
Abstract
Background
Breast cancer is a heterogeneous and a hormone-dependent disease. The detection of the estrogen receptor (ER) and progesterone receptor (PgR) is crucial for prognostic evaluation and treatment choice of breast cancer for clinical practice. The purpose of this study was to evaluate the expression of the hormonal receptors, their distribution, and their correlation with clinicopathologic prognostic parameters for the improvement of the patients’ treatment in Ivory Coast.
Methods
The 20-month prospective study included 302 patients who were diagnosed with primary invasive breast carcinomas at the Central Laboratory in Abidjan. The paraffin-embedded blocks of these patients were examined by immunohistochemistry to assess the ER and PgR status. The one-way analysis of variance and Chi-Square Test were used to analyze the data.
Results
The mean age of patients at diagnosis was 48 ± 11 years. The majority of the women were premenopausal in 180 cases (59.9%). The predominant histologic type was invasive ductal carcinoma not otherwise specified (IDC NOS) in 247 cases (82%). Tumor grade 2 was more frequent in 166 cases (55%). Among 302 patients, 169 (56%) and 154 (49%) expressed ER and PgR respectively. The ER+PgR+ group with 131 cases (43%) was predominant, followed by 116 cases (38%) of ER-PgR-. The expression of ER and PgR was correlated with the age of the patients (p = 0.026) and the tumor grade (p = 0.0004). However, there was not statistically significant correlation between ER/PgR and the menopausal status of patients (p = 0.149), nor between ER/PgR and the histologic type (p = 0.523).
Conclusion
The ER+PgR+ and ER-PgR- are the most common subgroups in women with breast cancer in Ivory Coast. The hormonal receptor status is associated with the age and the histologic grade in breast cancer patients. The systematic use of hormonal treatment should be reevaluated. A further study should be done to investigate the reasons of high rate of ER-PgR- in breast cancer patients in Ivory Coast.
Similar content being viewed by others


Background
Breast cancer is the most frequent malignant tumor and the most common cause of cancer-related death among women in the developed countries [1, 2]. Breast cancer is increasing in the developing countries, including Ivory Coast, where it ranks at the first cancer in women after cervical cancer [3]. Breast cancer is a hormone-dependent disease, and thus, resulting from the mitogenic effects of estrogen and progesterone [4, 5]. The positivity of the ER is generally more than 70% in women with breast cancer than that of PgR, 50% [6, 7]. The ER/PgR status is essential for clinical and therapeutic care of the breast cancer patients [8, 9]. The ER has well-established prognostic and predictive values [9, 10], while the PgR has a controversial additional predictive value [11, 12]. The presence or not of ER and PgR helps determine a possible relapse of breast cancer [9]. The hormonal receptor status allows to distinguish four subgroups of breast cancers: ER+PgR+, ER+PgR-, ER-PgR+, and ER-PgR- [8, 13, 14]. This classification helps to decide hormonal treatment for ER/PgR positive patients and chemotherapy for the ER/PgR negative patients [9, 15]. Although the immunohistochemical evaluation of ER and PgR is a routine clinical practice in the diagnosis and treatment of breast cancer management worldwide, the clinical utility of ER and PgR testing in breast cancer is currently performed since June 2013 in Ivory Coast. Moreover, very few studies have been done on small sample size (22 patients) to assess the hormonal receptor status of breast cancer in Ivory Coast [16]. The current research is essential to update the immunohistochemical activity of ER/PgR in primary breast cancers. Herein, the aim of this study was to evaluate the expression of ER and PgR, their distribution, and their correlation with classic clinicopathologic prognostic parameters (age, menopausal status, histologic type, and grade) to enhance the breast cancer patients’ medical care. The present study will contribute to classify patients into different subgroups based on their hormonal receptor status in order to determine the better treatment strategies for women with breast cancer in Ivory Coast.
Methods
Patients
The prospective study was conducted between November 2013 and June 2015, including 302 patients diagnosed with primary invasive breast carcinomas at the Central Laboratory in Abidjan, Ivory Coast. The histologic diagnosis was performed upon paraffin-embedded breast tissue blocks sampled from 261 (86.4%) needle core biopsies and 41 (13.6%) mastectomies. On each sample, the histologic type and the Nottingham grade of the tumor were determined according to the criteria of Elston and Ellis [17]. The parameters of the study were classic clinicopathologic parameters (age, menopausal status, histological type, and tumor grade) and the status of ER and PgR. Paraffin-embedded blocks of breast tissue were subjected to the immunohistochemical assessment.
ER/PgR immunohistochemical analysis
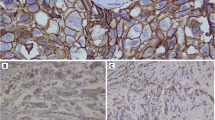
The immunohistochemical analysis was performed on 3 μm thickness of breast tissue sections. Tissue sections were deparaffinized and heated in the drying oven BINDER ® (BINDER Company, Tuttlingen, Germany) for at least 12 h at 600 C to unmask the antigenic sites. The sections were stained using the Ventana BenchMark ® GX in automatic mode (Ventana Medical Systems Inc., Tucson, AZ, USA) for the assessment of ER and PgR status. The antibody clones were monoclonal, developed in rats, consisted of SP1 for the ER and 1E2 for the PgR, and manufactured by Ventana Medical Systems, Inc.
Staining assessment of ER/PgR
The visual analysis through the optic microscope allowed to evaluate the staining intensity (weak, moderate, intense) and the percentage of tumor cells showing a nuclear immunostaining for ER and PgR (range: 0-100%). Breast tissue sections were considered positive for the ER and PgR if ≥ 1% of tumor cells displayed a positive nuclear staining in accordance with the recommendations of the American Society of Clinical Oncology/College of American Pathologists [18]. The immunostaining intensity and the percentages of stained cells for ER and PgR were reviewed independently by two pathologists. For the purpose of this study, the percentages of tumor cell nuclei positively stained for ER and PgR were considered.
Statistical analysis
Data were collected in an Excel database from Windows 8 (Microsoft Corporation, Redmond, WA, USA). The difference between the subgroups based on the status of ER/PgR and the mean age were evaluated by the one-way analysis of variance. The Chi-Square Test was used to analyze associations between classic clinicopathologic parameters (menopausal status, histological type, and tumor grade) and combined ER/PgR status. A p-value < 0.05 was considered statistically significant. The data were reported as frequencies for menopausal status, histological type, tumor grade, and ER/PgR status and as means for patients’age.
Results
Classic clinicopathologic parameters
The mean age of patients at diagnosis was 48 ± 11 years (extremes: 24–84 years). The clinicopathologic characteristics in breast cancer patients are shown in the Table 1. Among 302 patients, 180 cases (59.9%) were premenopausal patients compared to 112 cases (37.1%) of postmenopausal patients. The frequent histological type was IDC NOS with 247 cases (82%). Of these cancers, 41 (13.6%) were grade 1; 166 (55%) were grade 2; and 63 (20.9%) were grade 3.
Hormonal expression of ER and PgR
The Table 2 summarizes the combined ER/PgR status. ER and PgR positivity was 169 cases (56%) and 148 cases (50%) respectively. Almost half (131 cases; 43%) of the women in this study expressed both ER and PgR, followed by 116 cases (38%) in ER-PgR- patients.
Association of ER/PgR status with classic clinicopathologic parameters
A significant relationship was found between the ER/PgR status and the age of patients (p = 0.026); and between the ER/PgR status and the tumor grade of breast cancer (p = 0.0004), while the correlations of the ER/PgR status with the menopausal status (p = 0.149) and with the histologic type (p = 0,523) were not statistically significant (Table 3).
Discussion
For decades, samples of patients diagnosed with invasive breast carcinomas were sent to laboratories equipped with immunohistochemical techniques in the developed countries for ER and PgR examination. The Roche-Hoffman Laboratory in Ivory Coast, in collaboration with the Ivorian Health Ministry, has recently offered a Unit of Immunohistochemistry to the Central Laboratory to investigate the ER/PgR status of breast cancer patients for an efficient medical support. This study aimed at determining the hormonal receptor status to better characterize breast cancer subtypes and to assess the association of the hormonal receptor with age, menopausal status, histologic type, and tumor grade.
In the present study, several significant observations have been identified. The mean age of all patients at the diagnostic was 48 years, indicating that breast cancer appears early, before the menopause. This finding is similar to several studies conducted in Africa [16, 19–22] and in the Middle East [23]. However, the mean age of our patients is different from that of the developed countries [2, 6, 24], where breast cancer commonly occurs at the advanced age or at the postmenopausal period. The early occurrence of breast cancer in women in Ivory Coast could be due to the relative short life expectancy (54 years), the multiparity, and the early age at first childbirth. Parkin et al. found that the multiparity increased the risk of breast cancer before 45 years in a study in Zimbabwe [25]. Moreover, the multiparity [26, 27] and the early age at first childbirth [28] were the main risk factors for breast cancer in black American women. These observations may explain the high incidence of the breast cancer in premenopausal patients in our study.
In this study, IDC NOS associated with tumor grade 2 was predominant. These results are in agreement with data of other studies [7, 29], suggesting that clinical prognostic factors of breast cancer are worse in the African women, including Ivorian women. In contrast, the histologic type and the tumor grade have insufficient prognostic and predictive implications with limited clinical utility [30]. Therefore, it is valuable to detect ER and PgR status immunohistochemically in the current study to evaluate the survival of patients and to select their treatment.
The proportion of patients expressing ER is superior to those of PgR+. The same finding was reported by different authors in Europe, [29, 31, 32], in the USA [7, 8], and in Africa [21, 33]. In addition, ER+PgR+ and ER-PgR- were the most frequent subtypes in the current study. Our remarks corroborate with results of several studies [8, 13, 27, 33], suggesting that ER+PgR+ patients should be considered for hormonal therapy, and ER-PgR- patients should benefit from chemotherapy. Previously, a large number of breast cancer women underwent a systematic hormonal treatment in a blind manner in Ivory Coast. However, 38% of the study patients may not suitable for hormonal therapy, tamoxifen, since they do not express ER and PgR. As a result, they will not benefit from hormonal therapy, and the chemotherapy remains the only systematic treatment [9, 34, 35]. In this study, ER+PgR+ patients would more favorably respond to hormonal therapy than ER+PgR- and ER-PgR+ patients [9, 14, 36]. Additionally, ER+PgR+ patients, receiving hormonal therapy, have the advantage of avoiding a tumor relapse leading to a good long-term survival [9].
The high rate of ER-PgR- in our study is a remarkable finding and is approximately comparable with results reported by Seshie et al. in Ghana [37], Galukande et al. in Uganda [38], Adeniji et al. in Nigeria [39], and Palmer et al. in black American women [27]. Palmer et al. identified that the ER-PgR- subtype is greatly aggressive and resistant to hormonal therapy whose incidence is increased in the black American population. This high rate is related to the multiparity [27] and the early age at first childbirth [28]. Further studies should be done to determine the inherent reasons of the large frequency of ER-PgR- patients in Ivory Coast. Additionally, the increased proportion of ER-PgR- subtype could be explained by a deficiency of the preanalytical factors, particularly the fixation quality, investigated by Werner et al. [40] and Goldstein et al. [41]. Hence, a multidisciplinary collaboration between oncologists, radiologists, and pathologists is required to have sampled breast tissues fixed within the allotted time (6–18 h) to preserve hormonal receptor epitopes [40, 41].
In this current study, the ER-PgR+ subtype, accounting for 6%, is identical to that reported by Osborne et al. [8] and Hefti et al. [13]; however, differ from that of Nadji et al. [7] and Inwald et al. [32], who listed 0% and 0.8% respectively. Hefti et al. [13] have recently found that ER-PgR+ group does not represent a subtype of biologically distinct or clinically important cancer, and therefore, should be regarded as a false negative. This artifact subtype results from an inappropriate fixation leading to the loss of epitopes of paraffin-embedded breast tissue blocks [7, 40, 41].
Despite the unquestionable contribution of ER and PgR testing for a better therapeutic implication, it appears necessary to examine the correlation between ER/PgR status with standard clinicopathologic parameters of primary invasive carcinomas in 302 patients. There was a significant association between the age of the patients and the ER/PgR subgroups. The ER/PgR status has no significant influence on the menopausal status. Our results are consistent with findings of Elwood and Godolphin. Both authors revealed in an analysis of multiple regression study of age and menopausal status in 735 patients that the mean age was significantly associated with the ER/PgR, while there was no significant link between the ER/PgR and the menopausal status [6]. In the past, tamoxifen was given based on the menopausal status of patients in Ivory Coast because postmenopausal patients appeared to be ER+PgR+ and would better respond to tamoxifen than premenopausal patients. As a result, our data pinpoint that hormonal therapy should be given regardless of the menopausal status.
A correlation was found between the ER/PgR and the tumor grade, which corroborates with the literature data [6, 7]. In contrast, there was not significant association between ER/PgR status and the histologic type. This result differs from finding of numerous studies [6, 7, 34]. Nadji et al. observed that ER status predicted some histologic types in breast cancer, and thereby, a lack of such correlation in our study should suspect a technical problem [7]. In our study, this technical problem may be resulted from the morphologic diagnostic errors or the handling issue of preanalytical factors of breast samples, such as the duration and the type of fixation.
Conclusions
The ER+PgR+ and ER-PgR- are the most common subtypes and occur in premenopausal women. The hormonal receptor status is associated with the age and the tumor grade in breast cancer patients. Taken together, the results of this study help to eliminate a systematic use of hormonal therapy based on the menopausal status of the breast cancer patients. The increased proportion of ER-PgR- patients needs to be carefully considered in a future study. The ER/PgR status is no longer sufficient to treat breast cancer patients in Ivory Coast since the human epidermal growth factor receptor 2 (Her2) overexpression analysis and the Ki67 index are required to define the molecular classification of breast cancers for better treatment strategies.
Abbreviations
- ER:
-
Estrogen receptor
- Her2:
-
Human epidermal growth factor receptor 2
- IDS NOS:
-
Invasive ductal carcinoma not otherwise specified
- PgR:
-
Progesterone receptor
References
American Cancer Society. Cancer Facts & Figures 2013. Atlanta: American Cancer Society; 2013.
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, Forman D, Bray F. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–403.
Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11 [Internet]. Lyon: International Agency for Research on Cancer; 2013. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed 15 July 2015.
Anderson WF, Chatterjee N, Ershler WB, Brawley OW. Estrogen receptor breast cancer phenotypes in the Surveillance, Epidemiology, and End Results database. Breast Cancer Res Treat. 2002;76(1):27–36.
Knight 3rd WA, Osborne CK, McGuire WL. Hormone receptors in primary and advanced breast cancer. Clin Endocrinol Metab. 1980;9(2):361–8.
Elwood JM, Godolphin W. Estrogen receptors in breast tumors: Association with age, menopausal status, and epidemiological and clinical features in 735 patients. Br J Cancer. 1980;42(5):635–44.
Nadji M, Gomez-Fernandez C, Ganjei-Azar P, Morales AR. Immunohistochemistry of estrogen and progesterone receptors reconsidered: experience with 5,993 breast cancers. Am J Clin Pathol. 2005;123(1):21–7.
Osborne CK, Yochmowitz MG, Knight 3rd WA, McGuire WL. The value of estrogen and progesterone receptors in the treatment of breast cancer. Cancer. 1980;46 Suppl 12:2884–8.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Davies C, Godwin J, Gray R, Clarke M, Cutter D, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771–84.
Rastelli F, Crispino S. Factors predictive of response to hormone therapy in breast cancer. Tumori. 2008;94(3):370–83.
Olivotto IA, Truong PT, Speers CH, Bernstein V, Allan SJ, Kelly SJ, Lesperance ML. Time to stop progesterone receptor testing in breast cancer management. J Clin Oncol. 2004;22(9):1769–70.
Fuqua SA, Cui Y, Lee AV, Osborne CK, Horwitz KB. Insights into the role of progesterone receptors in breast cancer. J Clin Oncol. 2005;23(4):931–2.
Hefti MM, Hu R, Knoblauch NW, Collins LC, Haibe-Kains B, Tamimi RM, Beck AH. Estrogen receptor negative/progesterone receptor positive breast cancer is not a reproducible subtype. Breast Cancer Res. 2013;15(4):R68.
McGuire WL, Horwitz KB, Pearson OH, Segaloff A. Current status of estrogen and progesterone receptors in breast cancer. Cancer. 1977;39 Suppl 6:2934–47.
Barlett JM, Brookes CL, van de Velde CJ, Billingham LJ, Campbell FM, Grant M, et al. Estrogen receptor and progesterone receptor as predictive biomarkers of response to endocrine therapy: a prospectively powered pathology study in the tamoxifen and exemestane adjuvant multinational trial. J Clin Oncol. 2011;29:1531–8.
Didi-Kouko Coulibaly J, Effi AB, Horo GA, Diabate A, Mbra K, Adoubi I, et al. Hormonal status and overexpression of HER2 in breast cancer, Cancerology department of Treichville UHC. Preliminary results. Bull Cancer. 2008;95(9):799–803.
Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Histopathology. 1991;19(5):403–10.
Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010;28:2784–95.
Huo D, Adebamowo CA, Ogundiran TO, Akang EE, Campbell O, Adenipekun A, et al. Parity and breastfeeding are protective against breast cancer in Nigerian women. Br J Cancer. 2008;98:992–6.
Effi AB, N’Dah KJ, N’Guiessan AA, Doukouré B, Kouyaté M, Abouna AD, et al. Epidemiology and histopathology of cancers in Ivory Coast. Afr J Cancer. 2012;4(1):41–7.
Ermiah E, Buhmeida A, Abdalla F, Khaled BR, Salem N. PyrhönenS, Collan Y. Prognostic value of proliferation markers: immunohistochemical Ki-67 expression and cytometric S-Phase Fraction of women with breast cancer in Libya. J Cancer. 2012;3:421–31.
Fouad A, Yousra A, Kaoutar Z, Omar EM, Afaf A, Sanae B. Molecular Classification of breast cancer in Morocco. Pan Afr Med J. 2012;13:91.
Abulkhair O, Saghir N, Sedky L, Saadedin A, Elzahwary H, Siddiqui N, et al. Modification and implementation of NCCN guidelines on breast cancer in the Middle East and North Africa region. J Natl Compr Canc Netw. 2010;8 Suppl 3:S8–S15.
Goss PE, Ingle JN, Martino S, Robert NJ, Muss HB, Piccart MJ, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med. 2003;349(19):1793–802.
Parkin DM, Vizcain AP, Skinner MEG, Ndhlovu A. Cancer patterns and risk factors in the African population of Southwestern Zimbabwe 1963-1977. Cancer Epidemiol Biomarkers Prev. 1994;3:537–47.
Palmer JR, Wise LA, Horton NJ, et al. Dual effect of parity on breast cancer risk in African- American women. J Natl Cancer Inst. 2003;95:478–83.
Palmer JR, Boggs DA, Wise LA, Ambrosone CB, Adams-Campbell LL, Rosenberg L. Parity and lactation in relation to estrogen receptor negative breast cancer in African American women. Cancer Epidemiol Biomarkers Prev. 2011;20(9):1883–91.
Li CI, Beaber EF, Tang M-TC, Porter PL, Daling JR, Malone KE. Reproductive factors and risk of estrogen receptor positive, triple-negative, and HER2-neu overexpressing breast cancer among women 20–44 years of age. Breast Cancer Res Treat. 2013;137(2):579–87.
Loehberg CR, Almstedt K, Jud SM, Haeberle L, Fasching PA, Hack CC, et al. Prognostic relevance of Ki-67 in the primary tumor for survival after a diagnosis of distant metastasis. Breast Cancer Res Treat. 2013;138(3):899–908.
Visscher DW, Zarbo RJ, Greenawald KA, Crissman JD. Prognostic significance of morphological parameters and flow cytometric DNA analysis in carcinoma of the breast. Pathol Annu. 1990;25:171–210.
Joensuu K, Leidenius M, Kero M, Andersson LC, Horwitz KB, Heikkilä P. ER, PR, HER2, Ki-67 and CK5 in early and late relapsing breast cancer-reduced CK5 expression in metastases. Breast Cancer (Auckl). 2013;7:23–34.
Inwald EC, Klinkhammer-Schalke M, Hofstädter F, Zeman F, Koller M, Gerstenhauer M, Ortmann O. Ki-67 is a prognostic parameter in breast cancer patients: results of a large population-based cohort of a cancer registry. Breast Cancer Res Treat. 2013;139(2):539–52.
Ohene-Yeboah M, Adjei E. Breast cancer in Kumasi, Ghana. G M J. 2012;46(1):8–13.
Barnes DM, Harris WH, Smith P, Millis RR, Rubens RD. Immunohistochemical determination of oestrogen receptor: comparison of different methods of assessment of staining and correlation with clinical outcome of breast cancer patients. Br J Cancer. 1996;74:1445–51.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2008;365:1687–717.
Cui X, Schiff R, Arpino G, Osborne CK, Lee AV. Biology of progesterone receptor loss in breast cancer and its implications for endocrine therapy. J Clin Oncol. 2005;23(30):7721–35.
Seshie B, Adu-Aryee NA, Dedey F, Calys-Tagoe B, Clegg-Lamptey JN. A retrospective analysis of breast cancer subtype based on ER/PR and HER2 status in Ghanaian patients at the Korle Bu Teaching Hospital, Ghana. BMC Clin Pathol. 2015;15:14. doi:10.1186/s12907-015-0014-4.
Galukande M, Wabinga H, Mirembe F, Karamagi F, Asea A. Molecular breast cancer subtypes prevalence in an indigenous Sub Saharan African population. Pan Afr Med J. 2014;17:249. doi:10.11604/pamj.2014.17.249.330.
Adeniji KA, Huo D, Khramtsov A, Zhang C, Olopade OI. Molecular profiles of breast cancer in Ilorin, Nigeria. J Clin Oncol. 2010;28:15s. 2010 (suppl; abstr 1602).
Werner M, Chott A, Fabiano A, Battifora H. Effect of formalin tissue fixation and processing on immunohistochemistry. Am J Surg Pathol. 2000;24(7):1016–9.
Goldstein NS, Ferkowicz M, Odish E, Mani A, Hastah F. Minimum formalin fixation time for consistent estrogen receptor immunohistochemical staining of invasive breast carcinoma. Am J Clin Pathol. 2003;120(1):86–92.
Acknowledgements
The authors thank the Roche-Hoffman Laboratory and the Ministry of Health for implementing the first Unit of Immunohistochemistry at the Central Laboratory in Abidjan, Ivory Coast. The authors also thank Mr. Koffi Arthur and Ms. Gnenaho Pamela for performing the immunohistochemical technique.
Funding
This work was funded by the Roche-Hoffman and Novartis Laboratories - Ivory Coast. These funders have no role in the study design, in the collection, analysis, and interpretation of data and in the preparation of the manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Authors’ contributions
All authors substantially contributed to the present study. EAB conceived of the study, performed the immunohistochemical analysis, and reviewed the manuscript. NAA participated in the design of the study, performed the statistical analyses, carried out the immunohistochemical analysis, drafted and revised the manuscript. KDK, ZCT, BSK, and MK participated in sampling and histopathological analysis. All authors have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was approved by the Ivory Coast Advisory National Bioethics Committee. All patients in the present study gave written informed consent.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Effi, A.B., Aman, N.A., Koui, B.S. et al. Immunohistochemical determination of estrogen and progesterone receptors in breast cancer: relationship with clinicopathologic factors in 302 patients in Ivory Coast. BMC Cancer 17, 115 (2017). https://doi.org/10.1186/s12885-017-3105-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-017-3105-z