
Abstract
Background
Performing a kidney biopsy is necessary to accurately diagnose diseases such as glomerulonephritis and tubulointerstitial nephritis, among other such conditions. These conditions predispose patients to chronic kidney disease, as well as acute kidney injury (AKI). Notably, most epidemiological studies describing AKI have not investigated this patient population.
Methods
Included patients admitted to the nephrology ward of a tertiary hospital who underwent percutaneous kidney biopsy. AKI was diagnosed based on the Kidney Disease: Improving Global Outcomes criteria.
Results
Of the 223 patients investigated, 140 (62.8%) showed AKI. Of these, 91 (65%), 19 (13.6%), and 30 (21.4%) presented with AKI classified as stages 1, 2, and 3, respectively. The primary indication for performing biopsy was nephrotic syndrome or nephrotic proteinuria (73 [52.1%] in the AKI vs. 51 [61.4%] in the non-AKI group, p = 0.048). Focal segmental glomerulosclerosis was the most prevalent primary disease (24 [17.1%] in the AKI vs. 15 [18.0%] in the non-AKI group, p = 0.150). Multivariate analysis of risk factors associated with AKI showed hemoglobin levels (odds ratio [OR] 0.805, 95% confidence interval [CI] 0.681–0.951, p = 0.011), serum high-density lipoprotein cholesterol levels (HDL-c, OR 0.970, 95% CI 0.949–0.992, p = 0.008), and baseline serum creatinine levels (OR 2.703, 95% CI 1.471–4.968, p = 0.001) were significantly associated with AKI.
Conclusions
We observed a high prevalence of AKI in hospitalized patients who underwent kidney biopsy to investigate their renal disease, particularly glomerulonephritis. Higher levels of hemoglobin and serum HDL-c were associated with a lower risk of AKI.
Similar content being viewed by others


Background
Acute kidney injury (AKI) is a risk factor for the development of chronic kidney disease (CKD) and chronic end-stage renal disease (ESRD). AKI is also associated with increased short- and long-term mortality rates [1]. AKI is a complex and heterogeneous clinical syndrome observed mainly in elderly patients with several comorbidities. These patients are usually admitted to intensive care units (ICU), and AKI is primarily attributed to sepsis in such cases [2]. Percutaneous renal biopsy is usually contraindicated in these patients to prevent complications, and they are usually diagnosed with “acute tubular necrosis”.
In contrast, some kidney diseases such as glomerulonephritis and tubulointerstitial nephritis, among other such clinical conditions require histopathological analysis of kidney tissue specimens to accurately determine diagnosis, disease activity and chronicity [3, 4]. Notably, most epidemiological studies have investigated patients with AKI have not included this patient population in the analysis. For example, a meta-analysis analyzed the worldwide incidence of AKI observed that studies primarily included patients admitted to the ICU and those who underwent cardiac surgery [5].
Therefore, we investigated the prevalence and risk factors associated with AKI in hospitalized patients who underwent kidney biopsy for histopathological diagnosis.
Methods
Study design and patients
This was a retrospective cohort study, included patients admitted to the Nephrology ward of Hospital São Paulo, Universidade Federal de São Paulo, São Paulo, Brazil. Patients were eligible if submitted to percutaneous kidney biopsy performed with aged ≥16 years as indicated by the nephrologists. Exclusion criteria were kidney transplant recipients. In our center, all percutaneous native kidney biopsies were performed in patients admitted exclusively to the nephrology ward. We did not perform native kidney biopsy in outpatient setting. Data were obtained, between January 2008 and December 2014, from patients’ medical records and the electronic hospital database. The follow-up period underwent 12-month after the kidney biopsy.
Demographic and clinical data
We analyzed the following variables: age, sex, race, body mass index (BMI), major comorbidities such as hypertension, diabetes mellitus (DM), cancer, cardiovascular disease (CVD including heart failure, coronary artery disease, stroke, and peripheral artery disease), and systemic lupus erythematosus (SLE).
We evaluated the use of diuretics, antibiotics, statins, angiotensin-converting enzyme inhibitors (ACEI), and/or angiotensin receptor blockers (ARB), nonsteroidal anti-inflammatory drugs (NSAID), and contrast media (recent use as well as administration during hospitalization). Previous use of corticosteroids was also recorded.
Indications for renal biopsy were nephrotic syndrome (characterized by edema, hypoalbuminemia [< 3.5 g/L], dyslipidemia, and proteinuria ≥3.5 g/24 h [h]), or nephrotic-range proteinuria (proteinuria ≥3.5 g/24 h), rapidly progressive glomerulonephritis (RPGN, characterized by hematuria and/or proteinuria on urinalysis associated with rapid decline in renal function indicated by progressively increasing serum creatinine levels, which may occur over days, weeks, or months prior to renal biopsy), sub-nephrotic proteinuria (isolated proteinuria > 1.0 g/24 h), dysmorphic hematuria associated with some grade of proteinuria, renal dysfunction if unknown origin, and renal manifestations of systemic diseases.
Evaluation performed upon admission
The following parameters were evaluated upon admission: hemoglobin, serum sodium, potassium, ionic calcium, phosphorus, and albumin levels, pH and bicarbonate levels, serum total cholesterol and its fractions, serum triglycerides, serum creatinine and urea levels, as well as 24-h urinary protein excretion. The glomerular filtration rate (GFR) was estimated using the Modification of Diet in Renal Disease Study Group (MDRD) equation [6].
All patients underwent kidney and urinary tract ultrasonography. The length of the kidneys was recorded in all patients.
Optical microscopy analysis and immunofluorescence studies were performed for histopathological diagnostic confirmation as well electron microscopy, when indicated. All analysis was performed by a single renal pathologist.
We evaluated the serum creatinine level upon admission, during hospitalization, and specific time-points after discharge until 12 months after the kidney biopsy. The reading that showed the lowest level during hospitalization was considered the baseline serum creatinine level because laboratory data prior to hospitalization were unavailable. The highest serum creatinine level during hospitalization was used to diagnose AKI.
Acute kidney injury
We defined and classified AKI observed during hospitalization based on the Kidney Disease: Improving Global Outcomes (KDIGO) criteria using only serum creatinine levels [7]. AKI was defined as an increase in serum creatinine ≥0.3 mg/dL over ≤48 h or a ≥ 1.5-fold increase in serum creatinine over baseline levels within the 7 days. AKI was classified into 3 stages as follows: stage 1: ≥1.5 to 1.9-fold increase in serum creatinine levels or an increase of 0.3 mg/dL compared with baseline levels, stage 2: ≥2.0 to 2.9-fold increase in serum creatinine levels compared with baseline levels, and stage 3: > 3.0-fold increase in serum creatinine levels compared with baseline creatinine levels or serum creatinine levels > 4.0 mg/dL with an increase of at least 0.5 mg/dL, or the initiation of renal replacement therapy.
Outcomes
The following outcomes were assessed: kidney function (evaluated by serum creatinine levels), need for dialysis initiation, and mortality within 12 months after kidney biopsy.
Statistical analysis
Data were expressed as mean and standard deviation for normally distributed variables and as median and quartiles (25–75%) for variables showing non-normal distribution. Parametric distribution was confirmed using the Shapiro-Wilk test. We used the Student’s t-test or the Mann-Whitney test for numerical variables and the Chi-square test for comparison between nominal variables.
For covariance analyze repeated measures of creatinine and for intergroup comparison of data, we used the Generalized Estimation Equations and applied the autoregressive structure correlation matrix [1] and gamma distribution with log link.
Variables that were significantly associated with AKI on univariate analysis (p < 0.05) were subjected to multivariate logistic regression analysis for variables such as age and sex.
A p value < 0.05 was considered statistically significant. SPSS software, version 20.0 (IBM Corp, USA, 2011) was used for statistical analysis.
Results
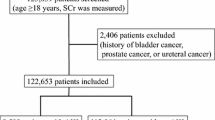
The study included 267 patients, of which 44 (16.5%) patients were diagnosed with ESRD during admission and were excluded from the study. Of the remaining patients (N = 223), 140 (62.8%) were diagnosed with AKI during hospitalization. No significant intergroup difference was observed in sex (men, 68 [48.6%] in the AKI vs. 41 [49.4%] in the non-AKI group, p = 0.508). Patients with AKI were older than patients without AKI (41.2 ± 17.7 vs. 35.3 ± 14.4 years, p = 0.03) with similar BMI (25.7 ± 5.4 in the AKI vs. 24.5 ± 4.0 kg/m2 in the non-AKI group, p = 0.291). Most patients were white in both groups (87 [62.8%] in the AKI vs. 51 [61.5%] in the non-AKI group, p = 0.482).
No statistically significant differences were observed between the AKI and non-AKI groups, respectively in the percentage of patients with hypertension (64 [45.7%] vs. 30 [36.1%], p = 0.096), patients with CVD (9 [6.4%] vs. 3 [3.6%], p = 0.279), and patients with a history of cancer (5 [3.6%] vs. 1 [1.2%], p = 0.273). DM was more prevalent in the AKI group (17 [12.1%] vs. 3 [3.6%], p = 0.023).
A lower percentage of patients in the AKI group used ACEIs/ARBs (57 [40.7%] vs. 45 [54.2%], p = 0.038). Additionally, a larger number of patients in the AKI group received a potentially nephrotoxic antibiotic (16 [11.4%] vs. 2 [2.4%], p = 0.012). No statistically significant difference was observed between the AKI and non-AKI groups with respect to the use of diuretics (42 [30.0%] vs. 32 [38.6%], p = 0.130), statins (31 [22.1%] vs. 23 [27.7%], p = 0.227), NSAIDs (19 [13.6%] vs. 9 [10.8%], p = 0.347), and corticosteroids (34 [3.0%] vs. 28 [33.7%], p = 0.091). No patient underwent contrast examination during hospitalization.
The primary indications for renal biopsy were nephrotic-range proteinuria or nephrotic syndrome (73 [52.1%] in the AKI vs. 51 [61.4%] in the non-AKI group, p = 0.048), renal dysfunction of undetermined etiology (23 [16.4%] in the AKI vs. 5 [6.0%] in the non-AKI group, p = 0.001), and hematuria with non-nephrotic-range proteinuria (11 [7.8%] in the AKI vs. 11 [13.2%] in the non-AKI group, p = 1,000). RPGN was an indication exclusively in the AKI group (18 [12.9%] vs. 0, p < 0.001).
Primary renal disease was the most common type of disease observed in both groups (86 [61.4%] in the AKI vs. 67 [80.7%] in the non-AKI group, p = 0.125). The primary diagnoses were focal segmental glomerulosclerosis (FSGS) (24 [17.1%] in the AKI vs. 15 [18.0%] in the non-AKI group, p = 0.150) and minimal change disease (MCD) (21 [15%] in the AKI vs. 15 [18%] in the non-AKI group, p = 0.317). Secondary diseases predominated in the AKI group (54 [38.6%] vs. 16 [19.3%], p < 0.001). SLE was the main cause of secondary renal disease, with classes III and IV being the most prevalent (Table 1).
Laboratory data and measurements of renal length are presented in Table 2. Statistically significant differences were observed between the AKI and non-AKI groups with respect to the following variables: serum hemoglobin (11.7 ± 2.7 vs. 13.4 ± 2.1 g/dL, p < 0.001), serum sodium (137 ± 3.7 vs. 138 ± 2.6 mEq/L, p = 0.047), serum urea (76.0 [55.0–115.0] vs. 57.0 [39.0–77.3] mg/dL, p < 0.001), serum bicarbonate (21.4 ± 5.5 vs. 25.7 ± 4.0 mEq/L, p < 0.001), and serum HDL-c (43.5 ± 16.2 vs. 56.3 ± 28.5 mg/dL, p < 0.001). No statistically significant intergroup difference was observed in renal length.
Table 3 shows an intergroup comparison of serum creatinine levels across different time-points in the study. We observed that the AKI group showed higher serum creatinine levels than the non-AKI group (p < 0.001) across the entire follow-up period. Compared with peak levels during admission, we observed a decrease in serum creatinine levels in the AKI group after 12 months (p < 0.05).
Among patients diagnosed with AKI (62.8%), 91 (65.0%) were classified as showing stage I disease, 19 (13.6%) as stage 2, and 30 (21.4%) as stage 3 disease.
Dialysis was performed in 19 (8.5%) patients in the AKI group and of these 19, 9 (4.0%) remained dependent on dialysis therapy at the time of discharge. All patients were dialysis-free at the end of 12 months. Notably, 8 patients (3.6%) died and 5 of them died of infections during hospitalization. Table 4 shows the multivariate analysis of factors associated with the development of AKI.
Discussion
This study showed a high prevalence of AKI in hospitalized patients who underwent kidney biopsy for renal disease primarily caused by glomerulonephritis. Most patients showed primary renal disease, and the most common indications for renal biopsy were nephrotic-range proteinuria or nephrotic syndrome. Among the primary diseases, FSGS showed the highest prevalence. Among all secondary diseases, lupus glomerulonephritis was the most common.
Epidemiological studies investigating AKI should necessarily describe patients’ baseline serum creatinine levels. In this study, we defined the lowest serum creatinine level during hospitalization as an estimate of baseline renal function, given the lack of previous values. Retrospective baseline serum creatinine levels (assuming GFR = 75 mL/min/1.73 m2) based on KDIGO criteria may miss the occurrence of AKI in the community [7]. Moreover, our study group comprised patients predominantly with glomerulonephritis, which tends to demonstrate an insidious onset and progression. Occasionally, in a few cases, AKI can be diagnosed in clinical practice only by analyzing temporal changes in serum creatinine levels. Our findings concur with this observation in that progressive improvement in renal function occurred in the AKI group throughout the study period.
We could not rule out the existence of a pre-renal component of AKI, particularly in patients with less severe AKI (stage 1). Despite the long-term protective effect of ACEI/ARB in renal diseases in patients with proteinuria, their use may cause acute and reversible renal dysfunction, particularly when used concomitantly with diuretics and in patients with other conditions causing hypovolemia [8, 9]. Interestingly, we observed a higher percentage of patients using ACEI/ARB in the non-AKI group. In contrast to data reported in the literature, the effect of AKI on glomerular hemodynamics (decreased filtration pressure) and the potential negative effect on renal function was not evident in the present study [8, 10]. For example, a recent study investigating patients with hypertension using ACEI/ARB and diuretics showed AKI was associated with CKD and poor cardiac performance [11]. Another study involving new users of ACEI/ARB reported a low incidence of AKI and showed AKI was more likely to be associated with the individual clinical characteristics than with the use of the medication itself [12].
Proteinuria and low serum albumin levels are risk factors for AKI [13, 14]. This is particularly evident in patients diagnosed with MCD, notably elderly patients with hypertension (showing arteriolar nephrosclerosis) and patients with more severe degrees of nephrotic syndrome [15]. In our cohort, no significant differences were observed in 24-h proteinuria, serum albumin levels, and the number of patients diagnosed with major proteinuria-causing diseases (FSGS, MCD and Membranous Glomerulonephritis) between the AKI and non-AKI groups. Previous studies have shown that DM is also an independent risk factor for AKI, mainly secondary to microvascular dysfunction [16, 17]. Although the AKI group included a greater number of patients with DM, it was not an independent risk factor in our study. Our study included younger patients than those studied previously, and owing to the multiple disease diagnosed, AKI could be attributed to other mechanisms as well.
Pre-existing kidney dysfunction serves as an independent risk factor for AKI in conditions such as sepsis and contrast-induced nephropathy, as well as in patients undergoing cardiac surgery or solid organ transplantation, and in patients admitted to the ICU [18,19,20,21,22]. This factor was also relevant in our study. Patients with CKD are at a higher risk of AKI secondary to the role of several etiopathogenetic contributors such as activation of transforming growth factor beta, action of hypoxia-inducible factors, mitochondrial and endothelial dysfunction, oxidative stress, chronic inflammation, and alterations in renal blood flow autoregulation observed in this patient population [23,24,25].
Anemia and AKI are occasionally associated. A few studies have shown anemia serves as an independent risk factor for AKI [26,27,28]. Previous studies have shown anemia was a risk factor for contrast-induced nephropathy in patients undergoing coronary angiography [29], postoperatively in patients undergoing hip arthroplasty [30], in patients admitted to the ICU [31], and postoperatively in patients undergoing cardiac surgery [32]. In these cases, AKI associated with anemia could be attributed to a reduction in the oxygen supply to renal tissues and the consequent aggravation of pre-existing ischemia occurring in hospitalized patients [32,33,34].
In our study, we observed a higher level of serum hemoglobin was associated with a lower incidence of AKI. Several studies have shown an association between anemia and AKI; however, it is unclear whether higher levels of serum hemoglobin could reduce the incidence of AKI. It could be deduced that early intervention, for example, through the use of recombinant human erythropoietin, could reduce the risk of AKI in specific diseases, such as in glomerulonephritis. Previous studies have shown the role of erythropoietin in patients admitted to the ICU and in those undergoing cardiac surgery was controversial and in a few cases the benefit was independent of hematocrit and serum hemoglobin levels [35].
Altered lipid metabolism is common in patients with renal disease, particularly in those with glomerulonephritis and nephrotic syndrome. Hypercholesterolemia and hypertriglyceridemia are the most common findings in such cases; however, low serum HDL-c levels may occur. Resolution of nephrotic syndrome usually tends to reverse these changes [36].
HDL-c possesses antioxidant properties, thereby reducing endothelial damage and the risk of atherosclerosis [37]. The MDRD study showed a low serum HDL-c level was an independent risk factor associated with a faster decline in GFR. In experimental AKI models, HDL-c showed anti-inflammatory actions and reduced ischemia and reperfusion injury [38, 39]. Roveran Genga et al. showed low levels of serum HDL-c in patients with sepsis were associated with a higher incidence of sepsis-associated AKI [40]. Another study reported by Smith et al. demonstrated higher levels of preoperative serum HDL-c decreased the incidence of AKI after cardiac surgery [41]. Arora et al. observed low levels of serum HDL-c were associated with AKI after revascularization surgery for chronic limb ischemia [42].
In our cohort, we observed an association between higher levels of serum HDL-c and lower incidence of AKI. We inferred perhaps intensive drug therapy for dyslipidemia in addition to exercise and dietary strategies could improve patients’ lipid profile and consequently reduce the incidence of AKI, particularly in patients with glomerulonephritis.
The following are the limitations of our study: [1] The lack of outpatient baseline serum creatinine values is the main limitation, since some cases of non-recovering AKI could be missed. [2] Because it is a retrospective and single-center study, a bias cannot be ruled out. [3] Histopathological heterogeneity and dropouts during follow-up are other limitations. [4] We do not have information regarding the treatment for each specific disease diagnosed by biopsy. Despite these limitations, the high prevalence of AKI observed in these subjects is concerning because this patient population is often excluded from epidemiological studies investigating AKI.
Conclusions
We observed a high prevalence of AKI in hospitalized patients who underwent kidney biopsy to investigate their renal disease, particularly glomerulonephritis. Higher levels of hemoglobin and serum HDL-c were associated with lower risks of AKI.
Availability of data and materials
The data that support the findings of this study are available from Universidade Federal de São Paulo (UNIFESP), but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Universidade Federal de São Paulo (UNIFESP).
Abbreviations
- ACEI:
-
angiotensin-converting enzyme inhibitors
- AKI:
-
Acute kidney injury
- ARB:
-
angiotensin receptor blockers
- BMI:
-
body mass index
- CKD:
-
chronic kidney disease
- CVD:
-
cardiovascular disease
- DM:
-
diabetes mellitus
- ESRD:
-
chronic end-stage renal disease
- FSGS:
-
focal segmental glomerulosclerosis
- GFR:
-
glomerular filtration rate
- HDL-c:
-
high-density lipoprotein cholesterol
- ICU:
-
intensive care units
- KDIGO:
-
Kidney Disease: Improving Global Outcomes
- MCD:
-
minimal change disease
- MDRD:
-
Modification of Diet in Renal Disease Study Group
- NSAID:
-
nonsteroidal anti-inflammatory drugs
- RPGN:
-
rapidly progressive glomerulonephritis
- SLE:
-
systemic lupus erythematosus
References
Forni LG, Darmon M, Ostermann M, Oudemans van Straaten HM, Pettilä V, Prowle JR, et al. Renal recovery after acute kidney injury. Intensive Care Med. 2017;43:855–66.
Ali T, Khan I, Simpson W, Prescott G, Townend J, Smith W, et al. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol. 2007;18:1292–8.
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, et al. National Kidney Foundation. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139:137–47.
Prakash J, Sen D, Kumar NS, Kumar H, Tripathi LK, Saxena RK. Acute renal failure due to intrinsic renal diseases: review of 1122 cases. Ren Fail. 2003;25:225–33.
Susantitaphong P, Cruz DN, Cerda J, Abulfaraj M, Alqahtani F, Koulouridis I, et al. Acute kidney injury advisory Group of the American Society of nephrology. World incidence of AKI: a meta-analysis. Clin J Am Soc Nephrol. 2013;8:1482–93.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of diet in renal disease study group. Ann Intern Med. 1999;130:461–70.
KDIGO AKI Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
Cox ZL, McCoy AB, Matheny ME, Bhave G, Peterson NB, Siew ED, et al. Adverse drug events during AKI and its recovery. Clin J Am Soc Nephrol. 2013;8:1070–8.
Kheterpal S, Tremper KK, Englesbe MJ, O'Reilly M, Shanks AM, Fetterman DM, et al. Predictors of postoperative acute renal failure after noncardiac surgery in patients with previously normal renal function. Anesthesiology. 2007;107:892–902.
Alabdan N, Gosmanova EO, Tran NQ, Oliphant CS, Pan H, Broyles JE, et al. Acute kidney injury in patients continued on renin-angiotensin system blockers during hospitalization. Am J Med Sci. 2017;353:172–7.
Chen Q, Zhu S, Liao J, He W. Study of acute kidney injury on 309 hypertensive inpatients with ACEI/ARB - diuretic treatment. J Natl Med Assoc. 2018;110:287–96.
Mansfield KE, Nitsch D, Smeeth L, Bhaskaran K, Tomlinson LA. Prescription of renin-angiotensin system blockers and risk of acute kidney injury: a population-based cohort study. BMJ Open. 2016;6(12):e012690.
Clark WF, Macnab JJ, Sontrop JM, Jain AK, Moist L, Salvadori M, et al. Dipstick proteinuria as a screening strategy to identify rapid renal decline. J Am Soc Nephrol. 2011;22:1729–36.
Shao M, Wang S, Parameswaran PK. Hypoalbuminemia: a risk factor for acute kidney injury development and progression to chronic kidney disease in critically ill patients. Int Urol Nephrol. 2017;49:295–302.
Smith JD, Hayslett JP. Reversible renal failure in the nephrotic syndrome. Am J Kidney Dis. 1992;19:201–13.
Thakar CV, Christianson A, Himmelfarb LAC. Acute kidney injury episodes and chronic kidney disease risk in diabetes mellitus. Clin J Am Soc Nephrol. 2011;6:2567–72.
Lee KW, Kim TM, Kim KS, Lee S, Cho J, Park JB, et al. Renal ischemia-reperfusion injury in a diabetic monkey model and therapeutic testing of human bone marrow-derived mesenchymal stem cells. J Diabetes Res. 2018;5182606, 9 pages.https://doi.org/10.1155/2018/5182606.
Kheterpal S, Tremper KK, Heung M, Rosenberg AL, Englesbe M, Shanks AM, et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology. 2009;110:505–15.
Mehta RH, Grab JD, O'Brien SM, Bridges CR, Gammie JS, Haan CK, et al. Society of Thoracic Surgeons National Cardiac Surgery Database Investigators: bedside tool for predicting the risk of postoperative dialysis in patients undergoing cardiac surgery. Circulation. 2006;114:2208–16.
Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP. A clinical score to predict acute renal failure after cardiac surgery. J Am Soc Nephrol. 2005;16:162–8.
Benko A, Fraser-Hill M, Magner P, Capusten B, Barrett B, Myers A, et al. Canadian association of radiologists: consensus guidelines for the prevention of contrast-induced nephropathy. Can Assoc Radiol. 2007;58:79–87.
Hsu CY, Ordonez JD, Chertow GM, Fan D, McCulloch CE, Go AS. The risk of acute renal failure in patients with chronic kidney disease. Kidney Int. 2008;74:101–7.
Robinson-Cohen C, Katz R, Price BL, Harju-Baker S, Mikacenic C, Himmelfarb J, et al. Association of markers of endothelial dysregulation Ang1 and Ang2 with acute kidney injury in critically ill patients. Crit Care. 2016;20:207.
Powell TC, Powell SL, Allen BK, Griffin RL, Warnock DG, Wang HE. Association of inflammatory and endothelial cell activation biomarkers with acute kidney injury after sepsis. Springerplus. 2014;3:207.
Sun CY, Chang SC, Wu MS. Uremic toxins induce kidney fibrosis by activating intrarenal renin-angiotensin-aldosterone system associated epithelial-to-mesenchymal transition. PLoS One. 2012;7:e34026.
Shema-Didi L, Ore L, Geron R, Kristal B. Is anemia at hospital admission associated with in-hospital acute kidney injury occurrence? Nephron Clin Pract. 2010;115(2):c168–76.
Haase M, Bellomo R, Story D, Letis A, Klemz K, Matalanis G, et al. Effect of mean arterial pressure, haemoglobin and blood transfusion during cardiopulmonary bypass on post-operative acute kidney injury. Nephrol Dial Transplant. 2012;27:153–60.
Shacham Y, Gal-Oz A, Leshem-Rubinow E, Arbel Y, Flint N, Keren G, et al. Association of admission hemoglobin levels and acute kidney injury among myocardial infarction patients treated with primary percutaneous intervention. Can J Cardiol. 2015;31:50–5.
Sreenivasan J, Zhuo M, Khan MS, Li H, Fugar S, Desai P, et al. Anemia (hemoglobin ≤ 13 g/dL) as a risk factor for contrast-induced acute kidney injury following coronary angiography. Am J Cardiol. 2018;122:961–5.
Choi YJ, Kim SO, Sim JH, Hahm KD. Postoperative Anemia is associated with acute kidney injury in patients undergoing Total hip replacement arthroplasty: a retrospective study. Anesth Analg. 2016;122:1923–8.
Han SS, Baek SH, Ahn SY, Chin HJ, Na KY, Chae DW, et al. Anemia is a risk fator for acute kidney injury and long-term mortality in critically ill patients. Exp Ther Med. 2015;237:287–95.
Karkouti K, Wijeysundera DN, Yau TM, et al. Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation. 2009;119:495–502.
Legrand M, Pirracchio R, Pirracchio R, Rosa A, Petersen ML, Van der Laan M, et al. Incidence, risk factors and prediction of post-operative acute kidney injury following cardiac surgery for active infective endocarditis: an observational study. Crit Care. 2013;17:R220.
Sickeler R, Phillips-Bute B, Kertai MD, Schroder J, Mathew JP, Swaminathan M, et al. The risk of acute kidney injury with co-occurrence of anemia and hypotension during cardiopulmonary bypass relative to anemia alone. Ann Thorac Surg. 2014;97(3):865–71.
Kim JH, Shim JK, Song JW, Song Y, Kim HB, Kwak YL. Effect of erythropoietin on the incidence of acute kidney injury following complex valvular heart surgery: a double blind, randomized clinical trial of efficacy and safety. Crit Care. 2013;17:R254.
Agrawal S, Zaritsky JJ, Fornoni A, Smoyer WE. Dyslipidaemia in nephrotic syndrome: mechanisms and treatment. Nat Rev Nephrol. 2018;14:57–70.
Jurek A, Turyna B, Kubit P, Klein A. LDL susceptibility to oxidation and HDL antioxidant capacity in patients with renal failure. Clin Biochem. 2006;39:19–27.
Cockerill GW, Huehns TY, Weerasinghe A, Stocker C, Lerch PG, Miller NE, et al. Elevation of plasma high-density lipoprotein concentration reduces interleukin- 1-induced expression of E-selectin in an in vivo model of acute inflammation. Circulation. 2001;103:108–12.
Thiemermann C, Patel NS, Kvale EO, Cockerill GW, Brown PA, Stewart KN, et al. High density lipoprotein (HDL) reduces renal ischemia/reperfusion injury. J Am Soc Nephrol. 2003;14:1833–43.
Roveran Genga K, Lo C, Cirstea M, Zhou G, Walley KR, Russell JA, et al. Two-year follow-up of patients with septic shock presenting with low HDL: the effect upon acute kidney injury, death and estimated glomerular filtration rate. J Intern Med. 2017;281:518–29.
Smith LE, Smith DK, Blume JD, Linton MF, Billings FT 4th. High-density lipoprotein cholesterol concentration and acute kidney injury after cardiac surgery. J Am Heart Assoc. 2017. https://doi.org/10.1161/JAHA.117.006975.
Arora P, Davari-Farid S, Gannon MP, Lohr JW, Dosluoglu HH, Nader ND. Low levels of high-density lipoproteins are associated with acute kidney injury following revascularization for chronic limb isquemia. Ren Fail. 2013;35:838–44.
Acknowledgments
We thank Dr. Marcello Fabiano de Franco (in memorian) for the histological analysis of the renal biopsies, Danilo Takashi Aoike for statistical analysis.
Funding
The present study is investigator-initiated research. The authors have received specific funding from Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP - www.fapesp.br) at number 2014/20605–7. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
The conception of the study was made by MSD, HPK, TOCS, TGVZ and SCP. All authors participated in the design of the study, data collection, and analysis and interpretation of data. The article was draft by MSD and HPK and was revised by all authors. The authors GMK and AT provided additional intellectual content and all the authors approved the final version of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All study was conducted in compliance with the principles of the Declaration of Helsinki and in accordance with Good Clinical Practice guidelines. The study was approved by the local Ethics Committee of Universidade Federal de São Paulo (UNIFESP), under number 385.749. Confidentiality of all data has been maintained. The requirement for informed consent was waived for this study owing to its retrospective design.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Konigsfeld, H.P., Viana, T.G., Pereira, S.C. et al. Acute kidney injury in hospitalized patients who underwent percutaneous kidney biopsy for histological diagnosis of their renal disease. BMC Nephrol 20, 315 (2019). https://doi.org/10.1186/s12882-019-1514-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-019-1514-8