
Abstract
Background
Radiogenic angiosarcoma of the breast (RASB) is a rare late sequela of local irradiation of the breast or chest wall after breast cancer. The prognosis of women with RASB is poor and there is no standardized therapy for this type of malignancy.
Case presentation
We present the case of a 54 year old woman with RASB (poorly differentiated angiosarcoma of the left breast; pT1, pNX, M0, L0, V0) and a history of invasive-ductal cancer of the left breast (pT1b, G2, pN0, ER positive, PR positive, HER-2/neu negative) treated in July 2012 with breast-conserving surgery, adjuvant chemotherapy with 6 cycles of epirubicin and cyclophosphamide, adjuvant irradiation of the left breast with 50 Gray, and adjuvant endocrine therapy with an aromatase inhibitor. In August 2016, a bilateral salpingo-oophorectomy was performed to remove a tumor of the left ovary, which was diagnosed as breast cancer recurrence. At the same time, a small, purple skin lesion of 1.2 cm in diameter was noted in the inner upper quadrant of the right breast. RASB was diagnosed by punch biopsy and the tumor was excised with clear margins. Imaging studies showed no evidence of further metastases. A systemic chemotherapy with 6 cycles of liposomal doxorubicin was initiated. Five months later, a local recurrence of RASB was diagnosed and mastectomy was performed. Six months later, the patient is alive with no evidence of disease.
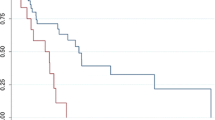
Three hundred seven cases of RASB were identified. The pooled incidence rate of RASB was 1/3754 women. The most common treatment of RASB was mastectomy in 83% of cases. Adjuvant radiotherapy or chemotherapy were rarely used with 6 and 4%, respectively, whereas in case of recurrence, chemotherapy was the mainstay of treatment, used in 58% of cases. Radiotherapy and repeated surgery were also common with 30 and 33% of cases, respectively. Overall, the prognosis of women with RASB was poor and the recurrence-free survival was short with a mean of 15.9 months. Mean overall survival was 27.4 months.
Conclusion
RASB is a rare late complication of breast irradiation. The prognosis of women with RASB is poor. Surgery is the mainstay of treatment for localized disease while systemic chemotherapy and re-irradiation are appropriate for women with disseminated or recurrent RASB.
Similar content being viewed by others
Background
Angiosarcoma of the breast is an unusual malignancy accounting for less than 1% of all soft tissue sarcomas [1]. It may develop spontaneously or subsequent to breast irradiation in women after surgical treatment of breast cancer. Sporadic angiosarcoma of the breast is extremely rare. For example, in a Danish region with a population of 1.25 million, Holm et al. identified 42 cases over a period of 35 years for a yearly population-based incidence of 1 in 1 million [2]. In contrast, radiogenic angiosarcoma of the breast (RASB) is much more common among women with a history of breast irradiation. Spontaneous and radiogenic angiosarcomas are morphologically undistinguishable, but there are notable pathogenetic differences. For example, Lae et al. compared the c-myc amplification on chromosome 8q24.21 in 32 RASB specimens and 15 sporadic angiosarcoma specimens [3]. Amplification (5- to 20-fold) of the c-myc oncogene was found in all RASB cases but only in one sporadic angiosarcoma demonstrating a specific oncogenic pathway for RASB. These data also suggest that c-myc may be a potential target for a targeted therapy of RASB.
Typically, RASB is diagnosed as a late sequela of breast irradiation following breast-conserving surgery for invasive breast cancer. In a series of 8 women with RASB treated over a period of 9 years, the cumulative incidence of RASB in the investigated population of women with breast cancer and breast irradiation was 0.14% [4]. Marchal et al. collected follow-up data of 18,115 breast cancer patients from 11 French cancer centers and identified 9 cases of RASB for an incidence of 5/10000 women [5]. In this retrospective case series, the median latency period between breast irradiation and the diagnosis of RASB was 74 (range 57 to 108) months. The prognosis of women with RASB in this case series was poor with 8/9 patients developing early recurrence with a median overall survival time of only 15 months. These data are consistent with a large series of 79 women with RASB from the Memorial-Sloan Kettering Cancer Center demonstrating a high rate of local and distant recurrences and poor survival [6]. In this study, the median interval between breast irradiation and RASB was 7 years and the median time interval between the first treatment of RASB and local or distant recurrence was 1.3 and 2.5 years, respectively. Median survival was 2.9 years. Of note, older age and deep infiltrating RASB were independent predictors of poor survival.
The clinical presentation of RASB is diverse. Lesions are often described as small, purple, teleangiectasia-like formations and may appear as nodules, plaques, or patches [3,4,5,6]. RASB often present as multiple, distinct lesions. Thus, a thorough clinical examination is important in order not to overlook satellite lesions. RASB can have different colours, but are mostly described as purple, blue, or black. Another important issue is diagnostic delay. Clearly, RASB is a rare finding and the clinical presentation is uncharacteristic. Therefore, in many patients described in the literature, a substantial time delay between the first notice of the lesion and the final diagnosis of RASB, which requires a histological specimen, has been noted [7, 8].
Due to the rarity of RASB, there is no standardized therapy regimen for women with this disease. Radical surgery of the tumor either by local resection or mastectomy is the most commonly cited treatment [4,5,6] and complete tumor resection is associated with an improved prognosis. For example, in a series of 21 women with RASB from the Netherlands, Strobbe et al. reported a 2 year overall survival rate of 86% after complete surgical resection compared to 0% after incomplete resection of the tumor [9]. In contrast to the well-established role of surgery, the value of re-irradiation and systemic chemotherapy is less clear. For example, in the series of D’Angelo et al. [6], 78 of 79 women underwent local surgery. Synchronous or metachronous chemotherapy was used in case of unresectable or metastatic disease and was applied to 23 of 79 patients. The most commonly used chemotherapy regimens in this patient cohort were liposomal doxorubicin and paclitaxel. In addition, the mTOR inhibitor sirolimus and targeted therapies such as sorafenib and brivanib were used empirically after chemotherapy had failed. In the treatment of metastatic soft tissue sarcomas and other non-gynecological sarcomas, pazopanib, sirolimus, and brivanib have been described to be active substances after the failure of standard chemotherapy [6, 10, 11]. Re-irradiation or adjuvant chemotherapy were not reported in this patient collective. However, re-irradiation of the breast in women with RASB is feasible and may be associated with a good long-term outcome in selected cases. For example, Smith et al. used hyperfractionated and accelerated re-irradiation with 45 to 75 Gray alone or combined with surgery in 14 women with RASB and reported a median survival of 7 years [12].
To highlight the clinical characteristics, management, and prognosis of women with RASB, we report the case of a woman with histologically verified RASB. In addition, we present a systematic review of the literature with cohort studies, case series, and case reports of women with RASB and discuss the most common therapies and respective outcomes.
Case presentation
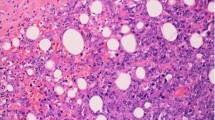
We present the case of a 54 year old woman with RASB (poorly differentiated angiosarcoma of the left breast; pT1a, pNX, M0, L0, V0) after a history of invasive-ductal cancer of the left breast, pT1c (1.8 cm), G3, pN3a (22/23), L1, V0, M0, ER positive, PR positive, HER-2/neu negative) treated in July 2012 with breast-conserving surgery with clear resection margins, adjuvant chemotherapy with 6 cycles of epirubicin and cyclophosphamide, adjuvant irradiation of the left breast and left axillary, supra-, and infraclavicular region with 50 Gray, and adjuvant endocrine therapy with the aromatase inhibitor anastrozole. In August 2016, a bilateral salpingo-oophorectomy was performed to remove a tumor of the left ovary, which was diagnosed as distant breast cancer recurrence. At the same time, in August 2016, a small, purple skin lesion of 1.2 cm in diameter was noted in the inner upper quadrant of the right breast. RASB was diagnosed by punch biopsy and the tumor was completely excised. Staging procedures (computed tomography scans of the thorax and abdomen, bone scintigraphy) showed no evidence of further recurrence. A systemic second-line chemotherapy with 6 cycles of liposomal doxorubicine was initiated. Five months later, a local recurrence of RASB was diagnosed and mastectomy was performed. Staging procedures (computed tomography scans of the thorax and abdomen, bone scintigraphy) were again performed and showed no evidence of distant metastases. No further chemotherapy was applied. After 5 months of follow-up, the patient is alive with no evidence of disease. Figure 1 shows the histological presentation of the RASB in the mastectomy specimen of the left breast as well as immunohistochemical stainings for proliferation marker protein Ki-67, platelet endothelial cell adhesion molecule (PECAM-1), trans-acting T-cell-specific transcription factor GATA-3, and cytokeratins. The tumor demonstrated strong positivity for MIB1 and PECAM-1, but negativity for GATA-3 and cytokeratin. Figure 2 shows an image of the initial RASB diagnosed in August 2016.

Hematoxylin-eosin (H&E) (a) and immunohistochemical (b–e) stains of a radiogenic angiosarcoma of the breast. The specimen demonstrated expression of proliferation marker protein Ki-67 and platelet endothelial cell adhesion molecule (PECAM-1), but no expression of trans-acting T-cell-specific transcription factor GATA-3 or cytokeratins (CK) was detected. Black bars, 50 μm

Hematoxylin-eosin (H&E) stain of the initial radiogenic angiosarcoma of the breast
In general, angiosarcomas including RASB are high-grade tumors of endothelial origin. They arise from small blood or lymphatic vessels and display varying degrees of nuclear atypia, hyperchromatic nuclei, large nucleoli, and frequent mitoses. Ultrastructural findings may include Weibel-Palade bodies (tubular structures found in normal endothelium) and pinocytic vesicles. Areas of hemorrhage into the surrounding stroma may also be present [1]. Pathology typically shows stratified squamous epithelium and a superficial dermal based proliferation of large, plump, atypical spindled and epithelioid cells with large, pleomorphic vesicular nuclei and prominent nucleoli [5, 10, 13, 14]. Additional typical features including spindle cells with pleomorphic epithelioid eosinophilic cytoplasm and small papillary proliferations.
Literature review
In a systematic literature search of the databases PubMed and Cochrane Central Register of Controlled Trials (search date 13–04-2017) using the search terms postirradiation[All Fields] AND (“hemangiosarcoma”[MeSH Terms] OR “hemangiosarcoma”[All Fields] OR “angiosarcoma”[All Fields]) AND (“therapy”[Subheading] OR “therapy”[All Fields] OR “treatment”[All Fields] OR “therapeutics”[MeSH Terms] OR “therapeutics”[All Fields]), we identified 39 citations. After screening all abstracts, 17 citations were identified reporting on women with RASB, defined for the purpose of this review as angiosarcoma of the breast after a history of ipsilateral invasive breast cancer and subsequent breast or chest wall irradiation independent of the time interval between breast irradiation and RASB [4, 13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. Studies not reporting on women with RASB, double publications, and studies reporting on women with primary angiosarcomas were excluded. The 17 identified studies were retrieved in full and cross reference searching was performed and identified 58 further studies reporting on women with RASB [5,6,7,8,9, 12, 29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80]. Therefore, in summary, 75 studies were analyzed for this review. Figure 3 shows a flow diagram of the literature search algorithm. Among the 75 studies, we found 8 retrospective cohort studies, 18 retrospective cases series, and 49 case reports. No prospectively collected data were identified. Only 5 studies reported on > 10 patients with RASB describing 79 [6], 21 [9], 14 [12], 31 [45], and 27 [64] cases, respectively. Table 1 shows the study characteristics and outcomes of patients with RASB described in all 75 studies. In summary, 307 cases of RASB have been reported in the literature. Seven studies described the patient populations within which RASB cases were identified [5, 9, 19, 21, 24, 45, 53], thus allowing for a calculation of the incidence of RASB. The respective incidences given in these studies were 9/18115 [5], 21/16500 [9], 4/423 [19], 2/5100 [21], 1/3120 [24], 31/220000 [45], and 3/3295 [53] for a pooled incidence rate of 1/3754.

Flow diagram of the literature search algorithm. RASB, radiogenic angiosarcoma of the breast
At the time of first presentation, single or multiple local lesions were described in 162 cases. Single and multiple lesions were evenly distributed with 87 and 75 cases, respectively. The mean time between breast cancer irradiation and the diagnosis of RASB was 77.2 months.
Treatment modalities and outcomes are shown in Table 2. The most commonly used treatment of RASB was mastectomy reported in 85% of cases. Adjuvant chemotherapy or adjuvant irradiation was rarely given with 4 and 6% of cases reported in the pooled analysis. After recurrence of RASB, however, chemotherapy was most often used with 58% of cases. There is no standard chemotherapy regimen for RASB, but anthracyclines and taxanes were the most commonly used substances. In addition, ifosfamide, doxorubicine, and gemcitabine were reported alone or in combination with anthracyclines and taxanes. Irradiation and repeated surgery were also common treatment modalities in women with recurrent RASB and have been reported in 30 and 33% of cases, respectively. Overall, the prognosis of women with RASB was poor. The recurrence-free survival was short with a mean of 15.9 months and overall survival was 27.4 months.
The largest cohort of women with RASB was published by D’Angelo et al. [6]. The authors described 79 women with RASB treated at the Memorial Sloan Kettering Cancer Center between 1982 and 2011. In this study, the diagnosis of RASB was defined pathologically by the presence of solid growth with variable angioformative features and overt cytologic atypia. Almost all women were initially treated with surgery, either mastectomy (65 cases) or local excision (13 cases). Complete RASB resection with free resection margins was achieved in 52/79 (66%) of cases. Follow-up data were available for 65 women, of whom 37 (60%) were still alive after a median follow-up of 4.5 years. The importance of radical initial surgery was underlined by a univariate analysis demonstrating that resection margin status was the single most important prognostic factor regarding distant recurrence-free survival. Older age and deeply infiltrating RASB (as opposed to superficial disease) were independent prognostic factors for disease-specific survival.
Three other large patient cohorts including 31 [45], 27 [64], and 21 [9] cases of RASB were identified. In line with the data of D’Angelo et al., Hodgson et al. reported mastectomy as the treatment of first choice in 81% and an overall mortality of 58% [45]. In a series of 27 cases, Billings et al. found that the median interval between breast irradiation and the diagnosis of RASB was 59 months [64]. Only in 5 women RASB occurred within less than 3 years after breast irradiation. Lymphedema was not a typical presentation of RASB. Multifocal appearance at first diagnosis was noted in half of the cases (13 of 27 cases) and all tumors had a vasoformative growth pattern. Other features characteristic for the histological appearance of RABS were a sieve-like pattern and high-grade nuclear features, whereas necroses were rare. All women were initially treated surgically with wide excision or mastectomy. Fourteen women experienced local recurrence and 6 had multiple recurrences. Metastasis was documented in 9 of 22 patients, 8 of whom died of the disease. Strobbe et al. collected data on 21 RASB cases diagnosed in the Netherlands between 1987 and 1995 [9]. In this series, the median interval between breast irradiation and RASB was 74 months and appeared to decrease with higher age. The 2 year overall and disease free survival rates were 72 and 35%, respectively. In accordance with the previously cited studies, complete initial resection of RASB was also an important prognostic factor with a 2 year overall survival rate after initial complete surgical resection of 86% compared to 0% after incomplete resection.
The bulk of studies identified in this systematic review were small case series and case reports [7, 8, 13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44, 46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63, 65,66,67, 70, 72,73,74,75,76,77,78,79,80]. As expected, the heterogeneity among these studies with low numbers of RASB patients was considerable. However, as shown in Table 2, most patients were treated with mastectomy, whereas adjuvant chemotherapy and radiotherapy were rarely used. Long-term survivors among these women were only found in cases of localized disease at initial presentation and complete tumor resection.
Discussion
In this case report and systematic review of the literature, we found that RASB is a rare late complication of breast irradiation and carries a poor prognosis. Surgery is the mainstay of treatment for localized disease while systemic chemotherapy and re-irradiation are appropriate for women with disseminated or recurrent RASB. Specifically, we identified and analyzed 307 cases of RASB for a pooled incidence rate of RASB of 1/3754 women after breast irradiation. Overall, the prognosis of women with RASB is poor and the reported mean recurrence-free survival is only 15.9 months. Mean overall survival is 27.4 months.
Chemotherapy, although only rarely used in the adjuvant setting, is used in the majority of cases after recurrence. In our pooled analysis, chemotherapy was given in 58% of women with recurrent RASB. The choice of drug regimen, clearly, was empirical due to the rarity of the disease and there is no standard chemotherapy regimen for RASB. Among the many regimens and substances, anthracyclines and taxanes were the most commonly used compounds. In addition, ifosfamide and gemcitabine have been used alone or in combination with anthracyclines and taxanes. This is in accordance with what has been reported in the treatment of patients with metastatic angiosarcoma. For example, in a large series of D’Angelo et al., including 119 cases of metastatic angiosarcomas [81], doxorubicin and taxanes were the most commonly used agents. The overall response rate to first line chemotherapy was 30% and below 10% in all subsequent chemotherapy lines. The median time to progression was 3.5 months for first line chemotherapy, 3.7 months for second line chemotherapy, and 2.7 months for third line chemotherapy. Of note, both anthracyclines and taxanes resulted in similar response rates and survival times. In addition, there was no apparent benefit for combination chemotherapy regimens compared to single agents. These results are in accordance with another analysis of chemotherapy efficiency among 117 cases with metastatic angiosarcomas published by Italiano et al. [82]. In this study, weekly paclitaxel (used in 64% of cases) and doxorubicin (used in 36% of cases) were again the most commonly used agents. Both had similar efficacy. In the doxorubicin group, 2 (6%) had complete response, 8 (23.5%) had partial response, 10 (29.5%) had stable disease, and 14 (41%) had progressive disease. In the paclitaxel group, 9 (13%) had complete response, 27 (40%) had partial response, 20 (29.5%) had stable disease, and 12 (17.5%) had progressive disease. Objective responses to weekly paclitaxel were more frequent in cutaneous angiosarcomas, whereas tumor location did not impact response to doxorubicin. Median progression-free survival was 4.9 months and median overall survival was 8.5 months. The dosage and therapy duration of regimens including taxanes and anthracyclines varied in the literature. For example, Italiano et al. used single-agent doxorubicin in a dosage of 60–75 mg/m2 on day 1 in a 3-week cycle or weekly paclitaxel at a dosage of 80 mg/m2/day in the first-line setting [82]. Others used polychemotherapy regimens with 6 cycles and the following dosages: cyclophosphamide 500 mg/m2, vincristine 1.4 mg/m2, doxorubicin 50 mg/m2 on day 1, and dacarbazine 400 mg/m2 on days 1 to 3 with cycles repeated every 28 days or doxorubicin 60 mg/m2 on day 1, ifosfamide 2.5 g/m2 on days 1 to 3, and dacarbazine 800 mg/m2, given on day 2, cycles repeated every 28 days or doxorubine 60 mg/m2 and cisplatin 100 mg/m2 on day 1 and ifosfamide 3 g/m2 on days 1 to 3, repeated every 28 days [18].
It is of note that angiogenesis inhibitors such as the vascular endothelial growth factor (VEGF) antibody bevacizumab have not been used in women with RASB, although this would be a logical treatment approach. On the other hand, bevacizumab has not proven efficacious in preliminary studies in women with metastatic sporadic angiosarcomas. For example, Ray-Coquard performed a randomized phase II trial and reported no additional benefit regarding progression-free survival and overall survival when adding bevacizumab (10 mg/kg once every 2 weeks) to weekly paclitaxel with 90 mg/m2 [83].
Another targeted substance with a rationale for the treatment of RASB is pazopanib, an antiangiogenic drug, which has been successfully used in angiosarcomas as well as other sarcoma entities, e.g. synovial sarcoma [84]. However, no data on the use of pazopanib in women with RASB are available.
The case report presented within this review had typical characteristics of RASB, for example the long time delay between the radiotherapy and the development of RASB. We chose complete local excision as the primary means of therapy based on our consultation of the literature. For example, in our literature review, 85% of RASB patients underwent mastectomy. In addition, we treated the patient with liposomal doxorubicine, because anthracyclines are active substances both in breast cancer and RASB. After the first recurrence of RASB, we performed mastectomy and suggested another line of chemotherapy, which was declined by the patient. Clearly, other therapy options such mTOR inhibitors or targeted therapies such as sorafenib and brivanib could have been used in this patient. However, she declined additional systemic therapies and thus opted for clinical follow-up.
Conclusions
In conclusion, we found that RASB is a rare late complication of breast irradiation. The prognosis of women with RASB is poor. Surgery is the mainstay of treatment for localized disease while systemic chemotherapy and re-irradiation are appropriate for women with disseminated or recurrent RASB.
Abbreviations
- ER:
-
Estrogen receptor
- HNPCC:
-
Hereditary non-polyposis colon cancer syndrome
- mTOR:
-
Mammalian target of rapamycin
- PECAM:
-
Platelet endothelial cell adhesion molecule
- PR:
-
Progesterone receptor
- RASB:
-
radiogenic angiosarcoma of the breast
- VEGF:
-
Vascular endothelial growth factor
References
Shah S, Rosa M. Radiation-associated angiosarcoma of the breast. Clinical and pathologic features. Arch Pathol Lab Med. 2016;140:477–81.
Holm M, Aggerholm-Pedersen N, Mele M, Jorgensen P, Baerentzen S, Safwat A. Primary breast sarcoma. A retrospective study over 35 years from a single institution. Acta Oncol. 2016;55:584–90.
Laé M, Lebel A, Hamel-Viard F, Asselain B, Trassard M, Sastre X, Kirova YM. Can c-myc amplification reliably discriminate postradiation from primary angiosarcoma of the breast? Cancer Radiother. 2015;19:168–74.
Fodor J, Orosz Z, Szabó E, Sulyok Z, Polgár C, Zaka Z, Major T. Angiosarcoma after conservation treatment for breast carcinoma. Our experience and a review of the literature. J Am Acad Dermatol. 2006;54:499–504.
Marchal C, Weber B, de Lafontan B, Resbeut M, Mignotte H, Du Chatelard PP, Cutuli B, Reme-Saumon M, Broussier-Leroux A, Chaplain G, Lesaunier F, Dilhuydy JM, Lagrange JL. Nine breast angiosarcomas after conservative treatment for breast carcinoma. A survey from French comprehensive Cancer Centers. Int J Radiat Oncol Biol Phys. 1999;44:113–9.
D’Angelo SP, Antonescu CR, Kuk D, Qin L, Moraco N, Carvajal RC, Chi P, Dickson MA, Gounder M, Keohan ML, Singer S, Schwartz GK, Tap WD. High-risk features in radiation-associated breast angiosarcomas. Br J Cancer. 2013;109:2340–6.
Esler-Brauer L, Jaggernauth W, Zeitouni NC. Angiosarcoma developing after conservative treatment for breast carcinoma. Case report with review of the current literature. Dermatol Surg. 2007;33:749–55.
Feigenberg SJ, Mendenhall NP, Reith JD, Ward JR, Copeland EM 3rd. Angiosarcoma after breast-conserving therapy. Experience with hyperfractionated radiotherapy. Int J Radiat Oncol Biol Phys. 2002;52:620–6.
Strobbe LJ, Peterse HL, van Tinteren H, Wijnmaalen A, Rutgers EJ. Angiosarcoma of the breast after conservation therapy for invasive cancer, the incidence and outcome. An unforseen sequela. Breast Cancer Res Treat. 1998;47:101–9.
Stacchiotti S, Van Tine BA. Synovial sarcoma: current concepts and future perspectives. J Clin Oncol. 2018;36(2):180–7.
Ji Y, Chen S, Xiang B, Li K, Xu Z, Yao W, Lu G, Liu X, Xia C, Wang Q, Li Y, Wang C, Yang K, Yang G, Tang X, Xu T, Wu H. Sirolimus for the treatment of progressive kaposiform hemangioendothelioma: a multicenter retrospective study. Int J Cancer. 2017;141(4):848–55.
Smith TL, Morris CG, Mendenhall NP. Angiosarcoma after breast-conserving therapy. Long-term disease control and late effects with hyperfractionated accelerated re-irradiation (HART). Acta Oncol. 2014;53:235–41.
Seo IS, Min K-W. Postirradiation epithelioid angiosarcoma of the breast. A case report with immunohistochemical and electron microscopic study. Ultrastruct Pathol. 2003;27:197–203.
Shaikh NA, Beaconsfield T, Walker M, Ghilchik MW. Postirradiation angiosarcoma of the breast--a case report. Eur J Surg Oncol. 1988;14:449–51.
Iqbal FM, Ahmed B, Vidya R. Double-edged sword of radiotherapy. A cause of secondary angiosarcoma after breast conservation therapy. BMJ Case Rep. 2016;2016. https://doi.org/10.1136/bcr-2016-215310.
Jayalakshmy PS, Sivaram AP, Augustine J, Bindu P. Postmastectomy-postirradiation atypical vascular lesion of the skin. Report of 2 cases. Case Rep Pathol. 2012;2012:710318.
Vertse G, Svastics E, Iványi A. Postirradiation angiosarcoma of the breast. Magy Seb. 2010;63:164–7.
Des Guetz G, Chapelier A, Mosseri V, Dorval T, Asselain B, Pouillart P. Postirradiation sarcoma. Clinicopathologic features and role of chemotherapy in the treatment strategy. Sarcoma. 2009;2009:764379.
West JG, Qureshi A, West JE, Chacon M, Sutherland ML, Haghighi B, Harrison J. Risk of angiosarcoma following breast conservation. A clinical alert. Breast J. 2005;11:115–23.
Rao J, Dekoven JG, Beatty JD, Jones G. Cutaneous angiosarcoma as a delayed complication of radiation therapy for carcinoma of the breast. J Am Acad Dermatol. 2003;49:532–8.
Polgár C, Orosz Z, Szerdahelyi A, Fodor J, Major T, Mágori A, Czeyda-Pommersheim F, Vámosi Nagy I, Szakolczai I, Fejös Z, Németh G. Postirradiation angiosarcoma of the chest wall and breast. Issues of radiogenic origin, diagnosis and treatment in two cases. Oncology. 2001;60:31–4.
Vesoulis Z, Cunliffe C. Fine-needle aspiration biopsy of postradiation epithelioid angiosarcoma of breast. Diagn Cytopathol. 2000;22:172–5.
Layfield LJ, Dodd LG. Cytologic findings in a case of postirradiation angiosarcoma of the breast. Acta Cytol. 1997;41:612–4.
Sole J, Guedea F, Matiasguiu X, Lerma E, Seral A. Long-term risk of sarcoma following radiation treatment for breast cancer. Oncol Rep. 1996;3:397–9.
Wijnmaalen A, van Ooijen B, van Geel BN, Henzen-Logmans SC, Treurniet-Donker AD. Angiosarcoma of the breast following lumpectomy, axillary lymph node dissection, and radiotherapy for primary breast cancer. Three case reports and a review of the literature. Int J Radiat Oncol Biol Phys. 1993;26:135–9.
Segal SL, Lenchner GS, Cichelli AV, Promisloff RA, Hofman WI, Baiocchi GA. Angiosarcoma presenting as diffuse alveolar hemorrhage. Chest. 1988;94:214–6.
Otis CN, Peschel R, McKhann C, Merino MJ, Duray PH. The rapid onset of cutaneous angiosarcoma after radiotherapy for breast carcinoma. Cancer. 1986;57:2130–4.
Lo TC, Silverman ML, Edelstein A. Postirradiation hemangiosarcoma of the chest wall. Report of a case. Acta Radiol Oncol. 1985;24:237–40.
Armengot-Carbó M, Roca-Estellés MJ, Quecedo-Estébanez E, Gimeno-Carpio E. Angiosarcoma of the skin after breast cancer radiotherapy. Actas Dermosifiliogr. 2012;103:557–9.
Fernández Ortega A, Gil Gil JM, Urruticoetxea A, Serra Payró JM. Angiosarcoma of the breast. Two cases following breast conserving treatment for invasive carcinoma. Clin Transl Oncol. 2006;8:536–9.
Di Tommaso L, Fabbri A. Cutaneous angiosarcoma arising after radiotherapy treatment of a breast carcinoma. Description of a case and review of the literature. Pathologica. 2003;95:196–202.
Friedrich M, Krauth M, Lange K. Angiosarcoma of the breast after breast-preserving therapy of invasive ductal carcinoma. Rofo. 1996;165:195–7.
Colville RJ, Ramsden A, Malcolm A, McLean NR. Angiosarcoma of the breast after quadrantectomy and postoperative radiotherapy for carcinoma. Br J Plast Surg. 2000;53:622–4.
Hogewind BF, Boutkan HB, de Jager-Nowak HK, Merkus JW. Angiosarcoma following breast-conserving therapy. Ned Tijdschr Geneeskd. 2004;148:995–7.
Williams EV, Banerjee D, Dallimore N, Monypenny IJ. Angiosarcoma of the breast following radiation therapy. Eur J Surg Oncol. 1999;25:221–2.
Mermershtain W, Cohen AD, Koretz M, Cohen Y. Cutaneous angiosarcoma of breast after lumpectomy, axillary lymph node dissection, and radiotherapy for primary breast carcinoma. Case report and review of the literature. Am J Clin Oncol. 2002;25:597–8.
Deutsch M, Safyan E. Angiosarcoma of the breast occurring soon after lumpectomy and breast irradiation for infiltrating ductal carcinoma. A case report. Am J Clin Oncol. 2003;26:471–2.
Pfeiffer DF, Bode-Lesniewska B. Fine needle aspiration biopsy diagnosis of angiosarcoma after breast-conserving therapy for carcinoma supported by use of a cell block and immunohistochemistry. Acta Cytol. 2006;50:553–6.
Griffa B, Basilico V, Clerici D, Bellotti R, Scognamiglio G, Zanardo M, Capriata G. Angiosarcoma of the breast after conservative surgery and radiotherapy for early breast carcinoma. Description of a case. Minerva Chir. 2000;55:799–802.
Kariniemi AL, Autio P. Angiosarcoma of the breast after radiotherapy. Duodecim. 1998;114:1963–5.
Hildebrandt G, Mittag M, Gütz U, Kunze ML, Haustein UF. Cutaneous breast angiosarcoma after conserving treatment of breast cancer. Eur J Dermatol. 2001;11:580–3.
Catena F, Santini D, Di Saverio S, Laneve A, Ansaloni L, Fogacci T, Gagliardi S, Gazzotti F, Guidi G, de Cataldis A, Taffurelli M. Skin angiosarcoma arising in an irradiated breast. Case-report and literature review. Dermatol Surg. 2006;32:447–55.
Moe M, Bertelli G. Breast angiosarcoma following lumpectomy and radiotherapy for breast cancer. A case with short latent period and false negative result on biopsies. Ann Oncol. 2007;18:801.
Lamblin G, Oteifa M, Zinzindohoue C, Isaac S, Termine L, Bobin JY. Angiosarcoma after conservative treatment and radiation therapy for adenocarcinoma of the breast. Eur J Surg Oncol. 2001;27:146–51.
Hodgson NC, Bowen-Wells C, Moffat F, Franceschi D, Avisar E. Angiosarcomas of the breast. A review of 70 cases. Am J Clin Oncol. 2007;30:570–3.
Weed BR, Folpe AL. Cutaneous CD30-positive epithelioid angiosarcoma following breast-conserving therapy and irradiation. A potential diagnostic pitfall. Am J Dermatopathol. 2008;30:370–2.
Bolin DJ, Lukas GM. Low-grade dermal angiosarcoma of the breast following radiotherapy. Am Surg. 1996;62:668–72.
Soldić Z, Salopek D, Jazvić M, Radić J, Marić-Brozić J, Tomas D, Kirac P, Bolanca A, Kusić Z. Parenchymal post-irradiation angiosarcoma. A case report. Acta Clin Croat. 2009;48:433–7.
Horevoets J, Devos B. Angiosarcoma of the breast. Case report and review of the literature. Acta Chir Belg. 2013;113:223–7.
Andrews S, Wilcoxon R, Benda J, Jacobson G. Angiosarcoma following MammoSite partial breast irradiation. Breast Cancer Res Treat. 2010;124:279–82.
Kajo K, Lúcan J, Macháleková K, Beratsová Z. Cutaneous angiosarcoma following conservative surgery and radiotherapy for breast carcinoma. A case report. Cesk Patol. 2007;43:59–63.
Nambisan M, Elwood E, Mammolito D. Locally recurrent angiosarcoma after excision in a patient treated with breast-conserving therapy. Am Surg. 2008;74:1227–8.
Zucali R, Merson M, Placucci M, Di Palma S, Veronesi U. Soft tissue sarcoma of the breast after conservative surgery and irradiation for early mammary cancer. Radiother Oncol. 1994;30:271–3.
Aydogdu M, Trams G. Angiosarcoma of the breast after conservatively operated breast carcinoma--a sequela of adjuvant radiotherapy? Geburtshilfe Frauenheilkd. 1996;56:60–2.
Del Mastro L, Garrone O, Guenzi M, Cafiero F, Nicolò G, Rosso R, Venturini M. Angiosarcoma of the residual breast after conservative surgery and radiotherapy for primary carcinoma. Ann Oncol. 1994;5:163–5.
Weber B, Marchal C. Three cases of breast angiosarcomas after breast-conserving treatment for carcinoma. Radiother Oncol. 1995;37:250–2.
Majeski J, Austin RM, Fitzgerald RH. Cutaneous angiosarcoma in an irradiated breast after breast conservation therapy for cancer. Association with chronic breast lymphedema. J Surg Oncol. 2000;74:208–12. discussion 212-3
Wiebringhaus P, Gröger A, Menke H. Secondary angiosarcoma of the breast after breast-conserving therapy. Handchir Mikrochir Plast Chir. 2015;47:134–8.
Bonetta A, Pagliari C, Morrica B. Post-radiation angiosarcoma of the breast. A clinical case. Tumori. 1995;81:219–21.
Nakamura R, Nagashima T, Sakakibara M, Nakano S, Tanabe N, Fujimoto H, Arai M, Kadowaki M, Oide T, Tanizawa T, Miyazaki M. Angiosarcoma arising in the breast following breast-conserving surgery with radiation for breast carcinoma. Breast Cancer. 2007;14:245–9.
Anania G, Parodi PC, Sanna A, Rampino E, Marcotti E, Di Loreto C, Zuiani C, Donini A. Radiation-induced angiosarcoma of the breast. Case report and self-criticism of therapeutic approach. Ann Chir. 2002;127:388–91.
Barbosa OV, Reiriz AB, Boff RA, Oliveira WP, Rossi L. Angiosarcoma in previously irradiated breast in patient with Li-Fraumeni syndrome. A case report. Sao Paulo Med J. 2015;133:151–3.
Nestle-Krämling C, Bölke E, Budach W, Peiper M, Niederacher D, Janni W, Eisenberger CF, Knoefel WT, Scherer A, Baldus SE, Lammering G, Gerber PA, Matuschek C. Hemangiosarcoma after breast-conserving therapy of breast cancer. Report of four cases with molecular genetic diagnosis and literature review. Strahlenther Onkol. 2011;187:656–64.
Billings SD, McKenney JK, Folpe AL, Hardacre MC, Weiss SW. Cutaneous angiosarcoma following breast-conserving surgery and radiation. An analysis of 27 cases. Am J Surg Pathol. 2004;28:781–8.
Sessions SC, Smink RD Jr. Cutaneous angiosarcoma of the breast after segmental mastectomy and radiation therapy. Arch Surg. 1992;127:1362–3.
Zafar A, Neary P, O’Donoghue G, Fiuza-Castinieria C. A breast surgeon’s paranoia pays off. The importance of keen clinical acumen in a case of postradiotherapy breast angiosarcoma. BMJ Case Rep. 2012;2012
Navarro Cecilia J, Jiménez Anula J, Luque López C, Martín Salvago MD, Dueñas Rodríguez B. Secondary breast angiosarcoma. Multifocal recurrence in a postmastectomy breast reconstruction flap. Cir Esp. 2015;93:260–2.
Uryvaev A, Moskovitz M, Abdach-Bortnyak R, Hershkovitz D, Fried G. Post-irradiation angiosarcoma of the breast. Clinical presentation and outcome in a series of six cases. Breast Cancer Res Treat. 2015;153:3–8.
Gennaro M, Valeri B, Casalini P, Carcangiu ML, Gronchi A, Conti AR, Agresti R, Greco M. Angiosarcoma of the breast and vascular endothelial growth factor receptor. Tumori. 2010;96:930–5.
Taat CW, van Toor BS, Slors JF, Bras J, Blank LE, van Coevorden F. Dermal angiosarcoma of the breast. A complication of primary radiotherapy? Eur J Surg Oncol. 1992;18:391–5.
Hui A, Henderson M, Speakman D, Skandarajah A. Angiosarcoma of the breast. A difficult surgical challenge. Breast. 2012;21:584–9.
Adhikari D, Hajdu SI, Levine D. Post-radiation angiosarcoma and bilateral mastectomy. Ann Clin Lab Sci. 2002;32:428–33.
Azizun-Nisa, Zeeshanuddin, Kayani N. Malignant vascular tumours associated with the breast. A study of 7 cases. J Pak Med Assoc. 2013;63:646–9.
Hanasono MM, Osborne MP, Dielubanza EJ, Peters SB, Gayle LB. Radiation-induced angiosarcoma after mastectomy and TRAM flap breast reconstruction. Ann Plast Surg. 2005;54:211–4.
Mocerino C, Iannaci G, Sapere P, Luise R, Canonico S, Gambardella A. Multidisciplinary approach to breast angiosarcoma in an elderly patient. Repeated local relapses and significant objective responses. Int J Immunopathol Pharmacol. 2016;29:537–42.
Scow JS, Reynolds CA, Degnim AC, Petersen IA, Jakub JW, Boughey JC. Primary and secondary angiosarcoma of the breast. The Mayo Clinic experience. J Surg Oncol. 2010;101:401–7.
Zemanova M, Rauova K, Boljesikova E, Machalekova K, Krajcovicova I, Lehotska V, Mikulova M, Svec J. Analysis of radiation-induced angiosarcoma of the breast. Bratisl Lek Listy. 2014;115:307–10.
Moskaluk CA, Merino MJ, Danforth DN, Medeiros LJ. Low-grade angiosarcoma of the skin of the breast. A complication of lumpectomy and radiation therapy for breast carcinoma. Hum Pathol. 1992;23:710–4.
Plichta JK, Hughes K. Radiation-induced angiosarcoma after breast-cancer treatment. N Engl J Med. 2017;376:367.
Boyan W Jr, Farr M, Georges R. High grade angiosarcoma fifteen years after breast conservation therapy with radiation therapy. A case report. Int J Surg Case Rep. 2014;5:1176–7.
D’Angelo SP, Munhoz RR, Kuk D, Landa J, Hartley EW, Bonafede M, Dickson MA, Gounder M, Keohan ML, Crago AM, Antonescu CR, Tap WD. Outcomes of systemic therapy for patients with metastatic angiosarcoma. Oncology. 2015;89:205–14.
Italiano A, Cioffi A, Penel N, Levra MG, Delcambre C, Kalbacher E, Chevreau C, Bertucci F, Isambert N, Blay J-Y, Bui B, Antonescu C, D’Adamo DR, Maki RG, Keohan ML. Comparison of doxorubicin and weekly paclitaxel efficacy in metastatic angiosarcomas. Cancer. 2012;118:3330–6.
Ray-Coquard IL, Domont J, Tresch-Bruneel E, Bompas E, Cassier PA, Mir O, Piperno-Neumann S, Italiano A, Chevreau C, Cupissol D, Bertucci F, Bay JO, Collard O, Saada-Bouzid E, Isambert N, Delcambre C, Clisant S, Le Cesne A, Blay JY, Penel N. Paclitaxel given once per week with or without bevacizumab in patients with advanced angiosarcoma: a randomized phase II trial. J Clin Oncol. 2015;33(25):2797–802.
Ishida Y, Otsuka A, Kabashima K. Cutaneous angiosarcoma: update on biology and latest treatment. Curr Opin Oncol. 2017; [Epub ahead of print]
Acknowledgments
We acknowledge support by the Open Access Publication Funds of the Ruhr-Universität Bochum.
Availability of data and materials
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
CT and AD designed the study, collected the material, analyzed the data, and wrote the manuscript. GR, PK, and GH participated in collecting and analyzing data. BS participated in analyzing the data and writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The patient provided written informed consent for this treatment. We did not obtain Ethics Committee approval, since no approval is required for a case report and literature review.
Consent for publication
Written informed consent for publication of the clinical details and images was obtained from the patient described in the case report. A copy of the consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Dogan, A., Kern, P., Schultheis, B. et al. Radiogenic angiosarcoma of the breast: case report and systematic review of the literature. BMC Cancer 18, 463 (2018). https://doi.org/10.1186/s12885-018-4369-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-018-4369-7