
Abstract
Background
In order to effectively and efficiently reduce maternal mortality and ensure optimal outcomes of pregnancy, equity is required in availability and provision of antenatal care. Thus, analysis of trends of socio-economic, demographic, cultural and geographical inequities is imperative to provide a holistic explanation for differences in availability, quality and utilization of antenatal care. We, therefore, investigated the trends in inequalities in four or more antenatal care visits in Ghana, from 1998 to 2014.
Methods
We used the World Health Organization’s (WHO) Health Equity Assessment Toolkit (HEAT) software to analyse data from the 1998 to 2014 Ghana Demographic and Health Surveys. We disaggregated four or more antenatal care visits by four equality stratifiers: economic status, level of education, place of residence, and sub-national region. We measured inequality through summary measures: Difference, Population Attributable Risk (PAR), Ratio, and Population Attributable Fraction (PAF). A 95% uncertainty interval (UI) was constructed for point estimates to measure statistical significance.
Results
The Difference measure of 21.7% (95% UI; 15.2–28.2) and the PAF measure of 12.4% (95% UI 9.6–15.2) indicated significant absolute and relative economic-related disparities in four or more antenatal care visits favouring women in the highest wealth quintile. In the 2014 survey, the Difference measure of 13.1% (95% UI 8.2–19.1) and PAF of 6.5% (95% UI 4.2–8.7) indicate wide disparities in four or more antenatal care visits across education subgroups disfavouring non-educated women. The Difference measure of 9.3% (95% UI 5.8–12.9) and PAF of 5.8% (95% UI 4.7–6.8) suggest considerable relative and absolute urban–rural disparities in four or more antenatal care visits disfavouring rural women. The Difference measure of 20.6% (95% UI 8.8–32.2) and PAF of 7.1% (95% UI 2.9–11.4) in the 2014 survey show significant absolute and relative regional inequality in four or more antenatal care visits, with significantly higher coverage among regions like Ashanti, compared to the Northern region.
Conclusions
We found a disproportionately lower uptake of four or more antenatal care visits among women who were poor, uneducated and living in rural areas and the Northern region. There is a need for policymakers to design interventions that will enable disadvantaged subpopulations to benefit from four or more antenatal care visits to meet the Sustainable Development Goal 3.1 that aims to reduce the maternal mortality ratio (MMR) to less than 70/100, 000 live births by 2030. Further studies are essential to understand the underlying factors for the inequalities in antenatal care visits.
Similar content being viewed by others

Background
Since the introduction of the Millennium Development Goals (MDGs) in 2000, the world saw a significant decline in maternal mortality ratio (MMR) from a 1.2% annual decrease between 1990 and 2000 to a 3.0% decrease between 2005 and 2015 [1, 2]. Despite these significant improvements in global MMR, low-and middle-income countries (LMICs), also within sub-Saharan Africa (sSA), continue to have high MMRs. Alkema et al. [3] postulated that sSA alone accounted for 66% of the global burden of maternal deaths in 2015. In Ghana, maternal mortality is a public health issue with an estimated MMR of 310 per 100,000 live births in 2017 [4].
One of the interventions that have been identified to be effective in reducing maternal mortality, morbidity and disability is antenatal care [ANC] [5]. Hence, WHO recommends a minimum of four ANC visits (from 2016 onwards increased to 8 visits). One purpose of ANC attendance is for early detection of potential complications, which allows health care providers to initiate interventions to mitigate the associated risks to reduce the risk of maternal mortality and severe morbidity [6]. This implies that failure to attend ANC at least 4 times may result in complications or even worsen already existing complications and potentially lead to the death of the mother or child or both.
It must be noted, however, that ANC attendance does not occur in isolation; it is dependent on a myriad of predisposing factors such as geographical, socioeconomic, religious, cultural, and demographic factors [7, 8]. These factors are in themselves inequalities that restrict pregnant women’s capacity to go through the required minimum of four ANC visits. In the case of Ghana, factors such as parity, religion, wealth, age, residence, cost of ANC as well as the quality and timing of ANC have been recognised to be influential on pregnant women’s ability to access four or more ANC visits [9, 10].
In order to effectively and efficiently avert or reduce the risk of adverse maternal health outcomes ( i.e., morbidity, disability and mortality), equality in the availability and provision of ANC is required. Evidence from the 2016 Lancet Global Burden of Disease study suggests that “achievement of the Sustainable Development Goal (SDG 3.1) will require 91% coverage of one ANC visit, 78% of four ANC visits, 81% of in-facility delivery, and 87% of skilled birth attendance.” [11]. These percentages may be instrumental to reduce MMRs to 70 per 100,000 live births by 2030. Thus, trend analysis of socio-economic, demographic, cultural and geographical inequities is imperative for a holistic explanation of differences in the availability, quality, and utilisation of ANC. On this premise, we sought to investigate the trends in inequalities in 4 + ANC visits among pregnant women in Ghana, from 1998 to 2014. Our findings may contribute to the knowledge on trends and inequalities in ANC attendance. Again, it would provide a framework to guide policy makers and programme developers to know what aspects of ANC ought to be altered to increase ANC visits and contribute to the reduction of maternal mortality considering the SDG 3 which seeks to reduce the global MMR to less than 70 per 100,000 live births and a neonatal mortality rate below 20 per 1.000 livebirths by 2030 [12].
Materials and methods
Study setting
The study setting is the Republic of Ghana, one of the countries in West Africa with a total land area of 238,533 square kilometres [13]. It is bounded by Burkina Faso in the north, Togo in the east and Côte d'Ivoire in the west. According to the different National Population Census (PHC), the population stood at 6,726,815 (1960); 8,559,313 (1970); 12,296,081 (1984); 18,912,079 (2000) and 24,658,823 (2010) [13]. At the time of the surveys, the country was divided into ten regions, which have currently increased to 16.
Data source
Secondary data obtained from the 1998, 2003, 2008, 2014 Ghana Demographic and Health Survey (GDHS) were used in this study. DHSs are conducted under the MEASURE DHS program in LMICs, mostly every five years since its start. The surveys focus on gathering information on women’s, children’s, men’s and households’ health. For women, some issues are about utilization of maternal health care, such as ANC visits. The survey used a two-stage sampling design, which begins with the selection of clusters across urban and rural locations from the entire nation. These clusters represent enumeration areas demarcated during the Ghana PHC. Next stage is the selection of households from predefined clusters. Details of the methodologies employed in the various rounds can be found in the final reports of GDHS [14]. In this study, only women with live births were considered. The sample sizes for each round of survey were as follows (n = 4141 in 2014, 2098 in 2008, 2643 in 2003 and 2310 in 1998). DHS data are available through the World Health Organization’s (WHO) Health Equity Assessment Toolkit (HEAT) and have two different ANC-visit measures (previous 2/3 years and previous 5 years). We only used the 5-years variable.
Selection and measures of variables
The outcome variable in this study was the utilization of ANC visits. Women were asked about the number of ANC visits they made during their recent pregnancy. This variable was dichotomized as 0–3 or 4 + ANC visits. Inequality in ANC visits was examined using four equity stratifiers: economic status (wealth index), level of education, place of residence and subnational region. In DHS, wealth index is computed using Principal Component Analysis (PCA) [15]. It is classified as poorest, poorer, middle, richer and richest quintiles. Level of education of the mother was categorized as no education, primary and secondary/higher education. Place of residence was classified as urban vs. rural and subnational regions were grouped into the then ten regions.
Statistical analyses
Using the 2019 updated WHO’s HEAT version 3.1 software [16], inequality in 4 + ANC visits was carried out in two steps. First, ANC visits were disaggregated by the four equity stratifiers: economic status, level of education, place of residence, and subnational region. This was done to present results on the distribution of the estimates and uncertainty intervals of 4 + ANC visits across the various equity stratifiers. Secondly, inequality was calculated using four measures of inequality: Difference, Population Attributable risk (PAR), Population Attributable Fraction (PAF) and Ratio. Difference and Ratio are simple measures whiles PAR and PAF are complex measures. While Ratio and PAF are relative measures, the remaining two are absolute summary measures. The choice of summary measures was based on evidence suggesting the scientific significance of adopting both absolute and relative summary measures in a single health inequality study [17, 18]. Whereas complex measures account for size of categories of sub-populations, simple measures do not. Notwithstanding, simple measures are easy for interpretation and understanding [17, 18]. Therefore, combining both relative and absolute measures helps to provide a more comprehensive analysis. Detailed procedure and calculation of the summary measures are available in the HEAT software technical notes [16, 17].
Results
Trends in prevalence of 4 + ANC visits across economic status, level of education, place of residence and Ghanaian sub-national regions
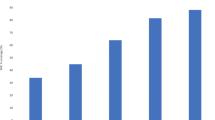
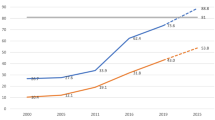
The prevalence of 4 + ANC visits changed over the years: it was 63.7% in 1998, it increased to 69.3% in 2003, 78.1% in 2008 and 87.2% in 2014. The extent of 4 + ANC visits varied across economic status, with higher concentrations among those in the richest wealth quintile (87.6% in 1998, 91.0% in 2003, 93.8% in 2008 and 98.1% in 2014). In terms of level of education, the prevalence of 4 + ANC visits was higher among women with secondary/higher education in 1998 [77.0%, 95% UI = 73.98–79.80], 2003 [80.7%, 95% UI = 77.69–83.4], 2008 [88.2%, 95% UI = 85.37–90.53] and 2014 [92.9%, 95% UI = 91.41–94.14]. The same trend of higher 4 + ANC visits was observed among women living in urban areas, compared to those in rural areas from 1998–2014. Except in 2014, where the concentration of 4 + ANC visits was higher among women who lived in the Ashanti region [93.5%, 95% UI = 89.54–96.01], the prevalence of 4 + ANC visits showed an increasing trend among women in the Greater Accra region (Table 1). However, the regions with relatively low prevalence of 4 + ANC visits in 2014 were the Volta region [77.3%, 95% UI = 69.2, 83.7], Eastern region [77.4%, 95% UI = 71.8, 82.1] and Northern region [72.3%, 95% UI = 60.3, 82.7]. Overall, we found that the prevalence of 4 + ANC visits in Ghana increased by 23.5% from 63.7% in 1998 to 87.3% in 2014.
Trends of 4 + ANC visits indicating the magnitude of inequality
Table 2 shows the socio-economic, urban–rural, educational and subpopulations disparities in 4 + ANC visits from 1998 and 2014, favouring women who are socio-economically advantaged, those with higher educational attainment, urban residents and those living in regions like the Greater Accra. More precisely, we found substantial absolute (D, PAR) and relative (R, PAF) wealth-driven disparities in 4 + ANC visits over the 16 years with higher coverage among advantaged subpopulations such as richest and richer women as compared to poorest and poorer. For instance, in the 2014 survey, the Difference measure of 21.7% [95% UI; 15.12–28.15] and the PAF of 12.4% [95% UI; 9.62–15.16] indicate significant absolute and relative economic-related disparities in 4 + ANC visits favouring economically advantaged women. Significant absolute and relative education-related disparities in 4 + ANC visits were discovered from 1998 to 2014 using all four summary measures, disfavouring non-educated subpopulations. For example, in the 2014 survey, the Ratio and PAR measures of 1.2% [95% UI; 1.09–1.25] and 5.6% [95% UI; 3.66–7.63] both indicate wide disparities in 4 + ANC visits across education subgroups disfavouring non-educated women.
Furthermore, this study shows extensive anti-rural inequalities in 4 + ANC visits using both absolute (Difference, PAR) and relative (Ratio, PAF) measures over the 16 year period. For example, the PAF measure of 5.8% [95% UI; 4.68–6.83] and PAR measure of 5.0% [95% UI; 4.09- 5.96] suggest considerable relative and absolute urban–rural disparities in 4 + ANC visits disfavouring rural women. The results further show sizeable subnational inequality in 4 + ANC visits over the 16 years using absolute (Difference, PAR) and relative (Ratio, PAF) measures. The Difference measure of 20.6% [95% UI; 8.82–32.23] and PAF of measure 7.1% [95% UI; 2.94–11.35] in the 2014 survey, show significant absolute and relative regional inequality in 4 + ANC visits, with significantly higher coverage among regions like Ashanti.
Discussion
This study shows an increasing trend in the prevalence of 4 + ANC visits from 63.7% in 1998 to 87.2% in 2014 in Ghana. This increasing trend could reflect state policies and interventions such as the free maternal healthcare policy and national health insurance scheme which are pro-maternal healthcare [19]. Another plausible explanation for this observation could be a resultant effect of the increased presence of Community-Based Health Planning and Services (CHPS) across the country since 1999. Also, we found the prevalence of 4 + ANC visits to be relatively higher among women who were economically advantaged, those with at least secondary education, urban residents, and those living in the Greater Accra and Ashanti regions.
In 2014, the prevalence of 87.3% is higher than the target of 78% recommended in the 2016 Lancet Global Burden of Diseases Study for the attainment of SDG 3, but certain socio-economic disparities could undo the gains made over the 16-years. The 2014 prevalence was higher than the 51% reported in Nigeria, 58.2% in Benin Republic, 78.1% in Liberia, 76% in Sierra Leone, 70.4% in Lesotho, and 64.8% in Zimbabwe [20, 21]. A key contributing factor to the 23.5% increase in the prevalence over the 16-year period could be the introduction of the free maternal health policy by the government of Ghana in 2008 to bridge financial access and inequality gaps [19].
In support of previous findings in Ghana, Malawi, Gabon, Nigeria, sSA and Pakistan, we found that women in the richest wealth quintile had higher prevalence of at least 4 ANC visits during the 16-year period [6, 22,23,24,25,26,27]. Despite the free ANC services in Ghana, there are other associated costs, such as transport to health facilities and medications, that are not covered by the national health insurance and could serve as potential barriers for women with low economic status [6]. However, the finding was incongruent with findings from a community-based survey in North Eastern Ethiopia where no economic inequalities were found with regard to 4 + ANC visits [28]. These divergences could be a result of socio-demographic differences in the two study populations.
Women with at least secondary education were consistently more advantageous in accessing 4 + ANC compared to those with less than secondary education. This aligns with the findings of previous studies in Ghana that revealed that education significantly influences ANC visits [5, 29,30,31]. Since education is known to increase health literacy and utilization, it may explain the reason for this observation [32, 33]. Additionally, educated women are more financially independent and may have better income to access ANC [34].
Women residing in urban areas had a higher prevalence of at least four ANC visits compared to those in rural areas. Previous studies have also reported significant positive associations between place of residence and ANC visits [35,36,37,38,39,40]. Even though Ghana has a free ANC program, there are reports of inequalities in the distribution of both skilled health workers and health facilities with respect to rural–urban areas [30]. Women in urban areas are more advantageous with respect to the availability of advanced health facilities and skilled health attendants. Conversely, women in rural areas have inadequate, unequipped, and often distant health facilities with few skilled health attendants leading to ANC drop-outs and high patronage of traditional birth attendants [30]. The Greater Accra and Ashanti Regions are predominantly urban with the two most densely populated cities in Ghana whereas the Northern Region is predominantly rural and one of the poorest regions in Ghana [12]. Therefore, the findings of our study imply the need for improvement in 4 + ANC visits not only in the Northern region but also in the Eastern and Volta regions where ANC visits were lower than the Lancet Report’s 78% attendance goal [11].
Strengths and limitations
The strength of this paper lies in its methodology. The study used nationally representative GDHS which allows generalization to all Ghanaian women. The use of both absolute and relative inequality measures provides multi-dimensionality to viewing the magnitude and trends of inequality in ANC visits. Also, this study presented the results through four equity stratifiers: economic status, level of education, place of residence, and sub-national region. As such, government, policy makers as well as responsible agencies can easily identify priority areas in revamping policies and interventions geared towards an increase in the proportion of 4 + ANC visits. Again, this will enable interventionists to optimize their resources in promoting 4 + ANC visits because they can now identify specific subpopulations and how to focus interventions towards the achievement of SDG 3.1 that seeks to reduce global MMR to less than 70 per 100,000 live births by 2030. Despite these strengths, there are some inherent limitations which should be considered. Our dataset was based on cross-sectional design; hence causal inferences cannot be established. Also, the results are entirely descriptive and ecological, and therefore no causal association can be inferred.
Conclusion
Evidence on inequities in 4 + ANC visits in Ghana was observed and a disproportionately lower uptake was found among women who were poor, uneducated, living in rural areas and the Northern region. There is a need for policy makers to design interventions that will enable disadvantaged subpopulations to benefit from ANC with 4 + visits to meet SDG 3.1 and 3.2, which aim to reduce MMR to less than 70/100, 000 live births and a neonatal mortality rate to as low as 12 per 1000 live births by 2030, respectively. Further studies are essential to understand the underlying factors for the observed inequalities in ANC attendance.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in the WHO’s HEAT version 3.1 [https://www.who.int/gho/health_equity/assessment_toolkit/en/].
Abbreviations
- ANC:
-
Antenatal care
- EA:
-
Enumeration Area
- GDHS:
-
Ghana Demographic and health Survey
- HEAT:
-
Health Equity Assessment Toolkit
- LMICs:
-
Low- and middle-income countries
- MMR:
-
Maternal mortality ratio
- PAF:
-
Population Attributable Fraction
- PAR:
-
Population Attributable Risk
- PCA:
-
Principal Component Analysis
- PPS:
-
Probability Proportional to Size
- SDG:
-
Sustainable Development Goal
- UI:
-
Uncertainty Intervals
- WHO:
-
World Health Organization
References
Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, Shackelford KA, Steiner C, Heuton KR, Gonzalez-Medina D, Barber R, Huynh C, Dicker D, Templin T. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;13(384):980–1004.
World Health Organization. Trends in maternal mortality: 1990–2015: estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: executive summary (No. WHO/RHR/15.23). World Health Organization. 2015.
Alkema L, Chou D, Hogan D, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet. 2016;30(387):462–74.
Ghana Statistical Service (GSS), Ghana Health Service (GHS), ICF. Ghana Maternal Health Survey 2017. Accra: GSS, GHS, and ICF; 2018.
Sakeah E, Okawa S, Rexford Oduro A, et al. Determinants of attending antenatal care at least four times in rural Ghana: analysis of a cross-sectional survey. Glob Health Action. 2017;10(1):1291879.
Arthur E. Wealth and antenatal care Use: implications for maternal health care utiliation in Ghana. Heal Econ Rev. 2012;2:14.
Gupta S, Yamada G, Mpembeni R, et al. Factors associated with four or more antenatal care visits and its decline among pregnant women in Tanzania between 1999 and 2010. PLoS ONE. 2014;9(7):e101893.
Joshi C, Torvaldsen S, Hodgson R, Hayen A. Factors associated with the use and quality of antenatal care in Nepal: a population-based study using the demographic and health survey data. BMC Pregnancy Childbirth. 2014;14(1):1–1.
Abekah-Nkrumah G, Abor PA. Socioeconomic determinants of use of reproductive health services in Ghana. Heal Econ Rev. 2016;6(1):1–5.
Pell C, Meñaca A, Were F, et al. Factors affecting antenatal care attendance: results from qualitative studies in Ghana, Kenya and Malawi. PLoS ONE. 2013;8(1): e53747.
Kassebaum NJ, Barber RM, Bhutta ZA, et al. Global, regional, and national levels of maternal mortality. 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1775–812.
Waniala I, Nakiseka S, Nambi W, et al. Prevalence, indications, and community perceptions of caesarean section delivery in Ngora District, Eastern Uganda: mixed method study. Obstet Gynecol Int. 2020;2020:5036260.
Ghana Statistical Service (GSS). Population and Housing Census: National analytical report”. Accra: GSS; 2010. p. 2013.
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF International. Ghana Demographic and Health Survey 2014. Rockville: GSS, GHS, and ICF International; 2015.
Rutstein S, Johnson K. DHS comparative reports no. 6: the DHS wealth index. Calverton: ORC Macro; 2004.
WHO. Health Equity Assessment Toolkit (HEAT): software for exploring and comparing health inequalities in countries. 2019. http://bmcmedresmethodol.biomedcentral.com.proxy.bib.uottawa.ca/articles/10.1186/s12874-016-0229-9%3e%3e. Accessed 5 Sept 2020.
World Health Organization. Handbook on health inequality monitoring with a special focus on low and middle income countries. Geneva: World Health Organization; 2013.
Hosseinpoor AR, Bergen N, Schlotheuber A, Victora C, Boerma T, Barros AJ. Data Resource Profile: WHO Health Equity Monitor (HEM). Int J Epidemiol. 2016;45(5):1404–1405e.
Asamoah BO, Agardh A, Pettersson KO, Östergren PO. Magnitude and trends of inequalities in antenatal care and delivery under skilled care among different socio-demographic groups in Ghana from 1988–2008. BMC Pregnancy Childbirth. 2014;14:295.
Dahiru T, Oche OM. Determinants of antenatal care, institutional delivery and postnatal care services utilization in Nigeria. Pan Afr Med J. 2015;21:321.
United State Agency for International Development (USAID) . STAT compiler: The DHS program. 2015. https://www.statcompiler.com/en/. Accessed 5 Sept 2020.
Yaya S, Bishwajit G, Shah V. Wealth, education and urban-rural inequality and maternal healthcare service usage in Malawi. BMJ Glob Health. 2016;1(2): e000085.
Sanogo NA, Yaya S. Wealth status, health insurance, and maternal health care utilization in Africa: evidence from Gabon. BioMed Res Int. 2020;(2020):1–12.
Fagbamigbe AF, Idemudia ES. Wealth and antenatal care utilization in Nigeria: policy implications. Health Care Women Int. 2017;38(1):17–37.
Okedo-Alex IN, Akamike IC, Ezeanosike OB, Uneke CJ. Determinants of antenatal care utilisation in sub-Saharan Africa: a systematic review. BMJ Open. 2019;9(10): e031890.
Alam N, Hajizadeh M, Dumont A, Fournier P. Inequalities in maternal health care utilization in sub-Saharan African countries: a multiyear and multi-country analysis. PLoS ONE. 2015;10(4): e0120922.
Ghaffar A, Pongponich S, Ghaffar N, Mehmood T. Factors associated with utilization of antenatal care services in Balochistan province of Pakistan: an analysis of the multiple indicator cluster survey (MICS) 2010. Pak J Med Sci. 2015;31(6):1447–52. https://doi.org/10.12669/pjms.316.8181.
Shibre G, Mekonnen W. Socio-economic inequalities in ANC attendance among mothers who gave birth in the past 12 months in Debre Brehan town and surrounding rural areas, North East Ethiopia: a community-based survey. Reprod Health. 2019;16(1):99.
Dickson KS, Darteh EKM, Kumi-Kyereme A, Ahinkorah BO. Determinants of choice of skilled antenatal care service providers in Ghana: analysis of demographic and health survey. Matern Health Neonatol Perinatol. 2018;4:14.
Dickson KS, Darteh EK, Kumi-Kyereme A. Providers of antenatal care services in Ghana: evidence from Ghana demographic and health surveys 1988–2014. BMC Health Serv Res. 2017;17(1):203.
Ganle JK, Parker M, Fitzpatrick R, Otupiri E. Inequities in accessibility to and utilisation of maternal health services in Ghana after user-fee exemption: a descriptive study. Int J Equity Health. 2014;13:89.
Agyemang S, Asibey BO. Effect of education on health care utilization in rural Ghana: the case of selected communities in The Bekwai municipality. KNUST J Geo & Dev. 2018;2(1):114–27.
Jansen T, Rademakers J, Waverijn G, Verheij R, Osborne R, Heijmans M. The role of health literacy in explaining the association between educational attainment and the use of out-of-hours primary care services in chronically ill people: a survey study. BMC Health Serv Res. 2018;18(1):394.
Grown C, Gupta GR, Pande R. Taking action to improve women’s health through gender equality and women’s empowerment. Lancet. 2005;365(9458):541–3. https://doi.org/10.1016/S0140-6736(05)17872-6.
Afulani PA. Rural/urban and socioeconomic differentials in quality of antenatal care in Ghana. PLoS ONE. 2015;10(2): e0117996.
Nketiah-Amponsah E, Senadza B, Arthur E. Determinants of utilization of antenatal care services in developing countries: recent evidence from Ghana. African J Eco Man Studies. 2013;4:1.
Basha GW. Factors affecting the utilization of a minimum of four antenatal care services in Ethiopia. Obstet Gynecol Int. 2019;2019:5036783.
Girum T. Assessment of timing of first antenatal care visit and associated factors among pregnant women attending antenatal care in Dilla town governmental health institutions, southern Ethiopia. Alternative and Integrative Medicine. 2016;5:3.
Ali AA, Osman MM, Abbaker AO, Adam I. Use of antenatal care services in Kassala, Eastern Sudan. BMC Pregnancy Childbirth. 2010;10:67. https://doi.org/10.1186/1471-2393-10-67.
Titaley CR, Dibley MJ, Roberts CL. Factors associated with underutilization of antenatal care services in Indonesia: results of Indonesia Demographic and Health Survey 2002/2003 and 2007. BMC Public Health. 2010;10:485. https://doi.org/10.1186/1471-2458-10-485.
Acknowledgements
Not applicable
Funding
No funding was received for this work.
Author information
Authors and Affiliations
Contributions
AS, JO, EB, HOD and BOA contributed to the conception and design of the study, interpreted the data, and prepared the first draft manuscript. AS, JO, EB, HOD and BOA contributed to the design of the study, interpreted the data, and critically reviewed the manuscript for its intellectual content. AS, JO, EB, HOD and BOA helped with data interpretation and critically reviewed the manuscript for its intellectual content. JO had the final responsibility to submit the manuscript for publication. All authors read and revised drafts of the paper and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was not required since the data is available to the public domain.
Consent for publication
Not applicable.
Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Seidu, AA., Okyere, J., Budu, E. et al. Inequalities in antenatal care in Ghana, 1998–2014. BMC Pregnancy Childbirth 22, 478 (2022). https://doi.org/10.1186/s12884-022-04803-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-022-04803-y