
Abstract
Background
Cervical cancer is one of the most important cancers worldwide with a high incident and mortality rate and is caused by the human papilloma virus (HPV). Among sexually active women who get infected with human papillomavirus (HPV), a small fraction progresses to cervical cancer disease pointing to possible roles of additional risk factors in development of the disease which include host genetic factors and other infections such as HSV-2. Since cellular apoptosis plays a role in controlling the spread of virus-infections in cells, gene variants altering the function of proteins involved in cell death pathways might be associated with the clearing of virus infections. Activity altering polymorphisms in FasR (−1377G > A and -670A > G), FasL (−844 T > C) and CASP8 (−652 6 N ins/del) genes have been shown to alter the mechanism of apoptosis by modifying the level of expression of their correspondent proteins.
In the present study, we set out to investigate the combined risks of CASP8, FasR, and FasL polymorphisms in cervical cancer, pre-cancerous lesions, HPV infection and HSV-2 infection.
Methods
Participants were 442 South African women of black African and mixed-ancestry origin with invasive cervical cancer and 278 control women matched by age, ethnicity and domicile status. FasR and FasL polymorphisms were genotyped by TaqMan and CASP8 polymorphism by PCR-RFLP. The results were analysed with R using haplo.stats software version 1.5.2.
Results
CASP8 -652 6 N del + FasR-670A was associated with a reduced risk (P = 0.019, Combined Polymorphism Score (CPS) = −2.34) and CASP8 -652 6 N ins + FasR-1377G was associated with a marginal increased risk (P = 0.047, CPS = 1.99) of cervical cancer among black Africans. When compared within the control group, CASP8 -652 6 N ins + FasR-1377A showed a reduced risk (P = 0.023, CPS = −2.28) of HSV-2 infection in both black African and mixed-ancestry population.
Conclusions
Our results show that the combined risks of variants in cell death pathway genes are associated with the cervical cancer as well as the HSV-2 infection in the black African and mixed-ancestry population.
Similar content being viewed by others

Background
Cervical cancer is the second most common cancer and the highest cause of cancer related deaths across the globe. Approximately 500, 000 new cases of cervical cancer and nearly 300, 000 deaths (52 %) caused by cervical cancer are reported each year making it the third most common cancer in women of all ages worldwide. Cervical cancer is the second most common cancer in southern Africa with approximately 6,500 new incidents and the second highest cause of cancer mortality with around 3000 cervical cancer related deaths (53 %) annually in women of all ages [1]. Persistent infection with oncogenic types of human papillomavirus (HPV) is the main cause of cervical cancer. Many sexually active women become infected with HPV during their life time but 70–90 % of the individuals positive for HPV DNA are able to clear the infection. Only a small percentage of the women with HPV progress to develop cervical cancer over their time [2]. This suggests a possible role of additional risk factors such as, host and viral genetic factors as well as environmental and lifestyle factors in the development of the cancer of the cervix [3].
Herpes simplex virus type 2 (HSV-2) is a common sexually transmitted virus that causes genital infections. HSV-2 has a high prevalence rate throughout the world, more so in the developing nations. Sub-Saharan Africa particularly harbours a high incidence rate with more women being affected than men [4]. HSV-2 in conjunction with HPV has been implicated as a co-factor for cervical cancer [5]. Once inside a human cell, HSV-2 evades the immune system by overcoming the apoptosis of the cell which is triggered by Fas-FasL-Caspase pathway. Fas mediated cytolysis plays an important role in clearing the HSV-2 from genital epithelium [6].
Apoptosis or programmed cell death is one of the most crucial mechanisms of the human immune system to control viral infection in human body [7]. The interaction between cell surface death receptor Fas (FasR), together with Fas ligand (FasL) activates a caspase-cascade leading to activation-induced cell death (AICD) that eventually leads to apoptosis to eliminate the virus-infected cells [8, 9]. Among various caspases, caspase-8 is central to activating the caspase-cascade [10] and plays one of the most important roles in generating apoptotic signals [9]. Therefore functional polymorphisms in the cell death pathway genes encoding FasR, FasL and caspase-8 might interfere with the apoptotic process associated with the spread and clearance of virus-infections inside human body.
The FasR and FasL genes are mapped on chromosome 10q23 and 1q23 respectively. Three functional single nucleotide polymorphisms (SNPs) in these two genes (FasR-1377G > A, FasR-670A > G and FasL-844 T > C) have been well studied. FasR-1377G > A and FasR-670A > G polymorphisms disrupt the SP1 and STAT1 binding sites respectively leading to reduced Fas gene expression and decreased apoptosis [11, 12]. FasL-844 T > C is observed to show higher basal expression that inhibits the apoptotic activity of the FasR-FasL pathway [13]. These three SNPs have been associated with different diseases [11, 13–24] including cervical cancer in different populations [14, 25–30]. The other important factor in the apoptotic pathway, caspase-8 is encoded by CASP8 gene which is mapped on chromosome 2q33. A six nucleotide deletion of AGTAAG at the position 652 in the promoter region of CASP8 gene (CASP8 -652 6 N ins/del) have been well studied. This six nucleotide deletion destroys the SP1-binding site which reduces the caspase-8 expression and thereby decreasing the apoptotic activity of the caspase-cascade [31]. This polymorphism has been associated with different types of diseases [31–41] including cervical cancer in different populations [31, 41].
No studies to date have attempted to find out the combined risks of all the four polymorphisms from FasR (−1377G > A, −670A > G), FasL (−844 T > C) and CASP8 (−652 6 N ins/del) genes on cervical cancer, HPV infection or HSV-2 infection in any population. We therefore re-analysed our data evaluating the combined risks of CASP8 polymorphism in the presence of both FasR and FasL polymorphisms, on cancer of the cervix susceptibility, HPV infection and HSV-2 infection in South African women of black African and mixed-ancestry origin.
Methods
Study participants
Participants in this study were recruited as part of a bigger case–control study to investigate the association of oral contraceptives with cervical cancer [41–43] and included 442 women with invasive cervical cancer (104 black African and 338 women of mixed-ancestry) and 278 control women (52 black African and 226 women of mixed-ancestry) without cancer of the cervix recruited from two previous studies from our lab that investigated the role of FasR (FasR-1377, FasR-670) and FasL (FasL-844) [30] and CASP8 polymorphisms (−652 6 N ins/del) [41] on cervical cancer.
Herpes simplex virus type 2 (HSV-2) detection, high-risk HPV type detection and papanicolau test
The detection of HSV-2 infection (by HerpeSelect 2 IgG enzyme-linked immunosorbent serologic assay), high-risk HPV infection (by Hybrid Capture II HPV test) and abnormal cytology (by Papanicolaou or Pap smear test) have been described previously [24, 43].
Clinical specimens, extraction of genomic DNA and genotyping
The collection and storage of clinical specimens, extraction and quantification of genomic DNA and determination of FasR (FasR-1377: rs2234767, assay id, C_12123966_10; FasR-670: rs1800682, assay id, C_9578811_10), FasL (FasL-844: rs763110, custom-designed) and CASP8 (rs3834129:–/AGTAAG;NM_001228.4) polymorphisms have been described previously [24, 41]. All experiments were performed in compliance with relevant laws and institutional guidelines (University of Cape Town Human Research Ethics Committee study approval number, REC REF: 075/2009) and in accordance with the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from each participant of this study.
Statistical analysis
The genotype distributions for all the polymorphisms were tested for Hardy-Weinberg equilibrium and linkage disequilibrium for cases and controls. Logistic regression was used to test for correlations and associations of different combinations of combined genotypes (CASP8 with FasR/FasL) with cervix cancer status as well as baseline characteristics and secondary outcomes such as age, ethnicity, smoking status, HSV-2 and HIV infection status in cases and controls. HPV and high-risk HPV infection and abnormal cytology status test was done only in the control group (the information for these categories were only available for the controls). Statistical analyses were done with R (the freely available environment for graphics and statistics), using haplo.stats software version 1.5.2 http://CRAN.R-project.org/package=haplo.stats. Broadly, haplo.stats uses the expectation maximisation (EM) algorithm, to calculate maximum likelihood estimates of probabilities of haplotype pairs (one paternal, one maternal) for each subject [44].
Results
No significant difference in age was observed between cases and controls (P = 0.271) (Table 1). 31 % (n = 135) cases and 40 % (n = 111) controls were tobacco smokers. Smoking was found to be associated with the cases and controls significantly (P = 0.01). The HSV-2 status was known for 429 cases and 263 controls. Among cases 68 % (n = 291) were positive for HSV-2 infection while among controls 164 (47 black African and 117 women of mixed-ancestry) were positive for HSV-2 infection (62 %). There was no significant difference in the HSV-2 infection between cases and controls. HIV infection status was known for 433 cases and 263 controls. Only 5 % of cases and 4 % of controls were HIV infected which was not found to be significant (Table 1). HPV infection, abnormal cytology and high-risk HPV infection status was known only among controls. HPV infection occurred at a frequency pf 28 % among the 170 controls who had results, while abnormal cytology and high-risk HPV infection was positive in 13 % and 14 %, respectively, among the 269 controls with available data Analysis of only the controls showed a significant association (P = 0.013) between abnormal cytology and ethnicity (Table 1).
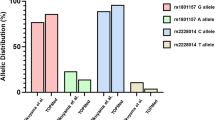
The observed genotype frequencies for all the polymorphisms were found to be in Hardy-Weinberg equilibrium (HWE) except for CASP8 -652 6 N ins/del which was slightly out of HWE (P = 0.045) in mixed-ancestry controls [30, 41]. FasR polymorphisms (−1377 and −670) were in strong linkage disequilibrium (LD) (P < 0.05) except in black African controls (P = 0.078) [30]. We have previously reported that the allele and genotype frequency distributions for FasR/FasL differ significantly between the ethnic groups (black African and mixed-ancestry) investigated [30]. Among all the baseline characteristics and secondary outcomes only smoking was found to be a significant confounding factor for cancer of the cervix as mentioned above. Therefore, all analyses were subsequently adjusted for both ethnicity and smoking by including in logistic regression models as covariates.
CASP8 polymorphism (CASP8 -652 6 N ins/del) was combined with any (and all) of the FasR (−1377, −670) and FasL (−844) polymorphisms which gave rise to 7 combinations of polymorphisms (total 52 different combinations) as shown in Additional file 1. None of the combinations showed any significant association (P < 0.05) with cancer of the cervix (both population combined) (Table 2). When stratified for different populations, the mixed-ancestry population again did not show any significant association (P < 0.05) with the disease (Table 2). However, the black Africans showed a marginal increased risk with CASP8 -652 6 N ins + FasR-1377G (P = 0.047, Combined Polymorphism Score (CPS) = 1.99) and cervical cancer and a reduced risk with CASP8 -652 6 N del + FasR-670A (P = 0.019, CPS = −2.34) with the same disease (CPS is similar as a haplotype score; a positive value suggests a positive association and a negative value suggests a negative association with the disease under investigation) (Table 2). The combined risks of CASP8 -652 6 N del + FasR-670A polymorphism showed a reduced risk of cervical cancer even when combined with FasR-1377 and FasL-844 polymorphisms (Table 2).
Comparing the different polymorphisms in smoking positive and HSV-2 positive cases and controls did not show any significant association (results not shown here) either.
The combined risks of the polymorphisms were also investigated only within the control group, as the controls represent the larger healthy South-African female population, unlike the cervical cancer group that is affected by a disease. When HSV-2 infection status was compared in the control group for the different combinations of the polymorphisms, a reduced risk was found with CASP8 -652 6 N ins + FasR-1377A (P = 0.023, CPS = −2.28) and HSV-2 infection (Table 3). The combined risks of these two polymorphisms showed a reduced risk of HSV-2 infection even when combined with FasR-670 and FasL-844 polymorphisms (Table 3). Comparing the other parameters such as, smoking, high-risk HPV infection and abnormal cytology status in the control group did not yield any significant association with any of the parameters mentioned (results not shown here).
Discussion
The cell death pathway is one of the most essential pathways in human immune system. This pathway is central to and regulates cellular apoptosis which is one of the mechanisms by which the immune system controls infections caused by pathogenic viruses [7]. Disruptions in cell death pathway can lead to impaired apoptotic mechanism which may affect the ability of the immune system to control the spread of virus-infections in cells. Three functional polymorphisms in FasR (FasR-1377, FasR-670) and FasL genes (FasL-844) and one in CASP8 gene (CASP8 -652 6 N ins/del), all in cell death pathway are known to disrupt the apoptotic mechanism by altering the level of expression of Fas and caspase-8 proteins, respectively [11–13, 31]. All the four polymorphisms have been investigated in different types of cancers such as breast [32, 33, 37], bladder [19, 40], lung [20, 23], squamous cell carcinoma [15, 22], colorectal [35], pancreatic [36], different leukaemia [11, 16], cervical [14, 25–31, 41] and several other pathological conditions [11, 13–23, 31–41], all presenting with conflicting results. Previously we have investigated these four polymorphisms in cervical cancer in South African women of black African and mixed-ancestry origin [24, 30, 41]. Comparing women with invasive cervical cancer with age, ethnicity and domicile (urban/rural) matched controls did not show any significant association for FasR and FasL polymorphisms with cervical cancer [30]. However, a secondary analysis only in the control group found a statistically significant association with FasR-1377A (P = 0.008) and FasR-1377/FasR-670 AG haplotype (P = 0.0001) with reduced risk of HSV-2 infection [24]. When CASP8 -652 6 N ins/del polymorphism was compared between cervical cancer cases and controls no significant association with cervical cancer was observed [41]. However, further analysis within only controls showed an association (positive) of CASP8 -652 6 N del/del (P = 0.03) polymorphism with high-risk HPV infection (only among black Africans) and a weak association (positive) with abnormal cytology (P = 0.048) suggesting a susceptible role for this genotype in the development of pre-cancers but not in cervical cancer [41]. The combined risks of all the four polymorphisms of FasR, FasL and CASP8 on cervical cancer, HPV infection, pre-cancerous lesions and HSV-2 infection have not been investigated in any population yet.
Since all the four polymorphisms play vital roles in the cell death pathway leading to altered mechanism of cellular apoptosis it is valuable to investigate the combined risks of CASP8 polymorphism with any (and all) of the FasR/FasL polymorphisms in cervical cancer, pre-cancerous lesions, HPV infection and HSV-2 infection. None of the combinations of the polymorphisms had any significant association with cancer of the cervix in both populations combined and also when stratified for mixed-ancestry population, which is in accordance with our previous individual results with FasR/FasL [30] and CASP8 polymorphisms [41]. However, when stratified among only black Africans a new reduced risk for cervical cancer was observed with CASP8 -652 6 N del combined with FasR-670 A allele (P = 0.019, CPS = −2.34). In the same population, a marginal susceptible risk to cervical cancer was also observed when CASP8 -652 6 N ins was combined with FasR-1377 G allele (P = 0.047, CPS = 1.99). This could be due to different factors. The black Africans are a homogenous population with well defined genetic conformation unlike the mixed-ancestry population that carries a highly mixed genetic makeup. It is also well known that disease susceptibility varies from population to population due to varying level of genetic markers present in various population.
When the combined risks of the polymorphisms were investigated only in the controls, a reduced risk for HSV-2 infection was observed with CASP8 -652 6 N ins + FasR-1377A. This is in consistence with our previous results [24] that showed a reduced risk for HSV-2 infection with FasR-1377A allele alone in the control group as mentioned above. CASP8 promoter polymorphism individually have also been associated with reduced risk of cutaneous melanoma, lung, esophageal, gastric, breast, colorectal and cervical cancer [31, 34] in different population even though in our own population we found an increased risk of this polymorphism with cervical cancer [41].
None of the combinations of the polymorphisms had any significant association with any other parameters in the control group suggesting the combined risks of the polymorphisms are not associated with smoking, high-risk HPV infection and abnormal cytology status in the larger South-African female population.
Conclusions
The present study showed a reduced risk to cervical cancer combining CASP8 -652 6 N del with FasR-670 A allele (P = 0.019, CPS = −2.34) and a marginal susceptible risk to cervical cancer with CASP8 -652 6 N ins + FasR-1377G (P = 0.047, CPS = 1.99), only in black Africans. This study also showed a reduced risk to HSV-2 infection with CASP8 -652 6 N ins + FasR-1377A in the control group. The results must be interpreted cautiously. This was a sub-group analysis of our original study and the results could be influenced due to several possible population or biological confounding factors that are hitherto unrecognized. Future studies on larger cohorts are warranted to further confirm these findings and to elucidate the mechanisms involved.
References
Who/ICO Information Centre on HPV and Cervical Cancer (HPV Information Centre). Human Papillomavirus and Related Cancers in World. Summary Report 2010 [Date Accessed] Available at www.whointhpvcentre.
Tindle RW. Immune evasion in human papillomavirus-associated cervical cancer. Nat Rev Cancer. 2002;2(1):59–65.
Martin CM, Kehoe L, Spillane CO, O'Leary JJ. Gene discovery in cervical cancer : towards diagnostic and therapeutic biomarkers. Mol Diagn Ther. 2007;11(5):277–90.
Weiss H. Epidemiology of herpes simplex virus type 2 infection in the developing world. Herpes. 2004;11 Suppl 1:24A–35A.
Smith JS, Herrero R, Bosetti C, Munoz N, Bosch FX, Eluf-Neto J, et al. Herpes simplex virus-2 as a human papillomavirus cofactor in the etiology of invasive cervical cancer. J Natl Cancer Inst. 2002;94(21):1604–13.
Dobbs ME, Strasser JE, Chu CF, Chalk C, Milligan GN. Clearance of herpes simplex virus type 2 by CD8+ T cells requires gamma interferon and either perforin- or Fas-mediated cytolytic mechanisms. J Virol. 2005;79(23):14546–54.
Dockrell DH. Apoptotic cell death in the pathogenesis of infectious diseases. J Infect. 2001;42(4):227–34.
Suda T, Takahashi T, Golstein P, Nagata S. Molecular cloning and expression of the Fas ligand, a novel member of the tumor necrosis factor family. Cell. 1993;75(6):1169–78.
Siegel RM. Caspases at the crossroads of immune-cell life and death. Nat Rev Immunol. 2006;6(4):308–17.
Ju ST, Panka DJ, Cui H, Ettinger R, el-Khatib M, Sherr DH, et al. Fas(CD95)/FasL interactions required for programmed cell death after T-cell activation. Nature. 1995;373(6513):444–8.
Sibley K, Rollinson S, Allan JM, Smith AG, Law GR, Roddam PL, et al. Functional FAS promoter polymorphisms are associated with increased risk of acute myeloid leukemia. Cancer Res. 2003;63(15):4327–30.
Kanemitsu S, Ihara K, Saifddin A, Otsuka T, Takeuchi T, Nagayama J, et al. A functional polymorphism in fas (CD95/APO-1) gene promoter associated with systemic lupus erythematosus. J Rheumatol. 2002;29(6):1183–8.
Wu J, Metz C, Xu X, Abe R, Gibson AW, Edberg JC, et al. A novel polymorphic CAAT/enhancer-binding protein beta element in the FasL gene promoter alters Fas ligand expression: a candidate background gene in African American systemic lupus erythematosus patients. J Immunol. 2003;170(1):132–8.
Lai HC, Sytwu HK, Sun CA, Yu MH, Yu CP, Liu HS, et al. Single nucleotide polymorphism at Fas promoter is associated with cervical carcinogenesis. Int J Cancer. 2003;103(2):221–5.
Zhang Z, Wang LE, Sturgis EM, El-Naggar AK, Hong WK, Amos CI, et al. Polymorphisms of FAS and FAS ligand genes involved in the death pathway and risk and progression of squamous cell carcinoma of the head and neck. Clin Cancer Res. 2006;12(18):5596–602.
Farre L, Bittencourt AL, Silva-Santos G, Almeida A, Silva AC, Decanine D, et al. Fas 670 promoter polymorphism is associated to susceptibility, clinical presentation, and survival in adult T cell leukemia. J Leukoc Biol. 2008;83(1):220–2.
Davidson WF, Giese T, Fredrickson TN. Spontaneous development of plasmacytoid tumors in mice with defective Fas-Fas ligand interactions. J Exp Med. 1998;187(11):1825–38.
Peters AM, Kohfink B, Martin H, Griesinger F, Wormann B, Gahr M, et al. Defective apoptosis due to a point mutation in the death domain of CD95 associated with autoimmune lymphoproliferative syndrome, T-cell lymphoma, and Hodgkin's disease. Exp Hematol. 1999;27(5):868–74.
Lee SH, Shin MS, Park WS, Kim SY, Kim HS, Han JY, et al. Alterations of Fas (Apo-1/CD95) gene in non-small cell lung cancer. Oncogene. 1999;18(25):3754–60.
Lee SH, Shin MS, Park WS, Kim SY, Dong SM, Pi JH, et al. Alterations of Fas (APO-1/CD95) gene in transitional cell carcinomas of urinary bladder. Cancer Res. 1999;59(13):3068–72.
Takahashi T, Tanaka M, Brannan CI, Jenkins NA, Copeland NG, Suda T, et al. Generalized lymphoproliferative disease in mice, caused by a point mutation in the Fas ligand. Cell. 1994;76(6):969–76.
Sun T, Miao X, Zhang X, Tan W, Xiong P, Lin D. Polymorphisms of death pathway genes FAS and FASL in esophageal squamous-cell carcinoma. J Natl Cancer Inst. 2004;96(13):1030–6.
Zhang X, Miao X, Sun T, Tan W, Qu S, Xiong P, et al. Functional polymorphisms in cell death pathway genes FAS and FASL contribute to risk of lung cancer. J Med Genet. 2005;42(6):479–84.
Chatterjee K, Dandara C, Gyllensten U, van der Merwe L, Galal U, Hoffman M, et al. A Fas gene polymorphism influences herpes simplex virus type 2 infection in South African women. J Med Virol. 2010;82(12):2082–6.
Lai HC, Lin WY, Lin YW, Chang CC, Yu MH, Chen CC, et al. Genetic polymorphisms of FAS and FASL (CD95/CD95L) genes in cervical carcinogenesis: An analysis of haplotype and gene-gene interaction. Gynecol Oncol. 2005;99(1):113–8.
Dybikowska A, Sliwinski W, Emerich J, Podhajska AJ. Evaluation of Fas gene promoter polymorphism in cervical cancer patients. Int J Mol Med. 2004;14(3):475–8.
Engelmark MT, Renkema KY, Gyllensten UB. No evidence of the involvement of the Fas −670 promoter polymorphism in cervical cancer in situ. Int J Cancer. 2004;112(6):1084–5.
Sun T, Zhou Y, Li H, Han X, Shi Y, Wang L, et al. FASL -844C polymorphism is associated with increased activation-induced T cell death and risk of cervical cancer. J Exp Med. 2005;202(7):967–74.
Ivansson EL, Gustavsson IM, Magnusson JJ, Steiner LL, Magnusson PK, Erlich HA, et al. Variants of chemokine receptor 2 and interleukin 4 receptor, but not interleukin 10 or Fas ligand, increase risk of cervical cancer. Int J Cancer. 2007;121(11):2451–7.
Chatterjee K, Engelmark M, Gyllensten U, Dandara C, van der Merwe L, Galal U, et al. Fas and FasL gene polymorphisms are not associated with cervical cancer but differ among Black and Mixed-ancestry South Africans. BMC Res Notes. 2009;2:238.
Sun T, Gao Y, Tan W, Ma S, Shi Y, Yao J, et al. A six-nucleotide insertion-deletion polymorphism in the CASP8 promoter is associated with susceptibility to multiple cancers. Nat Genet. 2007;39(5):605–13.
Cybulski C, Wokolorczyk D, Gliniewicz B, Sikorski A, Gorski B, Jakubowska A, et al. A six-nucleotide deletion in the CASP8 promoter is not associated with a susceptibility to breast and prostate cancers in the Polish population. Breast Cancer Res Treat. 2008;112(2):367–8.
Frank B, Rigas SH, Bermejo JL, Wiestler M, Wagner K, Hemminki K, et al. The CASP8 -652 6N del promoter polymorphism and breast cancer risk: a multicenter study. Breast Cancer Res Treat. 2008;111(1):139–44.
Li C, Zhao H, Hu Z, Liu Z, Wang LE, Gershenwald JE, et al. Genetic variants and haplotypes of the caspase-8 and caspase-10 genes contribute to susceptibility to cutaneous melanoma. Hum Mutat. 2008;29(12):1443–51.
Pittman AM, Broderick P, Sullivan K, Fielding S, Webb E, Penegar S, et al. CASP8 variants D302H and −652 6N ins/del do not influence the risk of colorectal cancer in the United Kingdom population. Br J Cancer. 2008;98(8):1434–6.
Yang M, Sun T, Wang L, Yu D, Zhang X, Miao X, et al. Functional variants in cell death pathway genes and risk of pancreatic cancer. Clin Cancer Res. 2008;14(10):3230–6.
De Vecchi G, Verderio P, Pizzamiglio S, Manoukian S, Barile M, Fortuzzi S, et al. Evidences for association of the CASP8 -652 6N del promoter polymorphism with age at diagnosis in familial breast cancer cases. Breast Cancer Res Treat. 2009;113(3):607–8.
Ji G, Gu A, Hu F, Wang S, Liang J, Xia Y, et al. Polymorphisms in cell death pathway genes are associated with altered sperm apoptosis and poor semen quality. Hum Reprod. 2009;24(10):2439–46.
Ni C, Ye Y, Wang M, Qian H, Song Z, Jia X, et al. A six-nucleotide insertion-deletion polymorphism in the CASP8 promoter is associated with risk of coal workers' pneumoconiosis. J Toxicol Environ Health A. 2009;72(11–12):712–6.
Wang M, Zhang Z, Tian Y, Shao J. A six-nucleotide insertion-deletion polymorphism in the CASP8 promoter associated with risk and progression of bladder cancer. Clin Cancer Res. 2009;15(7):2567–72.
Chatterjee K, Williamson AL, Hoffman M, Dandara C. CASP8 promoter polymorphism is associated with high-risk HPV types and abnormal cytology but not with cervical cancer. J Med Virol. 2011;83(4):630–6.
Hoffman M, Cooper D, Carrara H, Rosenberg L, Kelly J, Stander I, et al. Limited Pap screening associated with reduced risk of cervical cancer in South Africa. Int J Epidemiol. 2003;32(4):573–7.
Shapiro S, Rosenberg L, Hoffman M, Kelly JP, Cooper DD, Carrara H, et al. Risk of invasive cancer of the cervix in relation to the use of injectable progestogen contraceptives and combined estrogen/progestogen oral contraceptives (South Africa). Cancer Causes Control. 2003;14(5):485–95.
Schaid DJ, Rowland CM, Tines DE, Jacobson RM, Poland GA. Score tests for association between traits and haplotypes when linkage phase is ambiguous. Am J Hum Genet. 2002;70(2):425–34.
Acknowledgements
We would like to thank Prof. Ulf Gyllensten (Uppsala University, Sweden) for supervising the FasR/FasL work. We are grateful to all the patients and controls who participated in this study. This work is based upon research supported by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation. It was also supported by the NRF South Africa/Sweden Science and Technology Agreement’s Fund.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KC participated in planning of the study, performed extraction of DNA, genotyping, analyzing the results and advanced statistical analysis. A-LW was responsible for the storage of the biological samples, helped in planning and helped in interpretation of the results. AH performed advanced statistical analysis and helped with reporting and interpretation of results. CD helped in statistical analysis and supervising the study and interpreting of the results. All authors critically read and took part in finalizing the interpretation of the results.
Additional file
Additional file 1:
The Genotype combinations observed when analysing CASP8 (- 652 6 N ins/del), FasR-1377 (G > A), FasR-670 (A > G) and FasL-844 (T > C) genetic variants. (DOC 42 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chattopadhyay, K., Williamson, AL., Hazra, A. et al. The combined risks of reduced or increased function variants in cell death pathway genes differentially influence cervical cancer risk and herpes simplex virus type 2 infection among black Africans and the Mixed Ancestry population of South Africa. BMC Cancer 15, 680 (2015). https://doi.org/10.1186/s12885-015-1678-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-015-1678-y