
Abstract
Background
Renal perfusion may redistribute from cortex to medulla during systemic hypovolaemia and after renal ischaemia for other reasons, but there is no consensus on this matter. We studied renal perfusion after renal ischaemia and reperfusion.
Methods
Renal perfusion distribution was examined by use of 153Gadolinium-labeled microspheres (MS) after 2 h (hrs) and 4 h ischaemia of the pig kidney followed by 4 h of reperfusion. Intra-arterial injected MS are trapped in the glomeruli in renal cortex, which means that MS are not present in the medulla under normal physiological conditions.
Results
Visual evaluation after reperfusion demonstrated that MS redistributed from the renal cortex to the medulla in 6 out of 16 pigs (38%) subjected to 4 h ischaemia and in one out of 18 pigs subjected to 2 h ischaemia. Central renal uptake of MS covering the medullary/total renal uptake was significantly higher in kidneys subjected to 4 h ischaemia compared with pigs subjected to 2 h ischaemia (69 ± 5% vs. 63 ± 1%, p < 0.001), and also significantly higher than in the contralateral kidney (69 ± 5% vs. 63 ± 2%, p < 0.001). Analysis of blood and urine demonstrated no presence of radioactivity.
Conclusion
The study demonstrated the presence of MS in the renal medulla in response to renal ischaemia and reperfusion suggesting that severe ischaemia and reperfusion of the pig kidney leads to opening of functional shunts bypassing glomeruli.
Similar content being viewed by others


Background
Blood perfusion of the kidney is higher than the perfusion of any other organ when looking at flow in relation to the weight if the organ. In the human kidney, approximately 80% of the total perfusion distributes to the cortex providing only a minor fraction of the perfusion to the renal medulla [1], which also has a higher oxygen extraction during perfusion than the cortex. However, after severe systemic hypovolaemia, pale renal cortex with red highly perfused medulla is seen, and cortical necrosis with no regain of function is seen in some cases.
In 1947, Trueta and coworkers reported that renal blood flow appeared to be shunted to the renal medulla during haemorrhage or shock [2]. This phenomenon was termed “Cortical ischaemia with maintained blood flow through the medulla” [3, 4]. Redistribution of renal perfusion with relative cortical ischaemia is still an accepted outcome in response to haemorrhagic shock. Although almost 70 years have passed by since this original observation, there is still not a clear understanding on how this takes place [5,6,7,8,9].
Microspheres (MS) can be used to measure regional tissue blood flow [10]. Under normal physiological conditions intra-arterial injected microspheres are trapped in the glomeruli in the renal cortex. Thus, MS are not present in the renal medulla unless they have bypassed the glomeruli. We have developed a pig model where kidneys can be subjected to ischaemia by arterial clamping and subsequent reperfusion and we hypothesise that the number of MS present in the renal medulla is proportional to the number of functional shunts in the glomeruli. Thus, we examined the renal distribution of intra-arterial injected MS with the assumption that the presence of radio labeled MS in the renal medulla is a result of MS that have entered the renal medulla via shunts.
Methods
The methods are described in detail elsewhere [11]. In brief, 34 female Danish landrace/Yorkshire pigs with a mean weight of 38 ± 2 kg were exposed to unilateral warm ischaemia by clamping the renal artery for 2 h (n = 18) or for 4 h (n = 16) followed by 4 h of reperfusion. Catheters were inserted in the left jugular vein, and the carotid artery for continuous monitoring of blood pressure, infusion of drugs and fluid. Baby feeding tubes were placed in the ureters to collect urine. The aorta was catheterised through the femoral artery and the catheter tip for MS injection was placed in the aortic arch. After 4 h of reperfusion, renal perfusion was estimated by injection of 15–20 MBq of 153Gadolinium-labeled MS with a diameter of 15 µm. After termination and nephrectomy, the renal distribution of MS was studied in absolute counts over each kidney using a gamma-camera (BrightView, Philips Medical Systems, San Jose, CA, USA, 2009). Total renal counts and counts over the central renal areas including medulla were estimated by computer drawing of the region of the entire kidney and over the central 75% of the kidney. All counts were corrected for background radiation and acquisition time, and normalised to the amount of injected tracer.
Based on the visual perfusion redistribution of the scintigram, each kidney was graded from 0 – 3 in a blinded way by two observers: Grade 0: Homogeneous pattern similar to control kidneys. Grade 1: Weaker activity, but still homogeneous. Grade 2: Showing a pattern, identifying the medulla. Grade 3: Showing a pattern, clearly showing the medullary architecture and the anatomical outline of calyces.
Statistics
For statistical analysis an open-source statistical package from SciPy was used [12]. (version 0.17.1, www.scipy.org, 2016). Observer agreement were assessed using Cohen's Kappa statistic. Continuous data are expressed as mean ± standard deviation, geometric mean with 95% confidence interval (CI) or number with percentages, and with 95% CI when appropriate. Differences between groups were tested using Welsh T-test. Mann–Whitney U tests were used to compare independent groups when data were not normally distributed. A difference was considered significant when P < 0.05.
Results
The weight of the kidneys subjected to 4 h of ischaemia was significantly higher than the weight of the kidneys subjected to 2 h of ischaemia (p < 0.005) (Table 1). In both groups the renal weight was significantly higher than the weight of the contralateral non-ischaemic kidney (p < 0.001). At baseline (60 min), we found a mean single kidney GFR value of 30.2 ± 8.8 ml/min with no significant difference between groups [11]. During reperfusion the regain in GFR was close to zero.
The total renal uptake of MS as an indicator of blood flow was significantly lower after 4 h ischaemia than after 2 h ischaemia (p < 0.001). After 4 h ischaemia the MS uptake was also significantly lower than the uptake of the contralateral kidney (p < 0.001). The renal MS uptake after 2 h ischaemia did not differ significantly from the uptake of the contralateral kidney (p = 0.5) (Table 1).
Uptake of MS in the 75% central renal area including the medulla measured in per cent of uptake in the total kidney was significantly higher in kidneys subjected to 4 h compared to 2 h ischaemia (p < 0.001). In kidneys subjected to renal ischaemia for 4 h it was also significantly higher than in the contralateral kidney (p < 0.001) (Table 1).
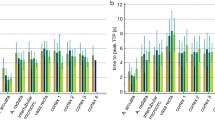
Redistribution of MS from cortex to medulla as assessed by blinded visual evaluation of the scintigrams showed redistribution in 6 out of 16 pigs (38%) subjected to ischaemia for 4 h, and in one out of 18 pigs (5%) with ischaemia for 2 h. Figure 1 shows an example of renal MS redistribution after 4 h ischaemia. The scintigram from the ischaemic side shows high activity in the medulla and faint activity in the renal cortex. Figure 2 shows that the higher the perfusion redistribution grade of the kidney, the higher uptake of MS in the central renal area including the medulla relative to uptake in total kidney.

Distribution of radio-labeled microspheres in a pig after renal ischaemia and reperfusion In comparison to the non-ischaemic right kidney, the left kidney shows an increased uptake of radio-labeled microspheres in renal medulla relative to the total kidney

Comparison of methods for the study of distribution of radio-labeled microspheresThe figure shows a positive correlation between visual distribution score grade 1–3 and the measured fraction of microspheres in the central kidney including medulla relative to the entire kidney (r2 = 0.98). Differences between 2 and 4 h ischaemia is marginally significant (p ~ 0.08). Grade 0 is a homogeneous pattern similar to control kidneys and Grade 3 is a pattern clearly showing the medullary architecture and the anatomical outline of calyces
Analysis of blood and urine samples demonstrated that no detectable radioactivity was present in these samples.
Discussion
The present study suggests that radioactive labeled microspheres (MS) can identify corticomedullary shunts after ischaemia and reperfusion of the human like polypapillary porcine kidney.
We studied renal blood flow by use of uptake of MS after unilateral renal ischaemia for 2 and 4 h followed by 4 h of observation after reperfusion. After intra-arterial injection of MS the absolute renal uptake of MS was significantly reduced in the kidneys subjected to 4 h total ischaemia. The uptake of MS after 2 h of renal ischaemia did not differ significantly from the uptake in the contralateral non-ischaemic kidney. After 4 h ischaemia, there was a relatively high uptake of MS in the central area of the kidney including the renal medulla both on the scintigrams and calculated from the absolute values. These observations may be explained by the special anatomy of blood supply to the kidneys. Blood supply to the nephron is maintained by two vascular systems organised in a serial manner: the capillaries in the glomeruli and the tubular capillaries in the renal medulla [1]. Thus, intra-arterial injected MS reach the renal cortex with the arterial blood, and in the glomeruli they are trapped due to their diameter of 15 µm and thereby separated from the blood stream. Thus, measuring total renal blood flow may be done from the number of MS in the whole kidney, whereas regional distribution of MS is unreliable in calculation of the relative distribution of renal perfusion. However, this normal trapping of MS in the glomeruli explained by renal anatomy makes it possible to quantify functional active shunts from the number of MS present in the renal medulla. In contrast to the early anatomical studie by Trueta and others [2] we made a physiological study with MS as a tracer. We measured uptake of radiolabelled MS on planar images by use of a 2-dimensional technique. We did not have access to SPECT/CT images in these pig studies. Therefore, due to anatomical overlap of medulla and cortex the uptake in renal medulla will be overestimated, but the uptake in the central 75% includes the total medulla. Our results are consistent with the opening of corticomedullary shunts in the ischaemic kidney. However, we cannot exclude that vasodilation in cortical juxtamedullary afferent arterioles after long-term ischaemia could explain our findings, although we believe that our 15 µm MS would not be able to pass the capillaries in glomeruli. Our visualisation technique seems to indicate presence of MS in medulla and not in the juxtamedullary cortex.
Our findings of corticomedullary shunts in severely ischaemic kidneys are in agreement with a resent published study by Schutter and coworkers [13]. By use of MRI they assessed the renal flow over time during normothermic machine perfusion (NMP) in porcine kidneys and human kidneys discarded for transplantation. Interestingly, they demonstrated by use or MRI, that the regional renal flow is entirely different from the total renal flow, and they found for all kidneys that the central region and medulla of the kidney was predominantely perfused initially, while the cortex reached a dominant perfusion state after 1–2 h, normalizing the flow distribution in the kidney. In addition, when they added a period of NMP hypoperfusion, demonstration a intrarenal shift of perfusion from the cortical area to the medullar regions. In their study, normal flow distribution was achieved in all kidneys, which was not the case in our study where the corticomedullary shunt remained in 38% and 5% of the kidneys subjected to 4 and 2 h ischemia followed by reperfusion. These are most likely the most damaged kidneys but it would have been interesting to see if these kidney could have improved had they been subjected to NMP instead of in situ reperfusion. From other experimental studies we know, that even severely damaged porcine kidneys with 75 min warm ischemia can be successfully transplanted in a survival model [14]. Prolonged warm ischemia remains a challenge in donation after circulatory death and a better understanding of the cotticomedullary shunts may be of benefit.
Conclusion
In conclusion, the study showed the presence of radiolabeled MS in the renal medulla in response to severe renal ischaemia suggesting that this leads after reperfusion to opening of functional shunts bypassing the glomeruli. Radiolabeled MS have been used for decades for the measurement of organ blood flow and perfusion and the present results point to functional intrarenal shunts, which have been suggested for decades, but not verified so far.
Availability of data and materials
The datasets generated and analysed during the current study are included in this published article, and are available from the corresponding author on reasonable request.
References
Munger K, Kost C Jr, Brenner B, Maddox D. The renal circulations and glomerular ultrafiltration. In: Taal M, Chertow G, Marsden P, Skorecki K, Yu Y, Brenner B, editors. Brenner and Rectors, The Kidney. Philadelphia: Elsevier Saunders; 2012. p. 94–137.
Trueta J, Barclay A, Daniel P. Studies of the renal circulation. Oxford: Blackwell Scientific Publications Ltd; 1947.
Daniel P, Peabody C, Prichard M. Cortical ischaemia of the kidney with maintained blood flow through the medulla. Q J Exp Physiol Cogn Med Sci. 1952;37:11–8.
Daniel P, Peabody C, Prichard M. Observations on the circulation through the cortex and the medulla of the kidney. Q J Exp Physiol Cogn Med Sc. 1951;36:199–203.
Lilienfields L, Maganzini H, Bauer M. Blood flow in the renal medulla. Circ Res. 1961;9:614–7.
Spinelli FR, Wirz H, Brucher C, Pehling G. Non-existence of shunts between afferent and efferent arterioles of juxtamedullary glomeruli in dog and rat kidneys. Nephron. 1972;9:123–8.
Stone AM, Stein T, LaFortune J, Wise L. Changes in intrarenal blood flow during sepsis. Surg Gynecol Obstet. 1979;148:731–4.
Greenfield SP, Lewis W III, Perry B, Wan J, Morin F III. Regional renal blood flow measurements using radioactive microspheres in a chronic porcine model with unilateral vesicoureteral reflux. J Urol. 1995;154:816–9.
Langenberg C, Bellomo R, May C, Wan L, Egi M, Morgera S. Renal blood flow in sepsis. Crit Care. 2005;9:R363–74.
Peters A, Myers M. Measurement of blood flow. In: Peters A, Myers M, editors. Physiological measurements with Radionuclides in Clinical Practice. Oxford: Oxford University Press; 2003. p. 63–7.
Pedersen SS, Keller AK, Nielsen MK, Jespersen B, Falborg L, Rasmussen JT, et al. Cell injury after ischemia and reperfusion in the porcine kidney evaluated by radiolabelled microspheres, sestamibi, and lactadherin. EJNMMI Res. 2013;3:62.
Jones E, Oliphant T, Peterson P. SciPy. Open source scientific tools for Python. 2001. Available from: http://www.scipy.org/. Accessed Sept 2013.
Schutter R, Lantiga VA, Hamelink TL, Pool MBF, Varsseveld OCV, Potze JH, et al. Magnetic resonance imaging assessment of renal flow distribution patterns during ex vivo normothermic machine perfusion in porcine and human kidneys. Transpl Int. 2021;34(9):1643–55. https://doi.org/10.1111/tri.13991.
Lohmann S, Eijken M, Møldrup U, Møller BK, Hunter J, Moers C, et. al.: Ex Vivo Administration of Mesenchymal Stromal Cells in Kidney Grafts Against Ischemia-reperfusion Injury-Effective Delivery Without Kidney Function Improvement Posttransplant.Transplantation. 2021 1;105(3):517–528. doi: https://doi.org/10.1097/TP.0000000000003429.
Acknowledgements
We thank Alain Prigent, Paris and Birger Hesse, Copenhagen for their advice and helpful suggestions and Ken Peter Kragsfeldt for help with the figures.
Funding
The project was carried out with financial support from the Faculty of Health Sciences, Aarhus University, the Institute of Clinical Medicine, Aarhus University, Helen & Ejnar Bjørnows Foundation, Sophus Jacobsen & Hustru Astrid Jacobsens Foundation, the A.P. Moeller Foundation, the Danish Kidney Foundation, and C.C. Klestrup & Hustru Henriette Klestrups Foundation.Sundhedsvidenskabelige Fakultet,Aarhus Universitet,Institut for Klinisk Medicin,Aarhus Universitet,Helen & Ejnar Bjørnows Fond,A.P. Møller og Hustru Chastine Mc-Kinney Møllers Fond til almene Formaal,The Danish Kidney Foundation,Snedkermester Sophus Jacobsen og Hustru Astrid Jacobsens Fond,C.C. Kelstrup &Hustru Henriette Klestrups FondThe Funding did not have anything to do with the study design, datacollection, analysis, interpretation or writing.
Author information
Authors and Affiliations
Contributions
MR, conception, design, interpretation, writing, SGS, conception, design, acquisition, analysis, interpretation, writing, AKK, conception, design, acquisition, interpretation, LEN, design, acquisition, analysis, writing, CF, interpretation, analysis, writing. BJ, conception, design, interpretation, writing, JF, interpretation, writing, All Authors have edited, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Animal experiments conform to internationally accepted standards and have been approved by the appropiate institutional review board. The study was approved by the Danish Inspectorate of Animal Experiments (2010/561–1837).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rehling, M., Skjøth, S.G., Frøkiær, J. et al. Corticomedullary shunting after ischaemia and reperfusion in the porcine kidney?. BMC Nephrol 23, 146 (2022). https://doi.org/10.1186/s12882-022-02780-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-022-02780-0