
Abstract
Background
Chemotherapy-induced thrombocytopenia (CIT) is a potentially serious complication that can lead to chemotherapy dose delays, dose reductions, or discontinuation, and increases the risk of serious bleeding events. The objectives of this study were to characterize the incidence, clinical consequences, and economic costs of CIT in current US clinical practice.
Methods
A retrospective cohort design and data from two US private healthcare claims repositories (01/2010–12/2016) were employed. Study population comprised adults who received selected myelosuppressive chemotherapy regimens for solid tumors or non-Hodgkin’s lymphoma. CIT was identified based on: diagnosis code for thrombocytopenia or bleeding; procedure code for platelet transfusion or bleeding control; or drug code for thrombopoietin-receptor agonist. Incidence of CIT was evaluated during the chemotherapy course (max. no. cycles = 8), and associated consequences and costs (2016US$) were evaluated during the cycle of the CIT episode.
Results
Among 215,508 cancer chemotherapy patients, CIT incidence during the course (mean no. cycles = 4.6) was 9.7% (95% CI: 9.6–9.8), and ranged from 6.1% (5.9–6.3) for regimens containing cyclophosphamide to 13.5% (12.7–14.3) for regimens containing gemcitabine; among all patients, incidence was 2.7% (2.6–2.8) in cycle 1, 2.7% (2.6–2.8) in cycle 2, and 2.9% (2.9–3.0) in cycles thereafter. One-third of CIT episodes were managed in hospital, and for the subset of patients hospitalized with a first-listed diagnosis of CIT, mean length of stay was 4.6 (4.4–5.0) days and mean cost of inpatient care was $36,448 (32,332-41,331). Across cycles with CIT, mean cost of CIT-related care was $2179 (2029-2329), comprising $1024 (881–1167) for inpatient care and $1153 (1119-1187) for outpatient care.
Conclusions
In this retrospective evaluation of cancer chemotherapy patients, CIT incidence was high, especially among patients receiving gemcitabine-based regimens, and the costs of CIT-related care were substantial. Accordingly, interventions aimed at identifying and targeting high-risk patients for preventative measures may yield substantial clinical and economic benefits.
Similar content being viewed by others


Background
Thrombocytopenia, an abnormally low blood platelet count, is a potentially serious and costly complication of myelosuppressive chemotherapy [1, 2]. Chemotherapy-induced thrombocytopenia (CIT) can complicate surgical procedures and can lead to chemotherapy dose delays, dose reductions, or discontinuation, which may result in suboptimal patient outcomes, and CIT increases the likelihood of serious bleeding events, which may result in hospitalization [2,3,4,5,6,7]. Currently, there are no drugs approved by the United States (US) Food and Drug Administration for the treatment of CIT, and thus options consist of reducing the intensity of or eliminating the offending treatment, platelet transfusions, or pharmacotherapy, although such options are not without risks and costs [1, 3, 4, 8].
Notwithstanding the potential implications of CIT, little is known about the incidence and consequences of this condition in current US clinical practice. To date, only two studies have evaluated the incidence of CIT using US data sources, and the data employed in these studies are now more than a decade old [2, 4]. Moreover, the study by Hitron et al. was based on a small sample of cancer patients receiving high-risk chemotherapy regimens from a single center, while that by Wu and colleagues was based on an electronic medical records database that did not include important information on characteristics of the study population. In addition, only one study has reported the results of a formal evaluation of the cost of CIT, and this study was based on a sample of 75 patients receiving chemotherapy over 20 years ago [5].
Since the incidence, severity, and duration of CIT varies across patient populations and chemotherapy regimens, and because the treatment of cancer has changed markedly over the past two decades, available evidence may not be reflective of current US clinical practice. The current study was therefore undertaken to evaluate the incidence and consequences of CIT among patients receiving selected myelosuppressive chemotherapy regimens for solid tumors or non-Hodgkin’s lymphoma (NHL) using data from two large healthcare claims repositories. The findings of this research were presented, in part, at the American Society of Clinical Oncology (ASCO) Annual Meeting, June 1–5, 2018 [9].
Methods
Study design and data sources
This study employed a retrospective cohort design and data from two large healthcare claims repositories spanning the period from January 1, 2010 through December 31, 2016. A detailed description of study methods—design, data source, and operational algorithms for selecting patients as well as identifying all other study variables (including corresponding diagnosis, procedure, and drug codes)—is set forth in Online Additional file 1.
Patient-level claims data from the two repositories were pooled to increase the precision and generalizability of study findings. The two study repositories―Truven Health Analytics MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits Databases (“MarketScan Database”), and IQVIA Real-World Data Adjudicated Claims PharMetrics Plus Database (“PharMetrics Database”)―comprise medical (i.e., facility and professional service) claims and outpatient pharmacy claims from a large number of participating private US health plans. The study databases were de-identified prior to their release to study investigators, and thus their use for health services research was fully compliant with the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule and federal guidance on Public Welfare and the Protection of Human Subjects (45 CFR 46 §46.101).
Source and study populations
The source population comprised patients aged ≥18 years who, between January 1, 2011 and December 31, 2015, initiated ≥1 course of myelosuppressive chemotherapy for a single primary solid tumor or NHL. For each patient in the source population, the first unique observed course of chemotherapy, and each cycle (up to 8 in total) within the first course, was identified. Patients were excluded from the source population if they had: < 6 months of continuous health benefits prior to chemotherapy initiation (e.g., if they were recently enrolled in a participating health plan, and thus their healthcare claims data were not available prior to this period); evidence of stem cell therapy or bone marrow transplant during the 12-month period preceding chemotherapy or during the chemotherapy course; evidence of thrombocytopenia during the 12-month period preceding chemotherapy; or evidence of secondary causes of thrombocytopenia during the 12-month period preceding chemotherapy or during the chemotherapy course.
From the source population, all patients who received chemotherapy regimens including ≥1 agent of interest—carboplatin, cisplatin, cyclophosphamide, fluorouracil, gemcitabine, oxaliplatin, and vincristine—were included in the study population, and all such patients were included in ≥1 non-mutually-exclusive subgroup based on receipt of the agents of interest. The agents of interest were selected based on previously published research suggesting that patients receiving chemotherapy regimens including these drugs were at elevated risk of CIT [1, 7, 10].
Study outcomes
Episodes of CIT
Episodes of CIT were ascertained on a cycle-specific basis during the chemotherapy course, from day 7 of each chemotherapy cycle through the end of the cycle, and were identified based on inpatient/outpatient medical claims with a diagnosis code (in any position) for thrombocytopenia (primary, secondary, or unspecified) or bleeding, or a procedure code for bleeding treatment, platelet transfusion, or receipt of a thrombopoietin receptor agonist (TPO-RA). CIT episodes identified in the ambulatory setting that preceded/followed CIT episodes identified in the inpatient setting during the same cycle were considered part of the inpatient episode (for purposes of stratifying CIT episodes by care setting).
Clinical and economic consequences of CIT
For each CIT episode, consequences were evaluated within the cycle of occurrence and included hospital admissions with a first-listed diagnosis code for thrombocytopenia or bleeding; ambulatory encounters with a diagnosis code for thrombocytopenia or bleeding, or a procedure code for selected transfusions, laboratory tests, control of bleeding, or CIT-related medications (i.e., glucocorticosteroids, immunoglobulin, and TPO-RAs); or outpatient pharmacotherapy with CIT-related medications. For CIT-related hospital admissions, consequences were characterized in terms of hospital length of stay, hospital mortality, diagnoses, and cost per admission, as well as in terms of the number of hospitalizations, number of hospital days, and hospital costs per patient-episode. For CIT-related ambulatory encounters, consequences were characterized in terms of care setting, diagnoses, procedures, outpatient pharmacotherapy, and cost per encounter, as well as in terms of the number of ambulatory encounters and ambulatory costs per patient-episode. Numbers and costs of outpatient CIT-related medications per patient-episode, and total cost per patient-episode, were also tallied. Costs were expressed in 2016US$, and were based on amounts paid by health plans and patients for services rendered by providers.
Patient characteristics
Characteristics of the study population included age; sex; chronic comorbidities; nutritional status; history of other conditions/events prior to chemotherapy; measures of health status and physical function. All baseline characteristics were assessed during the 12-month period preceding chemotherapy initiation, except for recent surgery, which was evaluated during the 90-day period prior to chemotherapy.
Statistical analyses
Crude risk of CIT—overall and by care setting—was summarized for all patients and for subgroups defined therein based on the agent of interest using incidence proportions and corresponding 95% confidence intervals (CIs); the latter were generated using the Wilson score interval method. CIT-related admissions, ambulatory encounters, and costs were summarized using means, frequencies, and corresponding 95% CIs, which were calculated using techniques of non-parametric bootstrapping. Since some of our measures of CIT-related care (e.g., red blood cell transfusions, labs, and pharmacotherapy) may capture services provided for other reasons (i.e., other than CIT), measures were also evaluated during cycles in which CIT episodes did not occur among our study population, for purposes of comparison. All analyses were also conducted within subgroups defined on cancer type as well as cancer type and chemotherapy agent.
Results
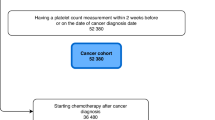
The two study databases included a total of 643,676 patients aged ≥18 years who received myelosuppressive chemotherapy between January 1, 2011 and December 31, 2015 (Table 1). Among these patients, 332,512 (52%) met all remaining inclusion/exclusion criteria and qualified for inclusion in the source population. From the source population, 215,508 patients also received chemotherapy regimens including an agent of interest—mostly commonly, cyclophosphamide (39%) and carboplatin (28%)—and thus qualified for inclusion in the study population. Mean (SD) age of study population was 57.3 (11.3) years, and 70% were female (Table 2). Common comorbidities included cardiovascular disease (16%), lung disease (16%), and diabetes (15%), and a large percentage of patients had a history of infection (61%) or anemia (21%). Characteristics of patients in subgroups defined in cancer type as well as cancer type and chemotherapy agent (Online Additional file 2: Table S1a-b) and characteristics of chemotherapy regimens and supportive care (Online Additional file 2: Table S2) are reported in Online Additional file 2.
Incidence of CIT during the chemotherapy course was 9.7% (95% CI: 9.6–9.8) among all patients in the study population, and ranged from 6.1% (5.9–6.3) among those receiving a cyclophosphamide-based regimen to 13.5% (12.7–14.3) among patients receiving a gemcitabine-based regimen; CIT incidence among patients receiving regimens including carboplatin was 13.2% (12.9–13.5) (Table 3). Incidence of CIT among all patients was 2.7% (2.6–2.8) in cycle 1, 2.7% (2.6–2.8) in cycle 2, and 2.9% (2.9–3.0) in subsequent cycles. Approximately one-third of CIT episodes were managed in hospital.
For hospital admissions with a principal diagnosis of CIT, mean length of stay was 4.6 (4.4–5.0) days, hospital mortality was 4.7% (2.8–6.6), and mean cost of inpatient care was $36,448 (32,332-41,331) (Table 4). For CIT-related ambulatory encounters, most of which occurred in a physician’s office (45%) or hospital outpatient department (41%), mean cost per encounter was $123 (121–125) for the former and $504 (486–524) for the latter. Across cycles with CIT, irrespective of care setting, mean number of CIT-related admissions was 0.03 (0.03–0.03) per patient-episode, and the mean number of CIT-related ambulatory encounters was 3.7 (3.7–3.8) per patient-episode; the total cost of CIT-related care was $2179 (2029-2329) per patient-episode, comprising $1024 (881–1167) for inpatient care and $1153 (1119-1187) for outpatient care. For purposes of comparison, across cycles without CIT, the cost of selected transfusions, labs, and pharmacotherapy (i.e., services that may have been provided for reasons other than CIT) totaled $271 (265–278) per patient-cycle. Incidence and burden of CIT within subgroups defined on cancer type as well as cancer type and chemotherapy agent are reported in Online Additional file 2 (Online Additional file 2: Table S3a-4b).
Discussion
Using a retrospective cohort design and data from two large healthcare claims repositories, we undertook an evaluation to better understand the current epidemiology and burden of CIT among persons receiving selected myelosuppressive chemotherapy regimens for solid tumors or NHL in US clinical practice. Our findings indicate that the incidence of CIT during the chemotherapy course is high (~ 10%), especially among patients receiving gemcitabine- or carboplatin-based chemotherapy regimens. Because episodes of CIT were identified based on evidence of thrombocytopenia or bleeding documented during healthcare encounters (and not via laboratory results), we believe our algorithm disproportionately captures more severe cases of disease and thus our estimates may not be reflective of the overall incidence of CIT including all cases, irrespective of disease severity.
Our estimates of CIT incidence are, not surprisingly, generally lower than those previously published, presumably due in large part to differences in case-ascertainment algorithms. In the study by Wu and colleagues, which utilized electronic medical records for patients (n = 47,159) treated in US oncology clinics between 2000 and 2007, CIT incidence—defined as a platelet count < 150 × 109 /L—among all patients was estimated to be 41.4%, ranging from 21.2% among patients receiving taxane-based regimens to 64.2% among patients who received gemcitabine-based regimens [2]. However, when employing the same threshold for CIT as employed in the smaller study published by Hitron et al. (i.e., platelet count < 75 × 109 /L, which along with other evidence, was considered to be clinically significant), overall incidence based on data from Wu et al. was calculated to be 13.8%. This estimate based on data from Wu et al. is comparable to CIT incidence reported by Hitron and colleagues (11.2%), CIT incidence reported in an ex-US study (11.9%, with CIT defined as platelet count < 75 × 109 /L), as well as that reported in the current study [4, 11].
Our findings also indicate that the economic costs of CIT-related care are substantial, averaging $2179 per episode, or $1908 more than cycles without CIT. Notwithstanding differences in study design, study populations, and CIT definitions, our estimate of the cost of CIT-related care is comparable to that reported previously by Elting and colleagues [5]. In their 2003 analysis of 75 patients with a solid tumor or lymphoma who developed thrombocytopenia during chemotherapy treatment, mean incremental cost of CIT was estimated to be $1037 in 1999US$, or $2011 in 2016US$. Among our 27,913 cycles with evidence of CIT, 75% (n = 20,920) had evidence of bleeding, and CIT-related costs in these cycles were substantially higher than in the 25% (n = 6993) of cycles without evidence of bleeding. In cycles with bleeding, mean costs of CIT-related care (per patient-episode) totaled $2632, including $1349 for CIT-related hospital admissions and $1281 for CIT-related ambulatory care; corresponding values for cycles without bleeding were $823 (total), $51 (hospital), and $770 (ambulatory).
We note several potential biases vis-à-vis patient (treatment) selection and outcome assessment that may impact the findings of this study as well as important limitations. The accuracy of the algorithm for identifying patients receiving chemotherapy for solid tumors and NHL is unknown, as it has not been validated. However, similar algorithms for identifying cancer chemotherapy patients in healthcare claims databases have been employed in several previously published studies [12,13,14]. Because a diagnosis code for CIT does not exist, and the study database does not include results of laboratory tests (i.e., platelet counts), an algorithm based on diagnosis codes for thrombocytopenia and bleeding, and procedure codes for bleeding treatment, platelet transfusion, and TPO-RA therapy, was employed to identify CIT. While the accuracy of this algorithm is unknown, we suspect—as noted above—that patients with less severe CIT may be disproportionately under-represented, and thus the estimated cost of CIT-related care must be interpreted accordingly. We also note that because thrombocytopenia, neutropenia, and anemia are all known hematological toxicities of myelosuppressive chemotherapy, the reported incremental cost of CIT may be, to some extent, confounded by the presence of anemia and/or neutropenia, and the impact of such bias is unknown. Algorithms and variables employed to identify chronic comorbidities and acute illnesses have not been validated, and their accuracy is unknown; also, some patients may be misclassified in terms of their characteristics because healthcare claims are available only during the study period. Data on hospital discharge disposition were available only in the MarketScan Database, and thus were assumed to be generalizable to the overall population of patients hospitalized for CIT. Health plans contributing claims data to the two study databases are different. However, patients may be insured by more than one health plan at the same time, and thus their healthcare claims may be included in both of the study databases; the magnitude of overlap is believed to be negligible. Finally, caution is warranted in generalizing results beyond this evaluation as the study population was disproportionately represented by non-elderly patients with commercial healthcare coverage.
Conclusions
In conclusion, in this retrospective evaluation of cancer chemotherapy patients, CIT incidence was high, especially among patients receiving gemcitabine-based regimens, and the costs of CIT-related care were substantial. Accordingly, interventions aimed at identifying and targeting patients at high risk of CIT for preventative measures may yield substantial clinical and economic benefits.
Abbreviations
- ASCO:
-
American Society of Clinical Oncology
- CI:
-
Confidence interval
- CIT:
-
Chemotherapy-induced thrombocytopenia
- HIPAA:
-
Health Insurance Portability and Accountability Act
- MarketScan Database:
-
Truven Health Analytics MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits Databases
- NHL:
-
Non-Hodgkin’s lymphoma
- PAI:
-
Policy Analysis Inc.
- PharMetrics Database:
-
IQVIA Real-World Data Adjudicated Claims PharMetrics Plus Database
- TPO-RA:
-
Thrombopoietin receptor agonist
- US:
-
United States
References
Kuter DJ. Managing thrombocytopenia associated with cancer chemotherapy. Oncology (Williston Park). 2015;29:282–94.
Wu Y, Aravind S, Ranganathan G, Martin A, Nalysnyk L. Anemia and thrombocytopenia in patients undergoing chemotherapy for solid tumors: a descriptive study of a large outpatient oncology practice database, 2000-2007. Clin Ther. 2009;31:2416–32.
Demetri GD. Targeted approaches for the treatment of thrombocytopenia. Oncologist. 2001;6(Suppl 5):15–23.
Hitron A, Steinke D, Sutphin S, Lawson A, Talbert J, Adams V. Incidence and risk factors of clinically significant chemotherapy-induced thrombocytopenia in patients with solid tumors. J Oncol Pharm Pract. 2011;17:312–9.
Elting LS, Cantor SB, Martin CG, et al. Cost of chemotherapy-induced thrombocytopenia among patients with lymphoma or solid tumors. Cancer. 2003;97:1541–50.
Tiwari R, Mandal DK, Patel J. A post marketing randomized placebo controlled study to evaluated the efficacy of study product UPLAT® (Carica papaya leaf extract + Tinospora cordifolia extract) in the cancer patients with thrombocytopenia induced by chemotherapy. Int J Clin Trials. 2018;5(4):170–6.
Elting LS, Rubenstein EB, Martin CG, et al. Incidence, cost, and outcomes of bleeding and chemotherapy dose modification among solid tumor patients with chemotherapy-induced thrombocytopenia. J Clin Oncol. 2001;19:1137–46.
Rodeghiero F, Carli G. Beyond immune thrombocytopenia: the evolving role of thrombopoietin receptor agonists. Ann Hematol. 2017;96:1421–34.
Weycker D, Hatfield M, Hanau A, et al. Risk and cost of chemotherapy-induced thrombocytopenia (CIT) in US clinical practice. J Clin Oncol. 2018;36(15_suppl):e18911. https://doi.org/10.1200/JCO.2018.36.15_suppl.e18911.
Tamamyan G, Danielyan S, Lambert MP. Chemotherapy induced thrombocytopenia in pediatric oncology. Crit Rev Oncol Hematol. 2016;99:299–307.
Ten Berg MJ, van den Bemt PM, Shantakumar S, et al. Thrombocytopenia in adult cancer patients receiving cytotoxic chemotherapy: results from a retrospective hospital-based cohort study. Drug Saf. 2011;34:1151–60.
Weycker D, Li X, Tzivelekis S, et al. Burden of chemotherapy-induced febrile neutropenia hospitalizations in US clinical practice, by use and patterns of prophylaxis with Colony-stimulating factor. Support Care Cancer. 2017;25:439–47.
Weycker D, Bensink M, Wu H, Doroff R, Chandler D. Risk of chemotherapy-induced febrile neutropenia with early discontinuation of pegfilgrastim prophylaxis based on real-world data from 2010 to 2015. Curr Med Res Opin. 2017;33:2115–20.
Weycker D, Bensink M, Lonshteyn A, Doroff R, Chandler D. Risk of chemotherapy-induced febrile neutropenia by day of pegfilgrastim prophylaxis in US clinical practice from 2010 to 2015. Curr Med Res Opin. 2017;33:2107–13.
Acknowledgements
The findings of this research were presented, in part, at the American Society of Clinical Oncology (ASCO) Annual Meeting, June 1-5, 2018.
Funding
Funding for this research was provided by Amgen Inc. to PAI. The study sponsor reviewed the study research plan and study manuscript; data management, processing, and analyses were conducted by PAI, and all final analytic decisions were made by study authors.
Availability of data and materials
There are restrictions on data sharing, as the study employed extracts comprising healthcare claims from the Truven Health Analytics MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits Databases and the IQVIA Real-World Data Adjudicated Claims PharMetrics Plus Database. The data are proprietary, provided by third-party vendors, and the authors do not have permission to disseminate these data without approval of the vendors.
Author information
Authors and Affiliations
Contributions
Authorship was designated based on the guidelines promulgated by the International Committee of Medical Journal Editors (2004). All persons who meet criteria for authorship are listed as authors on the title page. The contribution of each of these persons to this study is as follows: (1) conception and design (DC, AG, AH, MH, AS, DW), acquisition of data (DC, AH, MH, AL, AS, DW), analysis or interpretation of data (all authors); and (2) preparation of manuscript (AG, AH, DW), critical review of manuscript (DC, MH, AL, AS). All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The data extracts were de-identified prior to their release to study investigators, and thus their use for health services research is compliant with the HIPAA Privacy Rule and federal guidance on Public Welfare and the Protection of Human Subjects. This research is thus exempt from IRB review.
Consent for publication
Not applicable.
Competing interests
Aaron Grossman, Ahuva Hanau, Alexander Lonshteyn, and Derek Weycker are employed by PAI. David Chandler, Mark Hatfield, and Anjali Sharma are employed by, and own stock in, Amgen Inc.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Risk and Consequences of CIT v5, Study Methods and Appendices, description of study methods and operational algorithms/codes used to define study variables. (DOC 312 kb)
Additional file 2:
Risk and Consequences of CIT v2.1, Supplemental Findings, description of results from analyses within subgroups defined on cancer type and chemotherapy agent. (XLSX 327 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Weycker, D., Hatfield, M., Grossman, A. et al. Risk and consequences of chemotherapy-induced thrombocytopenia in US clinical practice. BMC Cancer 19, 151 (2019). https://doi.org/10.1186/s12885-019-5354-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-019-5354-5