
Abstract
Background
In a variety of animal species, hyperthermia in pregnancy has been recognized as teratogenic. Hyperthermia interferes with protein synthesis via heat-shock proteins, which can entail membrane disruption, cell death, vascular disruption, and placental infarction. This can induce severe fetal malformations or death. Fever during pregnancy, especially during embryogenesis, has also been associated with congenital malformations in human offspring.
The purpose of this large cohort study of clinically recognized pregnancies was to investigate whether fever during first trimester was associated with an increased risk of congenital malformations in the offspring.
Methods
The Danish National Birth Cohort is a population-based cohort of 100,418 pregnant women and their offspring recruited in 1996 to 2002. Information on fever during pregnancy was collected prospectively by means of two telephone interviews.
The study population comprised the 77,344 pregnancies enrolled in the Danish National Birth Cohort where self-reported information on fever during first trimester of pregnancy was available. Pregnancy outcomes were identified through linkage with the National Patient Registry. Congenital malformations within the first three and a half years of life were categorized according to EUROCAT’s classification criteria. Logistic regression models were used to estimate the associations between fever in first trimester and overall congenital malformations and congenital malformations by subgroups.
Results
Eight thousand three hundred twenty-one women reported fever during first trimester (10.8%) and 2876 infants were diagnosed with a congenital malformation (3.7%). Fever during first trimester did not affect the risk of overall fetal congenital malformation (OR 0.99, 95% CI 0.88–1.12). The subgroup analyses indicated slightly higher risk of congenital anomalies in the eye, ear, face and neck (OR 1.29, 95% CI 0.78–2.12) and in the genitals (OR 1.17, 95% CI 0.79–1.12), whereas lower risk of malformations in the nervous system (OR 0.47, 95% CI 0.21–1.08), the respiratory system (OR 0.56, 95% CI 0.23–1.29) and in the urinary subgroup (OR 0.58, 95% CI 0.35–0.99) was suggested, the latter constituting the only statistically significant finding.
Conclusions
Overall, this study did not show any association between maternal fever in pregnancy and risk of congenital anomalies.
Similar content being viewed by others


Background
Congenital malformations are in the top 20 of leading causes of burden of disease globally [1] and are a significant contributor to infant mortality with 11,3% of neonatal deaths caused by congenital malformations [2]. Congenital malformations may result in long-term disability and thereby have significant impact on individuals, families, health care systems, and societies [3]. Malformations may have infectious, genetic or environmental origin but for the majority the etiology remains unknown [2].
For several decades, hyperthermia in pregnancy has been recognized as a teratogen in a variety of animal species including guinea pigs, rats, mice, pigs, sheep, and monkeys [4,5,6]. Hyperthermia interferes with protein synthesis via heat-shock proteins, which can entail membrane disruption, cell death, vascular disruption, and placental infarction [7,8,9,10]. All these mechanisms can induce severe fetal malformations or death.
Several case-control studies in human beings have associated fever in pregnancy with among other neural tube defects [11,12,13,14], cardiac malformations [15,16,17,18], oral clefts [19, 20], and renal malformations [21]. The nature of the specific malformations appears to depend on the extent, duration and timing of maternal fever [7], and it is therefore important to include information about the timing of these febrile episodes.
In this study, we investigate the association between fever in pregnancy and fetal congenital malformations in a large population-based cohort. We focused on fever in first trimester of pregnancy, when any teratogenic effect on the fetus is most plausible to occur. We expected more pronounced associations between fever and congenital anomalies the higher the temperature, the longer the duration of the febrile incident and with the time of fever during embryogenesis. Furthermore, we expected the association between timing of fever episodes and the different congenital malformation subgroups to vary due to the timing of the organogenesis.
Methods
Study population
Data was obtained from the Danish National Birth Cohort (DNBC), which is an ongoing population-based cohort of 100,418 pregnant women and their offspring recruited between March 1996 and November 2002 [22].
General practitioners invited pregnant women to participate in the study at their first antenatal care visit. To be able to participate in DNBC, the women had to: be pregnant, intend to carry their pregnancy to term, speak Danish well enough to be interviewed by telephone in Danish, and have a permanent address in Denmark. The women consented to be interviewed twice during pregnancy and allowed information concerning their own and their offspring’s health to be obtained from national registries.
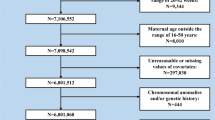
Of all the enrolled pregnancies (n = 100,418), those that resulted in birth of live-born singletons (n = 92,670) and where the woman had participated in both the first (n = 86,783) and the second interview (n = 80,781) were included in the study. Mother–infant pairs with more than one week of discrepancy between the mother’s report of gestational age in the two interviews (n = 1567) were excluded as the information regarding timing of fever were considered unreliable. Likewise, all mother-infant pairs with incomplete information on fever (n = 919) were excluded.
Incomplete information about any of the a priori defined confounders: parity (0, 1, 2 or ≥3), previous spontaneous abortion (yes or no), maternal age at conception (≤24, 25–29, 30–34 and ≥35), in vitro fertilization (yes or no/irrelevant), maternal diabetes mellitus (yes or no) or rheumatoid arthritis (yes or no), medical treatment of epilepsy (yes or no), binge drinking, defined as drinking five or more drinks at one occasion, during first trimester of pregnancy (yes or no), smoking during pregnancy (yes or no), and socio-occupational status (higher grade professionals, lower grade professionals, skilled workers, unskilled workers, students, and unemployed >1 year) (n = 951) also resulted in an exclusion from the study. The remaining 77,344 mother–infant pairs were included in the analyses.
Exposure
In this study the exposure of interest was fever during first trimester. Information about fever episodes was obtained in the two computer-assisted telephone interviews, where the first interview was completed at a median gestational age of 16 weeks (10th to 90th percentiles: 12–29 weeks) and the second at a median gestational age of 31 weeks (10th to 90th percentiles: 28–36 weeks). For the majority of women, information regarding fever was acquired from the first interview. For 7026 women, who participated in the first interview before the end of the 12th gestational week, we also used information about number and timing of fever episodes in the first trimester from the second interview. In both interviews, the women were asked about occurrence of fever, the maximum temperature, the timing of the fever episodes, the number of days with fever, and the number of fever episodes. English translations of the interviews are available at www.dnbc.dk.
In the analyses of the intensity of fever exposure, the maximum temperature was categorized as below 39 °C, over 39 °C, or unknown. The rationale for this categorization was based on literature showing that the teratogenic threshold effect in many species begins approximately at 1.5 °C above normal core body temperature [7].
Duration of fever was calculated as the longest period of consecutive days with fever (1 day, 2–3 days, 4 days or more, or unknown) and the fever episodes were divided into groups according to gestational age (pregnancy week 1–4, 5–8, and 9–12).
Outcome
Denmark has a Civil Registration System where all citizens are registered with a unique 10-digit identification number used in all registries to identify the person. The identification numbers were used to link information from the Danish National Patient Registry, where pregnancy outcomes including information on congenital malformations were identified [23].
Congenital malformations in live-born children were diagnosed by physicians according to the International Classification of Disease 10th version (ICD-10), and all children diagnosed with ICD-codes Q00.0 to Q99.9 during the first three and a half year of life were identified.
The congenital malformations were divided into categories according to the classification criteria of the European Surveillance of Congenital Anomalies (EUROCAT) as seen in Table 3, where the ICD-10 codes are also specified [24]. Isolated minor congenital malformations (n = 1692) were excluded as cases. According to EUROCAT, minor congenital malformations are characterized as malformations with lesser medical, functional or cosmetic importance [24] .
A small group of infants with aneuploidy (n = 36) was not included as cases, as this chromosomal anomaly is a result of errors in mitosis or meiosis happening before conception.
Some of the congenital malformation categories were joined to form a broader group. The ear, face and neck subgroup was pooled with the eye subgroup and the musculo-skeletal- and limb categories were also united. Finally, in addition to the ICD-10 codes defined by EUROCAT, the category “Other” included the subgroups with abdominal malformations and the chromosomal malformations other than aneuploidies.
Children with more than one malformation were included in each appropriate anomaly subgroup, but were only counted once in the “Overall malformations” group.
Covariates
Information on several covariates was obtained for main- and sub analyses (see Table 1). Information on the majority of the covariates was derived from the first interview, with the exception of medical treatment of epilepsy, use of antipyretics, and maternal infections, which was derived from the second interview.
Socio-occupational status was the household combined socio-occupational status, defined by the highest status within the couple. The information on maternal pre-diabetes mellitus was based on a combination of self-report and data from the National Patient Registry and this variable did not distinguish between Type I and Type II diabetes. Pre-conceptional intake of folic acid was self-reported at the time of recruitment to the cohort, and child sex came from the Civil Registration System. Maternal infections encompassed; urinary tract infections, vaginal infections, respiratory tract infections, gastroenteritis and childhood diseases.
Statistical analysis
The associations between fever in the first trimester of pregnancy and 1) all congenital malformations and 2) congenital malformations by subgroups were estimated as odds ratios (OR) using logistic regression. The estimated ORs were presented with 95% confidence intervals (CI). Crude and adjusted analyses were performed and the a priori defined covariates were included in the adjusted analyses.
Some of the children in the cohort were born to the same mother and to take this into account we estimated 95% CI using robust standard errors.
Sub analyses
To consider the influence of maternal infections during first trimester and use of antipyretics in first trimester on the estimated relationships, a first degree interaction between fever in first trimester, maternal infections and antipyretic use, respectively, was evaluated for overall congenital malformations using a Wald test.
Furthermore, the association between various measures of fever in first trimester (presented in Table 2) and overall congenital malformations was estimated while further adjusting for maternal infections in first trimester. Also, stratified analyses of the association between various measures of fever in first trimester and overall congenital malformations according to antipyretic use in the first trimester were performed.
Results
In total 2876 children of 77,344 live-born singletons in this study were diagnosed with a congenital malformation before the age of three and a half years. The overall malformation prevalence in the study population was 3.7%, and this figure was higher for offspring of mothers with diabetes mellitus (PP = 6.5%), rheumatoid arthritis (PP = 8.9%), and offspring of women receiving medical treatment for epilepsy (PP = 9.4%),
Overall, 46.6% of the mothers were nulliparas while 37.3% had given birth once before. However, in the subgroup of women with fever in first trimester only 40.6% were nulliparas while 42.1% were primiparas, Table 1.
Overall, 8321 (10.8%) women reported at least one episode of fever within the first 12 weeks of pregnancy. Of the women reporting fever, only 62,2% reported the maximum temperature and of these almost half (49,5%) reported fever incidents with a temperature of 39 °C or more. In contrast, almost all women provided information about the duration of the fever incident and the distribution can be seen in Table 2.
The analyses revealed no increased risk of overall congenital malformations when the exposure was fever at any point during first trimester of pregnancy (OR 0.99, 95% CI 0.88–1.12). The risk of congenital malformations was slightly higher if the fever episode occurred during the 1–4 gestational week (OR 1.13, 95% CI 0.83–1.54), though not statistically significant. The estimates for the other gestational periods were not associated with increased risk of congenital malformations and the same accounts for the intensity of fever and the number of days with fever, Table 2.
Sub analyses
Wald test showed no sign of interaction between fever in first trimester and maternal infections and antipyretic use, respectively (p-value = 0.95; p-value = 0.20). None of the estimates for the relationship between the various measures of fever in first trimester and overall congenital malformations as presented in Table 2 changed appreciably when further adjusting for maternal infections in first trimester or in the analyses stratified according to the use of antipyretics in first trimester (results not shown).
In relation to the subgroups of congenital malformations, fever during first trimester was associated with slightly increased risk of congenital malformations in the eye, ear, face and neck (OR 1.29, 95% CI 0.78–2.12) and in the genitals (OR 1.17, 95% CI 0.79–1.71), however, none of them statistically significant. Furthermore, a decreased risk of congenital malformations was seen in the following categories: nervous system (OR 0.47, 95% CI 0.21–1.08), urinary tract (OR 0.58, 95% CI 0.35–0.99) and respiratory system (OR 0.56, 95% CI 0.23–1.29). Of these, only the decreased risk of urinary tract congenital malformations was statistically significant. The remaining subgroups of congenital malformations were not associated with exposure to fever during first trimester of pregnancy, Table 3.
Discussion
In this large cohort study, fever during first trimester of pregnancy was not significantly associated with congenital malformations diagnosed within the child’s first three and a half years of life. The analyses demonstrated that there are no statistically significant association between fever in first trimester and any of the congenital malformation subgroups, except for a decreased risk of malformations in the urinary system. The reduced risk, although statistically insignificant, of having a congenital malformation in the nervous system is unexpected considering results from previous studies where central nervous system defects are among the most common consequences of hyperthermia [7, 11, 13, 25,26,27,28,29]. Since most malformations in the nervous system are extremely severe, a possible explanation might be that many of the fetuses with malformations in the nervous system were aborted before recognition of pregnancy or before the first antenatal care visit at the general practitioner and thereby before a possible enrollment into the DNBC.
A previous study reported that fever in the first 16 weeks of pregnancy did not increase the risk of spontaneous abortions in clinically recognized pregnancies in this cohort [8], and thus it seems unlikely that these congenital malformations resulted in spontaneous abortions at a later state in pregnancy.
During the study period, women over 35 years and women at high risk of having a child with congenital malformations were offered prenatal screening [22]. Hence, another feasible explanation of the decreased risk of having a child with malformations in the nervous system could be that the women, who had an ultrasonic examination diagnosing the fetus with severe malformations in the nervous system, subsequently had an induced abortion. Since the study population only includes live-born singletons, it is not possible to rule out that induced abortions could help explain the decreased risk of malformations in the nervous system. In order to address this question, we estimated the risk of induced abortion due to fetal disease among the women in the DNBC who participated in the first interview after week 12 (n = 82,003). The analysis indicated an increased risk of termination of pregnancy due to fetal abnormality (OR 1.56, 95% CI 0.96–2.55) if the women had fever during first trimester of pregnancy. Hence, this might partly explain the unexpected finding regarding nervous system anomalies.
The identification of a statistically significant reduced risk of giving birth to a child with urinary congenital malformations after having fever during first trimester of pregnancy found in this study does not correspond to the findings in a previous study [21]. However, as a number of statistical tests were conducted on the same overall study population this may be a chance finding and thus the result of a statistical type 1 error.
Previous studies on maternal fever and congenital malformations have reported different results. This inconsistency may be caused by differences in one or more study factors including the method used for measuring body temperature, duration and timing of fever episodes, recall bias in retrospective studies, small study sizes, and confounding.
Generally, participation rates in large cohort studies have diminished over the last decades to around the level observed in DNBC, where approximately 60% of the invited pregnant women in Denmark participated [22]. Because of the relatively low participation rate in the DNBC, selection bias is a possibility. The enrolled women have previously been observed to be slightly healthier overall than women in the source population; nevertheless, this have been shown to have very limited impact on risk estimates in DNBC [30], and the complete register-based follow-up of the cohort furthermore protects against selection bias.
Nonetheless, selection may still be the reason why a marginally lower proportion of overall congenital malformations is seen in our cohort when compared to the background population during the same time period [31]. In our cohort, the proportion of children diagnosed with a congenital malformation (including minor malformations) was 6% compared to 6.5% in the background population.
Higher socioeconomic profile and healthier life style are presumed to explain these differences, as women enrolled in cohorts have been shown to be healthier and more well-off [31,32,33,34]. Thus cohorts are selected samples, but baseline-selection is by definition independent of outcome and thereby does not introduce selection bias in the exposure-outcome association. However, baseline-selection may impact the confounding pattern, thus it is different from the source population of each cohort [35]. Strengths of the present study include the large sample size, the prospectively collected information on fever, the detailed information on body temperature, duration and timing of fever episodes, the nearly complete follow-up and the adjustment for a variety of covariates. Furthermore, since all confidence intervals in this study are relatively narrow the accuracy of the estimate is high.
A limitation in this study was that, like most studies on birth anomalies, only live-born children were included, since congenital malformations in stillbirths, spontaneous abortions and medically terminated pregnancies are not registered in Denmark.
Additionally, the relatively limited number of children with congenital anomalies in this study did not allow us to stratify the outcome further than the overall groups of congenital malformations recommended by EUROCAT. This lumping of specific malformations into body system groups might have masked slightly increased risk of the rarest malformations.
Information on fever in first trimester was collected prospectively, i.e. before pregnancy outcome was known, and thus any misclassification of exposure was non-differential, leading to an underestimation of the association. The lacking information on how body temperature was measured imparts an uncertainty to the data regarding temperature. Nonetheless, body temperature was (in the times of the data collection) usually measured with a rectal thermometer and the temperature information indicated can therefore likely be regarded as a measure of core temperature [8]. Additionally, the maximum temperature is not necessarily the correct maximum temperature for the event but the highest value measured.
The overall validity of data on diagnoses from the National Patient Registry is considered to be acceptable for general surveillance and epidemiological research [35], also when specifically considering congenital malformations [32]. Children diagnosed with a congenital malformation until the age of three and a half years were included in the study, and this period ensured that the majority of congenital malformations usually not detected at birth were also included. However, uncertainty and inaccuracies in the diagnoses are still seen in national registries, but incorrect diagnoses can at most lead to non-differential misclassification, which would result in an underestimation of the association.
Conclusions
While most case-control studies indicate positive associations between maternal fever and selected congenital anomalies, the results of this large-scale cohort study do not support a relation between maternal fever during first trimester of pregnancy and congenital anomalies.
References
Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet Lond Engl. 2012;380:2197–223.
WHO | Congenital anomalies [Internet]. WHO. [cited 2017 Oct 23]. Available from: www.who.int/mediacentre/factsheets/fs370
Sever L, Lynberg MC, Edmonds LD. The impact of congenital malformations on public health. Teratology. 1993;48:547–9.
Edwards MJ, Shiota K, Smith MS, Walsh DA. Hyperthermia and birth defects. Reprod Toxicol Elmsford N. 1995;9:411–25.
Edwards MJ. Congenital malformations in the rat following induced hyperthermia during gestation. Teratology. 1968;1:173–7.
Krausova T, Peterka M. Teratogenic and lethal effects of 2–24h hyperthermia episodes on chick embryos. J Therm Biol. 2007;32:193–203.
Graham JM, Edwards MJ, Edwards MJ. Teratogen update: gestational effects of maternal hyperthermia due to febrile illnesses and resultant patterns of defects in humans. Teratology. 1998;58:209–21.
Andersen A-MN, Vastrup P, Wohlfahrt J, Andersen PK, Olsen J, Melbye M. Fever in pregnancy and risk of fetal death: a cohort study. Lancet Lond Engl. 2002;360:1552–6.
Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL. Maternal fever and birth outcome: a prospective study. Teratology. 1998;58:251–7.
Edwards MJ, Walsh DA, Li Z. Hyperthermia, teratogenesis and the heat shock response in mammalian embryos in culture. Int J Dev Biol. 1997;41:345–58.
Yin Z, Xu W, Xu C, Zhang S, Zheng Y, Wang W, et al. A population-based case-control study of risk factors for neural tube defects in Shenyang, China. Childs Nerv Syst ChNS Off J Int Soc Pediatr Neurosurg. 2011;27:149–54.
Shaw GM, Todoroff K, Velie EM, Lammer EJ. Maternal illness, including fever and medication use as risk factors for neural tube defects. Teratology. 1998;57:1–7.
Suarez L, Felkner M, Hendricks K. The effect of fever, febrile illnesses, and heat exposures on the risk of neural tube defects in a Texas-Mexico border population. Birt Defects Res A Clin Mol Teratol. 2004;70:815–9.
Li Z, Ren A, Zhang L, Guo Z, Li Z. A population-based case-control study of risk factors for neural tube defects in four high-prevalence areas of Shanxi province, China. Paediatr Perinat Epidemiol. 2006;20:43–53.
Botto LD, Lynberg MC, Erickson JD. Congenital heart defects, maternal febrile illness, and multivitamin use: a population-based study. Epidemiol Camb Mass. 2001;12:485–90.
Tikkanen J, Heinonen OP. Maternal hyperthermia during pregnancy and cardiovascular malformations in the offspring. Eur J Epidemiol. 1991;7:628–35.
Oster ME, Riehle-Colarusso T, Alverson CJ, Correa A. Associations between maternal fever and influenza and congenital heart defects. J Pediatr. 2011;158:990–5.
Botto LD, Panichello JD, Browne ML, Krikov S, Feldkamp ML, Lammer E, et al. Congenital heart defects after maternal fever. Am J Obstet Gynecol. 2014;210:359.e1–359.e11.
Shahrukh Hashmi S, Gallaway MS, Waller DK, Langlois PH, Hecht JT, National Birth Defects Prevention Study. Maternal fever during early pregnancy and the risk of oral clefts. Birt Defects Res A Clin Mol Teratol. 2010;88:186–94.
Wang W, Guan P, Xu W, Zhou B. Risk factors for oral clefts: a population-based case-control study in Shenyang, China. Paediatr Perinat Epidemiol. 2009;23:310–20.
Abe K, Honein MA, Moore CA. Maternal febrile illnesses, medication use, and the risk of congenital renal anomalies. Birt Defects Res A Clin Mol Teratol. 2003;67:911–8.
Olsen J, Melbye M, Olsen SF, Sørensen TI, Aaby P, Andersen AM, et al. The Danish National Birth Cohort--its background, structure and aim. Scand J Public Health. 2001;29:300–7.
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39:30–3.
EUROCAT [Internet]. [cited 2017 Oct 23]. Available from: http://www.eurocat-network.eu/aboutus/datacollection/guidelinesforregistration/malformationcodingguides
Li Z, Ren A, Liu J, Pei L, Zhang L, Guo Z, et al. Maternal flu or fever, medication use, and neural tube defects: a population-based case-control study in northern China. Birt Defects Res A Clin Mol Teratol. 2007;79:295–300.
Layde PM, Edmonds LD, Erickson JD. Maternal fever and neural tube defects. Teratology. 1980;21:105–8.
Halperin LR, Wilroy RS. Maternal hyperthermia and neural-tube defects. Lancet Lond Engl. 1978;2:212–3.
Miller P, Smith DW, Shepard TH. Maternal hyperthermia as a possible cause of anencephaly. Lancet Lond Engl. 1978;1:519–21.
Dreier JW, Andersen A-MN, Berg-Beckhoff G. Systematic review and meta-analyses: fever in pregnancy and health impacts in the offspring. Pediatrics. 2014;133:e674–88.
Nohr EA, Frydenberg M, Henriksen TB, Olsen J. Does low participation in cohort studies induce bias? Epidemiol Camb Mass. 2006;17:413–8.
Varela MMM-S, Nohr EA, Llopis-González A, Andersen A-MN, Olsen J. Socio-occupational status and congenital anomalies. Eur J Pub Health. 2009;19:161–7.
Larsen H, Nielsen GL, Bendsen J, Flint C, Olsen J, Sørensen HT. Predictive value and completeness of the registration of congenital abnormalities in three Danish population-based registries. Scand J Public Health. 2003;31:12–6.
Nilsen RM, Vollset SE, Gjessing HK, Skjaerven R, Melve KK, Schreuder P, et al. Self-selection and bias in a large prospective pregnancy cohort in Norway. Paediatr Perinat Epidemiol. 2009;23:597–608.
Pizzi C, De Stavola BL, Pearce N, Lazzarato F, Ghiotti P, Merletti F, et al. Selection bias and patterns of confounding in cohort studies: the case of the NINFEA web-based birth cohort. J Epidemiol Community Health. 2012;66:976–81.
Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–90.
Acknowledgements
The Danish National Research Foundation has established the Danish Epidemiology Science Centre that initiated and created the Danish National Birth Cohort. The cohort is furthermore a result of a major grant from this foundation. Additional support for the Danish National Birth Cohort has been obtained from the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation and the Augustinus Foundation.
Funding
Funding for salary was provided by Department of Public Health, University of Copenhagen.
Availability of data and materials
The data that support the findings of this study are available from DNBC but restrictions apply to the availability of these data, which were used under license for the current study and are not publicly available. However, data are available from the authors upon reasonable request and with permission of both the Danish Data Protection Agency as well as the DNBC Steering Committee.
Author information
Authors and Affiliations
Contributions
Study design and analytical strategy were developed by AMNA and JK. LLRS, SKU, JWD and KSL carried out the data management and the statistical analyses. LLRS wrote the first version of the paper and all authors took part in the revision. All authors have seen and approved the final version of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The National Scientific Ethics Committees approved the DNBC before the beginning of the data collection, and in accordance with Danish legislation the Danish Data Protection Agency approved the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Sass, L., Urhoj, S.K., Kjærgaard, J. et al. Fever in pregnancy and the risk of congenital malformations: a cohort study. BMC Pregnancy Childbirth 17, 413 (2017). https://doi.org/10.1186/s12884-017-1585-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-017-1585-0