
Abstract
Background
Few studies have investigated the prevalence of refractive error (RE) in older adults in China, and most have focused on East China. Our study determined the prevalence and risk factors of RE in Han and Yi adults aged 40–80 years in rural and urban areas in Yunnan Province, Southwest China.
Methods
Our cross-sectional study is part of the China National Health Survey (CNHS). The age-adjusted prevalence rates of RE in Han and Yi adults aged 40–80 years in Yunnan were compared. We used a multivariate logistic regression model to identify risk factors for myopia and hyperopia.
Results
Among 1626 participants, the age-adjusted prevalence rates of myopia, hyperopia, high myopia and astigmatism were 26.35% (95%CI 24.01–28.70%), 19.89% (95%CI 18.16–21.61%), 2.64% (95%CI 1.75–3.53%), and 56.82% (95%CI 54.31–59.34%). Compared to the Yi population, the Han population had higher prevalence of myopia (31.50% vs 16.80%, p < 0.0001), high myopia (3.34% vs 1.31%, p = 0.049) and astigmatism (60.07% vs 50.67%, p = 0.026) but lower prevalence of hyperopia (16.58% vs 27.37%, p < 0.0001). In the multivariate logistic regression, individuals aged 45–49 (p < 0.001), 50–54 (p < 0.001), 55–59 (p = 0.014), and 60–64 years (p = 0.005) had a lower myopia risk than those aged 40–44 years, and individuals aged 50–54 (p = 0.002), 55–59, 60–64 and 65 years and older (all p < 0.001) had a higher hyperopia risk than those aged 40–44 years. Myopia was also associated with height (p = 0.035), time spent in rural areas (p = 0.014), undergraduate/graduate education level (p = 0.001, compared with primary school or lower education level) and diabetes (p = 0.008). The Yi population had a higher risk of hyperopia than the Han population (p = 0.025). Moreover, hyperopia was related to time spent in rural areas (p < 0.001) and pterygium (p = 0.019).
Conclusions
Our study investigated the overall prevalence of RE in older adults in rural and urban areas of Southwest China. Compared to the Yi population, the Han population had a higher prevalence of myopia, high myopia and astigmatism but a lower risk of hyperopia. The prevalence of myopia in the Han population in underdeveloped Southwest China was similar to that of residents in East China or of Chinese Singaporeans under urban or rural settings.
Similar content being viewed by others
Background
Refractive error (RE) is one of the most important ocular anomalies. Uncorrected RE is the leading cause of visual impairment [1]. In recent decades, myopia has become highly epidemic in children and young adults in East Asia. A Korean study reported a myopia prevalence of 83.3% in young adults aged 19 years [2]. In China, the myopia prevalence was 73.1% in teenagers 15 years of age in Guangzhou [3] and 95.5% among undergraduate or graduate students in Shanghai [4]. For older adults, studies in Singapore (Tanjong Pagar Study: myopia 38.7%), [5] Japan (Tajimi Study: myopia 41.8%), [6] India (Andhra Pradesh Eye Disease Study: myopia 34.6%), [7] and Burma (Meiktila Eye Study: myopia 42.7%) [8] showed a relatively higher prevalence of myopia than that in the United States (Multiethnic Study of Atherosclerosis: myopia 25.1%) [9] and Australia (Victoria Visual Impairment Project: myopia 17.0%) [10]. Studies in multiethnic countries revealed that Chinese individuals have a higher myopia prevalence and a lower hyperopia prevalence. In the United States, the prevalence of myopia in Chinese subjects is three times that in Hispanic subjects [9]. In Singapore, Chinese people have a higher risk of myopia and a lower risk of hyperopia than Malay and Indian people [11]. However, there are few studies investigating the RE prevalence in older adults in mainland China, and most of these studies were conducted in Eastern China with a large variation between the reported prevalence rates [5, 12,13,14,15,16,17].
The Chinese population is composed of the Han ethnicity (91.51%) and 55 ethnic minorities [18]. Previous studies indicated differences in the prevalence of myopia between the Han population and the ethnic minorities. An epidemiologic study in Xinjiang found that the prevalence of myopia is Han > Hui > Uygur in children aged 4–19 years [19]. Another study, involving undergraduates in Shanghai, reported a higher risk for myopia in Han individuals than in subjects from ethnic minorities [4]. Apart from Yunnan Minority Eye study, [17] few studies have investigated the difference in the prevalence of myopia between the Han population and the ethnic minorities in elder adults. Located on the southwestern border of China, Yunnan is crossed by the Tropic of Cancer. Yi is the seventh largest ethnicity of China, and 57.85% of the Yi population live in Yunnan Province as the largest ethnic minority in Yunnan [20]. Previous studies revealed the significant difference between the Yi and Han populations in health-related quality of life, [21] metabolic syndrome, [22] blood cell parameters [23] and certain gene loci [24].
The Yunnan Minority Eye Study has investigated the prevalence of myopia in rural areas in Yunnan [17]. To obtain a more comprehensive understanding of refractive error in Southwest China, our cross-sectional study, as part of the China National Health Survey (CNHS), described the overall prevalence of myopia, hyperopia, high myopia and astigmatism with sampling in a large city, a county site and a rural section containing Han and Yi populations aged 40–80 years in Yunnan. Furthermore, we explored the risk factors for myopia and hyperopia.
Methods
Study population
The CNHS was conducted by the Chinese Academy of Medical Sciences to evaluate the Physiological Constant and Health Condition in Chinese. The part reported in this study was conducted in Yunnan in 2015. The CNHS used a multistage cluster sampling method. According to the level of urbanization, three locations were randomly chosen for sampling in this cross-sectional study, including a large city (Health Examination Center of Wuhua District in Kunming City), a county seat (Xiuping Community Hospital in Luquan County), and a rural section (Chepanying Town in Luquan County). In each selected area, different districts were selected as sampling units.
Data collection
Questionnaire and routine physical examination
A questionnaire about demographic information and health history was administered during a comprehensive interview by well-trained interviewers. The questionnaire included information about age, sex, ethnicity, birthplace, current residence, migration date, education level, occupation, income per month, smoking and drinking practices, occupational and leisure-time physical activities, and medical history (including hypertension and diabetes status). An assessment of height, weight, blood pressure, and fasting blood glucose was included in routine physical examinations. Height was measured to the nearest 0.1 cm using a fixed stadiometer and in the standing position by bioelectrical impedance analysis (BIA) with a commercially available body composition analyser (BC-420, TANITA, Japan) with participants in lightweight clothes. A digital automatic blood pressure monitor was used to measure systolic and diastolic blood pressure, and the average of three measurements was recorded. Blood samples were drawn after fasting overnight for at least 8 h and were then immediately processed, refrigerated, transferred and assessed in the laboratory at the General Hospital of Chinese Peoples’ Liberation Army, Beijing. Body mass index (BMI) was calculated using the formula weight (kg)/height (m)2.
Eye examination
Well-trained ophthalmologists performed eye examinations on our participants. A logarithm of the minimum angle of resolution E chart (Wehen Co., Ltd., Guangzhou, China) was used for visual acuity measurement at 4 m. An auto ref-keratometer (ARK-510A, Nidek Co., Ltd., Tokyo, Japan) was used to measure noncycloplegic refraction and corneal curvature radium. The anterior segment of the eye was examined with a portable hand-held slit-lamp (KJ5S2, Suzhou Kangjie Medical Co. Ltd., Jiangsu, China).
Inclusion and exclusion criteria
Only participants whose parents were both Han or both Yi were included in our study. The proportions of Han and Yi participants in our study were similar to the natural proportions of the population distribution at the survey sites. Only people who had lived in their current residence for more than 1 year were included. Psychiatric patients, pregnant women and active duty soldiers were excluded. Thus, 1860 participants aged 40–80 years old were eligible for our study; 1665 participants completed the questionnaire and eye examination, with a response rate of 89.52%. After excluding individuals with a cataract or myopic surgical history, data of 1626 participants were included in the final analysis.
Stratification standard
All participants were divided into six age groups, which were 40–44, 45–49, 50–54, 55–59, 60–64, and 65+ years old. Education level was divided into three groups including primary school and lower, middle/high school, and undergraduate/graduate. Occupation information was divided into close-work (including workmen and government workers), and non-close-work (including farmers, waiters and domestic workers). Additionally, participants were divided into never-smokers and ever-smokers (including current smokers and former smokers). Alcohol consumption was divided into two categories: never-drinkers and ever-drinkers (including current drinkers and former drinkers). We merged occupational and leisure-time physical activity into an activity level and regrouped it into three levels: low, moderate and high.
Definitions of RE
In our study, myopia was defined as spherical equivalent (SE) < − 0.5D, and hyperopia was defined as SE > 0.5D. High myopia was defined as SE < − 6.0D. Astigmatism was defined as ≥0.5D of the cylinder.
Statistics
A high correlation between right and left eyes was found in our study (Spearman correlation test, p < 0.0001, r = 0.8291). We obtained similar statistical analysis results between right and left eyes and only reported the results of the right eye for concision. The Chi-square test and Mann-Whitney test were used to compare the demographic differences between Han and Yi populations. A linear regression model was used to compare the SE and RE prevalence among different age groups. The difference in RE distributions between ethnicities among different age groups was tested with a Chi-square test. The Wilcoxon signed rank test was used to test the difference in SE among different age groups between ethnicities. The risk factors for RE were identified through a multivariate logistic regression analysis. Myopic and hyperopic individuals were compared to emmetropic individuals. The age-standardized prevalence was based on the Sixth National Population Census of the People’s Republic of China. A p value less than 0.05 was considered significant. Statistical analyses were performed using Stata version 13.1 (StataCorp, USA) and Statistical Analysis System (SAS) version 9.4; figures were created using GraphPad Prism 5.0 (Graphpad Software Inc., USA).
Results
Characteristics of Han and Yi adults
In total, 1626 participants aged 40–80 years old, comprising 1085 Han participants and 541 Yi participants, were included in the final analysis (Table 1). The sex and age compositions were similar between the Han and Yi populations (p = 0.881 and p = 0.081 respectively). Additionally, no difference was found in lifestyles, including smoking and drinking practices, between the Han and Yi populations (p = 0.112 and p = 0.130 respectively). However, the Han and Yi participants differed in many demographic aspects in our study. The Han population was taller and heavier and had a higher BMI than the Yi population (all p < 0.001). A greater proportion of the Han population was born and now lived in an urban area and had a shorter time spent in rural areas (all p < 0.001). Moreover, more Han participants were influenced by hypertension (40.01% vs 34.01%, p = 0.006) and diabetes (5.99% vs 2.77%, p = 0.005). There were slight differences between the Han and Yi populations with respect to activity levels, and a higher proportion of the Yi population reported moderate and heavy activity levels (light: 15.21% vs 10.72%; moderate: 77.05% vs 80.59%; heavy: 7.74% vs 8.69%; p = 0.043).
Prevalence of RE in the Han and Yi populations
The age-adjusted prevalence rates of myopia, hyperopia, high myopia and astigmatism were 26.35% (95%CI 24.01–28.70%), 19.89% (95%CI 18.16–21.61%), 2.64% (95%CI 1.75–3.53%), and 56.82% (95%CI 54.31–59.34%) (Table 2). Moreover, there were differences in the prevalence of different RE values between the Han and Yi populations. The age-adjusted prevalences of myopia (31.50% vs 16.80%, p < 0.0001), high myopia (3.34% vs 1.31%, p = 0.049) and astigmatism (60.07% vs 50.67%, p = 0.026) were higher in the Han population than in the Yi population. However, the age-adjusted prevalence of hyperopia in the Yi population was higher than that in the Han population (27.37% vs 16.58%, p < 0.0001).
Distribution of RE and SE in different age groups
Participants included in the final analysis were divided into six age groups, which were 40–44, 45–49, 50–54, 55–59, 60–64, and 65 and over years old. The mean SE increased in the Han population as the age increased (p = 0.034), and the Yi population showed an increasing trend with age, although without statistical significance (p = 0.052) (Fig. 1a). The Yi population had the highest SE level in all age groups compared to the SE levels of the Han population (p = 0.031). The prevalence of hyperopia increased with ageing in both the Han (p = 0.002) and Yi populations (p = 0.012). The distributions of RE differed between the Han and Yi ethnicities for all age groups (40–44 p = 0.033, 45–49 p < 0.0001, 50–54 p = 0.005, 55–59 p < 0.0001, 60–64 p = 0.018, 65+ p = 0.017) (Fig. 1b).

Spherical equivalent (SE) and distribution of refractive error (RE) in different age groups in Yi and Han populations. a: SE in different age groups in Han and Yi populations; b: Distribution of RE in different age groups in Han and Yi populations. Chi-square tests were used to test the distribution difference in the prevalence of RE between Han and Yi populations (p < 0.05 *, p < 0.01 **, p < 0.001 ***)
Risk factors for myopia and hyperopia
A multivariate logistic regression with 12 indicators including ethnicity, sex, age period, height, length of time spent in rural areas, education level, activity level, occupation, income, pterygium status of the same eye, diabetes status and smoking practice was used to assess risk factors for myopia and hyperopia. Myopia and hyperopia results were compared to those of emmetropic individuals, and the results are presented in Table 3. Ethnicity was not a risk factor for myopia (OR 0.77, 95%CI 0.55–1.08, p = 0.127) but was associated with hyperopia, and Yi ethnicity (compared to Han ethnicity) was a risk factor for hyperopia (OR 1.45, 95%CI 1.05–2.00, p = 0.025).
For myopia (Fig. 2), compared to participants aged 40–44 years, those aged 45–49 (OR 0.44, 95%CI 0.29–0.67, p < 0.0001), 50–54 (OR 0.43, 95%CI 0.28–0.66, p < 0.0001), 55–59 (OR 0.55, 95%CI 0.34–0.89, p = 0.014), and 60–64 years (OR 0.49, 95%CI 0.30–0.81, p = 0.005) had a lower risk of myopia. Compared to those with a primary school or lower education level, participants who had an undergraduate/graduate education level had a much higher risk of myopia (OR 2.50, 95%CI 1.46–4.25, p = 0.001). Myopia was also identified to be associated with height (OR 0.97, 95%CI 0.95–1.00, p = 0.035) and time spent in rural areas (OR 0.99, 95%CI 0.98–1.00, p = 0.014). Moreover, individuals with diabetes had a much higher risk of myopia than those without diabetes (OR 2.11, 95%CI 1.21–3.66, p = 0.008).

Multivariate logistic regression results for myopia. A multivariate logistic regression model with 12 indicators (including ethnicity, sex, age range, height, length of time spent in rural areas, education level, activity level, occupation, income, pterygium status of the same eye, diabetes status and smoking practice) was used to assess risk factors for myopia. Myopic individuals were compared to emmetropic individuals. The OR of ethnicity was Yi/Han. The OR of sex was female/male. The OR of occupation was close-workers/non-close-workers. The OR of pterygium was the eye with pterygium/the eye without pterygium. The OR of diabetes was individuals with diabetes/individuals without diabetes. The OR of smoking was individuals who had smoked/individuals who had never smoked.
For hyperopia (Fig. 3), apart from ethnicity, age was also significantly related to the occurrence of hyperopia. Compared to those aged 40–44 years, in individuals aged 45–49 years, the risk of hyperopia did not increase. However, individuals aged 50–54 (p = 0.002), 55–59, 60–64, and 65+ years (all p < 0.0001) had a much higher risk of hyperopia than those aged 40–44 years, with an increasing OR with ageing; furthermore, the OR for the 65+ age group reached 21.28 (95%CI 8.07–55.56, p < 0.0001). Time spent in rural areas also changed the risk of hyperopia slightly (OR 1.02, 95%CI 1.01–1.03, p < 0.0001). Moreover, the pterygium status of the same eye increased the hyperopia risk, with an OR equal to 1.80 (95%CI 1.10–2.93, p = 0.019).

Multivariate logistic regression results for hyperopia. A multivariate logistic regression model with 12 indicators (including ethnicity, sex, age range, height, length of time spent in rural areas, education level, activity level, occupation, income, pterygium status of the same eye, diabetes status and smoking practice) was used to assess risk factors for hyperopia. Hyperopic individuals were compared to emmetropic individuals. The OR of ethnicity was Yi/Han. The OR of sex was female/male. The OR of occupation was close-workers/non-close-workers. The OR of pterygium was the eye with pterygium/the eye without pterygium. The OR of diabetes was individuals with diabetes/individuals without diabetes. The OR of smoking was individuals who had smoked/individuals who had never smoked.
Discussion
Our study described and compared the prevalence of RE in Han and Yi populations aged 40–80 years in Yunnan. The overall myopia prevalence among the subjects in our study was 26.35% (95%CI 24.01–28.70%), which is even higher than the prevalence of myopia in older adults in Beijing, [13] Suzhou [15] and Shanghai, [12] but lower than that in Chinese individuals in Singapore [5] and Guangzhou (Table 4) [14].
The Yunnan Minority Eye Study conducted in 2010, which focused only on myopia in those older than 50 years in rural areas, found a much lower prevalence of myopia than those in other studies of Chinese people [17]. However, it is difficult to draw a conclusion while comparing data under rural area settings to data from urban areas or urban/rural areas. Our study revealed that the age-standardized prevalence of myopia in the Han population was nearly double that in the Yi population (31.50% vs 16.80%, p < 0.0001). The Han population constitutes 91.6% of the population in China, and this proportion is even higher in Beijing and Southeast China [20]. Han is also the main ethnicity of Singaporean Chinese. To make the prevalence of myopia more comparable, we further calculated the prevalence of myopia separately under rural or urban settings for different age ranges (Fig. 4). We found that in urban settings, the prevalence of myopia in the Han population in our study was similar to those of the Tanjong Pajar study in Singapore, [5] slightly lower than that of the Liwan study in Guangzhou [14] and slightly higher than that in the Shanghai Eye Study (Fig. 4a) [12]. Similarly, under rural settings, the prevalence of myopia in the Han population in our study was nearly the same as that in the Handan Eye Study (Fig. 4b) [16]. Therefore, the Han population in underdeveloped Southwest China has a similar prevalence of myopia to those in East China or Singapore under urban or rural settings. If we only focused on subjects older than 50 years old in rural areas, the age-standard myopia prevalence was 14.3% in the Han population (95%CI 9.2–19.4%) and 11.5% (95%CI 7.0–16.0%) in the Yi population, which is higher than the results (Han 10.3, 95%CI 9.0–11.7%; Yi 8.1, 95%CI 6.8–9.4%) in the previous Yunnan Minority Eye Study under the same rural settings and age ranges [17]. This difference may have resulted from selection bias between different studies or from a possible increase in myopia prevalence over the last five years [25].

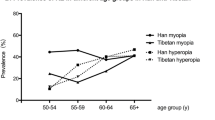
Prevalence of myopia in Chinese populations in selected studies. a Prevalence of myopia in Chinese populations in urban area; b Prevalence of myopia in Chinese populations in rural area. CNHS: Chinese National Health Survey; YMES: Yunnan Minorities Eye Study; Data for the age group of 70–79 years in the Han CNHS Yunnan 2015 study are not shown because of the limited number of samples (n < 15).
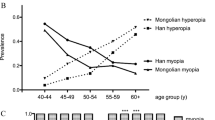
The age-standardized prevalence of hyperopia in our study was 19.89% (95%CI 18.16–21.61%) and was lower in the Han population than in the Yi population (16.58% vs 27.37%, p < 0.0001). With the multivariate logistic regression, compared to Yi ethnicity, Han ethnicity was found to be a protective factor in our study after being adjusted for age, sex, height, time spent in rural areas, education level, activity level, occupation, income, pterygium of the same eye, diabetes and smoking practice (p = 0.025). In a multiethnic study in Singapore, the Chinese population had the lowest hyperopia risk compared to that of Malay and Indian subjects [11]. Compared to studies focusing on populations older than 40 years and defining hyperopia as SE > 0.5D, our study found that the prevalence of hyperopia, especially in the Han population, was much lower than that in western countries, [5, 10, 26] Singapore, [27, 28] Japan, [6] Iran [29] and Mongolia (Table 4) [30].
Our study further identified several risk factors for myopia and hyperopia. For myopia, the prevalence of myopia first decreased and then increased with increasing age. A similar U-shaped curve was also reported in the Handan Eye Study, [16] Tanjong Pajar study, [5] Malay Eye Study in Singapore, [28] and Sumatra study in Indonesia [31]. The decreasing part of the U-curve could be explained by the intrinsic age-related decrease in the amount of an individual’s myopia [32] and/or cohort effect by which younger generations may have more reading exposure, less outdoor activity and other factors varying among birth cohorts [11]. Moreover, the increasing part of the U-curve might be related to the myopic shift in refraction due to cataract development [33]. Previous studies have indicated that compared to urban residence, rural residence could decrease the risk of myopia [13, 34, 35]. Considering the rapid urbanization process and that myopia development mainly happens in adolescence, we combined the residence information into time spent in rural areas, which was found to decrease the risk of myopia (p = 0.014) in our study. Education level was associated with a higher risk of myopia in our study, which has frequently been described in previous studies [36,37,38]. Moreover, we found that height was associated with myopia and that a taller height was protective. A relatively consistent view has been formed that height is positively related to the axial length of the eye [39,40,41]. However, the relationship between height and myopia is still controversial [9, 39, 42]. Our study also found that diabetes increases the risk of myopia significantly, as has previously been proven in the Los Angeles Latino Eye Study, [43] Barbados Eye Study, [26] and Handan Eye Study [16]. Furthermore, a higher level of HbA1c is a risk factor for myopia in patients with type 2 diabetes [44]. This relationship might be explained by the pathological change caused by the high level of blood glucose. Additionally, no relationship was found in some studies between diabetes and myopia [5, 45,46,47]. We found no association between myopia and activity level, occupation, and income level, which is consistent with the shift in the view that outdoor activities play a greater role than the young-age near-work model in decreasing the risk of myopia [48].
For hyperopia, the hyperopic shift with ageing has been proven in many longitudinal studies, [49,50,51] we found an increasing trend for the prevalence of hyperopia in both Han and Yi populations with an increasing age, and older age was found to be a significant risk factor for hyperopia. Additionally, the presence of a pterygium was found to increase the risk of hyperopia (p = 0.019), which was consistent with previous studies [52, 53]. A thinner cornea and sclera and more redundant conjunctivas were found in eyes with myopia compared to eyes with hyperopia, which might be protective from pterygium [54,55,56]. Pterygium is also related to older age, and the association between older age and hyperopia might also contribute [57].
The strength of this study included a relatively comprehensive population-based sample from a large city, county site and rural area; reasonable response rates; a standardized refraction assessment; and reliable demographic data. However, as this was a cross-sectional study, we were unable to establish causality between risk factors and RE. Cohort studies are recommended for the future. Moreover, further studies involving more participants in West China are highly recommended to draw an overall map of the understanding of RE in China.
Conclusions
Our study investigated the overall prevalence of RE including myopia, hyperopia, high myopia and astigmatism in rural and urban areas in Yunnan China in adults aged 40–80 years. The Han population had a higher prevalence of myopia, high myopia and astigmatism but a lower risk of hyperopia than the Yi population. With multivariate logistic regression, myopia was found to be associated with age, height, time spent in rural areas, education level, and diabetes. Hyperopia was associated with ethnicity, age, time spent in rural areas and pterygium. The Han population in underdeveloped Southwest China in our study had a similar prevalence of myopia to those in East China or in Chinese Singaporeans under urban or rural settings.
Abbreviations
- BIA:
-
Bioelectrical impedance analysis
- BMI:
-
Body mass index.
- CNHS:
-
China National Health Survey.
- RE:
-
Refractive error.
- SAS:
-
Statistical Analysis System.
- SE:
-
Spherical equivalent.
References
Pizzarello L, Abiose A, Ffytche T, Duerksen R, Thulasiraj R, Taylor H, Faal H, Rao G, Kocur I, Resnikoff S. VISION 2020: the right to sight: a global initiative to eliminate avoidable blindness. Arch Ophthalmol. 2004;122(4):615–20.
Lee JH, Jee D, Kwon JW, Lee WK. Prevalence and risk factors for myopia in a rural Korean population. Invest Ophthalmol Vis Sci. 2013;54(8):5466–71.
He MG, Zeng JW, Liu YZ, Xu JJ, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern China. Invest Ophth Vis Sci. 2004;45(3):793–9.
Sun J, Zhou J, Zhao P, Lian J, Zhu H, Zhou Y, Sun Y, Wang Y, Zhao L, Wei Y, et al. High prevalence of myopia and high myopia in 5060 Chinese university students in Shanghai. Invest Ophthalmol Vis Sci. 2012;53(12):7504–9.
Wong TY, Foster PJ, Hee J, Ng TP, Tielsch JM, Chew SJ, Johnson GJ, Seah SK. Prevalence and risk factors for refractive errors in adult Chinese in Singapore. Invest Ophthalmol Vis Sci. 2000;41(9):2486–94.
Sawada A, Tomidokoro A, Araie M, Iwase A, Yamamoto T, Tajimi Study G. Refractive errors in an elderly Japanese population: the Tajimi study. Ophthalmology. 2008;115(2):363–70 e363.
Krishnaiah S, Srinivas M, Khanna RC, Rao GN. Prevalence and risk factors for refractive errors in the south Indian adult population: the Andhra Pradesh eye disease study. Clin Ophthalmol. 2009;3:17–27.
Gupta A, Casson RJ, Newland HS, Muecke J, Landers J, Selva D, Aung T. Prevalence of refractive error in rural Myanmar: the Meiktila eye Study. Ophthalmology. 2008;115(1):26–32.
Pan CW, Klein BE, Cotch MF, Shrager S, Klein R, Folsom A, Kronmal R, Shea SJ, Burke GL, Saw SM, et al. Racial variations in the prevalence of refractive errors in the United States: the multi-ethnic study of atherosclerosis. Am J Ophthalmol. 2013;155(6):1129–38 e1121.
Wensor M, McCarty CA, Taylor HR. Prevalence and risk factors of myopia in Victoria, Australia. Arch Ophthalmol. 1999;117(5):658–63.
Pan CW, Zheng YF, Anuar AR, Chew M, Gazzard G, Aung T, Cheng CY, Wong TY, Saw SM. Prevalence of refractive errors in a multiethnic Asian population: the Singapore epidemiology of eye disease study. Invest Ophthalmol Vis Sci. 2013;54(4):2590–8.
He J, Lu L, He X, Xu X, Du X, Zhang B, Zhao H, Sha J, Zhu J, Zou H, et al. The relationship between crystalline Lens power and refractive error in older Chinese adults: the Shanghai eye Study. PLoS One. 2017;12(1):e0170030.
Xu L, Li J, Cui T, Hu A, Fan G, Zhang R, Yang H, Sun B, Jonas JB. Refractive error in urban and rural adult Chinese in Beijing. Ophthalmology. 2005;112(10):1676–83.
He MG, Huang WY, Li YT, Zheng YF, Yin QX, Foster PJ. Refractive error and biometry in older Chinese adults: the Liwan eye Study. Invest Ophth Vis Sci. 2009;50(11):5130–6.
Xu C, Pan C, Zhao C, Bi M, Ma Q, Cheng J, Song E. Prevalence and risk factors for myopia in older adult east Chinese population. BMC Ophthalmol. 2017;17(1):191.
Liang YB, Wong TY, Sun LP, Tao QS, Wang JJ, Yang XH, Xiong Y, Wang NL, Friedman DS. Refractive errors in a rural Chinese adult population the Handan eye study. Ophthalmology. 2009;116(11):2119–27.
Pan CW, Chen Q, Sheng X, Li J, Niu Z, Zhou H, Wei T, Yuan Y, Zhong H. Ethnic variations in myopia and ocular biometry among adults in a rural community in China: the Yunnan minority eye studies. Invest Ophthalmol Vis Sci. 2015;56(5):3235–41.
Tabulation on the 2010 population census of the People's Republic of China. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm.
Chin MP, Siong KH, Chan KH, Do CW, Chan HH, Cheong AM. Prevalence of visual impairment and refractive errors among different ethnic groups in schoolchildren in Turpan, China. Ophthalmic Physiol Opt. 2015;35(3):263–70.
Tabulation on the 2010 population cesus of the People's Republic of China. http://wwwstatsgovcn/tjsj/pcsj/rkpc/6rp/indexchhtm 2010.
Ran L, Jiang X, Li B, Kong H, Du M, Wang X, Yu H, Liu Q. Association among activities of daily living, instrumental activities of daily living and health-related quality of life in elderly Yi ethnic minority. BMC Geriatr. 2017;17(1):74.
Liu Y, Liu F, Jia H. The investigation of metabolism syndrome of Han, Yi and Miao ethnicity in southwest of China. Chinese General Practice. 2017;20(33):4199–203.
Yang S, Li L, Tang L, Li X, Fu X, Chen C, You P. The investigation of lab parameters of vein blood of 1709 participants of Han and Yi ethnicity. Lab Med. 2016;31(07):588–9.
Zhang X, Hu L, Du L, Zheng H, Nie A, Rao M, Bo Pang J, Nie S. Population data for 20 autosomal STR loci in the Yi ethnic minority from Yunnan Province, Southwest China. Forensic Sci Int Genet. 2017;28:e43–4.
Sensaki S, Sabanayagam C, Verkicharla PK, Awodele A, Tan KH, Chia A, Saw SM. An ecologic Study of trends in the prevalence of myopia in Chinese adults in Singapore born from the 1920s to 1980s. Ann Acad Med Singap. 2017;46(6):229–36.
Wu SY, Nemesure B, Leske MC. Refractive errors in a black adult population: the Barbados eye Study. Invest Ophthalmol Vis Sci. 1999;40(10):2179–84.
Pan CW, Wong TY, Lavanya R, Wu RY, Zheng YF, Lin XY, Mitchell P, Aung T, Saw SM. Prevalence and risk factors for refractive errors in Indians: the Singapore Indian eye Study (SINDI). Invest Ophthalmol Vis Sci. 2011;52(6):3166–73.
Saw SM, Chan YH, Wong WL, Shankar A, Sandar M, Aung T, Tan DT, Mitchell P, Wong TY. Prevalence and risk factors for refractive errors in the Singapore Malay eye survey. Ophthalmology. 2008;115(10):1713–9.
Hashemi H, Khabazkhoob M, Jafarzadehpur E, Yekta AA, Emamian MH, Shariati M, Fotouhi A. High prevalence of myopia in an adult population, Shahroud, Iran. Optom Vis Sci. 2012;89(7):993–9.
Wickremasinghe S, Foster PJ, Uranchimeg D, Lee PS, Devereux JG, Alsbirk PH, Machin D, Johnson GJ, Baasanhu J. Ocular biometry and refraction in Mongolian adults. Invest Ophthalmol Vis Sci. 2004;45(3):776–83.
Saw SM, Gazzard G, Koh D, Farook M, Widjaja D, Lee J, Tan DT. Prevalence rates of refractive errors in Sumatra, Indonesia. Invest Ophthalmol Vis Sci. 2002;43(10):3174–80.
Mutti DO, Zadnik K. Age-related decreases in the prevalence of myopia: longitudinal change or cohort effect? Invest Ophth Vis Sci. 2000;41(8):2103–7.
Pan CW, Cheng CY, Saw SM, Wang JJ, Wong TY. Myopia and age-related cataract: a systematic review and meta-analysis. Am J Ophthalmol. 2013;156(5):1021–33.
Guo Y, Liu LJ, Xu L, Lv YY, Tang P, Feng Y, Meng L, Jonas JB: Visual impairment and spectacle use in schoolchildren in rural and urban regions in Beijing. Eur J Ophthalmol. 2014;24(2):258-64.
Ip JM, Rose KA, Morgan IG, Burlutsky G, Mitchell P. Myopia and the urban environment: findings in a sample of 12-year-old Australian school children. Invest Ophthalmol Vis Sci. 2008;49(9):3858–63.
Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32(1):3–16.
Wojciechowski R. Nature and nurture: the complex genetics of myopia and refractive error. Clin Genet. 2011;79(4):301–20.
Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379(9827):1739–48.
Northstone K, Guggenheim JA, Howe LD, Tilling K, Paternoster L, Kemp JP, McMahon G, Williams C. Body stature growth trajectories during childhood and the development of myopia. Ophthalmology. 2013;120(5):1064.
Guo Y, Liu LJ, Xu L, Lv YY, Tang P, Feng Y, Meng M, Jonas JB. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology. 2013;120(2):277–83.
Saw SM, Chua WH, Hong CY, Wu HM, Chia KS, Stone RA, Tan D. Height and its relationship to refraction and biometry parameters in Singapore Chinese children. Invest Ophthalmol Vis Sci. 2002;43(5):1408–13.
Saw SM, Shankar A, Tan SB, Taylor H, Tan DT, Stone RA, Wong TY. A cohort study of incident myopia in Singaporean children. Invest Ophthalmol Vis Sci. 2006;47(5):1839–44.
Tarczy-Hornoch K, Ying-Lai M, Varma R. Los Angeles Latino eye Study G: myopic refractive error in adult Latinos: the Los Angeles Latino eye Study. Invest Ophthalmol Vis Sci. 2006;47(5):1845–52.
Song E, Qian DJ, Wang S, Xu C, Pan CW. Refractive error in Chinese with type 2 diabetes and its association with glycaemic control. Clin Exp Optom. 2018;101(2):213–9.
Attebo K, Ivers RQ, Mitchell P. Refractive errors in an older population: the Blue Mountains eye Study. Ophthalmology. 1999;106(6):1066–72.
Wang Q, Klein BE, Klein R, Moss SE. Refractive status in the beaver dam eye Study. Invest Ophthalmol Vis Sci. 1994;35(13):4344–7.
Cheng CY, Hsu WM, Liu JH, Tsai SY, Chou P. Refractive errors in an elderly Chinese population in Taiwan: the Shihpai eye Study. Invest Ophthalmol Vis Sci. 2003;44(11):4630–8.
Hornbeak DM, Young TL. Myopia genetics: a review of current research and emerging trends. Curr Opin Ophthalmol. 2009;20(5):356–62.
Hashemi H, Khabazkhoob M, Iribarren R, Emamian MH, Fotouhi A. Five-year change in refraction and its ocular components in the 40- to 64-year-old population of the Shahroud eye cohort study. Clin Exp Ophthalmol. 2016;44(8):669–77.
He M, Kong X, Chen Q, Zeng Y, Huang Y, Zhang J, Morgan IG, Meltzer ME, Jin L, Congdon N. Two-year changes in refractive error and related biometric factors in an adult Chinese population. JAMA Ophthalmol. 2014;132(8):978–84.
Han X, Guo X, Lee PY, Morgan IG, He M. Six-year changes in refraction and related ocular biometric factors in an adult Chinese population. PLoS One. 2017;12(8):e0183364.
Shiroma H, Higa A, Sawaguchi S, Iwase A, Tomidokoro A, Amano S, Araie M. Prevalence and risk factors of pterygium in a southwestern island of Japan: the Kumejima Study. Am J Ophthalmol. 2009;148(5):766–71 e761.
Lim CY, Kim SH, Chuck RS, Lee JK, Park CY. Risk factors for pterygium in Korea: the Korean National Health and nutrition examination survey V, 2010-2012. Medicine. 2015;94(32):e1258.
Linke SJ, Steinberg J, Eddy MT, Richard G, Katz T. Relationship between minimum corneal thickness and refractive state, keratometry, age, sex, and. Left or right eye in refractive surgery candidates. J Cataract Refract Surg. 2011;37(12):2175–80.
Jonas JB, Xu L. Histological changes of high axial myopia. Eye. 2014;28(2):113–7.
Mimura T, Usui T, Yamagami S, Funatsu H, Noma H, Toyono T, Mori M, Amano S. Relationship between conjunctivochalasis and refractive error. Eye Contact Lens. 2011;37(2):71–8.
Chen T, Ding L, Shan G, Ke L, Ma J, Zhong Y. Prevalence and racial differences in pterygium: a cross-sectional study in Han and Uygur adults in Xinjiang, China. Invest Ophthalmol Vis Sci. 2015;56(2):1109–17.
Vitale S, Ellwein L, Cotch MF, Ferris FL 3rd, Sperduto R. Prevalence of refractive error in the United States, 1999-2004. Arch Ophthalmol. 2008;126(8):1111–9.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Science and Technology Pillar Program during the Twelfth Five-Year Plan Period sponsored by the Ministry of Science and Technology of China (Grant 2012BAI37B02). The funders had no role in the study design, data collection, analysis or preparation of the manuscript.
Availability of data and materials
Not applicable.
Author information
Authors and Affiliations
Contributions
MW analysed and interpreted the data and drafted the manuscript. JC, XP, ZY, and JZ assisted with the acquisition of the data. GS, LP, YZ, and JM designed the study. GS also helped develop the statistical method. JM revised the final manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the tenets of the Declaration of Helsinki. Ethics approval was received from the bioethics committee of the Institute of Basic Medical Sciences, the Chinese Academy of Medical Sciences. Written informed consent was obtained from every participant after a full explanation of the nature and possible consequences of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, M., Cui, J., Shan, G. et al. Prevalence and risk factors of refractive error: a cross-sectional Study in Han and Yi adults in Yunnan, China. BMC Ophthalmol 19, 33 (2019). https://doi.org/10.1186/s12886-019-1042-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-019-1042-0