
Abstract
Background
Mouse and human studies support the promise of dry beans to improve metabolic health and to lower cancer risk. In overweight/obese patients with a history of colorectal polyps or cancer, the Beans to Enrich the Gut microbiome vs. Obesity’s Negative Effects (BE GONE) trial will test whether and how an increase in the consumption of pre-cooked, canned dry beans within the context of usual diet and lifestyle can enhance the gut landscape to improve metabolic health and reduce cancer risk.
Methods/design
This randomized crossover trial is designed to characterize changes in (1) host markers spanning lipid metabolism, inflammation, and obesity-related cancer risk; (2) compositional and functional profiles of the fecal microbiome; and (3) host and microbial metabolites. With each subject serving as their own control, the trial will compare the participant’s usual diet with (intervention) and without (control) dry beans. Canned, pre-cooked dry beans are provided to participants and the usual diet continually assessed and monitored. Following a 4-week run-in and equilibration period, each participant provides a total of 5 fasting blood and 6 stool samples over a total period of 16 weeks. The intervention consists of a 2-week ramp-up of dry bean intake to 1 cup/d, which is then continued for an additional 6 weeks. Intra- and inter-individual outcomes are assessed across each crossover period with consideration of the joint or modifying effects of the usual diet and baseline microbiome.
Discussion
The BE GONE trial is evaluating a scalable dietary prevention strategy targeting the gut microbiome of high-risk patients to mitigate the metabolic and inflammatory effects of adiposity that influence colorectal cancer risk, recurrence, and survival. The overarching scientific goal is to further elucidate interactions between diet, the gut microbiome, and host metabolism. Improved understanding of the diet-microbiota interplay and effective means to target these relationships will be key to the future of clinical and public health approaches to cancer and other major diet- and obesity-related diseases.
Trial registration
This protocol is registered with the U.S. National Institutes of Health trial registry, ClinicalTrials.gov, under the identifier NCT02843425. First posted July 25, 2016; last verified January 25, 2019.
Similar content being viewed by others


Background
A growing body of research indicates that diet can change the vast community of bacteria (or microbiome) known to affect obesity and cancer risk [1,2,3,4,5,6]; and presents a potentially effective strategy to improve outcomes among high-risk patients [7]. Provocative findings from controlled human feeding studies reveal that diet-induced changes in the gut microbiome can be both rapid and profound, but easily reversed [8, 9] signifying that beneficial bacteria or microbial communities may need to be continually cultivated to ultimately improve chronic health problems and to prevent latent cancers or their recurrence. Simple strategies are needed for overweight and obese patients who have likely suffered from a history of challenges surrounding food and weight control, as well as for high-risk individuals who prefer dietary approaches to drugs or who cannot tolerate other therapies.
Dry beans (Phaseolus vulgaris) are a prebiotic food source rich in bioactive compounds with anti-inflammatory, anti-lipidemic, and chemopreventive properties [10,11,12]. Despite supportive evidence from parallel obese mouse and human studies [13,14,15,16,17] dry beans are not a particularly popular or well-recognized dietary strategy for reducing the recurrence of colorectal polyps or cancer. One potential barrier to clinical and public health implementation is that none of the previous studies address whether simply increasing or adding beans to the usual diet, as suggested by observational findings in the Polyp Prevention Trial [18], is sufficient to improve gut and overall metabolic health to lower cancer risk. Secondly, the gut microbiome, a potentially transformative tool, has not yet been assessed in a whole dry bean intervention among high-risk, overweight or obese patients with a history of colorectal polyps or cancer.
The BE GONE trial is designed test whether and how a relatively simple increase in canned, pre-cooked dry bean intake can enrich the gut microbiome of overweight/obese patients with a history of precancerous colorectal polyps or colorectal cancer. The trial is also designed to assess whether changes in the gut microbiome precede or parallel changes in other established markers of gut health, metabolic health, and obesity-related cancer risk.
Hypotheses and objectives
Given the prebiotic and antineoplastic properties of beans, and that changes in host diet rapidly alter the composition of gut microbiota, we expect that the dry bean intervention among overweight/obese individuals positive for precancerous colorectal (CR) polyps or CR cancer (herein referred to as “high-risk CR patients”) will enrich or balance the gut microbiome with beneficial bacteria. We further hypothesize that these changes will correlate with improvements in microbial metabolites and host biomarkers that modulate host inflammation and metabolism; and/or lower levels of metabolites positively correlated with obesity-related factors. Characterizing fecal microbiota, blood markers, and metabolites to elucidate interactions between diet, the gut microbiome, and host metabolism will provide insight into overlapping obesity and cancer pathways and more effective methods of upstream dietary prevention (Fig. 1).

Fiber-rich diet shapes the composition, function and metabolic output of the gut microbiome. Diet modulates host metabolism and inflammation both directly and through the activities of the gut microbiome
Primary objective
To examine the effect of increased consumption of dry beans on the gut microbiome and blood biomarkers in high-risk CR patients otherwise consuming their usual diet.
Secondary objective
To develop the field and research procedures of a prospective randomized crossover dietary intervention of whole dry beans, including compliance in our target patient population and the modifying effects of the baseline gut microbiome and usual diet on participant’s response to the intervention.
Outcome measures
The primary outcome measures are parallel changes in gut microbiota profiles and circulating lipid and adipocytokine profiles from serial stool and fasting blood samples collected at baseline, week 4, and week 8 for each cross-over period. Secondary outcomes include fecal surrogates of gut inflammation and host and microbial metabolites.
Methods/design
Overview of trial design
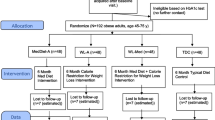
The study is a prospective, randomized, crossover trial (Figs. 2 and 3) of increased dry bean intake added to the participant’s usual diet (Intervention Diet), as compared to the participant’s usual diet excluding dry beans (Control Diet). Following an equilibration (control diet) period, sixty eligible subjects are randomized to one of two diet sequences - Control Diet then Intervention Diet or Intervention Diet then Control diet - with each subject acting as their own control. Canned beans are provided during the intervention period and multiple measurements are obtained at baseline and follow-up during each diet period in the sequence. Participants are free-living during the study period and able to choose and prepare their own meals, but are asked to not change any of their other usual habits for the duration of the study. To assess and monitor habitual behavior and adherence, participants are asked to complete web-based assessments at various time points during the study.

CONSORT flow chart for BE GONE Trial

Trial procedures and visit flow
Recruitment and setting
Our main goals are to recruit a diverse set of high-risk CR patients with variation in basal diet and microbiome to address important research questions for future, multicenter trials; and a clinically well-characterized patient population that we can continue to follow over time. The study is conducted at The University of Texas MD Anderson Cancer Center main campus in Houston, Texas. Patients are actively recruited throughout MD Anderson with concentrated efforts in the colorectal screening, treating and survivorship clinics, as well as Kelsey-Seybold, a local referral clinic. Current and former patients are also identified via the institutional tumor registry and electronic medical records. Potentially eligible patients receive invitation emails or postcards with a brief but clear description of the study and procedures. Interested subjects are recruited either during a clinic visit or from inquiry via phone or email.
Eligibility criteria
Recruitment is targeted to overweight or obese patients with a previous history of colorectal polyps or cancer. Full inclusion and exclusion criteria are included in Table 1.
Informed consent
All subjects must sign informed consent to participate in the study. This consent form fulfills the requirements set forth by the Institutional Review Board (IRB) of MD Anderson. Before signing the consent form, all relevant details and the voluntary nature of the research study, including its purpose, procedures, anticipated risks and benefits are discussed with the potential participant. This dietary study is considered low risk and Data Monitoring Committee exempt. The trial is monitored by the PI and study physicians.
Study intervention
Pre-visit, equilibration and run-in
To establish the basal diet and microbiome and to track compliance with study procedures prior to randomization, eligible and enrolled participants are asked to provide a stool sample and to complete anthropometric, dietary and other assessments during the pre-visit (Fig. 3). In the event that a recent clinical evaluation is not on file for an interested participant, a finger prick glucose test may also be administered. In the subsequent run-in period, participants are asked to follow the control diet (usual diet excluding dry beans) for the first 4 weeks.
Randomization and follow-up visits (V0-V4)
Participants who complete the run-in are randomized to begin the intervention diet or to continue the control diet for an additional 8 weeks (Fig. 2). The randomization list was generated by an independent analyst and allocated by a research team member not directly interacting with participants. Participants are block-randomized according to no use vs. regular use of chronic disease medications (namely statins and metformin) commonly prescribed to our target population of overweight/obese high risk CR patients. The randomization visit (V0) and all subsequent trial visits require a fasting blood draw and are conducted in the morning. There are a total of 5 in-person visits every 4 weeks from the randomization visit. At each visit, anthropometry and blood pressure are measured. Medications and changes in health status are reviewed. In addition, a stool sample is brought to each visit (Fig. 3).
Ramp-up and dose
Participants are provided with a supply of pre-cooked, canned organic navy beans (Phaseolus vulgaris) [19,20,21] stored in water with sea salt. To examine dose-response and temporal effects and to avoid gastrointestinal (GI) discomfort, participants are counseled to incorporate the canned beans in to their usual diet in a stepwise fashion during the intervention sequence (Fig. 3). Participants begin by consuming ½ cup (1 serving) of beans over the 2 week ramp-up period. At the end of the ramp-up period, participants provide a stool sample by mail. Following the ramp-up, participants consume 1 cup (2 servings) per day for an additional 6 weeks. At week 8, participants who complete the intervention diet crossover to the control diet and vice versa. Two ½ cup servings (260 g) of canned navy beans provide 220 kcal, 14 g protein, 38 g carbohydrate (~ 12% of 2000 kcal diet), 16 g of fiber (~ 64%), 200 mg of sodium (~ 8%), 660 mg of potassium (~ 22%), 12% of daily value for calcium and 20% of daily value for iron.
Compliance, adherence, and adverse effects
In addition to in-person visits, the study coordinator and registered dietitian (RD) maintain regular contact with participants via email and phone, while assuring and tracking all study procedures. When on the intervention diet, participants are provided simple, tailored tips and recipes for incorporating the beans in to their usual diet pattern. Participants are asked to keep a “bean log” to record adherence and track GI discomfort. In addition to frequent web-based dietary assessments, the bean log includes a week-by-week daily record of the date, time, amount and meal or manner in which the beans were consumed. Participants are considered adherent if they consume ≥80% of the beans over the intervention period and follow the prescribed regimen on at least 5 days/week. If despite consultation with the RD, some participants still experience difficulties adding the beans to their diet on their own or have specific needs (e.g., air travel), bean crackers prepared by the MD Anderson Cancer Center Bionutrition Research Core kitchen are provided. Participants may also continue the dietary intervention at a reduced/tolerable dose. Of the 30 previous dry bean and CVD trials reviewed, 11 trials reported GI symptoms, such as upset stomach, flatulence, bloating, and increased stool frequency. Across previous similar studies ≤2 participants per trial dropped out due to symptoms [22, 23]. In our study, all adverse events are documented at the time of report, recorded, and reviewed with the study physician. Grade 3 or above adverse effects, according to the Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0, are reviewed immediately with the study physician. If any of the Grade 3 or above adverse effects are deemed serious according to MD Anderson IRB policies, then the IRB is also notified immediately.
Withdrawal
Participants may withdraw from the study at any time during the run-in or over the course of the study period (Fig. 2). Reasons for withdrawal are recorded (e.g., intolerance or inability to consume the beans, or a reason unrelated to the intervention). We request that participants, if willing, return a final stool sample by mail.
Post-trial follow-up
To explore the post-trial feasibility and impact of diet change, we conduct extended follow-up of all participants who complete the trial to begin to assess whether a long-term increase in bean intake is feasible, maintainable, and/or desirable in our target population. We use both active and passive follow-up methods via email/telephone, and electronic patient records. We assess current dietary habits via the NCI-DHQ (at 6 months and 1-year post-trial completion), as well as health outcomes and results of any subsequent screening exams. Participants may request to cease contact at any time.
Biospecimen and data collection
Stool and fasting blood sample collection
An in-home, fresh-frozen stool sample collection kit, similar to that used in the Human Microbiome Project (HMP) [24] and refined in our previous studies is provided to participants with detailed instructions during the clinic visit. The participant is instructed to collect a stool sample before each scheduled in-clinic visit or return it via pre-paid express mail. Upon receipt, samples are transferred to − 80 °C storage. Fasting blood is collected at each morning in-clinic visit and immediately processed.
Diet and lifestyle assessment
Standard computer/web-enabled risk factor questionnaires (REDCap) are used to establish baseline status and monitor deviations over the study period (Fig. 3: Pre, V0, V1, V2, V3, V4). Participant’s diet is continually assessed and monitored throughout the study via biweekly NCI-Automated Self-Administered 24HR (ASA-24) [25] in conjunction with a “past month” web-based NCI diet history questionnaire (DHQ; every 4 weeks) [26]. Physical activity levels are assessed and monitored via validated long- and short versions of the International Physical Activity Questionnaire (IPAQ) [27, 28].
Data quality and integrity
All data is stored in a password protected REDCap and MS Access database on a secure and routinely backed-up institutional server. Audits of selected subsets of data are performed to ensure that appropriate safeguards of participant privacy are maintained. Privacy safeguards include appropriate password protection and physical security for all computer systems. Additional quality assurance procedures include a data collection protocol documented in a protocol manual; and a two-stage editing procedure for survey data collection. This two-stage process consists of the initial review of the data collection form by a project member immediately following data collection followed by a second review by a project member who will record any significant deviations from the protocol. Data entry systems, whether via REDCap, scannable forms, or hand entry with verification, specifically provide field checks, range checks for continuous variables and valid value checks for categorical variables; checks for legitimate dates and times and logical consistency. A specific audit trail system that identifies the date, time, and individual making changes on the database is part of the data-entry system. During data collection, we issue reports weekly, or even following any new data entry, depending on the needs of the project or upon the request of the PI.
Laboratory methods
Gut microbiome and metabolome
To examine the impact of a change in dry bean intake within the usual diet on the diversity and composition of the gut microbiome, we will conduct 16S rRNA gene sequencing on all stool samples collected. Following evaluation of relationships with established blood and stool markers, we will select an informative subset of pre and post-intervention stool samples from participants with marked differences in response to the intervention (e.g., responders vs. non-responders) to conduct whole genome shot-gun (WGS) sequencing and mass spectrometry-based metabolomic profiling of the gut microbiome. This will be complemented by characterization of host pathways via blood-based metabolomics.
Microbiome sequencing and data processing
We utilize state-of-the-art methods developed and benchmarked by our collaborating laboratory [29,30,31]. Briefly, bacterial genomic DNA is extracted and amplified with Illumina barcoded primers and analyzed on the Illumina MiSeq (16S) and HiSeq (WGS) platforms. Bacterial mock community samples (QC standards) are routinely included in each run. Alpha and beta (within and between sample) diversity analyses are performed to assess community diversity and richness by calculating the number of observed species for each sample at various sequencing depths. ANOVA and supervised machine learning techniques are used to identify taxa at the level of phylum, class, genus and species that differ significantly in abundance and discriminate between defined parameters. Various clustering algorithms assess whether distinct microbiome clusters or community types are formed.
Fecal and serum marker analysis
Fecal surrogates of subclinical intestinal inflammation and gut integrity linked to obesity and CRC risk [32, 33] are measured via established ELISA methods [34]. Fasting serum adipokines and cytokines linked to obesity-driven cancer risk and survival [35,36,37,38,39,40,41] and the gut microbiome [42, 43] are assessed via multiplex assays. For comparison with previous dry bean trials a lipid panel (TG, total, HDL, LDL, and VLDL cholesterol) is processed on the day of blood sample collection in a standard manner by a CLIA-certified laboratory.
Statistical considerations
Power
Based on parameters from bean trials of obese individuals that observed comparable changes in LDL cholesterol and inflammatory marker levels [44, 45], with an n of 60 we have > 80% power to detect ≥10% change in LDL levels at a 2-sided α = 0.001 (to account for multiple comparisons). Based on the observed diversity (Shannon Index) and standard deviation (mean 2.5, SD 0.6) among obese polyp patients from our pilot observational study [46, 47], we have > 80% power to detect ≥20% change in microbiome diversity at a 2-sided significance level of alpha = 0.001. For the correlation analyses of changes in the gut microbiome and changes in markers, we have > 80% power at α = 0.001 to detect a significant linear correlation coefficient “r” when the true value is 0.37 [48].
Data analysis
Change scores of outcomes will be based on the differences between the beginning and the end of each study period (Figs. 2 and 3); and by subtracting the change experienced over the control period from the change experienced over the intervention period. Paired t-tests will be conducted to assess whether there are significant differences between changes in each subject’s baseline and follow-up outcomes over the equilibration, control, and intervention period. Two-way ANOVA will be used to test for differences in the change scores by categories of other variables. Generalized linear mixed models (GLMMS) will be used to explore potential order or carry-over effects, and to adjust for other potential confounders and assess potential effect modifiers measured at pre-study and study visits. Hierarchically clustered phylotypes will be constructed by the similarity of their dynamics [31] across study periods and subjects and in relation to other variables, such as usual diet pattern.
To examine the effect of a dry bean intervention on the diversity and composition of the gut microbiome, the primary outcome measure will be changes in stool 16S rRNA gene profiles at baseline and follow-up for each cross-over period. We will quantify the microbial diversity within each subject at each time point; and calculate change scores and construct GLMMs (see above) with repeated measurements (PROC MIXED). We will also construct hierarchically clustered phylotypes by the similarity of their dynamics [31] across study periods and subjects and in relation to other variables, such as usual diet pattern.
To examine the relationship between changes in the gut microbiome and changes in fecal and serum markers, we will follow the procedures described above to quantify changes; and to assess the effects of other variables on these changes. We will assess Spearman correlations of changes in the gut microbiome with changes in fecal and serum markers and employ computational methods to identify taxa associated with differences in serum and fecal markers [49].
To explore relevant functional changes in the gut microbiome we will use a tiered approach. In the first round of analysis of 16S rDNA data to determine whether and where additional resources should be used for more comprehensive metabolomic and metagenomic profiling, we will use and compare established methods to infer metabolic functional profiles from 16S level data [50, 51]. To assess which compounds are related to which bacteria, we will use a combination of statistical methods and computational tools, including cluster and network analysis coupled with correlation-based non-parametric methods to explore the relationship between host markers and metabolomic pathways, microbial metabolites and gut bacterial species [52]. Principal component and coordinate analyses (PCA & PCoA) will be performed to examine intrinsic clusters within the metabolomic and microbiomic data between the control and intervention diets. In addition, heat maps will be generated using a hierarchical clustering algorithm to visualize the differences within the data set. Differences in gut microbiome composition will be further assessed using a nonparametric test, as described previously [53]. The correlation matrix between the microbial metabolites and gut bacterial species will be generated using Spearman and other correlation methods to explore the functional impact of dry beans on the gut microbiome. For analyses in which the multiplicity of tests is an issue, we will use the false discovery rate to report appropriately adjusted significance levels.
Discussion
Randomized and controlled, but also “real world” human studies are needed to improve our understanding of the significance of diet-induced changes in the composition and function of the gut microbiome and their multifaceted impact on human metabolic health and obesity-related cancer risk. Gut health requires a fine balance of multiple elements including microbes and their metabolic products (e.g., short chain fatty acids [SCFA]). Dysfunction in any of these components can result in gut dysbiosis linked to obesity and colorectal cancer risk [54,55,56,57,58]. Proposed mechanisms by which prebiotic foods may improve gut health and reduce metabolic complications among obese persons are similarly multidimensional (Fig. 1). This includes increasing populations of beneficial bacteria or functional communities that support intestinal health and barrier function, increasing satiety, and improving lipid or adipocytokine profiles. Whether or not obese patients experience improvements is likely to be strongly influenced by the metabolic output of the microbiota [3, 7]. In addition to promoting high microbial diversity and low pathogen abundance, microbial SCFAs have a major role in maintaining intestinal homeostasis. Locally in the gut they suppress the growth of gram-negative pathogens and function as energy sources for beneficial bacteria, but also have systemic effects on the host, including anti-inflammatory and pro-apoptotic effects [59, 60]. SCFA and in particular, butyrate-producing species are indicators of a diverse, healthy microbiota, and actively involved in maintaining a stable and healthy gut community. However, little is known about dry bean diet-induced, host-microbiota interactions, particularly the effects of differences in individual’s “starting points” with regard to the quality of usual diet and adaptability of the gut microbiome.
Dry beans provide a safe and viable strategy with strong potential for translation and broad implementation. The large PREDIMED study recently reported that higher intake of total legumes (lentils, chickpeas, fresh peas, and dry beans), as assessed by dietary questionnaires, was associated with a 49% lower risk of cancer mortality, an effect that was more pronounced among obese participants (62%) [61]. Dry beans have been tested in multiple CVD risk marker trials [22, 23] and comparatively limited trials in the cancer setting. A recent randomized-controlled trial among colorectal cancer survivors found that a diet enriched with navy bean powder enhanced fecal microbiota and metabolites to modulate metabolic and molecular pathways linked to colon health [17, 62]. The same group reported that navy bean powder was highly feasible to incorporate into meals to increase total fiber intake [63, 64], reaching amounts associated with colorectal cancer chemoprevention and survival outcomes [65].
This study additionally aims to target scientific questions of crucial importance to nutrition and microbiome research and its translation to patients and public health. Given the growing understanding of the complexity of the microbiome, one proffered solution is to challenge it with dramatic changes or high doses to drive physiologically relevant changes. A number of provocative, small, short-term trials and human feeding studies with gut microbiome endpoints testing dramatic and multiple shifts in diet [1, 66,67,68,69,70,71,72,73,74,75] have left us with a somewhat limited understanding of “real-world” functional changes in the microbiome that are more reflective of free-living human behavior to inform reasonable and scalable dietary prevention strategies. However, these ground-breaking studies provide a number of important lessons moving forward. Whether or not the target “takes” is largely dependent on the gut microbiota of the host and what the host provides to sustain it in terms of diet. Rapid, profound, and just as easily reversible diet-induced changes in the fecal microbiome similarly induce rapid and notable changes in markers of cancer and CVD risk [1, 2, 70, 76,77,78]. One implication is that a consistent dietary change would be needed to enrich beneficial bacteria (by fulfilling their nutritional needs) and shape the gut landscape to ameliorate chronic health problems and prevent latent cancers. Patients diagnosed with colorectal polyps or cancer may be initially highly motivated to improve their diets [79,80,81,82], but dramatic changes in diet are difficult for most individuals to adopt and sustain; and long-term changes will ultimately be required to impact risk and outcomes in this population. For obese individuals who have consistently struggled with weight and food restriction, small evidence-based changes (such as opening a can of beans) are more likely to be acceptable and ultimately effective.
This study will also generate a sizeable biorepository of serially collected stool and blood samples from clinically well-defined (and followed) high-risk CR patients. Linkage with extensive dietary, as well as lifestyle data collected throughout the trial, will enable us to conduct secondary epidemiologic and biomarker analyses to generate new hypotheses to test in future trials. We will also be able to identify blood-based metabolite biomarkers [83] linked to the fecal microbiome that can be assessed in large prospective cohorts of diet and cancer.
The findings from the BE GONE study will be disseminated through peer-reviewed publications following ICMJE recommendations (http://www.icmje.org/) and presented at international meetings to healthcare professionals. Further dissemination will be through the press and social media. It is expected that findings from the BE GONE trial may inform dietary recommendations and guidelines for high-risk patients and survivors.
Availability of data and materials
Not applicable.
Following publication of the primary analysis, we plan to deposit/make available de-identified data for the purposes of transparency and replication.
Abbreviations
- ANOVA:
-
Analysis of Variance
- ASA-24:
-
NCI-Automated Self-Administered 24HR
- BE GONE:
-
The Beans to Enrich the Gut microbiome vs. Obesity’s Negative Effects
- BMI:
-
Body mass index
- CLIA:
-
Clinical Laboratory Improvement Amendments
- CTCAE:
-
Common Terminology Criteria for Adverse Events
- CVD:
-
Cardiovascular disease
- DHQ:
-
NCI diet history questionnaire
- g:
-
Gram
- GI:
-
Gastrointestinal
- GLMM:
-
Generalized linear mixed models
- HDL:
-
High density lipoprotein
- IPAQ:
-
International Physical Activity Questionnaire
- IRB:
-
Institutional Review Board
- Kilocalories:
-
Kcal
- LDL:
-
Low density lipoprotein
- QC:
-
Quality control
- rRNA:
-
Ribsomal ribonucleic acid
- SCFA:
-
Short chain fatty acid
- TG:
-
Triglycerides
- V:
-
Visit
- VLDL:
-
Very low density lipoprotein
- WGS:
-
Whole genome shotgun
References
O'Keefe SJD, Li JV, Lahti L, Ou J, Carbonero F, Mohammed K, et al. Fat, fibre and cancer risk in African Americans and rural Africans. Nat Commun. 2015;6.
Russell WR, Duncan SH, Flint HJ. The gut microbial metabolome: modulation of cancer risk in obese individuals. Proc Nutr Soc. 2013;72(1):178–88.
Kovatcheva-Datchary P, Nilsson A, Akrami R, Lee YS, De Vadder F, Arora T, et al. Dietary Fiber-Induced Improvement in Glucose Metabolism Is Associated with Increased Abundance of Prevotella. Cell Metab. 2015;22(6):971–82.
Cani PD. Gut microbiota — at the intersection of everything? Nat Rev Gastroenterol Hepatol. 2017;14:321.
Cani PD, Jordan BF. Gut microbiota-mediated inflammation in obesity: a link with gastrointestinal cancer. Nat Rev Gastroenterol Hepatol. 2018;15(11):671–82.
Valdes AM, Walter J, Segal E, Spector TD. Role of the gut microbiota in nutrition and health. BMJ (Clinical research ed). 2018;361:k2179.
Daniel CR, McQuade JL. Nutrition and Cancer in the Microbiome Era. Trends Cancer. 2019;5(9):521–4.
Dubois G, Girard C, Lapointe FJ, Shapiro BJ. The Inuit gut microbiome is dynamic over time and shaped by traditional foods. Microbiome. 2017;5(1):151.
Singh RK, Chang H-W, Yan D, Lee KM, Ucmak D, Wong K, et al. Influence of diet on the gut microbiome and implications for human health. J Transl Med. 2017;15(1):73.
Rebello CJ, Greenway FL, Finley JW. A review of the nutritional value of legumes and their effects on obesity and its related co-morbidities. Obes Rev. 2014;15(5):392–407.
Daniel CR, Park Y, Chow WH, Graubard BI, Hollenbeck AR, Sinha R. Intake of fiber and fiber-rich plant foods is associated with a lower risk of renal cell carcinoma in a large US cohort. Am J Clin Nutr. 2013;97(5):1036–43.
Campos-Vega R, Bassinello PZ, Santiago RAC, Oomah BD. Chapter 20 - Dry Beans: Processing and Nutritional Effects. In: Grumezescu AM, Holban AM, editors. Therapeutic, Probiotic, and Unconventional Foods: Academic Press; 2018. p. 367–86.
Zhang C, Monk JM, Lu JT, Zarepoor L, Wu W, Liu R, et al. Cooked navy and black bean diets improve biomarkers of colon health and reduce inflammation during colitis. Br J Nutr. 2014;111(9):1549–63.
Hartman TJ, Albert PS, Zhang Z, Bagshaw D, Kris-Etherton PM, Ulbrecht J, et al. Consumption of a Legume-Enriched, Low-Glycemic Index Diet Is Associated with Biomarkers of Insulin Resistance and Inflammation among Men at Risk for Colorectal Cancer. J Nutr. 2009;140(1):60–7.
Sheflin AM, Borresen EC, Kirkwood JS, Boot CM, Whitney AK, Lu S, et al. Dietary supplementation with rice bran or navy bean alters gut bacterial metabolism in colorectal cancer survivors. Mol Nutr Food Res. 2016;61(1):1500905.
Perera T, Takata Y, Bobe G. Dry Bean Consumption Inhibits Colorectal Tumorigenesis in Preclinical Studies: A Meta-Analysis of Animal Studies. FASEB J. 2017;31(1_supplement) 790.21-21.
Baxter B, Oppel R, Ryan E. Navy Beans Impact the Stool Metabolome and Metabolic Pathways for Colon Health in Cancer Survivors. Nutrients. 2018;11(1):28.
Lanza E, Hartman TJ, Albert PS, Shields R, Slattery M, Caan B, et al. High dry bean intake and reduced risk of advanced colorectal adenoma recurrence among participants in the polyp prevention trial. J Nutr. 2006;136(7):1896–903.
Barampama Z, Simard RE. Effects of soaking, cooking and fermentation on composition, in-vitro starch digestibility and nutritive value of common beans. Plant Foods Hum Nutr. 1995;48(4):349–65.
Bressani R, de Mora DR, Flores R, Gomez-Brenes R. Evaluation of two methods to determine the polyphenol content in raw and cooked beans and its effect on protein digestibility. Arch Latinoam Nutr. 1991;41(4):569–83.
Traianedes K, O'Dea K. Commercial canning increases the digestibility of beans in vitro and postprandial metabolic responses to them in vivo. Am J Clin Nutr. 1986;44(3):390–7.
Ha V, Sievenpiper JL, de Souza RJ, Jayalath VH, Mirrahimi A, Agarwal A, et al. Effect of dietary pulse intake on established therapeutic lipid targets for cardiovascular risk reduction: a systematic review and meta-analysis of randomized controlled trials. CMAJ. 2014;186(8):E252–62.
Bazzano LA, Thompson AM, Tees MT, Nguyen CH, Winham DM. Non-soy legume consumption lowers cholesterol levels: a meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2011;21(2):94–103.
Aagaard K, Petrosino J, Keitel W, Watson M, Katancik J, Garcia N, et al. The Human Microbiome Project strategy for comprehensive sampling of the human microbiome and why it matters. FASEB J. 2012.
Subar AF, Kirkpatrick SI, Mittl B, Zimmerman TP, Thompson FE, Bingley C, et al. The Automated Self-Administered 24-hour dietary recall (ASA24): a resource for researchers, clinicians, and educators from the National Cancer Institute. J Acad Nutr Diet. 2012;112(8):1134–7.
Millen AE, Midthune D, Thompson FE, Kipnis V, Subar AF. The National Cancer Institute diet history questionnaire: validation of pyramid food servings. Am J Epidemiol. 2006;163(3):279–88.
Rosenberg DE, Bull FC, Marshall AL, Sallis JF, Bauman AE. Assessment of sedentary behavior with the International Physical Activity Questionnaire. J Phys Act Health. 2008;5(Suppl 1):S30–44.
Hagstromer M, Oja P, Sjostrom M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutr. 2006;9(6):755–62.
Gevers D, Knight R, Petrosino JF, Huang K, McGuire AL, Birren BW, et al. The Human Microbiome Project: a community resource for the healthy human microbiome. PLoS Biol. 2012;10(8):e1001377.
The Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature. 2012;486(7402):207–14.
Marino S, Baxter NT, Huffnagle GB, Petrosino JF, Schloss PD. Mathematical modeling of primary succession of murine intestinal microbiota. Proc Natl Acad Sci U S A. 2014;111(1):439–44.
John BJ, Abulafi AM, Poullis A, Mendall MA. Chronic subclinical bowel inflammation may explain increased risk of colorectal cancer in obese people. Gut. 2007;56(7):1034–5.
Tsukamoto S, Ishikawa T, Iida S, Ishiguro M, Mogushi K, Mizushima H, et al. Clinical significance of osteoprotegerin expression in human colorectal cancer. Clin Cancer Res. 2011;17(8):2444–50.
Mohamed JA, DuPont HL, Jiang ZD, Flores J, Carlin LG, Belkind-Gerson J, et al. A single-nucleotide polymorphism in the gene encoding osteoprotegerin, an anti-inflammatory protein produced in response to infection with diarrheagenic Escherichia coli, is associated with an increased risk of nonsecretory bacterial diarrhea in North American travelers to Mexico. J Infect Dis. 2009;199(4):477–85.
Vongsuvanh R, George J, Qiao L, van der Poorten D. Visceral adiposity in gastrointestinal and hepatic carcinogenesis. Cancer Lett. 2013;330(1):1–10.
Hursting SD, Dunlap SM. Obesity, metabolic dysregulation, and cancer: a growing concern and an inflammatory (and microenvironmental) issue. Ann N Y Acad Sci. 2012;1271:82–7.
Hursting SD, DiGiovanni J, Dannenberg AJ, Azrad M, LeRoith D, Demark-Wahnefried W, et al. Obesity, Energy Balance, and Cancer: New Opportunities for Prevention. Cancer Prev Res. 2012;5(11):1260–72.
Hursting SD, Hursting MJ. Growth signals, inflammation, and vascular perturbations: mechanistic links between obesity, metabolic syndrome, and cancer. Arterioscler Thromb Vasc Biol. 2012;32(8):1766–70.
Ho GY, Wang T, Gunter MJ, Strickler HD, Cushman M, Kaplan RC, et al. Adipokines linking obesity with colorectal cancer risk in postmenopausal women. Cancer Res. 2012;72(12):3029–37.
Doyle SL, Donohoe CL, Lysaght J, Reynolds JV. Visceral obesity, metabolic syndrome, insulin resistance and cancer. Proc Nutr Soc. 2012;71(1):181–9.
Shah MS, Fogelman DR, Ranghav KPS, Heymach JV, Tran HT, Jiang ZQ, et al. Joint prognostic effect of obesity and chronic systemic inflammation in metastatic colorectal cancer (forthcoming). Cancer. 2015.
Cotillard A, Kennedy SP, Kong LC, Prifti E, Pons N, Le Chatelier E, et al. Dietary intervention impact on gut microbial gene richness. Nature. 2013;500(7464):585–8.
Le Chatelier E, Nielsen T, Qin J, Prifti E, Hildebrand F, Falony G, et al. Richness of human gut microbiome correlates with metabolic markers. Nature. 2013;500(7464):541–6.
Finley JW, Burrell JB, Reeves PG. Pinto bean consumption changes SCFA profiles in fecal fermentations, bacterial populations of the lower bowel, and lipid profiles in blood of humans. J Nutr. 2007;137(11):2391–8.
Zhang Z, Lanza E, Kris-Etherton PM, Colburn NH, Bagshaw D, Rovine MJ, et al. A high legume low glycemic index diet improves serum lipid profiles in men. Lipids. 2010;45(9):765–75.
Daniel CR, Hoffman KL, Raju GS, Hanash SM, Hutchinson DS, Ajami NJ, et al. Abstract 238: Evidence of early colorectal cancer risk and prevention pathways in the fecal microbiome of colonoscopy patients: associations with diet and circulating adipocytokines. Cancer Res. 2017;77(13 Supplement):238.
Daniel CR, Hoffman KL, Sood A, Raju GS, Hanash SM, Wu X, et al. Abstract A26: Diet quality vs quantity in relation to the fecal microbiome among colonoscopy patients. Cancer Res. 2017;77(3 Supplement) A26-A.
Schoenfeld DA. Statistical considerations for clinical trials and scientific experiments Available from: http://hedwig.mgh.harvard.edu/sample_size/size.html.
Segata N, Izard J, Waldron L, Gevers D, Miropolsky L, Garrett WS, et al. Metagenomic biomarker discovery and explanation. Genome Biol. 2011;12(6):R60.
Langille MG, Zaneveld J, Caporaso JG, McDonald D, Knights D, Reyes JA, et al. Predictive functional profiling of microbial communities using 16S rRNA marker gene sequences. Nat Biotechnol. 2013;31(9):814–21.
Asshauer KP, Wemheuer B, Daniel R, Meinicke P. Tax4Fun: predicting functional profiles from metagenomic 16S rRNA data. Bioinformatics (Oxford, England). 2015;31(17):2882–4.
Shoaie S, Ghaffari P, Kovatcheva-Datchary P, Mardinoglu A, Sen P, Pujos-Guillot E, et al. Quantifying Diet-Induced Metabolic Changes of the Human Gut Microbiome. Cell Metab. 2015;22(2):320–31.
White JR, Nagarajan N, Pop M. Statistical methods for detecting differentially abundant features in clinical metagenomic samples. PLoS Comput Biol. 2009;5(4):e1000352.
Kant P, Fazakerley R, Hull MA. Faecal calprotectin levels before and after weight loss in obese and overweight subjects. Int Jf Obes (2005). 2013;37(2):317–9.
Song M, Chan AT. Diet, Gut Microbiota, and Colorectal Cancer Prevention: a Review of Potential Mechanisms and Promising Targets for Future Research. Curr Colorectal Cancer Rep. 2017;13(6):429–39.
Song M, Chan AT. Environmental Factors, Gut Microbiota, and Colorectal Cancer Prevention. Clin Gastroenterol Hepatol. 2019;17(2):275–89.
Tilg H, Adolph TE, Gerner RR, Moschen AR. The Intestinal Microbiota in Colorectal Cancer. Cancer Cell. 2018;33(6):954–64.
Chen J, Pitmon E, Wang K. Microbiome, inflammation and colorectal cancer. Semin Immunol. 2017;32:43–53.
Hagland HR, Soreide K. Cellular metabolism in colorectal carcinogenesis: Influence of lifestyle, gut microbiome and metabolic pathways. Cancer Lett. 2014.
Louis P, Hold GL, Flint HJ. The gut microbiota, bacterial metabolites and colorectal cancer. Nat Rev Microbiol. 2014;12(10):661–72.
Papandreou C, Becerra-Tomas N, Bullo M, Martinez-Gonzalez MA, Corella D, Estruch R, et al. Legume consumption and risk of all-cause, cardiovascular, and cancer mortality in the PREDIMED study. Clin Nutr. 2019;38(1):348–56.
Sheflin AM, Borresen EC, Kirkwood JS, Boot CM, Whitney AK, Lu S, et al. Dietary supplementation with rice bran or navy bean alters gut bacterial metabolism in colorectal cancer survivors. Mol Nutr Food Res. 2017;61(1):1500905.
Borresen EC, Brown DG, Harbison G, Taylor L, Fairbanks A, O'Malia J, et al. A Randomized Controlled Trial to Increase Navy Bean or Rice Bran Consumption in Colorectal Cancer Survivors. Nutr Cancer. 2016;68(8):1269–80.
Borresen EC, Gundlach KA, Wdowik M, Rao S, Brown RJ, Ryan EP. Feasibility of Increased Navy Bean Powder Consumption for Primary and Secondary Colorectal Cancer Prevention. Curr Nutr Food Sci. 2014;10(2):112–9.
Song M, Zhang X, Meyerhardt JA, Giovannucci EL, Ogino S, Fuchs CS, et al. Marine ω-3 polyunsaturated fatty acid intake and survival after colorectal cancer diagnosis. Gut. 2017;66(10):1790–6.
David LA, Maurice CF, Carmody RN, Gootenberg DB, Button JE, Wolfe BE, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. 2014;505(7484):559–63.
Cotillard A, Kennedy SP, Kong LC, Prifti E, Pons N, Le Chatelier E, et al. Dietary intervention impact on gut microbial gene richness. Nature. 2013;500(7464):585–8.
Russell WR, Gratz SW, Duncan SH, Holtrop G, Ince J, Scobbie L, et al. High-protein, reduced-carbohydrate weight-loss diets promote metabolite profiles likely to be detrimental to colonic health. Am J Clin Nutr. 2011;93(5):1062–72.
Berg D, Clemente JC, Colombel JF. Can inflammatory bowel disease be permanently treated with short-term interventions on the microbiome? Expert Rev Gastroenterol Hepatol. 2015:1–15.
Graf D, Di Cagno R, Fak F, Flint HJ, Nyman M, Saarela M, et al. Contribution of diet to the composition of the human gut microbiota. Microb Ecol Health Dis. 2015;26:26164.
Wu GD, Chen J, Hoffmann C, Bittinger K, Chen YY, Keilbaugh SA, et al. Linking long-term dietary patterns with gut microbial enterotypes. Science. 2011;334(6052):105–8.
Sonnenburg ED, Smits SA, Tikhonov M, Higginbottom SK, Wingreen NS, Sonnenburg JL. Diet-induced extinctions in the gut microbiota compound over generations. Nature. 2016;529:212.
Schmidt TSB, Raes J, Bork P. The Human Gut Microbiome: From Association to Modulation. Cell. 2018;172(6):1198–215.
Dominguez-Bello MG, Godoy-Vitorino F, Knight R, Blaser MJ. Role of the microbiome in human development. 2019;68(6):1108–14.
Aron-Wisnewsky J, Clément K. The gut microbiome, diet, and links to cardiometabolic and chronic disorders. Nat Rev Nephrol. 2015;12:169.
Bultman SJ. The microbiome and its potential as a cancer preventive intervention. Semin Oncol. 2016;43(1):97–106.
Riscuta G, Xi D, Pierre-Victor D, Starke-Reed P, Khalsa J, Duffy L. Diet, Microbiome, and Epigenetics in the Era of Precision Medicine. In: Dumitrescu RG, Verma M, editors. Cancer Epigenetics for Precision Medicine : Methods and Protocols. New York: Springer New York; 2018. p. 141–56.
Gopalakrishnan V, Helmink BA, Spencer CN, Reuben A, Wargo JA. The Influence of the Gut Microbiome on Cancer, Immunity, and Cancer Immunotherapy. Cancer Cell. 2018;33(4):570–80.
Pullar JM, Chisholm A, Jackson C. Dietary information for colorectal cancer survivors: an unmet need. N Z Med J. 2012;125(1356):27–37.
Skeie G, Hjartaker A, Braaten T, Lund E. Dietary change among breast and colorectal cancer survivors and cancer-free women in the Norwegian Women and Cancer cohort study. Cancer Causes Control. 2009;20(10):1955–66.
Hawkes AL, Chambers SK, Pakenham KI, Patrao TA, Baade PD, Lynch BM, et al. Effects of a telephone-delivered multiple health behavior change intervention (CanChange) on health and behavioral outcomes in survivors of colorectal cancer: a randomized controlled trial. J Clin Oncol. 2013;31(18):2313–21.
Grimmett C, Simon A, Lawson V, Wardle J. Diet and physical activity intervention in colorectal cancer survivors: a feasibility study. Eur J Oncol Nurs. 2015;19(1):1–6.
Perera T, Young MR, Zhang Z, Murphy G, Colburn NH, Lanza E, et al. Identification and monitoring of metabolite markers of dry bean consumption in parallel human and mouse studies. Mol Nutr Food Res. 2015;59(4):795–806.
Acknowledgements
The authors wish to acknowledge the University of Texas MD Anderson Center’s Center for Energy Balance in Cancer Prevention and Survivorship; the Duncan Family Institute for Cancer Prevention and Risk Assessment; the Assessment, Intervention and Measurement (AIM) Core; the Bionutrition Research Core (BRC); the Kelsey Research Foundation; mentors Roberd (Robin) Bostick and Johanna Lampe; and most importantly, our participants and their families.
Funding
The BE GONE trial is funded by the American Cancer Society (RSG-17-049-01-NEC) and the University of Texas MD Anderson Cancer Center (Institutional Research Grant) to PI: C.R. Daniel. This study protocol has undergone peer review by the two funding bodies. X. Zhang is funded (in part) by a Research Training Award for Cancer Prevention Post-Graduate Training Program in Integrative Epidemiology from the Cancer Prevention & Research Institute of Texas, grant number RP160097 (PI: M. Spitz). K. M. Basen-Engquist, S.M. Hanash, P.C. Okhuysen, P. Scheet, S. Kopetz, and C.R. Daniel are funded (in part) through the National Cancer Institute Cancer Center Support Grant (CCSG 5P30 CA016672–37) to MD Anderson (PI: P. Pisters).
Author information
Authors and Affiliations
Contributions
CRD designed and drafted the protocol and secured funding for the study. XZ, GB, and WS assisted with the writing and organization of the protocol manuscript. GB and WS are responsible for patient recruitment and assisted with study documentation, data collection, and the development of the manual of procedures. Study co-investigators and collaborators KBE, SMH, KLH, PCO, PS, JFP, and SK provided critical consultation on study design and laboratory tests, as well as statistical and clinical expertise. CRD is the principal investigator/chair and SK is the physician co-chair of the protocol. All authors critically reviewed and approved the content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The trial is conducted in accordance with the Declaration of Helsinki. Individuals participate in the study voluntarily and provide written informed consent prior to beginning the study. Individuals are informed that they can cease their participation in the study at any time without disclosing reasons for their cancellation and without negative consequences for their future medical care. The ethics review board and all responsible ethics committees of The University of Texas MD Anderson Cancer Center approved the study protocol. This protocol underwent extensive and multi-level review including scientific evaluation by the MD Anderson Scientific Review Committee (SRC, formerly known as the Clinical Review Committee) and Psychosocial, Behavioral, and Health Services Research Committee (PBHSRC) and ethical evaluation by the Institutional Review Board (IRB). The MD Anderson Offices of Human Subjects Protection and Protocol Review and Reporting further support regulatory oversight, review, and monitoring of protocols. The trial has been registered at ClinicalTrials.gov (reference: NCT02843425).
Consent for publication
NA – The manuscript does not contain any reference or image pertaining to an individual or research participant.
Competing interests
The authors declare that they have no competing interests. The funders did not play a role in the study design; collection and management; writing of the report; and the decision to submit the report for publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zhang, X., Browman, G., Siu, W. et al. The BE GONE trial study protocol: a randomized crossover dietary intervention of dry beans targeting the gut microbiome of overweight and obese patients with a history of colorectal polyps or cancer. BMC Cancer 19, 1233 (2019). https://doi.org/10.1186/s12885-019-6400-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-019-6400-z