
Abstract
Background
The PlusOptix photoscreeners (PlusOptix GmbH, Nuremberg, Germany) is used in many vision screening programs. The purpose of the present study was to further explore the accuracy of the PlusOptix A09 photoscreener in children with ametropia (myopia or hyperopia).
Methods
A total of 70 eyes (35 children) were prospectively included. Before administration with the cycloplegia treatment 1 % cyclopentolate hydrochloride, children underwent refraction measurement with the PlusOptix A09. A refraction was then performed after cycloplegia with either Retinomax hand-held or Nidek autorefractor before and after 3 years old, respectively.
Results
The median (interquartile range) age was 58 (18 to 86) months. The mean (SD) spherical equivalent differed between PlusOptix A09 and cycloplegic autorefraction (+0.54 [1.82] D vs +1.06 [2.04] D, p = 0.04). PlusOptix A09 refraction was positively correlated with cycloplegic autorefraction (r = 0.81, p < 0.001) with higher coefficient in myopic than in hyperopic children (r = 0.91, p = 0.0002 and r = 0.52, p = 0.01, respectively). The mean (SD) difference between PlusOptix A09 and cycloplegic autorefraction was higher with hyperopia than myopia (0.73 [1.34] vs 0.05 [0.66], p = 0.01). The proportion of children with < 1-D difference between cycloplegic and PlusOptix A09 refraction was 68.8 %, higher with myopia than hyperopia (90 % vs 54.5 %, p = 0.01).
Conclusion
The spherical equivalent value with non-cycloplegic PlusOptix A09 refraction is closer to that with cycloplegic autorefraction than non-cycloplegic autorefraction. The PlusOptix A09 photoscreener underestimated the hyperopia of 0.73 D and slightly overestimated myopia of 0.05 D. The PlusOptix A09 could be used for screening with higher accuracy in myopic than hyperopic children.
Similar content being viewed by others


Background
Whole-population screening of children younger than 5 years is applied in many countries. However, the procedures and details of vision screening are inconsistent worldwide. Some studies tended to use photorefraction for early detection of amblyopia risk factors in children’s vision screening. This screening approach was based on the evidence that noncycloplegic photorefraction had acceptable accuracy and advantages of speed and portability when compared with cycloplegic retinoscopy [1]. On the contrary, others regarded photorefraction without cycloplegia as unreliable because of poor accuracy and limited range of refractive errors [2].
A series of the PlusOptix photoscreeners (PlusOptix GmbH, Nuremberg, Germany) are newly designed photorefraction tools for vision screening in children are approved by the US Food and Drug Administration (FDA) as a refractor. There are some reports of the sensitivity and specificity of the PlusOptix S04 or S08 for detecting amblyopia risk factors [3–9]. The PlusOptix A08 had higher predictive values for refractive error than for strabismus screening, with sensitivity 88 and 52 %, respectively [3]. In a study of children 6–36 months old, the PlusOptix S08 photoscreener had high sensitivity (100 %) but low specificity (38.7 %) for detecting amblyopia risk factors as compared with retinoscopy [4]. In a study of 64 patients 2–19 years old, 70.2 % showed a significant difference between PlusOptix S04 without cycloplegia and cycloplegic retinoscopy of > 0.5 D [7].
The purpose of the present study was to further explore the accuracy of the PlusOptix A09 photoscreener in pediatric patients with ametropia (myopia or hyperopia).
Methods
The present study was approved by the medical ethics committee of Montpellier Hospital and was in accordance with the 1975 Declaration of Helsinki. We performed cycloplegic autorefraction only in patients with this indication. This is in accordance with article R. 1121–3 of French public health law (April 26, 2006). Written, informed consent was provided by the parents of the pediatric patients.
Study population
We prospectively included consecutive children 12 to 139 months (interquartile range [25–75 %] 18 to 86 months) examined in the ophthalmology department of Gui de Chauliac Hospital of Montpellier. Inclusion criteria were consulting for screening of refractive error or monitoring of strabismus or amblyopia. Children with organic amblyopia, history of congenital cataract, significant media opacities or retinopathy were excluded.
Refraction assessment
Three different autorefractors were used: autorefractors (Retinomax hand-held and Nidek ARK-530A) and the PlusOptix A09 distance photoscreener.
The portable Retinomax autorefractor was used with its front support for stabilizing the measurement and a vertical mark to determine the correct vertical position. The value of the sphere can be measured from – 18 to + 23 D in increments of 0.25D, and from 0 to + 12 D for the cylinder in increments of 0.25D.
The fixed Nidek ARK-530A autorefractor provides a measure of refraction every 0.3 s. The value of the sphere can be measured from – 30 to + 25 D in increments of 0.01 D, and from 0 to 12 D for the cylinder in increments of 0.01D. We considered the refraction valuable if at least 3 readings were obtained with Retinomax and Nidek ARK-530A with quality control value > 7. In the present analysis, we used the mean value provided by the autorefractor.
The PlusOptix A09 photoscreener was placed at a distance of one meter in front of the patient in a darkroom and operated by a trained nurse. The fixation target of the instrument was designed as a smile face on the camera. Once pressing the start button, the smile face was automatically lighted and a warble sound could be heard to draw the child’s attention to the camera. The children were asked to gaze at the nose of the smile face on the camera during the test. Then the camera was moved slightly (within 50 mm) until green circles were evident around both pupils on the monitor screen, which was followed by automatic measurement. The results were displayed on the monitor. The PlusOptix A09 photoscreener has a spherical and cylindrical range of −7.0 to +5.0 D in increments of 0.25 D. If the spherical equivalent (SE) is out of the range, the measurement value only displays “Hyperopia” or “Myopia”. Ocular misalignment ≥10° could not be measured binocularly, and was changed to a sequential monocular measurement mode. Each patient was tested twice and the average value was the final result.
Study protocol
Before cycloplegia treatment, all children underwent refraction measurement with the PlusOptix A09 and an autorefractor depending on the age of the patient (Retinomax hand-held before 3 years and Nidek autorefractor after 3 years). Measurements with a autorefractor were also performed after administration of 1 % cyclopentolate hydrochloride.
Cycloplegia
Cycloplegia treatment with 1 % cyclopentolate hydrochloride was used according to the following protocol: 1 drop every 0, 5 and 10 min and refraction measured 45 to 60 min after the first drop.
Statistical analysis
We first compared the mean (SD), medians and the interquartile ranges of spherical equivalence between the right and left eyes. Myopia and hyperopia gold standards were defined by cycloplegic autorefraction. Paired t tests were used to compare spherical equivalents, sphere, cylinder, axis and anisometropia before and after cycloplogia. The Bonferroni correction was used to correct p-values of the main comparison of spherical equivalent between non-cycloplegic photorefraction PlusOptix and cycloplegic refraction. Pearson coefficients were used to correlate refraction values. The Bland-Altman method was used to assess the difference in refraction with the PlusOptix A09 and cycloplegic autorefraction. The mean difference and difference in means between PlusOptix A09 and cycloplegic autorefraction were plotted. SAS 9.4 (SAS Inst., Cary, NC) was used for data analysis. Significance was set at P < 0.05.
Results
Population characteristics
We initially examined 35 children; 3 were excluded from the analysis because the PlusOptix A09 measurement failed (hyperopia = 10 D for n = 1 and excessive mydriasis for n = 2). All patients underwent non-cycloplegic and cycloplegic autorefraction. The 32 children included 16 boys; the median (interquartile range) age was 58 months (18–86) months (11 children < 3 years old and 21 children > 3 years old). Most children consulted for follow-up for refractive error (75 %) or for monitoring amblyopia (15.6 %) or strabismus (9.4 %). After cycloplegia, 14 children were myopic and 18 hyperopic.
Values for right and left eyes did not differ for spherical equivalents with the non-cycloplegic autorefraction, PlusOptix A09 and cycloplegic autorefraction (p = 0.16, p = 0.55 and p = 0.21, respectively). Therefore, the right eye was used for all analyses.
Comparison of spherical equivalents between non-cycloplegic autorefraction, PlusOptix A09 and cycloplegic autorefraction
Mean (SD) spherical equivalents differed between non-cycloplegic autorefraction and the PlusOptix A09 (−0.70 [3.14] vs 0.54 [1.82] D, p = 0.02), between spherical equivalents with the PlusOptix A09 and cycloplegic autorefraction (0.54 [1.82] vs 1.06 [2.04] D, p = 0.04) and between spherical equivalents with the non-cycloplegic autorefraction and cycloplegic autorefraction (−0.70 [3.14] vs 1.06 [2.04] D, p = 0.004, Table 1).
Comparison of sphere, cylinder and axis among non-cycloplegic autorefraction, PlusOptix A09 and cycloplegic autorefraction
As shown in Table 1, we observed significant differences in mean sphere, cylinder and axis values between non-cycloplegic autorefraction (−0.02 D, −1.16 D and 72.75°, respectively), PlusOptix A09 (+1.27 D, −1.46 D and 84.41°, respectively) and cycloplegic autorefraction (+1.77 D, −1.41 D and 73.50°, respectively). Sphere values were significant between non-cycloplegic autorefraction and PlusOptix A09 (p = 0.007) and between PlusOptix A09 and cycloplegic autorefraction (p = 0.044). All comparisons concerning cylinder and axes were not statistically significant among non-cycloplegic, PlusOptix and cycloplegic autorefraction.
Anisometropia observed with each refraction method
The frequency of anisometropia > 1 D for PlusOptix A09, non-cycloplegic and cycloplegic autorefraction was 15.63, 37.50 and 12.50 %, respectively. Anisometropia differed between PlusOptix A09 and cycloplegic autorefraction (p = 0.04) and between non-cycloplegic and cycloplegic autorefraction (p = 0.005).
Comparison of difference (PlusOptix A09 – cycloplegic autorefraction) between myopic and hyperopic children
The mean (SD) difference in spherical equivalents between PlusOptix A09 and cycloplegic autorefraction was higher for hyperopic than myopic children (0.73 [1.34] vs 0.05 [0.66], p = 0.01) (Table 2). The proportion of children with < 1-D difference between cycloplegic and PlusOptix A09 refraction was 68.8 %, higher with myopia than hyperopia (90 % vs 54.5 %, p = 0.01).
Correlation between PlusOptix A09 and autorefraction
Figure 1 shows the correlation between non-cycloplegic photorefraction with PlusOptix A09 and cycloplegic autorefraction (r = 0.81, p < 0.001); the correlation between non-cycloplegic photorefraction with PlusOptix A09 and non-cycloplegic autorefraction (r = 0.70, p < 0.001); and the correlation between non-cycloplegic autorefraction and cycloplegic autorefraction (r = 0.77, p < 0.001).

Correlation between autorefractor and PlusOptix A09. Top left graph: Correlation between non-cycloplegic autorefraction with PlusOptix A09 and cycloplegic autorefraction with a autorefractor (r = 0.81, p < 0.001); top right graph: non-cycloplegic autorefraction with PlusOptix A09 and with autorefractor (r = 0.70, p < 0.001), down left graph non-cycloplegic autorefraction and cycloplegic autorefraction (r = 0.77, p < 0.001)
Bland-Altman analysis
Between PlusOptix A09 and cycloplegic autorefraction
The mean (SD) difference between the PlusOptix A09 and cycloplegic autorefraction was 0.52 [1.82] D. The mean difference and difference in means did not differ between PlusOptix A09 and cycloplegic autorefraction (r = 0.19; p = 0.31) (Fig. 2 top left graph), so the difference (cycloplegic autorefraction minus PlusOptixA09) did not increase in extreme values. The 95 % limits of agreement according to the Bland-Altman definition was from −1.55D to +3.15D.

Bland and Altman analysist. Top left graph: Correlation between the mean difference and difference in means between non-cycloplegic autorefraction with PlusOptix A09 and cycloplegic autorefraction (r = 0.19; p = 0.31), red curve: bias (mean difference between the measures = 0.52, blue curves: limit of agreements [−1.55 to +3.15 D]; top right graph: Correlation between the mean difference and difference in means between PlusOptix A09 refraction and non-cycloplegic autorefraction (r = −0.58; p = 0.0005), red curve: biais (mean difference between the measures = 1.24, blue curves: limit of agreements [−4.94 to 4.79 D]; down left graph: Correlation between the mean difference and difference in means between non-cycloplegic autorefraction and cycloplegic autorefraction (r = −0.51; p = 0.0029), red curve: bias (mean difference between the measures = 1.75, blue curves: limit of agreements [−4.42 to 4.79 D]
Between PlusOptix A09 refraction and non-cycloplegic autorefraction
The mean (SD) difference between the PlusOptix A09 and non-cycloplegic autorefraction was 1.24 (2.48) D. The mean difference and difference in means differed between PlusOptix A09 and non-cycloplegic autorefraction (r = −0.58; p = 0.0005) (Fig. 2 top right graph), so the difference (non-cycloplegic autorefraction minus PlusOptixA09) was increased in extreme values. The 95 % limits of agreement according to the Bland-Altman definition was from −4.94 to 4.79 D, but they are not statistically valuable because of a significant r correlation coefficient.
Between non-cycloplegic autorefraction and cycloplegic autorefraction
The mean (SD) difference between non-cycloplegic and cycloplegic autorefraction was 1.75 (1.82) D. The mean difference and difference in means differed between non-cycoplegic and cycloplegic autorefraction (r = −0.51; p = 0.0029) (Fig. 2 down left graph), so the difference (non-cycloplegic autorefraction minus cycloplegic autorefraction) was increased in extreme values. The 95 % limits of agreement according to the Bland-Altman definition was from −4.42 to 4.79D, but they are not statistically valuable because of a significant r correlation coefficient.
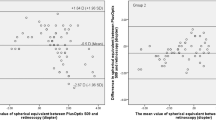
Correlation between PlusOptix A09 and cycloplegic autorefraction in myopic and hyperopic children
Overall the PlusOptix A09 refraction was positively correlated with cycloplegic autorefraction with higher coefficient in myopic than in hyperopic children (r = 0.91, p = 0.0002 and r = 0.52, p = 0.01, respectively) (Fig. 3).

Correlation between non-cycloplegic autorefraction with PlusOptix A09 and cycloplegic autorefraction among myopic and hyperopic children: left graph: in myopic children (r = 0.91, p = 0.0002), right graph: in hyperopic children (r = 0.52, p = 0.01)
Discussion
The present study provides additional information regarding the performance of the PlusOptix A09 photoscreener in children. The accuracy of the PlusOptix A09 is higher in myopic than hyperopic children and the proportion of children with < 1-D difference between cycloplegic autorefraction and PlusOptix A09 was higher for myopic than hyperopic children.
Studies of diagnostic performance of PlusOptix have found sensitivity 98 to 99 %, specificity 82 to 88 % [10, 11]. With its high sensitivity and acceptable specificity, the PlusOptix A09 can be used in a general screening programs. In myopia screening programs among children ≥ 4 years old, long-distance visual acuity could be used instead of refraction measurement. The benefit of using PlusOptix A09 is to obtain an estimation of severity of myopia [12]. Schimitzek and Lagrèze showed that the mean difference in values between the cycloplegic autorefraction and the photorefractor was 0.73; the spherical equivalent tended to be underestimated because of uncontrolled accommodation in children [13]. In the present study, the non-cycloplegic photorefraction with the PlusOptix A09 was closer to cycloplegic autorefraction than with autorefractors. Non-cycloplegic refraction has lower agreement than use of the PlusOptix A09 because we found a significant correlation between the mean difference and the difference in means between non-cycloplegic and cycloplegic autorefraction. Thus there are more “errors” in extreme values for non-cycloplegic than PlusOptix A09 as compared with cycloplegic autorefraction. We also found an underestimation of the spherical equivalents measured with the PlusOptix A09 as compared with cycloplegic autorefraction but with a smaller difference than in the study performed by Schimitzek et al. (0.52 vs 0.73, respectively). Our result differed from Schimitzek et al. probably because of the younger age of our patients as compared with those in the Schimitzek et al. study (58 months vs. 43 years).
In the present study, the PlusOptix A09 is revealed to have a general trend towards myopic values which is in accordance with previous reports of the PlusOptix photoscreeners [5, 14]. Nevertheless, the diopters shifting to myopia were variable in different reports. Moghaddam et al. [4], reported that the mean difference of SE measured between the PlusOptix and via retinoscopy was 0.16 D on children aged 6 months to 3 years. Erdurmus’s study [15] included a cohort of healthy children (age: 7.1 ± 2.4 years (mean ± SD); range, 9 months to 14 years) and showed that the difference of SE between the PlusOptix and cycloplegic retinoscopy was 0.70 D. Dahlmann-Noor et al. [16], recruited 126 children with a mean age of 5.5 years attending hospital-based pediatric eye service to their study, and confirmed a myopic shift of 1.90 D. The working distance of the PlusOptix A09 is 1.0 m, so stimulation to accommodate does not occur in patients with myopia ≥ −1.0 D because the far point is ≤ 1.0 m. For patients with myopia ≤ −1.0 D, those with emmetropia or hyperopia may accommodate exactly onto the target, and the device will detect a SE = −1.0 D regardless of the real ametropia. Thus, in the present study, a separated analysis was performed between myopic and hyperopic children. The PlusOptix A09 photoscreener underestimated the hyperopia of 0.73 D and slightly overestimated myopia of 0.05 D.
Rajavi et al. [17], and Erdurmus et al. [15], studied the relationship between the PlusOptix photoscreener and cycoplegic retinoscopy by means of Pearson correlation. The accuracy of the PlusOptix photoscreener was controversial because the refractive result of the PlusOptix was not consistent with that of cycloplegic retinoscopy [16, 18]. In the present study, we found that linear regression had significant correlation between the PlusOptix photoscreener and cycoplegic refraction with higher coefficient in myopic than in hyperopic children.
Comparison between Retinomax and Nidek was not the aim of this study. Of note, a previous study found that non-cycloplegic Retinomax values were significantly lower than 0.80 D as compared with Nidek values [2].
The limitations of the present study include the low number of children. The paucity of high hyperopes in our study limits the generalization of our conclusions in this high risk of amblyopia population. Also since the subjects involved were patients attending our eye department, the results may be affected by a higher prevalence of eye diseases than those in a healthy population. A population based large-scale photorefraction in a normal child population is underway to further substantiate the results obtained herein. However, the new information comparing myopic and hyperopic children is of interest for users of PlusOptix A09.
Conclusion
We found that PlusOptix A09 gives closer values for cycloplegic autorefraction than non-cycloplegic autorefraction. The accuracy of the PlusOptix A09 is higher in myopic than hyperopic children. Distance refraction can constitute a tool for screening or follow up that have higher values than non-cycloplegic autorefraction Retinomax/Nidek. However it cannot replace cycloplegic autorefraction for first-spectacle correction and during strabismus or amblyopia management.
References
Cordonnier M, Kallay O. Non-cycloplegic screening for refractive errors in children with the hand-held autorefractor Retinomax: final results and comparison with non-cycloplegic photoscreening. Strabismus. 2001;9(2):59–70.
Cordonnier M, Dramaix M. Screening for refractive errors in children: accuracy of the hand held refractor Retinomax to screen for astigmatism. Br J Ophthalmol. 1999;83(2):157–61.
Bloomberg JD, Suh DW. The accuracy of the plusoptiX A08 photoscreener in detecting risk factors for amblyopia in central Iowa. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2013;17(3):301–4. doi:10.1016/j.jaapos.2013.03.014.
Moghaddam AAS, Kargozar A, Zarei-Ghanavati M, Najjaran M, Nozari V, Shakeri MT. Screening for amblyopia risk factors in pre-verbal children using the Plusoptix photoscreener: a cross-sectional population-based study. Br J Ophthalmol. 2012;96(1):83–6. doi:10.1136/bjo.2010.190405.
Paff T, Oudesluys-Murphy AM, Wolterbeek R, et al. Screening for refractive errors in children: the plusoptiX S08 and the Retinomax K-plus2 performed by a lay screener compared to cycloplegic retinoscopy. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2010;14(6):478–83. doi:10.1016/j.jaapos.2010.09.015.
Matta NS, Arnold RW, Singman EL, Silbert DI. Comparison between the plusoptiX and MTI Photoscreeners. Arch Ophthalmol Chic Ill 1960. 2009;127(12):1591–5. doi:10.1001/archophthalmol.2009.294.
Ayse YK, Onder U, Suheyla K. Accuracy of Plusoptix S04 in children and teens. Can J Ophthalmol J Can Ophtalmol. 2011;46(2):153–7.
Matta NS, Singman EL, Silbert DI. Performance of the Plusoptix vision screener for the detection of amblyopia risk factors in children. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2008;12(5):490–2. doi:10.1016/j.jaapos.2008.04.004.
Arthur BW, Riyaz R, Rodriguez S, Wong J. Field testing of the plusoptiX S04 photoscreener. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2009;13(1):51–7. doi:10.1016/j.jaapos.2008.08.016.
Silbert D, Matta N, Tian J, Singman E. Comparing the SureSight autorefractor and the plusoptiX photoscreener for pediatric vision screening. Strabismus. 2014;22(2):64–7. doi:10.3109/09273972.2014.904896.
Matta NS, Singman EL, Silbert DI. Performance of the plusoptiX S04 photoscreener for the detection of amblyopia risk factors in children aged 3 to 5. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2010;14(2):147–9. doi:10.1016/j.jaapos.2010.01.006.
Wang X, Yi H, Lu L, et al. Population prevalence of need for spectacles and spectacle ownership among urban migrant children in Eastern China. JAMA Ophthalmol. 2015;133(12):1399–406. doi:10.1001/jamaophthalmol.2015.3513.
Schimitzek T, Lagrèze WA. Accuracy of a new photo-refractometer in young and adult patients. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Für Klin Exp Ophthalmol. 2005;243(7):637–45. doi:10.1007/s00417-004-1056-y.
Mirzajani A, Heirani M, Jafarzadehpur E, Haghani H. A comparison of the Plusoptix S08 photorefractor to retinoscopy and cycloretinoscopy. Clin Exp Optom. 2013;96(4):394–9. doi:10.1111/cxo.12063.
Erdurmus M, Yagci R, Karadag R, Durmus M. A comparison of photorefraction and retinoscopy in children. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2007;11(6):606–11. doi:10.1016/j.jaapos.2007.04.006.
Dahlmann-Noor AH, Comyn O, Kostakis V, et al. Plusoptix Vision Screener: the accuracy and repeatability of refractive measurements using a new autorefractor. Br J Ophthalmol. 2009;93(3):346–9. doi:10.1136/bjo.2008.138123.
Rajavi Z, Parsafar H, Ramezani A, Yaseri M. Is noncycloplegic photorefraction applicable for screening refractive amblyopia risk factors? J Ophthalmic Vis Res. 2012;7(1):3–9.
Dahlmann-Noor AH, Vrotsou K, Kostakis V, et al. Vision screening in children by Plusoptix Vision Screener compared with gold-standard orthoptic assessment. Br J Ophthalmol. 2009;93(3):342–5. doi:10.1136/bjo.2008.138115.
Availability of data and materials
I had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Authors’ contributions
AP participated in the design of the study and drafted the manuscript and gave final approval of the version to be published. CME performed refraction assessment and acquisition of data and gave final approval of the version to be published. VT performed acquisition of data and gave final approval of the version to be published. MV performed acquisition of data and gave final approval of the version to be published. VD participated in the design of the study and drafted the manuscript and gave final approval of the version to be published.
Competing interests
The authors declare that they have no competing interests.
Consent to publish
All authors read and approved the final manuscript and agreed for publication.
Ethics and consent to participate
The present study was approved by the medical ethics committee of Montpellier Hospital and was in accordance with the 1975 Declaration of Helsinki. We performed cycloplegic autorefraction only in patients with this indication. This is in accordance with article R. 1121–3 of French public health law (April 26, 2006). Written, informed consent was provided by the parents of the pediatric patients.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Payerols, A., Eliaou, C., Trezeguet, V. et al. Accuracy of PlusOptix A09 distance refraction in pediatric myopia and hyperopia. BMC Ophthalmol 16, 72 (2016). https://doi.org/10.1186/s12886-016-0247-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-016-0247-8