
Abstract
Background
Prevention of myopia has become a public health priority in China. This study is to investigate the prevalence of myopia and vision impairment, and their associated factors in school students in eastern China.
Method
In this cross-sectional school-based study of 4801 students from 16 schools ranging from kindergarten to high school, students underwent refraction using non-cycloplegic autorefractor and visual acuity testing using logMAR chart with tumbling E. Myopia was defined as spherical equivalent (SPHE) ≤ − 0.5 diopter (D) and uncorrected visual acuity (UCVA) 20/25 or worse. High myopia was defined as SPHE ≤ − 6.0 D and UCVA 20/25 or worse. Vision impairment was defined as UCVA 20/40 or worse. Logistic regression models were used to determine factors associated with myopia and vision impairment.
Results
Among 4801 children (55% male) with mean age (standard deviation) 12.3 (3.8) years, 3030 (63.1, 95% CI: 61.7–64.5%) had myopia, 452 (9.4, 95% CI: 8.6–10.3%) had high myopia, and 2644 (55.1, 95% CI, 53.7–56.5%) had vision impairment. The prevalence rate of myopia increased with grade in a non-linear manner, 12% in kindergarten, 32% in grade 2, 69% in grade 5, and approximately 90% by grade 10 or above. The prevalence rate of high myopia was relatively low in grade 4 or below (< 1.5%), 4–7% in grade 5 to 7, 13–15% in grade 8–9, and > 20% in grade 10 to 12. The prevalence rate of vision impairment was 4% in kindergarten, 37% in elementary school, 77% in middle school and 87% in high school students. Higher grade (p < 0.0001), female (p < 0.0001) and higher school workload (p = 0.007) were independently associated with higher prevalence rates of myopia and vision impairment, while higher grade (p < 0.0001) and higher school workload (p < 0.0001) were independently associated with higher prevalence of high myopia.
Conclusion
Prevalence of myopia and vision impairment was high among Chinese school students and increased with grade in a non-linear manner, reaching alarming high in high school students accompanied by high prevalence of high myopia. Increasing study burden on school students at younger age plays an important role on the higher prevalence rate of myopia and vision impairment.
Similar content being viewed by others

Background
The prevalence of myopia has been increasing and reached alarming high rate in middle or high school students (> 80%) in East Asia [1, 2]. Myopia is projected to affect 50% of the world population by 2050 [3], and is recognized as a major twenty-first century public health problem globally [4, 5]. As a significant cause of vision loss, myopia is associated with ocular diseases including glaucoma and retinal detachment. Prevention of myopia has become an important public health priority in China.
Both genetic and environment factors play important roles in myopia development and progression, although their exact mechanisms are not yet known. Epidemiological studies have demonstrated that many factors are associated with higher rate of myopia including increasing age, larger amount of near work, family history, while more hours of outdoor activities are associated with lower risk of myopia [6,7,8,9]. The socioeconomic status and education burden on students have been reported to be associated with myopia prevalence [10, 11]. Although it is well-known that the myopia prevalence is high in China, studies suggested that there is high variation in the myopia prevalence across geographical regions of China, likely due to the differences in socioeconomic status and the education intensity of students [11]. In recent years, China has been undergoing dramatic economic development, accompanied by the increasing education pressure on the young children. These changes may have substantial impact on the myopia prevalence. The purpose of this study is to evaluate the prevalence of myopia in a high socio-economic region in East China, where educational pressure on students from schooling systems and parental expectation on academic achievements are higher than most regions of eastern China.
Methods
This is a cross-sectional school-based study of myopia prevalence conducted in May 2019 in YiWu, a county-level city of about 1.2 million people in central Zhejiang province, P. R. China. The city is famous for its small commodity trade and vibrant market (thus called International Trade City). Yiwu is well-developed and ranked as one of top 10 richest counties in P.R. China.
For this study, a random sample of 18 schools including kindergarten, elementary school (grade 1 to 6), middle school (grade 7–9) and high school (grade 10–12) were selected. Among the selected schools, random sample of classes from each grade were selected and all students from the selected classes were invited to participate the study to reach at least 80 students from each grade of the selected schools.
The information on student name, date of birth, gender and grade were obtained from each selected classes of the school. The information on school workload was obtained from school to classify school as low, moderate and high school workload based on the number of hours in class during school day, homework assignments and frequency of tests at school. All participants underwent eye examination following the standard study protocol by the trained eye-care professionals (optometrists or ophthalmologists) for common ocular diseases, tests for the distance visual acuity using retro-illuminated logMAR chart with tumbling-E optotypes followed by measuring for refractive error using table-mounted NIDEK noncycloplegic autorefractor (Model: AR-1 s, Japan). Three readings of refractive error were taken from each eye and their average was entered for analysis. If the difference between any of two readings from an eye was greater than 0.5 diopters, refractive error for that eye was re-taken.
Before test of visual acuity, students were asked whether they wear glasses, contact lens or orthokeratology contact lens. For the students not wearing glasses, the uncorrected visual acuity (UCVA) was tested for each eye. For those wearing glasses, visual acuity was first measured without correction, then was measured with best correction at 30 min after removing the glasses. Students who were found having ocular diseases (pediatric cataract, glaucoma, optic neuropathy) or ocular injuries other than the significant refractive error were not eligible for the study.
For quality control, autorefractors were calibrated every day for measuring refractive error. Approximately 5% of students were randomly chosen to repeat the test of refraction. The data were double entered into excel sheets and the differences were resolved by checking with the original paper record.
The study was approved by the Institutional Review Board. Written informed consent was obtained from legal parent/guardian for participants less than 18 years old, and from participants directly for those 18 years or older.
The study was designed to provide precise estimate of prevalence rate of myopia and hyperopia. The sample size of 4800 students in this study provides half length of 95% confidence interval of 1.4% for myopia and 0.8% for high hyperopia assuming the prevalence rate of 60% for myopia and 9% for high hyperopia.
Statistical analysis
Spherical equivalent for each eye was calculated as sphere plus half of the cylinder. Because the correlation between left eye and right eye is high for both spherical equivalent and visual acuity (Pearson correlation coefficient = 0.89 for both spherical equivalent and uncorrected visual acuity), the spherical equivalent from the more myopic eye and the uncorrected visual acuity from eye with worse visual acuity was used for analysis. Since the refractive error was measured using non-cycloplegic autorefractor, which tended to over-measure the myopic magnitude, particularly in young children [12, 13], we defined myopia using combination of spherical equivalent and UCVA. Myopia was defined as spherical equivalent ≤ − 0.5 diopter and UCVA 20/25 or worse. High myopia was defined as spherical equivalent ≤ − 6.0 diopters and UCVA 20/25 or worse. Including the UCVA into the definition of myopia was found to improve the accuracy of myopia using non-cycloplegic autorefractor refractive error [14]. Vision impairment was defined as UCVA 20/40 or worse in either eye.
Comparisons of spherical equivalent across levels of each risk factors were performed using analysis of variances, and comparisons of prevalence rates of myopia, high myopia and vision impairment across levels of each risk factor were performed using the chi-square test. To evaluate the independent association of the each risk factors (grade, gender, school location, school workload) with refractive error and prevalence of myopia and vision impairment, multivariate linear regression model was used for refractive error, and multivariate logistic regression models were used for myopia and vision impairment. In the multivariate regression models, the grade instead of age was used, because age and grade was highly correlated (Pearson correlation coefficient of 0.99) and grade was slightly more predictive of myopia and vision impairment than age. All the statistical analyses were performed in SAS v9.4 (SAS Institute Inc., Cary, NC) and two-sided p < 0.05 was considered to be statistically significant.
Results
Total of 4801 school-aged students from 16 schools of 8 towns in YiWu were enrolled into study. The student grade ranged from Kindergarten to grade 12 with number of students ranging from 331 to 403 in each grade. The mean (SD) of age was 12.3 (3.8) years ranging from 5 to 20 years, with 2647 (55.1%) male, and 2691 (56.1%) were from urban schools. Majority of students (80.0%) were from moderate workload schools, and 657 (13.7%) were from high workload schools (Table 1). Among all students, 3030 (63.1, 95% CI: 61.7–64.5%) had myopia, and 452 (9.4, 95% CI: 8.6–10.3%) had high myopia. The UCVA worse than 20/40 occurred in 2644 (55.1, 95% CI: 95% CI: 53.7–56.5%) students, including 364 (7.6%) students with UCVA 20/200 or worse.
Among all 4801 students, 2034 (42.4%) students wore glasses. However, among 3030 students with myopia, 1041 (34.5%) students did not wear glasses, 112 (10.8%) of them had UCVA 20/100 or worse, and 642 (62%) had UCVA 20/40 or worse (Table 2). Among 452 students with high myopia, 14 (3.1%) students did not wear glasses, half of them had UCVA 20/100 or worse and 79% of them had visual acuity 20/40 or worse (Table 2).
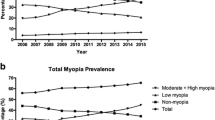
In univariate analysis (Table 3), increasing age and higher grade were significantly associated with more negative spherical equivalent, higher prevalence rates of myopia, high myopia and vision impairment (all p < 0.0001). The prevalence rate of myopia and vision impairment increased with grade following similar non-linear pattern (Fig. 1). The prevalence rates of myopia (and vision impairment) was 12% (3%) in kindergarten, 32% (21%) in grade 2, 69% (57%) in grade 5, 81% (75%) in grade 8 and approximately 90% (86%) by grade 10 or above. The prevalence rate of high myopia was relatively low in grade 4 or below (< 1.5%), 4–7% in grade 5 to 7, 13–15% in grade 8–9, and above 20% in grade 10–12 (Table 3).

The prevalence rate of myopia, high myopia and vision impairment from kindergarten (grade 0) to grade 12. The figure shows the non-linear increase of myopia and vision impairment with increasing grade following the similar pattern
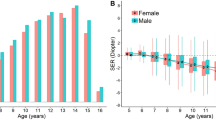
Students in urban school had more negative refractive error (− 2.8 vs. -2.2 D, p < 0.001), higher prevalence rates of myopia (66.7% vs. 58.5%, p < 0.0001), high myopia (11.3% vs. 7.0%, p < 0.0001) and vision impairment (58.7% vs. 50.4%, p < 0.0001). Female students had more negative refractive error (− 2.7 D vs. -2.5 D, p = 0.006), higher prevalence rates of myopia (67.7% vs. 59.4%, p < 0.001) and vision impairment (58.6% vs. 52.2%, p < 0.0001), but similar in high myopia (9.6% vs. 9.3%, p = 0.68).
In multivariate analysis for the spherical equivalent (Table 4), higher grade (p < 0.0001), female (p = 0.02), urban school (p = 0.004), and high workload (p < 0.0001) were independently associated with more myopia refractive error (Table 4). These factors explained about 38% of the variation of refractive error across students. The grade alone explained 36% of the variation of refractive error across students.
In multivariate analysis for myopia (Table 5), higher grade (p < 0.0001), female (p < 0.0001) and higher workload (p = 0.007) were independently associated with higher prevalence rate of myopia, while school location (p = 0.63) was not associated with myopia prevalence. These factors predicted myopia with area under ROC curve (AUC) of 0.833 (95% CI: 0.821 to 0.845). Grade alone predicted myopia with AUC of 0.827 (95% CI: 0.814 to 0.839).
In multivariate analysis of high myopia (Table 5), higher grade (p < 0.0001) and more intense education program (p < 0.0001) is independently associated with higher risk of high myopia, while gender (p = 0.76) and school location (p = 0.26) was not significantly associated with high myopia. These factors predicted high myopia with AUC of 0.810 (95% CI: 0.793 to 0.827). Grade alone predicted high myopia with AUC of 0.802 (95% CI: 0.785 to 0.819).
In multivariate analysis of vision impairment (Table 6), higher grade (p < 0.0001), female (p < 0.0001) and more intense education program (p < 0.0001) were independently associated with higher prevalence rate of vision impairment. School location (p = 0.28) was not significantly associated with vision impairment. These factors predicted vision impairment with AUC of 0.842 (95% CI: 0.831 to 0.854). Grade alone predicted vision impairment with AUC of 0.837 (95% CI: 0.825 to 0.848).
Discussion
This study evaluated the prevalence of myopia, high myopia and vision impairment in school-aged students in the well-developed YiWu city of eastern China. We found that the overall rate among school-aged students was 63% for myopia, 9.4% for high myopia and 55.1% for vision impairment. These rates are similar to those reported in the school-aged children of well-developed East Asia countries including Singapore, Hongkong and Taiwan [15], but is higher than those reported in previous studies in China [10]. We found grade was associated with myopia and high myopia in a non-linear manner, with myopia prevalence rate of 12% even for kindergarten children, 76% for grade 6 elementary school students, above 80% for middle school students and approximately 90% for high school students. The prevalence rate of high myopia was low (0.5%) for kindergarten children, but it reached 5.7% for grade 6 elementary school students, 14.5% for grade 9 middle school students and 26% for grade 12 students. These high prevalence rates of myopia and high myopia suggests myopia is becoming a major public health problem in China.
Our study found that myopia is common even in kindergarten and increases in prevalence and severity through childhood. By grade 6 of elementary school, 76% students had myopia and 5.7% had high myopia. This prevalence rates of myopia and high myopia among elementary school students in this study were higher than previous studies [10, 15]. This high rate of myopia in elementary school students suggests that the myopia onset occurred earlier than before, likely due to earlier education than before in kindergarten and the increasing education burden on elementary school students. The intense education system leads to high number of hours on near work activities and reduced time on outdoor activities, which have been established as strong risk factors for myopia [6,7,8,9]. This earlier myopia onset can lead to high rate of high myopia by high school, as observed in our study that 24% high school students had high myopia. Since high myopia is associated with increased risk of vision loss and ocular diseases, prevention/intervention strategies should be developed to prevent myopia or its progression.
Compared to our study, the study by Pan et al. reported very low prevalence rate of myopia (2.4% in grade 1 and 29.4% in grade 7) and high myopia (0.1% in grade 1, 0.4% in grade 7) in 2346 rural Chinese school students with low education pressure in Mojiang of Southwestern China. However, their study also clearly showed the higher grade was associated with higher prevalence of both myopia and high myopia [5]. The low prevalence of myopia in school students in rural China suggest that Chinese students may not have a genetic predisposition to myopia and environmental factors may play a major role in the development of school myopia in Chinese children.
Our study found prevalence of myopia and high myopia was high in both elementary school students and high school students. A similarly high prevalence rate of myopia (76.5% in elementary school and 94.9% in junior high school) and high myopia (4.0% in elementary school, and 11.3% in junior high school) were recently reported in Japanese school students [16]. The high rate of myopia in both Japanese and Chinese students may be due to large amount of near work activities and limited time on outdoor activities, as students in China and Japan have high education pressure and are in the very competitive learning environment even among elementary school students.
Our study found the myopia prevalence rate increases with grade in a not linear manner, from prevalence rate of 11.6% in kindergarten, 14.8% in grade 1, jumped to 32% in grade 2, 55% by grade 4 and 69% by grade 5, and reached above 80% by grade 8 and 90% by grade 12. This increase in the prevalence rate of myopia can be partially due to the increase in the intensity of education system in China starting from elementary school [17]. However, previous studies in Chinese students found that the annual incidence of myopia is reasonably constant between ages of approximately 7 and 15 years, and by the age of 18 years, prevalence rate reached approximately 80% in urban-Chinese students regardless of the geographic locality [3, 10]. The large increase in the prevalence of myopia at 1 year after elementary school suggests that the optimal time for studying the effect of risk factors on myopia onset and for evaluating the prevention strategy for the onset of myopia.
Our study found that although myopia was common among school students, more than one third of myopic students did not wear glasses. Among those not wearing glasses, about 11% of them had very poor visual acuity of 20/100 or worse and more than half (60%) had visual acuity 20/40 or worse. These students needed glasses but they did not own glasses. Without correction by glasses for visual acuity, these students may not see the blackboard clearly, thus face challenges in effective learning in the classroom. A study of 7681 students aged 5 to16 years in rural Yunan of China found that among the students who needed glasses, only 18.9% owned them [18], which is lower than the study in urban (35.3%) [19] and rural (61.2%) China [20]. The reasons underlying low spectacles wearing among myopia might be multifactorial, including the lack of screening for detecting myopia, teasing or bullying by peers, the low attention and consciousness of the need for glasses, or the mis-conception by parents or students that wearing glasses will make the myopia worse [19,20,21]. A recent study found that the teasing or bullying by peers (48.6%) and the lost or forgot or stolen spectacles (26.1%) are the major reason of not wearing the prescribed glasses [21]. Thus, education on students and parents about the importance of timely screening for myopia and wearing glasses for best vision is very important to improve student learning and academic achievement.
Our study found that students in urban schools were likely immersed in an intensive education environment thus had higher prevalence rate of both myopia and high myopia. This is consistent with previous findings that location of residency (urban vs. rural) of an individual are associated with the likelihood of myopia [8], and the association between more near work or less outdoor activities are associated with higher risk of myopia [6, 7, 9].
The strength of the study includes the large sample size with representative sample of school students of all grades, allowing us to evaluate the association of myopia and vision impairment with age and grade. The study is limited in that the risk factors evaluated are very limited, and the refractive error was measured with non-cycloplegic autorefractor. Although our myopia definition was based on the combination of spherical equivalent and visual acuity to minimize the over-estimate myopia prevalence from using non-cycloplegic refractive error for defining the myopia, our estimate of myopia and high myopia can still be biased.
Conclusions
This school-based cross-sectional study found that myopia and vision impairment are very common in school-age students, reaching alarming high in high school students. Increasing grade and higher school workload were associated with higher prevalence rate of myopia and vision impairment. Future longitudinal studied are needed to evaluate the progression from myopia to high myopia in school-aged children and to develop the intervention strategies to prevent or slow down the progression of myopia.
Availability of data and materials
De-identified data are available upon request to the first author.
Abbreviations
- AUC:
-
Area under receiver operating curve
- BCVA:
-
Best corrected visual acuity
- CI:
-
Confidence interval
- D:
-
Diopter
- SD:
-
Standard deviation
- SE:
-
Standard error
- SPHE:
-
Spherical equivalent
References
Dolgin E. The myopia boom. Nature. 2015;519(7543):276–8.
Li Y, Liu J, Qi P. The increasing prevalence of myopia in junior high school students in the Haidian District of Beijing, China: a 10-year population-based survey. BMC Ophthalmol. 2017;17(1):88.
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–42.
Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32(1):3–16.
Pan CW, Wu RK, Li J, Zhong H. Low prevalence of myopia among school children in rural China. BMC Ophthalmol. 2018;18(1):140.
He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA. 2015;314(11):1142–8.
Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–85.
Rose KA, Morgan IG, Smith W, Burlutsky G, Mitchell P, Saw SM. Myopia, lifestyle, and schooling in students of Chinese ethnicity in Singapore and Sydney. Arch Ophthalmol. 2008;126(4):527–30.
Wu PC, Tsai CL, Wu HL, Yang YH, Kuo HK. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013;120(5):1080–5.
Morgan IG, French AN, Ashby RS, et al. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res. 2018;62:134–49.
Morgan IG, French AN, Rose KA. Intense schooling linked to myopia. BMJ. 2018;361:k2248.
Fotedar R, Rochtchina E, Morgan I, Wang JJ, Mitchell P, Rose KA. Necessity of cycloplegia for assessing refractive error in 12-year-old children: a population-based study. Am J Ophthalmol. 2007;144(2):307–9.
Zhao J, Mao J, Luo R, Li F, Pokharel GP, Ellwein LB. Accuracy of noncycloplegic autorefraction in school-age children in China. Optom Vis Sci. 2004;81(1):49–55.
Wang NL, Wei SF. Emphasizing the standardized use of cycloplegics in the epidemiological studies of myopia. Zhonghua Yan Ke Za Zhi. 2019;55(8):561–4.
Rudnicka AR, Kapetanakis VV, Wathern AK, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. Br J Ophthalmol. 2016;100(7):882–90.
Yotsukura E, Torii H, Inokuchi M, et al. Current Prevalence of Myopia and Association of Myopia With Environmental Factors Among Schoolchildren in Japan. JAMA Ophthalmol 2019;137(11):1233–39.
Ma Y, Qu X, Zhu X, et al. Age-specific prevalence of visual impairment and refractive error in children aged 3-10 years in Shanghai, China. Invest Ophthalmol Vis Sci. 2016;57(14):6188–96.
Qian DJ, Zhong H, Li J, Niu Z, Yuan Y, Pan CW. Myopia among school students in rural China (Yunnan). Ophthalmic Physiol Opt. 2016;36(4):381–7.
Wang X, Yi H, Lu L, et al. Population prevalence of need for spectacles and spectacle ownership among urban migrant children in eastern China. JAMA Ophthalmol. 2015;133(12):1399–406.
Congdon N, Zheng M, Sharma A, et al. Prevalence and determinants of spectacle nonwear among rural Chinese secondary schoolchildren: the Xichang pediatric refractive error study report 3. Arch Ophthalmol. 2008;126(12):1717–23.
Morjaria P, Evans J, Gilbert C. Predictors of spectacle Wear and reasons for nonwear in students randomized to ready-made or custom-made spectacles: results of secondary objectives from a randomized noninferiority trial. JAMA Ophthalmol. 2019;137(4):408–14.
Acknowledgements
Not Applicable.
Funding
Dr. Ying is supported by the Foundation Fighting Blindness and the Mackall Trust Funds. The funding bodies has have no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
JW contributed to the design and conduct of the study, data collection and management, and results interpretation and wrote the whole paper. GSY performed the statistical analysis and critically revised the manuscript. XF contributed to the design and conduct of the study, data collection, and critically revised the manuscript. RZ, JM, FG, and JL contributed to the design and conduct of the study, data collection, and critically revised the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethics approval was obtained from Ethics Committee of The First Affiliated Hospital of Zhejiang University. Written informed consent was obtained from legal parent/guardian for participants less than 18 years old, and from participants directly for those 18 years or older.
Consent for publication
Yes
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, J., Ying, Gs., Fu, X. et al. Prevalence of myopia and vision impairment in school students in Eastern China. BMC Ophthalmol 20, 2 (2020). https://doi.org/10.1186/s12886-019-1281-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-019-1281-0