 3 months and stunting (Table 2).
At multivariable analysis, factors that increased likelihood of anaemia included; number of children in a household, child’s age, sub county of residence, and stunting, while being educated was protective (Table 3).
Discussion
This study assessed the prevalence and non-infectious factors associated with anaemia among children aged 6 to 59 months in Namutumba district in Uganda. We found that 58.8% of the children aged 6 to 59 months were anaemic. Anaemia prevalence was highest among the male children (61.3%) and those aged 12 to 23 months (68.5%) followed by children aged 6 to 11 months, (63.5%). The prevalence of malnutrition was also very high with 27.7% of the children having chronic malnutrition/stunting and 5.3% with acute malnutrition/wasting. Factors associated with anaemia included; number of children in a household, respondents education level, area of residence, stunting, and child’s age.
The most prevalent conditions were moderate and mild anaemia, probably because mild and moderate anaemia is usually asymptomatic and may remain undetected and untreated [5, 19]. The prevalence of anaemia among the children was slightly lower than the East central regional average of 67.5% reported in the 2011 Uganda Demographic and Health Survey [11] but remains unacceptably high and is much higher than the prevalence in several sub-Saharan Africa countries such as Mali, Benin, Ethiopia, Senegal and the Middle East [9, 20–23]. Anaemia impairs the children’s immune system, leads to growth retardation and in severe cases may cause death if not well managed [24]. However, mothers can be taught and supported to prevent childhood anaemia at community level. The prevalence of anaemia in this region is of severe public health significance, well above the 40% WHO threshold, and clearly demands more aggressive interventions [14].
The high prevalence of anaemia in this district happens within the context of high levels of malnutrition with close to one third of the children having malnutrition. Stunting was significantly associated with anaemia unlike other nutrition indices such as wasting and underweight. Both stunting and anaemia (IDA) may be caused by malnutrition, and thus follow a similar causal pathway that is; feeding children less than four times a day and low dietary diversity [9, 25–28]. Both anaemia and stunting may result from failure to meet micronutrient requirements, including iron [29, 30]. Although the food consumption score was not significantly associated with anaemia, there was a high proportion of children with borderline and poor food consumption score with anaemia than those who had an acceptable food consumption score. This may be attributed to lack of diversified meals [9]. Presence of fever in the past three weeks was not significantly associated with anaemia in this study. However, the high levels of anaemia and chronic malnutrition might have been caused by infection diseases such as Malaria. Infections and especially malaria are major causes of anaemia in Africa [31].
According to the recent Uganda malaria indicator survey [32], malaria prevalence among children under five years was highest in the East Central region (where Namutumba lies), where 36% of children tested positive for malaria. Thus interventions to address anaemia and chronic malnutrition should be delivered in an integrated manner in order to comprehensively address the anaemia and various underlying problems.
Child age (6 to 23 months) was significantly associated with anaemia. The prevalence of anaemia was highest among the youngest age groups and generally reduced with increase in the age of the children [26, 27, 33, 34]. Iron stores are generally depleted among children by 6 months of age while the blood volume doubles from 4 to 12 months after birth. Thus, the dietary sources of iron are very important to keep up with this rapid rate of red blood cell synthesis and anaemia may result if the dietary sources are inadequate [1, 2].
The prevalence of anaemia was higher in the rural Bulange sub-county (79.0%) compared to Namutumba and Magada sub-counties probably due to higher levels of illiteracy and poorer access to health services, including health education [22]. Indeed, the prevalence of anaemia dropped with increase in the mother’s or caregiver’s level of education, as reported in other studies [1, 20, 26, 35, 36]. Although not significantly associated with anaemia, one third of the mothers/caregivers in this district did not know how to prevent anaemia, an indicator of the need for more education.
Families with seven or more children were less likely to have anaemic children compared to those with more children and the prevalence of anaemia increased with increasing number of children in the family. High maternal parity has been associated with anaemia as a high number of children impacts on the ability to feed them appropriately [37]. Most mothers, who had one to three children, were young mothers and two out of every three children among these young mothers had anaemia. Young mothers generally have challenges with child care due to limited resources and experience with child care and their children may have poorer health outcomes [38].
These findings highlight anaemia and underlying malnutrition among children as major challenges among rural communities in Eastern Uganda. There is need to concomitantly prioritize interventions to prevent anaemia and malnutrition in these communities in order to realize the much needed reduction of morbidity and mortality among infants and children in Uganda and other countries in sub-Saharan Africa.
Study limitations
Some potential causes of anaemia (e.g.,; infections and other diseases), and the type of anaemia were not assessed. Also, as a cross sectional study, causality could not be established for any of the associated variables.
Strength of the study
This household survey highlights the magnitude of anaemia in a rural district, one of the major and persistent contributors to childhood morbidity and mortality in Uganda and sub-Saharan Africa that has not received adequate attention.
Conclusion
There was a very high prevalence of child anaemia noted in this rural district of Uganda, most prevalent among children aged 12 to 23 months. The prevalence of chronic malnutrition was also high and was associated with anaemia. There is need to invest in age specific measures to prevent anaemia, including routine screening and management, especially among children 6 to 23 months, children in the rural areas and those with low caregiver education.
Abbreviations
- APR:
-
Adjusted prevalence ratio
- CI:
-
Confidence interval
- ENA:
-
Emergency nutrition assessment
- FCS:
-
Food consumption score
- HAZ:
-
Height-for-age Z score
- Hb:
-
Haemoglobin
- IPTc:
-
Intermittent preventive treatment for children
- IRB:
-
Internal review board
- ITN:
-
Insecticide treated nets
- PR:
-
Prevalence ratio
- SD:
-
Standard deviation
- SMART:
-
Standardized monitoring assessment relief transitions
- UN WFP:
-
United Nations World Food Programme
- UNICEF:
-
United Nations Children’s Fund
- VHTs:
-
Village health teams
- WAZ:
-
Weight-for-age Z score
- WHO:
-
World Health Organisation
- WHZ:
-
Weight-for-Height Z score
References
Leal LP, Batista Filho M, Lira PIC, Figueiroa JN, Osório MM. Prevalence of anemia and associated factors in children aged 6–59 months in Pernambuco, Northeastern Brazil. Rev Saude Publica. 2011;45(3):457–66.
Cardoso MA, Scopel KK, Muniz PT, Villamor E, Ferreira MU. Underlying factors associated with anemia in Amazonian children: a population-based, cross-sectional study. PLoS One. 2012;7(5):e36341.
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–51.
McLean E, de Benoist B, Egli I, Cogswell M, Wojdyla D. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005: Global database on anaemia. Public Health Nutr. 2008;12(4):444–54.
Schellenberg D, Schellenberg JR, Mushi A, Savigny D, Mgalula L, Mbuya C, Victora CG. The silent burden of anaemia in Tanzanian children: a community-based study. Bull World Health Org. 2003;81(8):581–90.
Shaw JG, Friedman JF. Iron deficiency anemia: focus on infectious diseases in lesser developed countries. Anemia. 2011;2011:10.
Kiguli S, Maitland K, George EC, Olupot-Olupot P, Opoka RO, Engoru C, Akech SO, Nyeko R, Mtove G, Reyburn H, et al. Anaemia and blood transfusion in African children presenting to hospital with severe febrile illness. BMC Med. 2015;13:21.
Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E, Carter JA. Child development: risk factors for adverse outcomes in developing countries. Lancet. 2007;369(9556):145–57.
Kikafunda JK, Lukwago FB, Turyashemererwa F. Anaemia and associated factors among under-fives and their mothers in Bushenyi district, Western Uganda. Public Health Nutr. 2009;12(12):2302.
Crawley J. Reducing the burden of anemia in infants and young children in malaria-endemic countries of Africa: from evidence to action. Am J Trop Med Hyg. 2004;71(2 Suppl):25–34.
Uganda Bureau of Statistics (UBOS), ICF. I. Uganda demographic and health survey 2011. Kampala: UBOS and Calverton, Maryland ICF International Inc; 2012.
MOH U, ACF. Nutrition survey report namutumba district, Uganda. Kampala: Ministry of Health Uganda; 2011.
Bhaskaram P, Balakrishna N, Radhakrishna KV, Krishnaswamy K. Validation of hemoglobin estimation using hemocue. Indian J Pediatr. 2003;70(1):25–8.
WHO, UNICEF, UNU. Iron deficiency anaemia: assessment, prevention and control, a guide for programme managers. Geneva: World Health Organization; 2001.
Group WMGRS. WHO child growth standards:length/height-for-Age, weight-for-Age, weight-for-length, weight-for-height and body mass index-for-Age: methods and development. Geneva: Group WMGRS; 2006.
Thompson ML, Myers JE, Kriebel D. Prevalence odds ratio or prevalence ratio in the analysis of cross sectional data: what is to be done? Occup Environ Med. 1998;55(4):272–7.
Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3:21.
WFP: Food Consumption Analysis: Calculation and use of the food consumption score in food security analysis, in Strengthening Emergency Needs Assessment Capacity, V. unit,.In. Rome: Editor World Food Programme; 2008.
Crawley J. Reducing the burden of anaemia in infants and young children in malaria- endemic countries of Africa: From evidence to action. Am J Trop Med Hyg. 2004;71(2):25–34.
Habte D, Asrat K, Magafu MG, Ali IM, Benti T, Abtew W, Tegegne G, Abera D, Shiferaw S. Maternal risk factors for childhood anaemia in Ethiopia. Afr J Reprod Health. 2013;17(3):110–8.
Ngnie-Teta I, Receveur O, Kuate-Defo B. Risk factors for moderate to severe anemia among children in Benin and Mali: insights from a multilevel analysis. Food Nutr Bull. 2007;28(1):76–89.
Rawat R, Saha KK, Kennedy A, Rohner F, Ruel M, Menon P. Anaemia in infancy in rural Bangladesh: contribution of iron deficiency, infections and poor feeding practices. Br J Nutr. 2014;111(1):172–81.
Tine RCK, Faye B, Ndour CT, Sylla K, Sow D, Ndiaye M, Ndiaye JL, Magnussen P, Alifrangis M, Bygbjerg IC, et al. Parasitic infections among children under five years in Senegal: prevalence and effect on anaemia and nutritional status. ISRN Parasitol. 2013;2013:6.
Ekiz C, Agaoglu L, Karakas Z, Gurel N, Yalcin I. The effect of iron deficiency anemia on the function of the immune system. Hematol J. 2005;5(7):579–83.
Xiaoliang Y, Rongwei Y, Junchi Z, Lei J, Jianmeng L, Ren A. The relationship between anemia and physical development among children at the ages of 3–6 years in 21 counties of China. Wei Sheng Yan Jiu. 2009;38(6):688–91.
Ayoya MA, Ngnie-Teta I, Raphin MN, Mamadoultaibou A, Boldon E, Saint-Fleur JE, Koo L, Bernard S. Prevalence and risk factors of anemia among children 6 to 59 months Old in Haiti. Anemia. 2013;2013:3.
Leite M, Cardoso A, Coimbra C, Welch J, Gugelmin S, Lira PC, Horta B, Santos R, Escobar A. Prevalence of anemia and associated factors among indigenous children in Brazil: results from the First National Survey of Indigenous People’s Health and Nutrition. Nutr J. 2013;12(1):69.
Paudel R, Pradhan B, Wagle RR, Pahari DP, Onta SR. Risk factors for stunting among children: a community based case control study in Nepal. Kathmandu Univ Med J. 2012;10(39):18–24.
Branca F, Ferrari M. Impact of micronutrient deficiencies on growth: the stunting syndrome. Ann Nutr Metab. 2002;46 Suppl 1:8–17.
Santos RF, Gonzalez ESC, Albuquerque EC, Arruda IKG, Diniz AS, Figueroa JN, Pereira APC. Prevalence of anemia in under five-year-old children in a children’s hospital in Recife, Brazil. Rev Bras Hematol Hemoter. 2011;33(2):100–4.
Ehrhardt S, Burchard G, Mantel C, Cramer J, Kaiser S, Kubo M, Otchwemah R, Bienzle U, Mockenhaupt F. Malaria, anemia, and malnutrition in african children--defining intervention priorities. J Infect Dis. 2006;194:108–14.
Uganda Bureau of Statistics (UBOS), ICF. I. Uganda Malaria Indicator Survey 2014–15. Kampala, Uganda, and Rockville, Maryland: UBOS and ICF International; 2015.
Thorne CJ, Roberts LM, Edwards DR, Haque MS, Cumbassa A, Last AR. Anaemia and malnutrition in children aged 0–59 months on the Bijagos Archipelago, Guinea-Bissau, West Africa: a cross-sectional, population-based study. Paediatr Int Child Health. 2013;33(3):151–60.
Pita GM, Jimenez S, Basabe B, Garcia RG, Macias C, Selva L, Hernandez C, Cruz M, Herrera R, O’Farrill R, et al. Anemia in children under five years old in Eastern Cuba, 2005–2011. MEDICC Rev. 2014;16(1):16–23.
Oliveira MA, Osorio MM, Raposo MC. Socioeconomic and dietary risk factors for anemia in children aged 6 to 59 months. J Pediatr. 2007;83(1):39–46.
Abubakar A, Uriyo J, Msuya SE, Swai M, Stray-Pedersen B. Prevalence and risk factors for poor nutritional status among children in the Kilimanjaro region of Tanzania. Int J Environ Res Public Health. 2012;9(10):3506–18.
Conde-Agudelo A, Rosas-Bermudez A, Castano F, Norton MH. Effects of birth spacing on maternal, perinatal, infant, and child health: a systematic review of causal mechanisms. Stud Fam Plann. 2012;43(2):93–114.
Finlay JE, Ozaltin E, Canning D. The association of maternal age with infant mortality, child anthropometric failure, diarrhoea and anaemia for first births: evidence from 55 low- and middle-income countries. BMJ Open. 2011;1(2):e000226.
Acknowledgements
We thank Dr. Henry Wamani of the Makerere University School of Public Health, who provided us with the equipment, the Makerere University School of Public Health IRB and Namutumba district local government who gave us permission to conduct the study. Special thanks go to care takers who participated and gave their consent for their children to be tested. We would like to appreciate Dr. Fredrick Makumbi of Makerere University School of Public Health, who provided us with statistical advice.
Funding
The research was funded from the authors’ resources. No company/organization contributed any form of funding.
Availability of data and materials
Data is available in the computer readable programmes (Ms Excel 2010).
Authors’ contributions
Contribution: FK initiated the research topic, led the data collection and wrote the first draft of the manuscript. RKW and YA contributed to the design of the study, interpretation and writing of the manuscript. All authors read and approved the final manuscript.
Authors’ information
F. K. is a Graduate Student of Makerere University School of Public Health, College of Health Sciences.
R. K. W. is an Associate Professor in the Makerere University School of Public Health, College of Health Sciences.
Y. A. is a Lecturer in the Medical School in the College of Health Sciences, Makerere University.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Consent for publication of findings was also obtained from mothers of the participating children using the same informed consent form.
Ethics approval and consent to participate
The higher degrees research and ethics committee of the Makerere University School of Public Health and Namutumba District Health Office approved this study.
Written informed consent was obtained from caregivers of participating children. Hb results for all children who participated in the study were given to their caregivers and those with anaemia were referred to the nearest health facility for treatment.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kuziga, F., Adoke, Y. & Wanyenze, R.K. Prevalence and factors associated with anaemia among children aged 6 to 59 months in Namutumba district, Uganda: a cross- sectional study. BMC Pediatr 17, 25 (2017). https://doi.org/10.1186/s12887-017-0782-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-017-0782-3