
Abstract
Background
Morgan and Scheiman’s Optometric Extension Program (OEP) expected binocular vision findings have longstanding use in optometry. With technological advances, the demands and standards of binocular function have changed. This study aimed to investigate which binocular visual functions can effectively predict visual behavior performance.
Methods
Participants aged 15–24 years were recruited from two colleges and two universities. After completing the CSMU-Visual Behavioral Performance questionnaire (CSMU-VBP, with four components: near work, visual perception, visual comfort, and whole-body balance), participants were divided into symptomatic and asymptomatic groups based on questionnaire findings (cutoff: < 12 vs. ≥ 12 symptoms). Then a 24-step binocular visual examination was undertaken. Data were analyzed with one-sample, Student’s, and paired t-tests. Additionally, receiver operating characteristic analysis was used to determine the predictors of binocular visual function required for near work, visual perception, visual comfort, and body balance dimensions.
Results
Among 308 participants, 43 (14%) and 265 (86%) were symptomatic and asymptomatic, respectively. Among the 46 participants with abnormal binocular vision, 36 (78%) reported that they had no obvious symptoms. The commonest dysfunctions were accommodative excess and convergence excess. Most of the binocular visual findings significantly diverged from traditional normal values: amplitude of accommodation, as well as base-in prism to break and recovery points at distance were higher than traditional normal values, whereas others were lower than traditional normal values. Total CSMU-VBP scores indicated that the asymptomatic and symptomatic groups had significant differences in DBO recovery (t = 2.334, p = 0.020) and BAF (t = 1.984, p = 0.048). Receiver operating characteristic curve analysis yielded the following binocular visual functional cutoff points: near work (DBO blur < 7, DBO recovery < 5.5), visual perception (MAF < 10.5, BAF < 10.25), visual comfort (DLP < − 2.25, DBI break > 11.5, NBI blur > 15, NBI break > 17.5, NBI recovery > 13, NPC < 5.75), and body balance (NFD_H > − 0.5, gradient AC/A [minus] > 2.25, NPC < 4.75).
Conclusions
The mean values of binocular visual function among young Taiwanese adults were statistically different from traditional normative values. Further research is required to confirm whether these findings reflect impaired binocular vision or stringent criteria. Assessments of binocular visual function, especially binocular accommodation sensitivity, are crucial in routine optometric examination.
Similar content being viewed by others


Introduction
In the context of normal eye structure, the ability to combine evaluations of binocular vision, large visual field overlap, and retinal cell potential with comprehensive brain analysis has optimized imaging resolution, facilitating the ability to perceive three-dimensional visuospatial and stereoptic information for further assessing (and potentially enhancing) fine motor coordination and manipulation abilities [1,2,3]. Binocular visual dysfunction can be associated with many symptoms, such as blurred vision, headache, eye strain or discomfort, intermittent diplopia, inattention, eye rubbing, excessive blinking, and photophobia [4,5,6,7,8,9]. Such dysfunction and symptomatology can lead to abnormal visual behavior performance, such as reading with finger assistance, skipping or missing, letter reversal, or lack of interest in near vision. Moreover, binocular visual problems may lead to other related physiological or perceptual problems, including issues with peripheral perception [10], athletic ability [11], visuospatial discernment, and sense of direction [12]. In the study reported herein, we defined visual behavior performance as near work, visual perception, visual comfort, and body balance.
The standards and expected values of Morgan and Scheiman’s Optometric Extension Program (OEP) [1, 13], which are frequently cited in clinical binocular vision examinations in optometry, have been well established since 1944. Over time, with scientific and technological advancements, habits and functional demands associated with vision have changed. Additionally, in light of genetic and regional variations, the suitability of these standards values requires re-evaluation [14,15,16,17,18,19,20]. Age is an important factor that affects binocular vision, including the elements of contrast sensitivity [21], visual acuity [22], accommodation [23], and vergence [24,25,26]. Furthermore, aging reduces the amplitude and time of vergence peak velocity [27] and phoria adaptation [28]; such changes are often detected in patients with binocular dysfunction, especially in patients with convergence insufficiency [29,30,31,32]. However, the Morgan and Scheiman OEP standards were not established with age-specific considerations.
Besides age, optometrists should pay attention to the correlations between visual function, brain injury [33], dry eye [34,35,36], migraines [37], sleep disturbance [38, 39], dyslexia [40], inattention [41, 42], work in high-tech industries [43], and athletic activity [44]. Moreover, with the emergence of virtual reality technology in recent years, associated problems with motion sickness are yet unsolved; this has been shown to be associated with binocular vision problems, but to our knowledge, no published studies have investigated this problem in Taiwan among Taiwanese populations [14]. Therefore, the application of traditional standards for related clinical diagnoses in Taiwan may be problematic. This study investigated binocular visual function among young adults in Taiwan and compared the findings with traditional standard values. Furthermore, the study aimed to further analyze binocular visual function tests to determine accurate standard requirements for different visual tasks.
Materials and methods
This cross-sectional study was conducted from November 18, 2019, to May 30, 2020. The study protocol was reviewed and approved by the institutional review board of Chung Shan Medical University Hospital (approval no. CS19110). Additionally, the study strictly adhered to the principles of research ethics specified in the Declaration of Helsinki and its later amendments, and this article followed the STROBE guidelines [45].
Participants
Non-probability and convenience sampling techniques were used, and study participants were recruited from two colleges and two universities. According to information from the Taiwan Ministry of Education, 98.94% of young people in Taiwan are studying in colleges and universities, that is, most Taiwanese youths and young adults, aged 15–24, are college and university students. A total of 327 young individuals, aged 15 to 24 years, consented to participate. The exclusion criteria were as follows: refractive errors of sphere ≤ − 6.00 D or > + 1.00 D; astigmatism ≤ − 1.00 D; long-term use of contact lenses; previous eye or brain surgery; and ophthalmic, metabolic, immune, physiological, or psychological diseases. Additionally, patients with severe visual complaints which had great influence on their quality of life were also excluded. All participants were confirmed to be healthy through objective and subjective screening procedures. Among those who consented to participate, 10 had incomplete questionnaires and eye examinations, five had best corrected visual acuity ratios ≤ 1.0, one had Ménière's disease, one had Tourette's disease, one had amblyopia, and one had strabismus, and the final analysis included 308 participants. The Kolmogorov–Smirnov test revealed that the participants’ spherical equivalent power data were under normally distributed (right eye: D = 0.068, p = 0.148; left eye: D = 0.062, p = 0.236). The participants’ characteristics are summarized in Table 1.
Research materials
The assessment procedures used in this study were non-invasive, non–risk-conferring, and involved no drug administration. Accordingly, the research tools and examination items were divided into two parts:
Binocular visual function examination
To ensure accurate measurement results, possible confounding factors, such as laboratory brightness, visual target distance, and subjective differences in measurement tools and equipment operators, were controlled. Additionally, to avoid any potential sources of bias, each test was performed by the same optometrist. The binocular visual function examination and materials included:
-
a.
Refraction: Shin-NiPon Openfield Refraction (Tokyo, Japan)
-
b.
Subjective refraction: Topcon Manual Phoropter VT-10(Tokyo, Japan)
-
c.
Distance visual acuity and distance vergence range: Digital Chart System VM-VLC-1900
-
d.
Near visual acuity and near vergence range, negative relative accommodation (NRA), and positive relative ac-commodation (PRA): TMVC Near Point Test Card, plus lens power is added binocularly, 0.25D at a time.
-
e.
Horizontal and vertical phoria: Von Graefe, Risley rotating prisms on phoropter.
-
f.
Accommodation amplitude (AA): Donder’s push-up method with the RAF near point ruler
-
g.
Monocular and binocular accommodation facility (MAF, BAF), convergence facility, near-fixation disparity (NFD): ± 2.00 D flippers for accommodation, 8BI/8BO flippers for vergence, and the Saladin near point balance card
-
h.
near-point convergence (NPC), near-point accommodation (NPA): Royal Air Force(RAF) ruler with a vertical line target.
-
i.
Fusional vergence range: Risley rotating prisms on phoropter; Fusional vergence facility: 12 PD base-out and 3 PD base-in flipper performed at 40 cm.
Visual behavior performance questionnaire
Notably, most questionnaires used to investigate or query binocular function focus on near work or visual symptoms, and few such questionnaires have focused on visual behavior indicators, such as visual perception, walking posture, or balance. The CSMU-Visual Behavioral Performance questionnaire (CSMU-VBP) was developed by this study’s investigators and was based on the convergence insufficiency symptom survey(CISS) [46], college of optometrists in vision development quality of life checklist (COVD-QoL) [47], and the students' visual status questionnaires [48]. The content of CSMU-VBP(48 questions) was screened and analyzed by Analytical Hierarchy Process(AHP) by three optometric experts, and has been widely used in binocular vision and visual training research in Taiwan [49,50,51,52]. Factor analysis divided the questionnaire (overall Cronbach's alpha = 0.851) into four dimensions (each question may be calculated repeatedly), with 25 questions pertaining to near-vision work (Cronbach's alpha = 0.837), 20 on perception (Cronbach's alpha = 0.780), 14 on comfort (Cronbach's alpha = 0.705), and 12 on postural balance (Cronbach's alpha = 0.775) [49].
According to CSMU-VBP responses, participants were divided into the asymptomatic (good visual performance, total score < 12) and symptomatic (poor visual performance, total score ≥ 12) groups by using the lowest quartile as the cutoff criterion [53]. Logistic regression analysis indicated that the accuracy of all binocular visual function examinations in predicting symptomatic or asymptomatic partcipatns (according to questionnaire responses) was as high as 86.4%, especially with regard to NLP (exp(β) = 1.102, p = 0.040), DBI recovery (exp(β) = 1.287, p = 0.025), BAF (exp(β) = 0.853, p = 0.032), and AA (exp(β) = 1.129, p = 0.025) [49].
Data and statistical analysis
One-sample, Student’s, and paired t-tests, the Kolmogorov–Smirnov test, logistic regression analysis, and receiver operating characteristic (ROC) curve analysis were performed, and data were analyzed using SPSS Statistics for Windows, version 26.0 (Armonk, NY, USA); a p-value < 0.05 was considered statistically significant.
Results
Of 308 participants, 83 were males, and 225 were females. The mean age was 18.7 ± 1.7 years. There was no significant difference between the gender in terms of spherical equivalent power (male: − 3.47 ± 2.51 D, female: − 3.25 ± 2.59 D; t = 0.766, p = 0.444); therefore, differences between the gender were not analyzed further.
Among the 308 participants, 43 (14%) were classified as symptomatic, and the remaining 265 (86%) were asymptomatic. There was no significant difference between the symptomatic and asymptomatic groups in terms spherical equivalent power according to eye laterality (right eye: t = 0.775, p = 0.439; left eye: t = 1.095, p = 0.274). There was also no significant difference between the left and right eyes in terms of spherical equivalent power according to stud group (total: t = − 0.935, p = 0.351; symptomatic: t = 0.746, p = 0.460; asymptomatic: t = − 1.406, p = 0.161). The total CSMU-VBP score (t = − 21.659, p = 0.001), near work (t = − 20.337, p = 0.001), perception (t = − 11.038, p = 0.001), comfort (t = − 10.193, p = 0.001), and body balance (t = − 7.592, p = 0.001) dimensions yielded significant differences between the symptomatic and asymptomatic groups (Table 1).
Binocular visual function and visual behavior performance in young Taiwanese adults
According to Scheiman and Wick’s criteria [1], the proportion of normal binocular vision in this study was ascertained to be 85% (n = 262), and the frequency of abnormal accommodation and convergence was 15% (n = 46). Among all the participants, 20 only had accommodation dysfunction (AD, 6.5%), among whom excessive accommodation was the commonest problem (n = 13, 4.2%). Twenty-three participants only had vergence dysfunction (VD, 7.5%), among whom excessive convergence was the commonest problem (n = 12, 3.9%). Three participants simultaneously had AD and VD (1%; Table 2 and Fig. 1).

Frequency of Scheiman and Wick’s criteria and CSMU-VBP
Among the 46 participants with abnormal binocular visual function, 78% (36 participants) reported that they had no obvious symptoms (Table 2), three had exophoria, four had esophoria, and three had abnormal accommodation and vergence. Half of the participants with impaired accommodative facility or convergence-insufficient cohesion had symptoms. In particular, among the 262 participants with normal binocular visual function that were classified according to traditional diagnostic criteria, 33 (12.6%) had visual complaints, and only 10 (21.7%) of the 46 participants with abnormal visual function complained of poor visual behavior performance, indicating that the patients who reported that they had visual behavior problems may not have had binocular visual problems (Fig. 1). Due to the fact that different types of visual work require different binocular visual functions; the clinical characteristics and Scheiman and Wick's diagnostic criteria for binocular visual dysfunction can be further considered.
Comparison of binocular visual function values of Morgan and Scheiman’s OEP
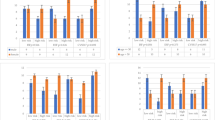
The mean values of distance phoria; near phoria; gradient AC/A plus and minus; DBI break and recovery; DBO blur, break, and recovery; NBI blur, break, and recovery; NPC, MAF, BAF, NRA, PRA, and AA, all diverged significantly from the Morgan and Scheiman standards. In particular, the mean values of DBI break, recovery, and AA were all higher than the Morgan and Scheiman standard, and the remainder of the assessed criteria were lower than the standard values.
Compared with the expected OEP values, except for DBO blur, there were statistically significant differences in distance phoria, near phoria, DBI break and recovery, DBO break and recovery, NBI blur, break, and recovery, as well as NRA and PRA. Among the investigated variables with significant differences (except for DBI break, which yielded a higher mean value than the expected OEP value), the mean values of the rest of the items were lower than the expected values (Table 3).
Although the mean binocular visual function assessment values for young people in Taiwan were lower than the traditional standard values, in fact, the proportion of participants expressing distress or disturbance was low (21.7%). Furthermore, it should be noted that the standard deviations were quite large, reflecting heterogeneity among participants; therefore, variations in visual habits or visual demands might be an interesting topic for further research. Additionally, the results can be interpreted as reflecting a lower demand for binocular vision in visual work due to improved clarity of printed materials, the evolution of accessibility interfaces for 3C products, or the development of diversified sports and games. Future research should determine whether these differences resulted from binocular visual impairment or lower demand for binocular vision, with emphasis on applicability in clinical settings.
Cutoff criteria of binocular visual functions for different visual tasks
In this study, the four dimensions of the visual behavior performance, namely, (1) near work, (2) perception, (3) comfort, and (4) physical balance, were scored according to quartiles. The first (lowest) quartile represented the 25th percentile of the data. This analysis was conducted to identify the presence or absence of symptoms. According to the different dimensions, participants were divided into the asymptomatic and symptomatic groups. Previous studies have confirmed that with this classification method, through t-test and logistic regression analysis, the questionnaire scores of each visual task can effectively predict the problems associated with binocular vision, and they can also have a significant amount of explained variance [49]. Next, the results of the binocular visual function testing were analyzed by using ROC curve analysis to identify the binocular vision appraisal items and standards for different visual tasks.
In terms of the mean total CSMU-VBP scores, t-test analysis on binocular visual functions revealed DBO recovery and BAF to be significantly different between the asymptomatic and symptomatic groups (Table 4). In the ROC curve analysis of the total scale, the base-out recovery (AUC = 0.619, p = 0.018) and binocular accommodative facilities (AUC = 0.588, p = 0. 605) could significantly identify visual behavior performance of the participants. The cutoff value of base-out recovery was 5.5 PD (sensitivity = 0.605, specificity = 0.606; Morgan and Scheiman and OEP standard both 10 PD). The cutoff value of binocular accommodative facility was 10.25 cpm (sensitivity = 0.588, specificity = 0.605; Scheiman standard = 10 cpm). The t-test and ROC analysis results were consistent with one another.
Near work
In the ROC curve analysis of the near-work dimension, the cutoff point for DBO blur (AUC = 0.598, p = 0.028) was 7 degrees (sensitivity = 0.74, specificity = 0.471; Morgan and Scheiman standard = 9). The cutoff point for DBO recovery (AUC = 0.591, p = 0.052) was 5.5 degrees (sensitivity = 0.543, specificity = 0.601; Morgan and Scheiman standard = 10 PD). Poor ability to revert to fusion was more likely to cause complaints about near work. This was similar to the criterion of pure exophoria (5 degrees) in the Scheiman binocular visual dysfunction diagnostic criteria. Therefore, these two functions should have considerable discriminative power when used to predict the conscious performance of the near-work dimension (Table 5).
Perceptual
In the ROC curve analysis of the perceptual dimension (Table 5 right), the cutoff point for MAF (AUC = 0.583, p = 0.088) was 10.5 cpm (sensitivity = 0.756, specificity = 0.419; Scheiman criterion = 11 cpm). The cutoff for BAF (AUC = 0.621, p = 0.012) was 10.25 cpm (sensitivity = 0.70, specificity = 0.481; Scheiman standard = 10 cpm). Individuals with good monocular and binocular accommodation ability can switch between binocular distance and near vision with high levels of smoothness and comfort, and their vision is more stable and not too strained. Such individuals can focus more on cognition and learning [54, 55]. In contrast, individuals with poor binocular accommodation facilities find it very difficult and experience unstable vision when looking at objects of varying distances, with excessive mental effort needed to adjust vision; thus, they find it difficult to focus their working attention; moreover, they experience much difficulty not only in three-dimensional perception [56], but also in visual recognition and comprehension [57]. The cutoff point (10.25 cpm) analyzed in this study is close to the traditional standard value (10 cpm); therefore, MAF and BAF functions can be used to predict the perception dimension, and conscious performance should have facilitated considerable discrimination.
Comfort
In the ROC curve analysis of comfort (Table 6), the cutoff point for DLP (AUC = 0.567, p = 0.050) was 2.25 PD of exophoria (sensitivity = 0.459, specificity = 0.673; Morgan and Scheiman criterion = 1 PD of exophoria; OEP standard = 0.5 PD of exophoria). The cutoff point for DBI break (AUC = 0.574, p = 0.031) was 11.5 PD (sensitivity = 0.593, specificity = 0.563; Morgan and Scheiman standard = 7 PD; OEP standard = 9 PD). The cutoff for NBI blur (AUC = 0.561, p = 0.039) was 15 PD (sensitivity degree = 0.229, specificity = 0.884; Morgan and Scheiman standard = 13 PD; OEP standard = 14 PD). For NBI break (AUC = 0.585, p = 0.014), the cutoff was 17.5 PD (sensitivity = 0.697, specificity = 0.449; Morgan and Scheiman standard = 21 PD; OEP standard = 22 PD). The cutoff value for NBI recovery (AUC = 0.581, p = 0.019) was 13 PD (sensitivity = 0.422, specificity = 0.717; Morgan and Scheiman standard = 13 PD; OEP criteria = 18 PD). For NPC, the cutoff point 5.75 cm (AUC = 0.570, p = 0.042, sensitivity = 0.679, specificity = 0.452; Scheiman standard = 5 cm). The six above-mentioned binocular vision criteria can significantly identify the comfort dimension with regard to an easy starting point and appropriate convergence and divergence abilities, both in terms of far and near vision. This can allow the eyes to easily relax and retract [58,59,60]. Therefore, these six binocular visual function items can be used to predict the conscious performance of the comfort dimension with considerable discriminating power.
Balance
In the ROC curve analysis of the balance dimension (Table 6), the cutoff point for NFD (AUC = 0.629, p = 0.005) was 0.5 PD of exotropic shift (sensitivity = 0.809, specificity = 0.368; the standard value of an optometry practical textbook is ortho). The cutoff point for the negative gradient AC/A was 2.25△/D (AUC = 0.590, p = 0.050; sensitivity = 0.652, specificity = 0.558; Morgan and Scheiman criterion = 4Δ/D; OEP criterion = 4Δ/D). For NPC (AUC = 0.584, p = 0.033), the cutoff was 4.75 cm (sensitivity = 0.596, specificity = 0.591; Scheiman standard = 5 cm). NFD represents the accuracy and stability of near gaze. The standard (0.5 PD exotropic shift) analyzed in this study was similar to the standard value (ortho) specified in an optometry clinical practice textbook. The results indicated that the deviation of NFD was higher than 0.5 exotropic PD when the direction of the esotropic NDF increased, and balance-related complaints increased simultaneously [61]. Gradient AC/A (negative) indicates that convergence will be generated under the stimulation of 1D accommodation. The cutoff node (2.25△/D) analyzed in the study was 1.75△/D less than the traditional standard value (4△/D), which means that as long as the gradient AC/A (negative) ratio of the subject exceeds 2.25△/D, there will be significant complaints about balance-related symptoms [62]; the converging near point represents the maximum amplitude that can be converged [63], and the cutoff point (4.75 cm) determined by this study was close to the Scheiman standard value of 5 cm, which means that the convergence point is related to postural balance [62]. Postural balance ability correlated with NFD, negative gradient AC/A, and NPC.
Discussion
According to the analysis of the results of the binocular visual function examination in this study, the proportion of accommodation excess and convergence excess among young adults in this study were the highest, which is similar to the results reported elsewhere [64,65,66,67]. However, the findings of this study are very different from those of most previous studies with regard to accommodation and convergence insufficiency [9, 68, 69]. Previous research has suggested that long-term use of 3C products at close visual range [70,71,72,73] results in myopia and an inability to relax accommodation and convergence; this might reasonably to explain the diagnoses of accommodation and convergence excesses in Taiwanese youths [67, 74]. However, the classical diagnostic criteria for the clinical assessment and classification of abnormal binocular visual function are nearly 80 years old, and many reports have confirmed race- and age-specific observations [15, 16, 18, 20, 75,76,77,78]; therefore, the diagnostic criteria for binocular vision dysfunction should be re-evaluated [16,17,18,19].
The binocular visual functional outcome values of young Taiwanese diverged from the standard values that are often referred to in clinical practice, and the actual values were mostly lower than the standard values. Except for established ethnic differences and age differences [15, 16, 18, 20, 75,76,77,78], most of the differences from standard values did not take refractive errors, visual demands, and technological developments into consideration [79,80,81]. Although it might not confer reading difficulties [82,83,84] when the accommodation range and the DBI break are both relatively high, overuse of near vision as well as excessive use of accommodation and cohesion, resulting in functional fatigue or rigidity, may lead to poor overall binocular visual performance (Fig. 2). Regardless of the study findings, it can be confirmed that the development of new Taiwanese binocular vision standard values should constitute a direction for future research.

Binocular visual relationship diagram related to various visual tasks
In this study, ROC curve analysis was used to identify standard binocular vision criterion values for different visual behavior performance dimensions. When patients have visual disturbances, the visual behavior scale questionnaire can be used to distinguish between different categories of patients. After identification of the type of visual disturbance in each dimension, binocular vision inspection items can be used to discriminate each dimension to determine whether measured and calculated values meet diagnostic criteria (cutoff points). Next, the values thus obtained can be used to adjust prescriptions or vision training [85,86,87,88] to help patients resolve or manage their visual problems. For example, the patient fills in the CSMU-Visual Behavioral Performance questionnaire, and the score in the perception dimension is 7 points (≥ 5 is symptomatic), which reflects perceptual visual disturbance. The results of monocular and binocular accommodation evaluations are 8 and 7 cpm, respectively (lower than the cutoffs for MAF [< 10.5 cpm] and BAF [< 10.25 cpm]). The examiner can preliminarily determine that the patient has abnormal function in monocular and binocular accommodation. By improving binocular visual function, the perceptual ability can also be improved simultaneously. Figure 2 is a simplified representative diagram, which indicates that different visual tasks correlated with different binocular visual functions [89].
Comparing Tables 3 and 4, it can be found that although DBO recovery and BAF were significantly different between the asymptomatic and symptomatic groups, the DBO recovery values of the two groups were both lower than the standard value. In contrast, the BAF performance of all participants was not significantly different from the standard value, but there was a significant difference between the two groups, which indicates that BAF is the most important indicator for clinical diagnosis.
In summary (Fig. 2), a high frequency of near work among Taiwanese young adults has increased the values for the following variables: accommodation range (AA↑), near point of convergence (NPC↑), distance-near convergence ability (BO↑), and binocular accommodation facility (BAF↑). However, excessive near work and related habits leads to excessive accommodation and convergence, which leaves individuals exhausted and fatigued, unable to relax, resulting in poor binocular visual function. Therefore, such people will have more visual disturbance–related complaints than those who do not meet the standard values for accommodation and convergence. If the starting point of eye positioning is close to ortho (DLPΦ) at distance, the endpoints of near fixation disparity close to exotropia (NFD↓), good binocular accommodation facility (BAF↑), and visual behavior disturbance symptoms will be naturally better.
Conclusions
The average binocular visual function of young people in Taiwan is worse than that which would be expected according to traditional reference values. When using the traditional binocular visual function classification criteria, nearly 80% of the patients diagnosed with binocular vision abnormality have no obvious symptoms. Visual habits and demands vary with technological and scientific advancements over time and with racial differences. Moreover, future research should focus on related topics regarding the development of human interface technology products, as well as whether these findings reflect binocular vision abilities or demands. Binocular visual functions, especially binocular accommodation sensitivity, should be part of routine optometric examinations to ascertain patients' visual behavior performance.
Finally, this study analyzed the binocular visual function of Taiwanese youths based on questionnaires and binocular vision examinations; however, there are some limitations owing to the large difference in the proportion of male and female participants in this study, as well as the validity and application of the CSMU-VBP questionnaire in clinical practice.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files. Correspondence and requests for materials should be addressed to C.-Y.C.
References
Scheiman M, Wick B. Clinical management of binocular vision: heterophoric, accommodative, and eye movement disorders: Lippincott Williams & Wilkins; 2008.
Jones RK, Lee DN. Why two eyes are better than one: the two views of binocular vision. J Exp Psychol Hum Percept Perform. 1981;7(1):30.
Sheedy JE, Bailey IL, Buri M, Bass E. Binocular vs. monocular task performance. Optometry and Vision Science. 1986;63(10):839–46.
Borsting E, Rouse MW, Deland PN, Hovett S, Kimura D, Park M, et al. Association of symptoms and convergence and accommodative insufficiency in school-age children. Optometry (St Louis, Mo). 2003;74(1):25.
Letourneau J, Ducic S. Prevalence of convergence insufficiency among elementary school children. Can J Optom. 1988;50:194–7.
Rouse MW, Hyman L, Hussein M, Solan H. Frequency of convergence insufficiency in optometry clinic settings. Convergence Insufficiency and Reading Study (CIRS) Group. Optom Vis Sci. 1998;75(2):88–96.
Ciuffreda KJ, Scheiman M, Ong E, Rosenfield M, Solan HA, Ciuffreda KJ. Irlen lenses do not improve accommodative accuracy at near. Optom Vis Sci. 1997;74(5):298–302.
Sterner B, Abrahamsson M, Sjöström A. Accommodative facility training with a long term follow up in a sample of school aged children showing accommodative dysfunction. Doc Ophthalmol. 1999;99(1):93–101.
Dwyer P. The prevalence of vergence accommodation disorders in a school-age population. Clin Exp Optom. 1992;75(1):10–8.
Francis EL, Owens DA. The accuracy of binocular vergence for peripheral stimuli. Vision Res. 1983;23(1):13–9.
Erickson GB. Sports vision: vision care for the enhancement of sports performance: Elsevier Health Sciences. 2007.
Kaplan M. Seeing through new eyes: Changing the lives of children with autism. Asperger syndrome and other developmental disabilities through vision therapy: Jessica Kingsley Publishers; 2005.
Morgan MW Jr. The clinical aspects of accommodation and convergence. Optom Vis Sci. 1944;21(8):301–13.
Chan, IC. Establishing the ocular movement model by using ReadAlyzer of elementary school students in Taiwan. 2013, Master's thesis, Department of biomedical science, Chung Shan Medical University.https://doi.org/10.6834/CSMU.2013. 00068
Yekta A, Khabazkhoob M, Hashemi H, Ostadimoghaddam H, Ghasemi-Moghaddam S, Heravian J, et al. Binocular and accommodative characteristics in a normal population. Strabismus. 2017;25(1):5–11.
Jimenez R, Pérez M, Garcia J, González MD. Statistical normal values of visual parameters that characterize binocular function in children. Ophthalmic Physiol Opt. 2004;24(6):528–42.
Chen AH, Abidin AHZ. Vergence and accommodation system in Malay primary school children. The Malaysian journal of medical sciences: MJMS. 2002;9(1):9.
Álvarez CP, Puell MC, Sánchez-Ramos C, Villena C. Normal values of distance heterophoria and fusional vergence ranges and effects of age. Graefes Arch Clin Exp Ophthalmol. 2006;244(7):821–4.
Lyon DW, Goss DA, Horner D, Downey JP, Rainey B. Normative data for modified Thorington phorias and prism bar vergences from the Benton-IU study. Optometry. 2005;76(10):593–9.
Wajuihian SO. Normative values for clinical measures used to classify accommodative and vergence anomalies in a sample of high school children in South Africa. Journal of optometry. 2019;12(3):143–60.
Owsley C. Aging and vision. Vision Res. 2011;51(13):1610–22.
Chou R, Dana T, Bougatsos C. Screening older adults for impaired visual acuity: a review of the evidence for the US preventive services task force. Ann Intern Med. 2009;151(1):44–58.
Polat U, Schor C, Tong J-L, Zomet A, Lev M, Yehezkel O, et al. Training the brain to overcome the effect of aging on the human eye. Sci Rep. 2012;2(1):1–6.
Maxwell J, Tong J, Schor CM. The first and second order dynamics of accommodative convergence and disparity convergence. Vision Res. 2010;50(17):1728–39.
Semmlow JL, Hung GK. Binocular interactions of vergence components. Am J Optom Physiol Opt. 1980;57(9):559–65.
Yuan W, Semmlow JL, Alvarez TL, Munoz P. Dynamics of the disparity vergence step response: a model-based analysis. IEEE Trans Biomed Eng. 1999;46(10):1191–8.
Rambold H, Neumann G, Sander T, Helmchen C. Age-related changes of vergence under natural viewing conditions. Neurobiol Aging. 2006;27(1):163–72.
Winn B, Gilmartin B, Sculfor DL, Bamford JC. Vergence adaptation and senescence. Optom Vis Sci. 1994;71(12):797–800.
Brautaset R, Jennings J. Distance vergence adaptation is abnormal in subjects with convergence insufficiency. Ophthalmic Physiol Opt. 2005;25(3):211–4.
Erkelens IM, Thompson B, Bobier WR. Unmasking the linear behaviour of slow motor adaptation to prolonged convergence. Eur J Neurosci. 2016;43(12):1553–60.
Sreenivasan V, Bobier WR. Increased onset of vergence adaptation reduces excessive accommodation during the orthoptic treatment of convergence insufficiency. Vision Res. 2015;111:105–13.
Sreenivasan V, Irving EL, Bobier WR. Binocular adaptation to near addition lenses in emmetropic adults. Vision Res. 2008;48(10):1262–9.
Conrad JS, Mitchell GL, Kulp MT. Vision therapy for binocular dysfunction post brain injury. Optom Vis Sci. 2017;94(1):101–7.
Rueff EM, Sinnott LT, Bailey MD, King-Smith PE. The similarity between symptoms of binocular vision disorders and dry eye. Investigative Ophthalmology & Visual Science. 2014;55(13):1990-.
Rueff EM, King-Smith PE, Bailey MD. Can binocular vision disorders contribute to contact lens discomfort? Optom Vis Sci. 2015;92(9):e214–21.
Talens-Estarelles C, Cerviño A, García-Lázaro S, Fogelton A, Sheppard A, Wolffsohn JS. The effects of breaks on digital eye strain, dry eye and binocular vision: Testing the 20–20–20 rule Cont Lens Anterior Eye. 2022;101744. https://doi.org/10.1016/j.clae.2022.101744.
Harle DE, Shepherd AJ, Evans BJ. Visual stimuli are common triggers of migraine and are associated with pattern glare. Headache. 2006;46(9):1431–40.
Horne J. Binocular convergence in man during total sleep deprivation. Biol Psychol. 1975;3(4):309–19.
Stone LS, Tyson TL, Cravalho PF, Feick NH, Flynn-Evans EE. Distinct pattern of oculomotor impairment associated with acute sleep loss and circadian misalignment. J Physiol. 2019;597(17):4643–60.
Tseng SY, Cheng CY, Chang YS. Vision disorders interfering with children’s reading and learning: the importance of diagnosis and treatment. Special Education Quarterly. 2010;114:10–5.
Lee SH, Moon B-Y, Cho HG. Improvement of vergence movements by vision therapy decreases K-ARS scores of symptomatic ADHD children. J Phys Ther Sci. 2014;26(2):223–7.
Redondo B, Vera J, Molina R, García JA, Ouadi M, Muñoz-Hoyos A, et al. Attention-deficit/hyperactivity disorder children exhibit an impaired accommodative response. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):1023–30.
Wolffsohn JS, Sheppard AL, Vakani S, Davies LN. Accommodative amplitude required for sustained near work. Ophthalmic Physiol Opt. 2011;31(5):480–6.
Patti Andrich O, Royalton N, Motz OVA. Article 4 Comparison of Three Types of Vision Therapy Exercises on Visual Skills of Sports Performance.
Sunjic-Alic, A.; Zebenholzer, K.; Gall, W. Reporting of Studies Conducted on Austrian Claims Data. Stud. Health Technol. Inform. 2021, 279, 62–69. https://pubmed.ncbi.nlm.nih.gov/33965920/. (Accessed on 20 Dec 2021). Available online
Borsting E, Mitchell GL, Kulp MT, Scheiman M, Amster DM, Cotter S, et al. Improvement in academic behaviors following successful treatment of convergence insufficiency. Optom Vis Sci. 2012;89(1):12.
Maples W. Test-retest reliability of the college of optometrists in vision development quality of life outcomes assessment. Optometry (St Louis, Mo). 2000;71(9):579–85.
Wang CY. Visual Complications Associated with Topical Cycloplegic in Elementary School Students in Taiwan: An Example of Tamsui Distrct. 2014, Master's thesis, Department of biomedical science, Chung Shan Medical Univesity. DOI: https://doi.org/10.6834/CSMU.2014.00009.
Zhong XY. Correlation between Binocular Vision and Visual Behavioral Performance in Taiwan Non-Presbyopic Adults. 2020, Master's thesis, Department of Optometry, Chung Shan Medical Univesity.
Chen JT. Correlation Between Binocular Visual Functions, Visual Perception and Motion Sickness: Blue Filter Lenses Intervention on Visual Perception on Patients with Motion Sickness. 2022 Unpublished master’s thesis, Department of Optometry, Chung Shan Medical University
Huang, HY. Yellow filter intervention of binocular vision, visual perception and reading efficiency on young adults. 2022 Unpublished master’s thesis, Department of Optometry, Chung Shan Medical University
Chen ST, Tung HC, Chen YT, et al. The influence of contact lenses with different optical designs on the binocular vision and visual behavior of young adults. Sci Rep. 2022;12:6573. https://doi.org/10.1038/s41598-022-10580-7.
Lezak, MD., Howieson, DB., Loring, DW., Hannay, HJ., Fischer, JS. Neuro- psychological Assessment, 4th ed. Oxford University Press, 2004.
Dusek WA, Pierscionek BK, McClelland JF. An evaluation of clinical treatment of convergence insufficiency for children with reading difficulties. BMC Ophthalmol. 2011;11(1):21.
Palomo-Álvarez C, Puell MC. Accommodative function in school children with reading difficulties. Graefes Arch Clin Exp Ophthalmol. 2008;246(12):1769–74.
Garzia R, Nicholson S. A study of binocular accommodative and vergence facility and predictive analysis of global stereopsis. J Behav Optom. 1991;2:3–6.
Evans BJ, Drasdo N, Richards IL. Investigation of accommodative and binocular function in dyslexia. Ophthalmic Physiol Opt. 1994;14(1):5–19.
Owens DA, Tyrrell R. Lateral phoria at distance: contributions of accommodation. Invest Ophthalmol Vis Sci. 1992;33(9):2733–43.
Mahto R. Eye strain from convergence insufficiency. Br Med J. 1972;2(5813):564–5.
Gur S, Ron S, Heicklen-Klein A. Objective evaluation of visual fatigue in VDU workers. Occup Med. 1994;44(4):201–4.
Ogle KN. Fixation disparity and oculomotor imbalance. American Orthoptic Journal. 1958;8(1):21–36.
Dusek W, Pierscionek BK, McClelland JF. A survey of visual function in an Austrian population of school-age children with reading and writing difficulties. BMC Ophthalmol. 2010;10(1):16.
Benjamin WJ. Borish's Clinical Refraction-E-Book: Elsevier Health Sciences; 2006.
Abdi S, Rydberg A. Asthenopia in schoolchildren, orthoptic and ophthalmological findings and treatment. Doc Ophthalmol. 2005;111(2):65–72.
Hoseini-Yazdi SH, Yekta A, Nouri H, Heravian J, Ostadimoghaddam H, Khabazkhoob M. Frequency of convergence and accommodative disorders in a clinical population of Mashhad. Iran Strabismus. 2015;23(1):22–9.
Lara F, Cacho P, García Á, Megías R. General binocular disorders: prevalence in a clinic population. Ophthalmic Physiol Opt. 2001;21(1):70–4.
Porcar E, Montalt JC, Pons ÁM, España-Gregori E. Symptomatic accommodative and binocular dysfunctions from the use of flat-panel displays. Int J Ophthalmol. 2018;11(3):501.
Montés-Micó R. Prevalence of general dysfunctions in binocular vision. Ann Ophthalmol. 2001;33(3):205–8.
Daum KM. Accommodative insufficiency. Am J Optom Physiol Opt. 1983;60(5):352–9.
Tsai C-C, Lin SS. Analysis of attitudes toward computer networks and Internet addiction of Taiwanese adolescents. Cyberpsychol Behav. 2001;4(3):373–6.
Yen J-Y, Yen C-F, Chen C-C, Chen S-H, Ko C-H. Family factors of internet addiction and substance use experience in Taiwanese adolescents. Cyberpsychol Behav. 2007;10(3):323–9.
Whang LS-M, Lee S, Chang G. Internet over-users’ psychological profiles: a behavior sampling analysis on internet addiction. Cyberpsychology & Behavior. 2003;6(2):143–50.
Kao, BL. Applying Association Rules to Study the Influence between Self-Control and Internet Addiction through Monitoring 3C Product Mechanism for School Children ─ A Case Study of High Grade Students of an Elementary School in Taipei. 2016, Master's thesis, Department of Digital Technology Design(Master Program in Toy and Game Design, National Taipei University of Education.
Ehrlich DL. Near vision stress: vergence adaptation and accommodative fatigue. Ophthalmic Physiol Opt. 1987;7(4):353–7.
Kragha IK. Accommodative vergence and related findings for a Nigerian population. Ophthalmic Physiol Opt. 1985;5(4):435–9.
Buzzelli AR. Vergence facility: developmental trends in a school age population. Am J Optom Physiol Opt. 1986;63(5):351–5.
Edwards MH, Law LF, Lee CM, Leung KM, Lui WO. Clinical norms for amplitude of accommodation in Chinese. Ophthalmic Physiol Opt. 1993;13(2):199–204.
Chen AH, Abidin AH. Vergence and accommodation system in malay primary school children. Malays J Med Sci. 2002;9(1):9–15.
Lin SK. The correlation between visual fatigue and accommodation system. 2015, Master's thesis, Department of biomedical science, Chung Shan Medical Univesity. https://doi.org/10.6834/CSMU.2015.00126
Chang SC. Correlation between after-school learning and refractive error of elementary school students in Taiwan. 2013, Master's thesis, Department of biomedical science, Chung Shan Medical Univesity
Lin MW. The Intervention of Eye Care Education on Myopia Development and its Effect on Myopic Physiological Factors – a Study in Central Taiwan Schoolchildren. Master’s thesis. Department of biomedical science: Chung Shan Medical Univesity; 2018.
Kapoula Z, Bucci MP, Jurion F, Ayoun J, Afkhami F, Brémond-Gignac D. Evidence for frequent divergence impairment in French dyslexic children: deficit of convergence relaxation or of divergence per se? Graefes Arch Clin Exp Ophthalmol. 2006;245(7):931–6.
Palomo-Álvarez C, Puell MC. Binocular function in school children with reading difficulties. Graefes Arch Clin Exp Ophthalmol. 2010;248(6):885–92.
Wahlberg-Ramsay M, Nordström M, Salkic J, Brautaset R. Evaluation of aspects of binocular vision in children with dyslexia. Strabismus. 2012;20(4):139–44.
Adler P. Efficacy of treatment for convergence insufficiency using vision therapy. Ophthalmic Physiol Opt. 2002;22(6):565–71.
Vasudevan B, Ciuffreda KJ, Ludlam DP. Accommodative training to reduce nearwork-induced transient myopia. Optom Vis Sci. 2009;86(11):1287–94.
Ma MM-L, Scheiman M, Su C, Chen X. Effect of vision therapy on accommodation in myopic Chinese children. Journal of Ophthalmology. 2016;2016.
Rouse MW. Management of binocular anomalies: efficacy of vision therapy in the treatment of accommodative deficiencies. Am J Optom Physiol Opt. 1987;64(6):415–20.
Ansons AM and Davis H. Diagnosis and management of ocular motility disorders (4th Edition). Chichester, West Sussex; Hoboken, New Jersey : Wiley, 2014.
Acknowledgements
Not applicable.
Funding
This research was funded by the Chung Shan Medical University research project (FCU/CSMU 110-003) in Taiwan.
Author information
Authors and Affiliations
Contributions
Conceptualization, C.-Y.C., P.-H.W. and. S.-T.C.; investigation, data curation, and formal analysis, C.-Y.C., P.-H.W., S.-T.C., and X.-Y.Z.; writing—original draft preparation, C.-Y.C. and P.-H.W.; writing—review and editing, C.-Y.C., and K.-C.S. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Chung Shan Medical University Hospital (Taichung, Taiwan) (approval number: CS19110). Informed written consent was obtained from all individual participants included in the study.
Consent for publication
Patients signed informed written consent regarding the publication of their data or photographs.
Competing interests
The authors have no relevant financial or non‐financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
CSMU - Visual Behavioral Performance
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, ST., Su, KC., Wang, PH. et al. Routine binocular examination of young Taiwanese adults as a predictor of visual behavior performance. BMC Ophthalmol 23, 47 (2023). https://doi.org/10.1186/s12886-022-02731-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-022-02731-1