
Abstract
Background
Investigation of the prevalence of climatic droplet keratopathy (CDK) in Tacheng, Xinjiang, China.
Methods
A total of 1030 participants, in their 40s or older, from the Kazakh ethnic group in Tacheng, were randomly sampled by stratification method. Ophthalmic examinations and surveys were carried out on these participants. Factors associated with CDK were analyzed with logistic regression models.
Results
CDK was found in 66 (6.4%; 95% confidence interval [CI]: 4.9–7.9%) Kazakh individuals.
After multiple regression model analysis, it demonstrated that age (< 0.001), exposure time (< 0.001), exposure protection (< 0.001), and vegetable intake (< 0.001) were of correlation with CDK, of which age (OR = 1.21[CI]: 1.16–1.27) and long-term outdoor exposure (OR = 2.42[CI]: 1.26–4.67) were the risk factors, and that vegetable intake (OR = 0.29[CI]: 0.14–0.59) and wearing a hat (OR = 0.24[CI]: 0.10–0.56) were protective factors.
Conclusions
This study has revealed the risk and protective factors of CDK, providing a new insight on related research.
Similar content being viewed by others
Background
Climatic droplet keratopathy (CDK) is also known as the spheroidal keratopathy, Labrador keratopathy, or Bietti’s keratopathy [1,2,3]. CDK is characterized by corneal opacity which results from a increment of oil-like deposits on the anterior elastic lamina and anterior stromal layer [4]. Previous studies have indicated that the prevalence of CDK varies widely in different regions and ethnic groups, with rates as low as 2.7% [5] and as high as 100% [6]. Zhang et al. (1991) reported that in Inner Mongolia, CDK mainly occurs in middle-aged and elderly Mongolians with the prevalence being 8.1% in adults over the age of 30 [7]. Currently, high-quality research in the field of CDK is absent.
Generally, CDK is considered to be a degenerative corneal disease associated with chronic corneal damage. The exact pathogenesis of CDK is still not clear, but there are many risk factors for CDK including: exposure to ultraviolet radiation, aging, dietary habits, and occupational hazards. Among them, ultraviolet radiation is the most widely established factor [1, 8]. Studies have reported that the intensity and time of exposure to ultraviolet radiation correlates significantly to the prevalence of CDK [1].
Currently, there are no specific pharmacological treatments for CDK, but superficial keratectomy along with amniotic membrane transplant or corneal transplantation are available for advanced CDK cases [9]. However, the procedure is not able to be practiced in several impoverished regions. The epidemiology and pathogenesis of CDK gain little attention because only a few patients seek medical assistance due to its mild symptoms in the early stage [1].
In our clinical work in Tacheng, CDK can only be found among middle-aged and elderly Kazakhs, especially those who have been farming or herding outdoors for many years. The main focus of this study was to identify the most important factors influencing CDK, thus boosting early detection and intervention. To the best of our knowledge, no study has been conducted to investigate the prevalence of CDK among the Kazakh ethnic group in Xinjiang. This study reports the prevalence of CDK and its associated risk factors in the Kazakh ethnic group in Tacheng, Xinjiang, and reviews existing literature on the prevalence of CDK.
Methods
Sampling
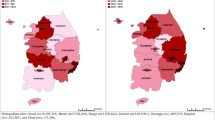
Tacheng prefecture (longitude 82° 16′- 87° 21′, east; latitude 43 25′- 47 ° 15′, north) (Fig. 1) is in the Northwestern part of Xinjiang Uyghur Autonomous Region, China. It has an area of 98824km2, and is divided into two county-level cities (Tacheng and Usu), four counties (Emin County, Shawan County, Toli County, and Yumin County), and an autonomous county (Hoboksar Mongol Autonomous County).

The map of China highlighting site of this work (Tacheng prefecture) (Artificial drawing created by author ZXH)
Sample size was calculated with the cross-sectional study formula \( N=\frac{z_{1-\raisebox{1ex}{$a$}\!\left/ \!\raisebox{-1ex}{$2$}\right.}^2p\left(1-p\right)}{d^2} \), where Z1-α/2 = 1.96. As α = 0.05, p stands for the prevalence of CDK (which was 5.0% in our pretest), and d is admissible error (which is 2%). According to the formula, the theoretical sample size was 502, which includes an extra 10% for subject’s loss.
We have randomly selected 7 different townships in different cities and counties. The final selection was made by assigning each township with a number and use a random number generator from WinPepi to select numbers within the range of the township list. A public hospital was chosen in each township for participants examination.
The study included only Kazakh residents who had lived in the area for more than 5 years and aged 40 years or above. Monocular patients were excluded. In addition, the study also excluded patients with a history of ocular surgery or ocular trauma and other diseases such as mental illness which could potentially affect the evaluation of CDK. The study was based on the principles of the Declaration of Helsinki. Ethical approval was granted by the bioethical committee of the Ninth Division Hospital of Xinjiang Production and Construction Corps.
Data collection
Data was collected from September 2019 to December 2019 by a team of ophthalmologists and other medical staff from The Ninth Division Hospital of Xinjiang Production and Construction Corps. During the data collection process, each participant underwent a comprehensive interview by trained interviewers.
The questionnaire comprised basic personal information, lifestyle habits, and medical history. Basic personal information included name, age, gender, ethnicity, occupation (farmer, herder, worker, housework, and others), dietary habits (vegetables, fruits, meat, and milk tea), lifestyle (smoking and alcohol consumption), and disease history (e.g., hypertension, hyperlipidemia, diabetes, arthritis, and emphysema). Vegetables refer only to leafy green vegetables. We listed several types of local vegetables in the questionnaire. (see supplementary questionnaire)Agricultural and animal husbandry work were identified as outdoor occupations, while the others were considered as indoor occupations. Height and weight were measured in centimeters and kilograms respectively. Body mass index (BMI) was calculated using the universally recognized formula: weight (kg) / height (m2). Systolic and diastolic blood pressures were measured with a digital automatic blood pressure monitor. The average of the three measurements was recorded.
The questionnaire was written in Chinese, and each Kazakhs participant had undergone a comprehensive interview by trained interviewers, who is proficient in Kazakh and Chinese. Before the preliminary experiment, our questionnaire was reviewed by Dr. Luo, an expert on epidemiology and statistics. We have conducted a preliminary experiment and tested our questionnaires at a sheep farm (Township-level administrative unit) in Emin County, Tacheng Prefecture, with 121 participants in total. The results showed that the questionnaire had a Cronbach’s alpha of 0.83 and Kaiser-Meyer-Olkin (KMO) of 0.842, which demonstrates good questionnaire reliability and validity.
The anterior segments of all participants were examined carefully with a slit lamp (YZ5E, Six-six, Suzhou, China), followed by the recording of all uncorrected visual acuity and abnormal performance of the conjunctiva, cornea, lens, etc. The diagnosis of CDK (in either eye) was based on the clinical symptoms and slit-lamp examinations, and the degeneration was divided into three stages (Table 1) [1, 2].
Statistical analysis
All statistical analyses were performed using the SPSS software program (Statistical Package for Social Sciences Inc., Chicago, IL, USA, Version 21.0.0.0). The data was presented as figures using GraphPad Prism 7.0. The prevalence of CDK and the age-adjusted prevalence was calculated with references from the 2010 China Population Census. For independent samples, t-test and chi-square test were used to analyze the demographic characteristics and the grades of CDK. In addition, univariate analysis between the presence of CDK and prevalent factors was performed. The factors showing statistical or clinical significance were included in multiple logistic regression models. A P value of < 0.05 was considered to be statistically significant.
Result
Out of 1197 eligible Kazakh residents, 1095 underwent ophthalmo-logical examinations, with an overall response rate of 91.48%. We finally included 1030 people who were 40 or older (as seen in the flow chart (Fig. 2)). The mean age of the participants in the study was 54.59 ± 9.58 years old with their ages ranging from 40 to 93 years, and 46.9% (n = 483) of them were women. CDK was found in 66 (6.4%; 95% confidence interval [CI]: 4.9–7.9%) subjects where 5 (7.6%) of them were unilateral while 61 (92.4%) were bilateral. A comparison of the patient baseline characteristics between CDK group and normal group (non-CDK group) is illustrated in Table 2. And the distribution of CDK in different townships is illustrated in supplementary table. The results indicate that the overall prevalence (P) of CDK among the population was 6.4% (95% CI: 4.9–7.9%), and the prevalence of CDK was higher in men than women (8.9% vs. 4.2%, p < 0.05).

The flow chart of our study
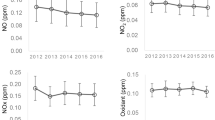
Fourteen out of all sixty-six patients diagnosed with CDK in this study are in different stages of the disease respectively in the two eyes, nine patients had a binocular disease, and five patients had monocular disease with the other eye being normal. However, patients with CDK in one eye were also included in the patient group to harmonize the data, and the disease stage was determined using the more severe eye. Among all CDK patients, 28 patients (42.4%) were classified as Grade 1, 28 patients (42.4%) were in Grade 2, and 10 patients (15.2%) were in Grade 3. The distribution of the three grades of CDK with regards to age and gender is shown in Figs. 3 and 4. The mean logMAR for the CDK patients’ uncorrected visual acuity is 0.87 ± 1.06. The mean logMAR in grade 1, grade2 and grade3 is 0.69 ± 0.90, 1.02 ± 1.22, 0.91 ± 0.97.

Distribution of residents among the different age group

Distribution of residents in different grade and gender
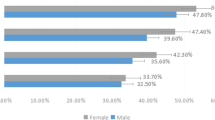
Logistic regression model was used to evaluate the relationship between the occurrence of CDK and the significant factors in Table 2 (P < 0.05). The results are presented in Fig. 5. The results found that age and exposure time were the risk factors for CDK whereas exposure protection (especially hat-wearing) and vegetable intake were the protective factors.

Multivariate analysis of factors associated with CDK
Discussion
This work conducted the first cross-sectional study on the prevalence of CDK in Xinjiang with its results indicating that the prevalence rate among the subjects was 6.4%. We speculated that the prevalence in this study may be slightly lower than clinical expectations. Based on existing literature, the prevalence rate of CDK depends on the environment, climate, and medical condition. Results obtained from studies done among the areas with reported cases of CDK indicate that the prevalence of CDK varies widely in different regions, ethnic groups, and education background. Table 3 provides an overview of the previous studies done on the prevalence of CDK. However, only studies done after 1980 are included since the definition and grading standards of CDK in earlier research were unclear.
Johnson (1981) reported that the peak prevalence of CDK occurred between a latitude of 55 and 56 degrees and the UVR in Labrador reached a peak almost exactly on the same latitude [6]. This study was conducted in Tacheng prefecture (43° 25′- 47° 15′, north) which has a lower latitude than Labrador, therefore, the prevalence of CDK was significantly lower than that in Labrador. Intriguingly, the prevalence of CDK in this study was consistent with the prevalence in Inner Mongolia [7]. However, it was significantly lower than that of Mongolia. It is worth noting that Xinjiang, Mongolia, and Inner Mongolia border each other and are on roughly similar latitudes. This indicated that there were some other factors associated with the prevalence of CDK in addition to latitude and UVR.
In this study, the occurrence of CDK was shown to be associated with age, because with the prevalence increasing with age. This finding is consistent with results from all studies listed in Table 3. Based on the positive correlation between CDK prevalence and age, we believe that the prevalence of CDK in Tacheng will increase due to the aging population. As above, the development of CDK has been known to be associated with overexposure to UVR [1]. Chronic exposure to UVR causes actinic keratosis or keratopathies which primarily affects the epithelium and the anterior stroma. The association between CDK and older age can be attributed to the cumulative exposure to UVR and ocular physiologic changes like dryness in people with increased age. This explanation was reinforced by the finding in this study that wearing hats for sun protection was a protective factor against CDK.
The impact of gender on the prevalence of CDK is still controversial. Most studies have shown that the prevalence of CDK is higher in men than in women with the exception being in some earlier studies [23, 24]. The studies attributed the result to the fact that men usually have longer outdoor exposure time than women. Despite there being a difference in the prevalence of CDK among Kazakh men and women (8.9% vs. 4.2%, p < 0.05) in this study, it did not constitute a protective or risk factor when further regression analysis was done (p > 0.05). We attributed this result to the fact that the Kazakh people in the Tacheng prefecture make a living by grazing. Therefore, men and women are engaged in similar outdoor farming and animal husbandry activities thereby resulting in no significant difference in exposure time between men and women.
Results obtained from this study indicated that there was a relationship between the dietary habits and CDK prevalence. Up to now, most Kazakhs still maintain the traditional nomadic pastoral lifestyle. They prefer eating meat over vegetables and fruits and have retained the habit of drinking a lot of traditional milk tea. Their dietary habits are significantly different from other ethnic groups. Therefore, we simply summarized their eating habits as a compound diet with high fat and low-vegetable content.
Studies have shown that a high-fat diet can cause tear film dysfunction, damaging the patient’s ocular surface, and induces dry eye symptoms [25, 26]. Additionally, several studies have reported that a high-fat diet results in high oxidative stress in the body [27,28,29], which increases the consumption of antioxidants and enzymes thereby indirectly perfecting conditions for CDK development. Therefore, we concluded that a high-fat diet might be a risk factor for CDK even though in this study meat intake was not a significant risk factor. We speculated that this could be ascribed to the fact that Kazakhs have a high meat intake. A high-fat diet has already resulted in high BMI levels in the sample population (BMI > 24). In addition, a long-term study conducted in Xinjiang indicated that Xinjiang Kazakhs were a high-risk group for metabolic syndrome and cardiovascular diseases [30]. This further confirmed the negative effects of the above diet structure on the Kazakhs.
The role of low-vegetable diet on the occurrence of CDK is prominent when compared with the high-fat diet. Results obtained from this study confirmed that the insufficient variety and quantity of vegetable intake was a risk factor for CDK. Since humans cannot synthesize vitamin C (VC) autonomously, insufficient daily vegetable intake causes a lack of VC in the body. A study in Argentina indicated that CDK patients there had abnormal dietary habits similar to the dietary habits of Kazakhs. In addition, the patients’ serum VC levels were significantly lower than the controls’, which was consistent with results obtained in this study [21]. Vitamin C has both antioxidant and metabolic functions [31, 32], and it also helps in the formation of the collagen structure. Studies have confirmed that VC plays an important role in the cornea’s defense system to counteract the damaging effects of UVR [33, 34]. Therefore, it is evident that the lack of VC increases the risk of CDK. However, further research should be done on the role of dietary habits and nutrients on the occurrence of CDK. It is possible to prevent or delay the development of CDK by changing the existing dietary habits of the patients or supplementing their nutritional deficiencies. Exploration of dietary habits also provides a new direction for the study of the pathogenesis of CDK.
The virtue of this work is that it included the in-depth analysis of life-style and dietary habits. However, this work also had some limitations. First, self-reports by patients may be limited by the accuracy of their recall and different perceptions of disease. Second, the number of patients was relatively small and only a single ethnic population from a single center was evaluated.
Conclusion
This study investigated the prevalence and associated factors of CDK among Kazakhs in Tacheng, Xinjiang, China. Obtained results indicated that the overall prevalence of CDK was 6.4% and the exposure time and age were risk factors associated with CDK occurrence. In addition, increasing the variety and quantity of vegetable intake and wearing a hat were protective factors for CDK. Based on this study, health education should be emphasized for Kazakh farmers and herdsmen should be advised to change their current dietary structure, increase vegetable intake, and take protective measures such as wearing a hat or sunglasses during outdoor work.
Availability of data and materials
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CDK:
-
Climatic droplet keratopathy
- BMI:
-
Body mass index
- VC:
-
Vitamin C
- UVR:
-
Ultraviolet radiation
- P:
-
Prevalence
- CI:
-
Confidence interval
References
Serra HM, Holopainen JM, Beuerman R, Kaarniranta K, Suárez MF, Urrets-Zavalía JA. Climatic droplet keratopathy: an old disease in new clothes. Acta Ophthalmol. 2015;93(6):496–504. https://doi.org/10.1111/aos.12628.
Freedman A. Climatic droplet keratopathy. I Clinical Aspects Arch Ophthalmol. 1973;89(3):193–7. https://doi.org/10.1001/archopht.1973.01000040195006.
Gray RH, Johnson GJ, Freedman A. Climatic droplet keratopathy. Surv Ophthalmol. 1992;36(4):241–53. https://doi.org/10.1016/0039-6257(92)90093-9.
Keshav BR, Zacheria G, Ideculla T, Bhat V, Joseph M. Epidemiological characteristics of corneal ulcers in south sharqiya region. Oman Med J. 2008;23(1):34–9.
Forsius H, Maertens K, Fellman J. Changes of the eye caused by the climate in Rwanda, Africa. Ophthal Epidemiol. 1995;2(2):107–13. https://doi.org/10.3109/09286589509057090.
Johnson G. Aetiology of spheroidal degeneration of the cornea in Labrador. Brit J Ophthalmol. 1981;65(4):270–83. https://doi.org/10.1136/bjo.65.4.270.
Zhang J. Clinical analysis and epidemiological investigation of proteinoid corneal degeneration. Chin J Ophthalmol. 1991;27(6):348–50.
Suárez MF, Serra HM. Corneal anti oxidative mechanisms malfunction are involved in the genesis of climatic droplet keratopathy; 2019.
Rao A, Sridhar U, Gupta AK. Amniotic membrane transplant with superficial keratectomy in superficial corneal degenerations: efficacy in a rural population of North India. Indian J Ophthalmol. 2008;56(4):297–302. https://doi.org/10.4103/0301-4738.39664.
Taylor H. The prevalence of corneal disease and cataracts in Australian aborigines in northwestern Australia. Aust J Ophthalmol. 1980;8(4):289–301. https://doi.org/10.1111/j.1442-9071.1980.tb00285.x.
Taylor H. Climatic droplet keratopathy and pterygium. Aust J Ophthalmol. 1981;9(3):199–206. https://doi.org/10.1111/j.1442-9071.1981.tb01013.x.
Norn M. Spheroid degeneration, keratopathy, pinguecula, and pterygium in Japan (Kyoto). Acta Ophthalmol. 1984;62(1):54–60. https://doi.org/10.1111/j.1755-3768.1984.tb06756.x.
Johnson G, Green J, Paterson G, Perkins E. Survey of ophthalmic conditions in a Labrador community: II. Ocular disease. Can J Ophthalmol. 1984;19(5):224–33.
Resnikoff S. Epidemiology of Bietti's keratopathy. Study of risk factors in Central Africa (Chad). J Fr Ophtalmol. 1988;11(11):733–40.
Taylor H, West S, Rosenthal F, Munoz B, Newland H, Emmett E. Corneal changes associated with chronic UV irradiation. Arch Ophthalmol-Chic. 1989;107(10):1481–4. https://doi.org/10.1001/archopht.1989.01070020555039.
Hill JC, Maske R, van der Walt S, Coetzer P. Corneal disease in rural Transkei. SAMJ S Afr Med J. 1989;75(10):469–72.
Resnikoff S, Filliard G, Dell'Aquila B. Climatic droplet keratopathy, exfoliation syndrome, and cataract. Brit J Ophthalmol. 1991;75(12):734–6. https://doi.org/10.1136/bjo.75.12.734.
Minassian DC, Baasanhu J, Johnson GJ, Burendei G. The relationship between cataract and climatic droplet keratopathy in Mongolia. Acta Ophthalmol. 1994;72(4):490–5. https://doi.org/10.1111/j.1755-3768.1994.tb02803.x.
Urrets-Zavalía J, Knoll E, Maccio J, Urrets-Zavalía E, Saad J, Serra H. Climatic droplet keratopathy in the argentine Patagonia. Am J Ophthalmol. 2006;141(4):744–6. https://doi.org/10.1016/j.ajo.2005.10.044.
Gelaw Y, Abateneh A. Ocular morbidity among refugees in Southwest Ethiopia. Ethiop J Health Sci. 2014;24(3):227–34. https://doi.org/10.4314/ejhs.v24i3.6.
Suarez MF, Correa L, Crim N, et al. Climatic droplet keratopathy in Argentina: involvement of environmental agents in its genesis which would open the prospect for new therapteutic interventions. In: Corneal Anti Oxidative Mechanisms Malfunction are Involved in the Genesis of Climatic Droplet Keratopathy. Avidscience; 2015. p. 1–31.
Mohan A, Jamil Z, Bhatanagar V, Gajraj M. Prevalence of spheroidal degeneration of cornea and its association with other eye diseases in tribes of Western Rajasthan. Indian J Ophthalmol. 2017;65(10):1010–4. https://doi.org/10.4103/ijo.IJO_84_17.
Freedman J. Nama keratopathy. Br J Ophthalmol. 1973;57(9):688–91. https://doi.org/10.1136/bjo.57.9.688.
Rodger FC. Clinical findings, course, and progress of Bietti's corneal degeneration in the Dahlak islands. Br J Ophthalmol. 1973;57(9):657–64. https://doi.org/10.1136/bjo.57.9.657.
Wu Y, Wu J, Bu J, Tang L, Yang Y, Ouyang W, et al. High-fat diet induces dry eye-like ocular surface damages in murine. Ocul Surf. 2020;18(2):267–76. https://doi.org/10.1016/j.jtos.2020.02.009.
Módulo CM, Machado Filho EB, Malki LT, et al. The role of dyslipidemia on ocular surface, lacrimal and meibomian gland structure and function. Curr Eye Res. 2012;37(4):300–8. https://doi.org/10.3109/02713683.2011.631720.
Varlamov O. Western-style diet, sex steroids and metabolism. BBA-Mol Basis Dis. 2017;1863(5):1147–55. https://doi.org/10.1016/j.bbadis.2016.05.025.
Hotamisligil GS, Davis RJ. Cell signaling and stress responses. CSH Perspect Biol. 2016;8(10):a006072.
Tan BL, Norhaizan ME, Liew W-P-P. Nutrients and oxidative stress: friend or foe? Oxidative Med Cell Longev. 2018;2018:9719584.
Mao L, He J, Gao X, Guo H, Wang K, Zhang X, et al. Metabolic syndrome in Xinjiang Kazakhs and construction of a risk prediction model for cardiovascular disease risk. PLoS One. 2018;13(9):e0202665. https://doi.org/10.1371/journal.pone.0202665.
Chen J, Lan J, Liu D, Backman LJ, Zhang W, Zhou Q, et al. Ascorbic acid promotes the Stemness of corneal epithelial stem/progenitor cells and accelerates epithelial wound healing in the cornea. Stem Cells Transl Med. 2017;6(5):1356–65. https://doi.org/10.1002/sctm.16-0441.
Biesalski HK, Tinz J. Nutritargeting. Adv Food Nutr Res. 2008;54:179–217. https://doi.org/10.1016/S1043-4526(07)00005-8.
Wu K, Kojima M, Shui YB, Sasaki H, Sasaki K. Ultraviolet B-induced corneal and lens damage in guinea pigs on low-ascorbic acid diet. Ophthalmic Res. 2004;36(5):277–83. https://doi.org/10.1159/000081208.
Vizzarri F, Palazzo M, Bartollino S, Casamassima D, Parolini B, Troiano P, et al. Effects of an antioxidant protective topical formulation on eye exposed to ultraviolet-irradiation: a study in rabbit animal model. Physiol Res. 2018;67(3):457–64. https://doi.org/10.33549/physiolres.933759.
Acknowledgements
None.
Funding
The study was funded by the Xinjiang Production and Construction Corps Financial Technology Plan Project (Grant 2020CB030). The funders had no role in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
JY designed the study. ZXH, GQL, LL, XLH and LMG performed the research. ZXH, XYH and JFL analyzed the data and wrote the paper. JY and JFL supervised the study. Dr. Jin Yang and Dr. Jianfeng Luo contributed equally to this work. Dr. Jin Yang (jin_er76@hotmail.com) and Dr. Jianfeng Luo (jfluo@shmu.edu.cn) are co-corresponding authors of this work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the Ninth Division Hospital of Xinjiang Production and Construction Corps. Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Ethics review.
Additional file 2.
Questionnaire.
Additional file 3.
Table: Distribution of CDK in different townships.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hua, Z., Han, X., Li, G. et al. Prevalence and associated factors for climatic droplet keratopathy in Kazakhs adults: a cross-sectional study in Tacheng, Xinjiang, China. BMC Ophthalmol 21, 316 (2021). https://doi.org/10.1186/s12886-021-02065-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-021-02065-4