
Abstract
Background
Poor cancer prognosis has been observed in patients with pre-existing psychiatric disorders. Therefore, we need better knowledge about the diagnosis of cancer in this patient group. The aim of the study was to describe the routes to cancer diagnosis in patients with pre-existing psychiatric disorders and to analyse how cancer type modified the routes.
Methods
A register-based cohort study was conducted by including patients diagnosed with incident cancer in 2014–2018 (n = 155,851). Information on pre-existing psychiatric disorders was obtained from register data on hospital contacts and prescription medication. Multinomial regression models with marginal means expressed as probabilities were used to assess the association between pre-existing psychiatric disorders and routes to diagnosis.
Results
Compared to patients with no psychiatric disorders, the population with a psychiatric disorder had an 8.0% lower probability of being diagnosed through cancer patient pathways initiated in primary care and a 7.6% higher probability of being diagnosed through unplanned admissions. Patients with pre-existing psychiatric disorders diagnosed with rectal, colon, pancreatic, liver or lung cancer and patients with schizophrenia and organic disorders were less often diagnosed through cancer patient pathways initiated in primary care.
Conclusion
Patients with pre-existing psychiatric disorders were less likely to be diagnosed through Cancer Patient Pathways from primary care. To some extent, this was more pronounced among patients with cancer types that often present with vague or unspecific symptoms and among patients with severe psychiatric disorders. Targeting the routes by which patients with psychiatric disorders are diagnosed, may be one way to improve the prognosis among this group of patients.
Similar content being viewed by others


Background
Each year, more than 40,000 Danes are diagnosed with cancer which also is the leading cause of death in Denmark [1, 2]. The prognosis after cancer has previously been reported to be strongly associated with the patient’s Route to Diagnosis (RtD). Across cancer types, patients presenting through an emergency route have displayed inferior prognosis compared to patients beginning their diagnostic trajectory in primary care, e.g. through urgent referrals to secondary care like the two-week wait (TWW) in the United Kingdom or a Cancer Patient Pathway (CPP) in Scandinavia [3, 4]. In Denmark, more than 75% of all cancer patients begin the diagnostic process by presenting symptoms in primary care [5], and 45% are diagnosed after referral to a CPP [6].
The prevalence of psychiatric disorders is around 8–30% in the general population, depending on the included disorders and timeframe [7,8,9]. Patients with psychiatric disorders have a reduced life expectancy of up to 20 years compared to the general population [10, 11]. This excess mortality has been linked with several factors, e.g. lifestyle, social issues, adverse medication effects, healthcare provision, suicide risk and comorbidity [10, 12, 13] and challenges have also been reported across the entire spectrum of cancer care, from symptom presentation to end-of-life care [13,14,15,16]. Inferior cancer prognosis has been reported in patients with psychiatric disorders [14, 17,18,19] and suboptimal diagnostic process in this patient group has been highlighted as a possible explanation [10, 20] including underdetection, delayed diagnosis and lower screening uptake [14, 21,22,23,24]. To our knowledge, only limited research has explored the RtD among cancer patients with pre-existing psychiatric disorders [25].
Further attention is warranted on the diagnostic process in cancer patients with psychiatric disorders [10, 14]. A starting point could be to study how this patient group enters the diagnostic pathway, and whether specific subgroups are particularly challenged by less favourable diagnostic trajectories (defined here as lower referral to primary care initiated CPP and higher rates of unplanned admissions as this have been linked with worse prognosis after cancer [3, 6]). We hypothesised that patients with pre-existing psychiatric disorders were more often diagnosed through less favourable routes than patients without psychiatric disorders. We also hypothesised that some subgroups of patients with psychiatric disorders, e.g. schizophrenia, would more often present through unplanned admission compared to patients with other subtypes of psychiatric disorders. Finally, we hypothesised that the association between pre-existing psychiatric disorders and RtD would vary between cancer types.
Methods
Aim and design
The aim of the study was to describe the Routes to Diagnosis of cancer among patients with pre-existing psychiatric disorders and to analyse how cancer type modified the routes. This was studied by conducting a national cohort study using national register-based data in Denmark.
Setting
Denmark has a population of 5.8 million inhabitants, and 98% of the population is listed with a general practice clinic. The healthcare system is based on free and equal access to most medical services, which are funded by tax revenues. The general practitioner (GP) serves as gatekeeper to secondary care [26] and can refer patients to one of the 30 existing CPPs covering approximately 40 different cancer diseases implemented between 2008 and 2010. If relevant, the GP can also refer to other diagnostic services at the hospital or at private specialist clinics. National screening programmes exist for cervical cancer, colorectal cancer and breast cancer [27, 28].
Study population
The study population was defined as patients aged 18 years or older with a first-time cancer, excluding non-melanoma skin cancer (International Classification of Diseases, 10th version (ICD-10): C44), recorded in the Danish Cancer Registry [29] between 1 January 2014 and 31 December 2018. In total, 159,189 patients were identified. The final study population comprised 155,851 patients (97.9%) after exclusion of patients with no registration on sex (n = 1391) or age (n = 798), patients who had migrated within 10 years prior to the cancer diagnosis (n = 534), patients registered with multiple cancer types on the same date of diagnosis (n = 446) and male patients with breast cancer (as no specific route could be assigned to this group) (n = 169).
Data collection
The data was collected from the national registers and clinical databases described below. We used the unique civil registration number assigned to all Danish citizens to link data between registers at the individual level [30].
Definition of routes to diagnosis (RtD)
Danish registers have no systematically collected data on RtD for cancer. Thus, an algorithm developed by Danckert B et al. [6] was used to assign each included patient with a RtD. The algorithm used national register data to identify the most likely RtD based on the patient’s contacts in the healthcare system in the time leading up to the cancer diagnosis. The following registers provided the basis for the defined RtD. The Danish Cancer Registry provided information on cancer type and whether the patient was diagnosed by death certificate only (DCO). The Danish National Patient Registry (DNPR) [31] provided data on all contacts with somatic hospitals in Denmark, including information on inpatient and outpatient visits, dates, department codes and CPP registrations from both primary and secondary care (both from the private and public sector). Three clinical databases the Danish Breast Cancer Group [32], the Danish Colorectal Cancer Database [33] and the Danish Quality Database for Cervical Cancer Screening [34], provided information on screening for breast, colorectal and cervical cancer. Finally, the Danish Register of Causes of Death [35] provided information of vital status and date of death.
Eight mutually exclusive routes were identified: 1) death certificate only (DCO) in which only the death certificate provided information on the diagnosis, 2) screening in which the patient was diagnosed with breast cancer, colorectal cancer or cervical cancer detected in a national screening programme, 3) CPP – primary care in which the patient was diagnosed after CPP referral by a healthcare professional in primary care within 90 days of the diagnosis and no registration of screening detection, 4) CPP – secondary care in which the patient was diagnosed after CPP referral by a healthcare professional in secondary care, such as a medical specialist in a hospital within 90 days of the diagnosis and no previous registration of CPP from primary care or screening detection, 5) unplanned admission in which the patient had an inpatient hospital admission coded as acute within 30 days before the cancer diagnosis and no prior CPP initiation or screening detection, i.e. comprising both patients admitted through emergency and patients admissions which was not scheduled or planned, 6) planned admission (elective) for other reasons than cancer within 30 days before the cancer diagnosis and no prior CPP initiation or screening detection, 7) outpatient visit (outpatient hospital specialist clinic) within 30 days before the cancer diagnosis and no prior CPP initiation, planned admission or screening detection and 8) unknown when no specific route could be assigned to the patient based on the existing data.
Definition of pre-existing psychiatric disorders
Data on pre-existing psychiatric disorders was obtained from the Danish Psychiatric Central Research Register (PCRR), which holds information on inpatient, outpatient and emergency contacts to all psychiatric hospitals in Denmark since 1970 [36]. To ensure inclusion of all registered psychiatric disorders, diagnosis codes were also searched in the DNPR. The following groups of pre-existing psychiatric disorders were included: organic disorders (ICD-10: F00-F09), substance use disorders (ICD-10: F10-F19), schizophrenia and psychotic disorders (ICD-10: F20-F29), mood disorders (ICD-10: F30-F39), anxiety disorders (ICD-10: F40-F41) and stress disorders (ICD-10: F43). Further, data on prescription medication was obtained from the Danish National Prescription Registry [37]. We included the variable “prescription-based mental disorders”, which was defined as individuals who had been prescribed antidepressants (Anatomical Therapeutic Chemical (ATC): N06A), anxiolytics (ATC: N05B) or antipsychotics (ATC: N05A) at least two times within 1 year of the cancer diagnosis date and had no registrations in any of the other included subgroups. This subgroup was included to describe patients with pre-existing psychiatric disorders treated mainly in primary care.
Covariates
The following variables were assessed as potential confounders. Sex and age were obtained from the Danish Civil Registration System. Age was categorised in five groups: 18–49, 50–59, 60–69, 70–79 and 80+ years. The patient’s highest attained education in the year of diagnosis was defined according to the International Standard Classification of Education (ISCED) [38] and divided into short (≤10 years), medium (11–15 years) and long education (> 15 years). Ethnicity was divided into Danish and immigrant. Marital status was divided into married/cohabiting and living alone. Year of diagnosis and cancer type were defined based on registrations in the Danish Cancer Registry, and 23 types of cancer were defined (see Additional file 1 for overview). The patient’s burden of comorbidity was assessed by means of the Charlson’s Comorbidity Index (CCI) [39] (excluding cancer) based on diagnosis registrations in the DNPR for up to 10 years prior to the diagnosis. Comorbidity burden was categorised into none (CCI score of 0), low (CCI score of 1–2) and high (CCI score of ≥3). Region of residence was based on the five geographically defined areas in Denmark.
Statistical analyses
A descriptive overview of the RtD was provided by assessing the proportion of RtD, including 95% confidence intervals (CI), according to pre-existing psychiatric disorders and subgroups of psychiatric disorders.
Multinomial logistic regressions (MLRs) were performed to assess the RtD for patients with psychiatric disorders compared to those without. An unadjusted model is presented and followed by a model adjusted for sex, age, CCI, ethnicity, marital status, education, year of diagnosis, ethnicity and region of residence. Cluster robust standard errors were used to account for the effect of clustering of observations around cancer diagnoses. The results are presented as relative risk ratios (RRRs) with “CPP – primary care “as the reference (Table 3).
Stratified MLRs were conducted after an interaction test between cancer type, pre-existing psychiatric disorders and RtD. The cancer-specific analyses (Fig. 1) and the analyses based on subtypes of psychiatric disorders (Fig. 2) focused on two outcomes only: “CPP – primary care” and “unplanned admission”. They were chosen as the largest absolute difference in having a pre-existing psychiatric disorder were observed for these routes and because they also represented the poorest and the best prognosis among symptomatic cancer types [6]. The results are expressed as probabilities and are based on marginal means, which were computed with covariates at their observed value. The models were fully adjusted as described above, where each analysis for a specific subgroup of psychiatric disorders was additionally adjusted for the other subgroups of psychiatric disorders due to the risk of psychiatric comorbidity [40] . Robust variance estimates were included in all stratified analyses to allow for clustering of patients by general practice.
Sensitivity analyses were conducted when 1) the pre-existing psychiatric disorders included patients registered in the PCRR and the DNPR within 2 years of the diagnosis (instead of 5 years) and expanding to 10 year prior to the diagnosis, when 2) the assessment of psychiatric disorders were based on only registrations in the PCRR and the DNPR at 5 years prior the diagnosis, thus excluding the category “prescription based mental disorders”, and when 3) the analyses stratified on cancer type were also conducted without prescriptions as an indication for pre-existing psychiatric disorder.
Results
Descriptive data
The study population had a mean age of 66 years, and 48.5% were female. In total, 18.1% were registered with a pre-existing psychiatric disorder. The most common category was prescription-based mental disorders, which was followed by substance abuse disorders. The most common RtD was CPP through primary care and the rarest group was DCO. Unplanned admission comprised 15.5% of the routes (Table 1). In total, 82.7% of the unplanned admissions were due to unscheduled admission and 17.2% was due to emergency which was similar for patients with and without psychiatric disorders (18.0% vs 17.0%) (data not shown). The most common cancer types were breast, prostate and lung cancer (Table 1) (Additional file 1, part 1).
RtD among patients with pre-existing psychiatric disorders
Table 2 presents the proportions of RtD according to pre-existing psychiatric disorders. Diagnosis through a CPP initiated in primary care was seen for 45.7% for patients without and for 37.7% for patients with psychiatric disorders; the lowest percentage was observed for patients with organic disorders (31.9%). The proportion of diagnoses following unplanned admission was highest for patients with organic disorders (31.5%) and lowest for patients without psychiatric disorders (14.2%).
Patients with psychiatric disorders had higher risk of being diagnosed with cancer through DCO, CPP initiated in secondary care, unplanned admission, elective and outpatient care (relative to a CPP initiated in primary care) compared to the corresponding risk in patients without psychiatric disorders (Table 3). For example, patients with psychiatric disorders had a higher risk of presenting through an unplanned admission (relative to a CPP initiated in primary care) compared to patients without psychiatric disorders (RRR: 1.41, 95% CI 1.28–1.55). These estimates were largely comparable across different definitions of pre-existing psychiatric disorders (Additional file 1, part 3).
Cancer type and RtD for patients with pre-existing psychiatric disorders
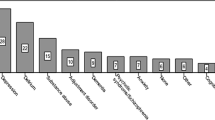
A test for interaction showed that the association between psychiatric disorders and RtD was statistically different across cancer types (p < 0.001). No major difference could be observed in the probability to be diagnosed through a CPP initiated in primary care between patients with and without psychiatric disorders for breast, melanoma, uterus, lymphoma, multiple myeloma, and head and neck cancer. In the sensitivity analysis, excluding prescription medication, the results were comparable, although with accentuated associations (Additional file 1, part 4).

Estimated* probabilities of patients presenting through a CPP in primary care and unplanned admission for each cancer type according to any pre-existing psychiatric disorders. *Adjusted for sex, age, year of diagnosis, comorbidity, education, ethnicity, cohabitation and region of residence
Subtypes of pre-existing psychiatric disorders and routes to diagnosis
The probability of being diagnosed through a CPP initiated in primary care or an unplanned admission varied for subtypes of psychiatric disorders (Fig. 2). The lowest probability of being diagnosed through a CPP initiated in primary care was observed among patients with schizophrenia (41.9, 95% CI: 38.8–45.1) and patients with organic disorders (43.6, 95% CI: 41.8–45.4). These two groups also had the highest probability of being diagnosed after an unplanned admission. Patients with stress disorders had a higher probability (although not statistically significant) of being diagnosed after a CPP referral from primary care compared to patients with no psychiatric disorders also after adjustments of other psychiatric disorders.

Estimated* probabilities of patients presenting through CPP - primary care and unplanned admission according to subgroups of pre-existing psychiatric disorders. Abbreviation: no = no pre-existing psychiatric disorder, schizophrenia = schizophrenia and psychotic disorders, Prescription: prescription-based mental disorders. *Adjusted for sex, age, year of diagnosis, comorbidity, education, ethnicity, cohabitation, region of residence, cancer diagnosis and for each of the other subgroups of pre-existing psychiatric disorders. The grey line represents the probability of each route for patients with no pre-existing psychiatric disorders
Discussion
Main findings
Patients with pre-existing psychiatric disorders had a statistically significantly lower probability of being diagnosed through a CPP initiated in primary care and a higher probability of being diagnosed after an unplanned admission compared to patients without psychiatric disorders. This was most pronounced for patients with rectal, colon, pancreatic, liver or lung cancer and for patients with schizophrenia or organic disorders. The RtD did not differ for patients with stress disorders compared to those with no psychiatric disorders, and no differences were seen for breast and melanoma cancer.
Strengths and limitations
The main strengths of this study was the population-based design and the use of national registers from both the public and private sector with high data validity and almost complete coverage of the Danish population [29, 31, 41]. This minimised the risk of selection bias and information bias. The algorithm for RtD was developed in an international collaboration and modified to fit the Danish healthcare system. Comparing the Danish algorithm to data from England, the Danish algorithm performed similar with expected variations across cancer types (see also [6]). Embedded timeframes constitute an assumption of the algorithm, e.g. information on CPP referral was assessed for up to 90 days before a diagnosis. Patients with psychiatric disorders may be more likely to experience long diagnostic intervals [23] and thus more susceptible to misclassification by the algorithm, e.g. by initiation of a CPP more than 3 months prior to the diagnosis. The underlying reason for unplanned admission is not transparent within the data, and the registered contact could be caused by other reasons than cancer, e.g. injury. Thus, the definition of RtD is defined contextually as opposed to based on the particular medical condition, yet, RtD is accepted as a relevant clinical marker for severity due to the poorer prognosis among patients diagnosed following an unplanned admission [3, 6]. The distribution of unplanned contacts caused by an emergency was similar in patients with and without psychiatric disorders (17 vs 18%, see result section). This could indicate that the higher probability of unplanned admission among patients with psychiatric disorders was not caused primarily by this group’s risk of e.g. injury or substance related emergencies [10, 14].
The large study population allowed us to stratify the analyses on both cancer types and subgroups of psychiatric disorders. However, overlaps were seen in the confidence intervals, particularly for unplanned admissions, which may have been related to low power for some of the cancer types.
The definition of pre-existing psychiatric disorders was based on previous work [24, 42, 43], as no standardised or internationally accepted method exists to assess general psychiatric disorders based on register data, and many psychiatric disorders are treated in primary care without hospital involvement. The inclusion of prescription medication made it possible to assess the impact on RtD from both psychiatric disorders that required involvement of a psychiatric department in secondary care and those primarily treated in general practice (and therefore no diagnosis was registered in the PCRR). However, it is not possible to determine the indication for prescription from the Danish National Prescription Registry, and it cannot be excluded that some of the included prescriptions were based on pre-diagnostic cancer symptoms such as inflammation rather than the psychiatric disorder. Sensitivity analysis, were prescription medication were excluded, did however not change the results markedly neither when different time frames were used. This indicates robust findings regardless of the definition used.
The stratified analysis focused primarily on CPP from primary care and unplanned admissions as research have found substantial difference in the cancer prognosis in these groups [3, 6]. However, the proportions of higher DCO in patients with psychiatric disorders were also interesting. Yet, due to a low sample in this group (n < 800), the analysis stratified on psychiatric subgroups would entail low statistical precision (e.g. with only 55 patients with anxiety and diagnosed through DCO).
Results compared with existing literature
Previous studies have found that patients with dementia have higher probability of presenting as emergency [25]. To our knowledge, no studies have assessed the association between different pre-existing psychiatric disorders and RtD. For most of the assessed subtypes of psychiatric disorders, particularly severe disorders, the patients entered the diagnostic pathway more often through unplanned admissions and less often through CPPs from primary care even after adjustments psychiatric comorbidity. These results confirm the hypothesis of this study, but the explanations are likely to be complex. At the personal level, several factors in patients with psychiatric disorders may challenge the diagnostic process, including a lifestyle with high alcohol and substance abuse [44], little awareness of physical symptoms and difficulty comprehending messages from healthcare providers due to cognitive deficits [13, 15]. Feeling of hopelessness in depressed individuals has also been related to less motivation to act in general [15], which could delay healthcare seeking when experiencing symptoms. Further, research has found that patients with schizophrenia often experience healthcare discrimination, which may discourage these patients to seek care [13, 14]. Finally, acute challenges, such as delirium or psychosis, may challenge the diagnostic workup [14]. At the provider level, it has been proposed that symptoms from the psychiatric disorder can mask physical symptoms [14, 23], which in turn could delay or reduce the GP’s referral propensity. Finally, at the system level, research has found inferior quality of healthcare provided for patients with psychiatric disorders and challenges in coordinating care between healthcare sectors, which may lead to fragmented care for patients with severe mental disorders [12, 13]. Combinations of these factors may partially explain the higher risk of a less favourable RtD in patients with severe psychiatric disorders. One exception was patients with a stress disorder, who had a similar probability of being diagnosed through a CPP initiated in primary care or an unplanned admission as that of patients with no psychiatric disorders. This indicates that this subgroup of psychiatric disorders may differ from the other subgroups in terms of help-seeking and referral from primary care.
The results indicate that variations exist between cancer types in terms of the association between psychiatric disorders and RtD. We found that cancer types that are more likely to be diagnosed through a CPP initiated in primary care (e.g. breast cancer, melanoma), i.e. the so-called easy-to-diagnose cancer types [45, 46], showed fewer variations in RtD according to psychiatric disorders. Reversely, for more of the cancer types that are less likely to be diagnosed through a CPP initiated in primary care (e.g. pancreatic, lung, liver cancer), i.e. the so-called hard-to-diagnose cancer types [45, 46], we found a statistically significantly lower probability of being diagnosed through a CPP initiated in primary care in patients with psychiatric disorders compared to other patients. To some extent, these differences could be explained by the typical symptom presentation for these cancer types, which seems to be amplified in individuals with psychiatric disorders. The cancer types that are difficult to diagnose, e.g. due to unspecific symptom presentation, may also challenge the diagnostic work-up at individual, provider and system levels, which may result in lower recognition of bodily sensations, lower referral propensity and more acute presentations among patients with psychiatric disorders.
Implications
In studies on cancer in general, low likelihood of being diagnosed after referral from primary care to an urgent cancer pathway and high likelihood of being diagnosed after an acute or emergency presentation have been linked with poor prognosis [3, 4]. Similar patterns were observed for patients with psychiatric disorders in this study, thus, based on this study, it could be hypothesised that focusing on the route to cancer diagnosis among patients with psychiatric disorders could be one strategy to improve the cancer survival in this group. Further research are also needed with particular focus of cancer diagnostics in primary care among patients with psychiatric disorders, as most cancer pathways is initiated in the primary sector [5] where challenges have been reported in the diagnostics of patients with psychiatric disorders [22, 23].
International literature suggests that challenges in the cancer pathway for this patient group are not limited to the RtD, which was illuminated in this study; their challenges also concern help-seeking behaviour, delays, advanced tumour stage at diagnosis, inferior treatment, survivorship and end-of-life care [13,14,15,16, 20, 21, 23]. Thus, as supported by other studies, there seems to be substantial potential to optimise the cancer pathway for patients with psychiatric disorders.
More research should focus on supportive measures, e.g. integrated care models, shared care, case managers [13] and multidisciplinary teams [14], to ensure better cancer pathways for these patient groups. Our findings suggest that there is room for improving the referral of patients with pre-existing psychiatric disorders to CPPs. More knowledge is needed on how the GPs can be supported in diagnosing cancer in this patient group as many appear to go undetected [13]. To target the efforts, more insight is also needed into whether special attention should be given to specific patients groups, e.g. patients with pre-existing psychiatric disorders who are socially deprived or have physical comorbidity.
Conclusion
This register-based cohort study found that patients with pre-existing psychiatric disorders more often experience less favourable RtD. All three hypotheses were confirmed, i.e. that patients with pre-existing psychiatric disorders were more often diagnosed through less favourable routes than patients without, that patients with severe psychiatric disorders were more often diagnosed after unplanned admissions, and that the association between pre-existing psychiatric disorders and RtD varied with cancer type. Low CPP referral from primary care was more pronounced for many hard-to-diagnose cancer types and severe psychiatric disorders. However, there were exceptions, such as patients with stress disorders.
This study underpins the literature reporting that patients with pre-existing psychiatric disorders are more likely to experience substantial challenges in the cancer pathway. Research is needed to help both the patients and the healthcare providers ensure optimal diagnostics of cancer in this patient group.
Availability of data and materials
All data is assessed and provided through Statistics Denmark [29, 31,32,33,34,35,36,37]. Data is closed for public access and it is not possible for the authors to share the raw data because all data are stored only at Statistics Denmark according to the Danish regulations of research and can only be accessed by remote access VPN. Statistics Denmark does not allow to subtract data from Statistics Denmark which can identify any included patient. Therefore, no data can be shared from this project.
Abbreviations
- ATC:
-
Anatomical Therapeutic Chemical
- CCI:
-
Charlson’s Comorbidity Index
- CI:
-
Confidence intervals
- CPP:
-
Cancer patient pathway
- DCO:
-
Death certificate only
- DNPR:
-
Danish National Patient Registry
- GP:
-
General practitioner
- ICD-10:
-
International Classification of Diseases, 10th version
- ISCED:
-
International Standard Classification of Education
- MLR:
-
Multinomial logistic regression
- PCRR:
-
Danish Psychiatric Central Research Register
- RRR:
-
Relative risk ratio
- RtD:
-
Route to diagnosis
- SD:
-
Standard deviation
- TWW:
-
Two-week wait
References
The Danish Health Data Authority, new cancer cases in Denmark [In Danish: nye kræfttilfælde i Danmark]. Copenhagen; 2019.
Ssi. Register for death [In Danish: Dødsårsagsregisteret - tal og analyse]. Copenhagen: SSI; 2018.
Elliss-Brookes L, McPhail S, Ives A, Greenslade M, Shelton J, Hiom S, et al. Routes to diagnosis for cancer - determining the patient journey using multiple routine data sets. Br J Cancer. 2012;107(8):1220–6.
Jensen H, Torring ML, Vedsted P. Prognostic consequences of implementing cancer patient pathways in Denmark: a comparative cohort study of symptomatic cancer patients in primary care. BMC Cancer. 2017;17(1):627.
Jensen H, Torring ML, Olesen F, Overgaard J, Vedsted P. Cancer suspicion in general practice, urgent referral and time to diagnosis: a population-based GP survey and registry study. BMC Cancer. 2014;14:636.
Danckert B, Falborg AZ, Christensen NL, Frederiksen H, Lyratzopoulos G, McPhail S, et al. Routes to diagnosis and the association with the prognosis in patients with cancer - a nationwide register-based cohort study in Denmark. Cancer Epidemiol. 2021;74:101983.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43.
Friis K, Pedersen MH, Larsen FB, Lasgaard M. A National Population Study of the co-occurrence of multiple long-term conditions in people with multimorbidity, Denmark, 2013. Prev Chronic Dis. 2016;13:E12.
Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980-2013. Int J Epidemiol. 2014;43(2):476–93.
Nordentoft M, Wahlbeck K, Hallgren J, Westman J, Osby U, Alinaghizadeh H, et al. Excess mortality, causes of death and life expectancy in 270,770 patients with recent onset of mental disorders in Denmark, Finland and Sweden. PLoS One. 2013;8(1):e55176.
Plana-Ripoll O, Pedersen CB, Agerbo E, Holtz Y, Erlangsen A, Canudas-Romo V, et al. A comprehensive analysis of mortality-related health metrics associated with mental disorders: a nationwide, register-based cohort study. Lancet. 2019;394(10211):1827–35.
De Hert M, Cohen D, Bobes J, Cetkovich-Bakmas M, Leucht S, Ndetei DM, et al. Physical illness in patients with severe mental disorders. II. Barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level. World Psychiatry. 2011;10(2):138–51.
Lawrence D, Kisely S. Inequalities in healthcare provision for people with severe mental illness. J Psychopharmacol. 2010;24(4 Suppl):61–8.
Irwin KE, Henderson DC, Knight HP, Pirl WF. Cancer care for individuals with schizophrenia. Cancer. 2014;120(3):323–34.
DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–7.
Niedzwiedz CL, Knifton L, Robb KA, Katikireddi SV, Smith DJ. Depression and anxiety among people living with and beyond cancer: a growing clinical and research priority. BMC Cancer. 2019;19(1):943.
Ribe AR, Laurberg T, Laursen TM, Charles M, Vedsted P, Vestergaard M. Ten-year mortality after a breast Cancer diagnosis in women with severe mental illness: a Danish population-based cohort study. PLoS One. 2016;11(7):e0158013.
Kisely S, Crowe E, Lawrence D. Cancer-related mortality in people with mental illness. JAMA Psychiatry. 2013;70(2):209–17.
Toender A, Munk-Olsen T, Vestergaard M, Larsen JT, Suppli NP, Dalton SO, et al. Impact of severe mental illness on cancer stage at diagnosis and subsequent mortality: a population-based register study. Schizophr Res. 2018;201:62–9.
Renzi C, Kaushal A, Emery J, Hamilton W, Neal RD, Rachet B, et al. Comorbid chronic diseases and cancer diagnosis: disease-specific effects and underlying mechanisms. Nat Rev Clin Oncol. 2019;16(12):746–61.
O'Rourke RW, Diggs BS, Spight DH, Robinson J, Elder KA, Andrus J, et al. Psychiatric illness delays diagnosis of esophageal cancer. Dis Esophagus. 2008;21(5):416–21.
Mounce LTA, Price S, Valderas JM, Hamilton W. Comorbid conditions delay diagnosis of colorectal cancer: a cohort study using electronic primary care records. Br J Cancer. 2017. https://doi.org/10.1038/bjc.2017.127.
Van Hout AM, de Wit NJ, Rutten FH, Peeters PH. Determinants of patient's and doctor's delay in diagnosis and treatment of colorectal cancer. Eur J Gastroenterol Hepatol. 2011;23(11):1056–63.
Jensen LF, Pedersen AF, Bech BH, Andersen B, Vedsted P. Psychiatric morbidity and non-participation in breast cancer screening. Breast (Edinburgh, Scotland). 2015. https://doi.org/10.1016/S0960-9776(15)00212-X.
Wallace D, Walker K, Kuryba A, Finan P, Scott N, van der Meulen J. Identifying patients at risk of emergency admission for colorectal cancer. Br J Cancer. 2014;111(3):577–80.
Pedersen KM, Andersen JS, Sondergaard J. General practice and primary health care in Denmark. J Am Board Fam Med. 2012;25(Suppl 1):S34–8.
Probst HB, Hussain ZB, Andersen O. Cancer patient pathways in Denmark as a joint effort between bureaucrats, health professionals and politicians--a national Danish project. Health Policy. 2012;105(1):65–70.
Danish Health Authority. Cancer Patient Pathway [in Danish: Kræftpakkeforløb]. https://www.sst.dk/da/Viden/Kraeft/Kraeftpakkeforloeb. Assessed 26 Apr 2022.
Gjerstorff ML. The Danish Cancer registry. Scand J Public Health. 2011;39(7 Suppl):42–5.
Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22–5.
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–3.
Christiansen P, Ejlertsen B, Jensen MB, Mouridsen H. Danish breast Cancer cooperative group. Clin Epidemiol. 2016;8:445–9.
Ingeholm P, Gogenur I, Iversen LH. Danish colorectal Cancer group database. Clin Epidemiol. 2016;8:465–8.
Rygaard C. The Danish quality database for cervical Cancer screening. Clin Epidemiol. 2016;8:655–60.
Helweg-Larsen K. The Danish register of causes of death. Scand J Public Health. 2011;39(7 Suppl):26–9.
Mors O, Perto GP, Mortensen PB. The Danish psychiatric central research register. Scand J Public Health. 2011;39(7 Suppl):54–7.
Kildemoes HW, Sorensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health. 2011;39(7 Suppl):38–41.
UNESCO. ISCED: International standard classification of education; 2014. p. 2014.
Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–82.
Plana-Ripoll O, Pedersen CB, Holtz Y, Benros ME, Dalsgaard S, de Jonge P, et al. Exploring comorbidity within mental disorders among a Danish National Population. JAMA Psychiatry. 2019;76(3):259–70.
Thygesen LC, Daasnes C, Thaulow I, Bronnum-Hansen H. Introduction to Danish (nationwide) registers on health and social issues: structure, access, legislation, and archiving. Scand J Public Health. 2011;39(7 Suppl):12–6.
Momen NC, Plana-Ripoll O, Agerbo E, Benros ME, Børglum AD, Christensen MK, et al. Association between mental disorders and subsequent medical conditions. N Engl J Med. 2020;382(18):1721–31.
Prior A, Fenger-Gron M, Larsen KK, Larsen FB, Robinson KM, Nielsen MG, et al. The association between perceived stress and mortality among people with multimorbidity: a prospective population-based cohort study. Am J Epidemiol. 2016;184(3):199–210.
Batki SL, Meszaros ZS, Strutynski K, Dimmock JA, Leontieva L, Ploutz-Snyder R, et al. Medical comorbidity in patients with schizophrenia and alcohol dependence. Schizophr Res. 2009;107(2–3):139–46.
Koo MM, Hamilton W, Walter FM, Rubin GP, Lyratzopoulos G. Symptom signatures and diagnostic timeliness in Cancer patients: a review of current evidence. Neoplasia. 2018;20(2):165–74.
Lyratzopoulos G, Neal RD, Barbiere JM, Rubin GP, Abel GA. Variation in number of general practitioner consultations before hospital referral for cancer: findings from the 2010 National Cancer Patient Experience Survey in England. Lancet Oncol. 2012;13(4):353–65.
Acknowledgements
We thank Statistics Denmark for hosting the data and the Danish Clinical Quality Program – National Clinical Registries (RKKP) for granting permission to use data from the Danish Breast Cancer Group, the Danish Colorectal Cancer Database and the Danish Quality Database for Cervical Cancer Screening database. We wish to thank Bolette Danckert for her work in developing the RtD algorithm and for valuable inputs to the methods and manuscript. Finally, we thank Kaare Rud Flarup for data management assistance and Lone Niedziella for language revision.
Funding
This project was financially supported by the Danish Cancer Society and the Danish General Practice Fund. The funders were not involved in the development of the study, data analyses or the interpretation of the results.
Author information
Authors and Affiliations
Contributions
All authors conceived the idea of the study. LFV were primarily responsible for the data management, data analysis, reporting and writing of the paper. All authors contributed with constructive input throughout the project and to editing of the drafts. All authors read and approved the final version of the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The project is registered in the Record of Processing Activities at the Research Unit for General Practice, Aarhus (ID 951) in accordance with the Danish Data Protection Act (Act No. 502 of 23 May 2018) and the General Data Protection Regulation (GDPR) by the European Union. The study did not require approval from the Committee on Health Research Ethics of the Central Denmark Region as no biomedical intervention was performed. No consent from patients were required as the Danish Data Protection Act exempts statistical or scientific studies of significant importance to society. Statistics Denmark approved the project and access to registers used in this project [29, 31,32,33,34,35,36,37].
Consent for publication
According to the Danish Data Protection Act as stated above, register projects do not need specified consent for publication from included patients. Personal rights are ensured by Statistics Denmark, where data are pseudo anonymous and Statistics Denmark does not allow reporting of data which can be personal identified.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Part 1
. Distribution of cancer types. Part 2. Distribution of RtD according to different definitions of pre-existing psychiatric disorder (n = 155,851). Part 3. Relative risk ratio* for presenting in each route compared with “CPP – primary care” according to different definitions of pre-existing psychiatric disorders. Part 4. Estimated probability* of presenting through “CPP – primary care” and “unplanned admission” for each cancer type according to pre-existing psychiatric disorders based on hospital diagnosis registration.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Virgilsen, L.F., Vedsted, P., Falborg, A.Z. et al. Routes to cancer diagnosis for patients with pre-existing psychiatric disorders: a nationwide register-based cohort study. BMC Cancer 22, 472 (2022). https://doi.org/10.1186/s12885-022-09598-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09598-x