
Abstract
Background
IgA nephropathy (IgAN) is the most common primary glomerulonephritis worldwide. Urinary micro-RNA (miRNA) level is increasingly reported to as non-invasive markers of various kidney diseases. We aim to identify urinary miRNA targets for the diagnosis of IgAN.
Methods
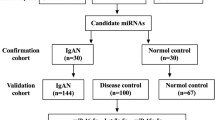
In the development cohort, we performed complete miRNA profiling of urinary sediment in 22 patients with IgAN and 11 healthy controls (CTL). Potential miRNA targets were quantified by a separate validation cohort of 33 IgAN patients and 9 healthy controls.
Results
In the development cohort, we identified 39 miRNA targets that have significantly different expression between IgAN and CTL (14 up-regulated, and 25 down-regulated). Among the 8 miRNA targets chosen for validation study, urinary miR-204, miR-431 and miR-555 remained significantly reduced, and urinary miR-150 level was significantly increased in the IgAN as compared to CTL. The area-under-curve of the receiver operating characteristic (ROC) curve for urinary mi-204 level for the diagnosis of IgAN was 0.976, and the diagnostic performance of combining additional miRNA targets was not further improved. At the cut-off 1.70 unit, the sensitivity and specificity of urinary miR-204 was 100 and 55.5%, respectively, for diagnosing IgAN.
Conclusions
Urinary miR-150, miR-204, miR-431 and miR-555 levels are significantly different between IgAN and healthy controls; urinary miR-204 level alone has the best diagnostic accuracy.
Similar content being viewed by others

Background
Immunoglobulin A nephropathy (IgAN) is the most common primary glomerulonephritis in the world [1]. The clinical course of IgAN, however, is highly variable. Around one-third of the patients progress to dialysis-dependent renal failure in 10 years [2], while many others remain asymptomatic despite persistent abnormal urinalysis [3]. At present, the major clinical tools for predicting prognosis of IgAN are baseline renal function, proteinuria, and histological grading [2,3,4]. Non-invasive biomarkers are much needed for risk stratification as well as monitoring of response to treatment.
MicroRNA (miRNA) is a group of short noncoding RNA molecules with a length around 22 bases that regulates gene expression at the post-transcriptional level by incomplete base pairing with the 3′-untranslated region of target messenger RNAs [5]. In the context of IgAN, a genome-wide analysis of peripheral blood mononuclear cell miRNA profile showed that abnormal miR-148b expression in B lymphocyte may be responsible for the aberrant glycosylation of IgA1, and plays a central role in the early phase of pathogenesis [6]. On the other hand, intra-renal miR-29c level is important for the regulation of renal fibrosis and later stages of IgAN progression [7].
Recently, miRNA level in urinary sediment has been explored as non-invasive biomarkers of kidney diseases [8,9,10]. A few early studies suggest that urinary levels of several miRNAs are substantially changed in IgAN [11]. For example, urinary miR-200a, miR-200b and miR-429 levels were reported to be decreased in IgAN [12], while urinary miR-29b, miR-29c, and miR-93 levels correlated with renal function and the severity of histological damage [13]. Published data on urinary miRNA, however, are scattered and focused on target miRNAs. In the present study, our objective is to identify a panel of urinary miRNA targets that could be used for the diagnosis and risk stratification of IgA nephropathy.
Methods
Overall study design
This is an observational study approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong. All study procedures were in compliance with the Declaration of Helsinki. For the development cohort, we recruited 22 patients with biopsy-confirmed IgAN and 6 healthy volunteers as controls (CTL). For the validation cohort, we recruited 33 patients with biopsy-confirmed IgAN and 9 healthy volunteers as controls (CTL). For the IgAN group, we excluded patients with crescentic changes in the kidney biopsy, IgA vasculitis, or concomitant urinary tract infection.
After written informed consent, a whole-stream early morning urine specimen was collected for RNA extraction. We reviewed the patients’ demographic, clinical, and pathological information. Clinical parameters reviewed included proteinuria, estimated glomerular filtration rate (GFR) as estimated by a standard equation [14].
miRNA extraction
RNA isolation kit was purchased from Ambion, Inc. Austin, TX, USA. The methods of RNA extraction from urine have been described previously [15]. Briefly, urine specimens were collected and sent to laboratory for processing immediately or stored in 4 °C overnight. Urine samples were centrifuged at 3000-g for 30 min and at 13000-g for 5 min at 4 °C. Specimens were then be stored at − 80 °C until use.
NanoString miRNA assay
The digital multiplexed NanoString nCounter miRNA Expression Assay (NanoString Technologies, Seattle, WA) was performed according to manufacturer’s instructions with total RNA extracted [16]. Briefly, we prepared miRNA by ligating a specific tag onto the 3′ end of each mature target, followed by hybridization at 65 °C overnight to nCounter Reporter and Capture probes. Residual Reporter and Capture probes were removed by an automated station. Bound complexes were then immobilized in standard cartridges, which were then placed in a digital analyzer for data acquisition. The nSolver Analysis software (NanoString) (version 2.5) was used for data analysis. Gene counts were control-normalized and compared to that of β2-microglobulin.
Quantification of specific miRNA
For the validation cohort, urinary level of RNA targets identified in the previous part were measured by real-time quantitative polymerase chain reaction (RT-QPCR) using the ABI Prism 7900 Sequence Detection System (Applied Biosystems, Foster City, CA, USA). We used commercially available unlabeled Taqman® primers and FAM™ dye-labeled TaqMan® MGB probe for the targets (Applied Biosystems), and the RNU48 as the house-keeping gene [10, 11]. We analyzed the results by Sequence Detection Software version 2.0 (Applied Biosystems). For quantitation, we used the relative ΔΔCT method. As described previously [17, 18], when there was no detectable transcript after 40 cycles, we assigned the value half of the detection limit for non-parametric analysis.
Histological assessment
Histological lesions were classified by the revised Oxford classification [19]. The severity of glomerulosclerosis and tubulointerstitial fibrosis were further assessed by morphometric study as described previously [20, 21]. Briefly, Jones’ silver staining was performed on 4 μm thick sections of renal biopsy specimen. Computerized image analysis method was then performed by the MetaMorph 4.0 image-analyzing software (Universal Imaging Corporation™, Downingtown, PA). Ten glomeruli and 10 randomly selected tubulointerstitial areas were assessed for each patient.
Clinical follow up
We further reviewed the progression of renal function during subsequent follow up. The slope of decline of estimated GFR was calculated by the least squares regression method. Renal events were defined as 30% worsening of estimated GFR as compared to baseline or the need of dialysis.
Statistical analysis
Statistical analysis was performed by SPSS for Windows software version 24.0 (IBM corporation, Armonk, NY). Data were expressed as mean ± standard deviation or median (inter-quartile range [IQR]) as appropriate. The levels of individual miRNA targets were compared by Mann Whitney U test between groups, and the correlation with clinical parameters were explored by the Spearman’s rank correlation coefficient. Receiver operating characteristic (ROC) curves were constructed by standard methods. P value below 0.05 was considered statistically significant. All probabilities were two-tailed.
Results
Characteristics of study participants
The clinical and demographic characteristics of patients participating in this study are summarized in Table 1. The pathological characteristics of the IgAN group are summarized in Table 2.
Urinary miRNA level in the development cohort
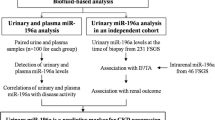
The correlation between the average urinary miRNA level and the fold of change in urinary miRNA level between IgAN and CTL groups is depicted in Fig. 1. Among the miRNA targets that are highly expressed in the urinary sediment, we identified 39 miRNA targets that have significantly different expression between IgAN and CTL groups (14 up-regulated, and 25 down-regulated) (Table 3).

Scatter plot depicting the distribution and correlation between average urinary miRNA of the IgA nephropathy (IgAN) group and the change in urinary miRNA levels (IgAN as compared to the control group) in the development cohort. Urinary miRNA levels were compared to that of β2-microglobulin (see Patients and Methods for details). The change in urinary miRNA levels is presented as log2 of the ratio between average urinary miRNA levels of the IgAN to the CTL group. Each dot represents one miRNA target
Of the 39 potential targets identified, 8 were chosen for further validation. Specifically, miR-16, miR-26a, and miR-150 were the three most up-regulated targets, miR-204, miR-431, and miR-555 were the three most down-regulated ones, miR-221 is the only target that was significantly up-regulated in the IgAN group as well as correlated with estimated GFR, and miR-155 has been reported by our previous study [22].
Urinary miRNA level in the validation cohort
In the validation cohort, there were close internal correlation between urinary levels of miR-16, miR-26, miR-155 and miR-221 (Additional file 1: Table S1). The urinary miRNA levels of the IgAN and CTL groups in the validation cohort are summarized and compared in Fig. 2. In essence, urinary miR-204, miR-431 and miR-555 remained significantly reduced, but only urinary miR-150 level was significantly increased in the IgAN group as compared to the CTL group. In the validation cohort, the median increase in urinary miR-150 was 1.44 log (IQR − 0.21 to 2.12, p = 0.007); the median decrease in urinary miR-204, miR-431 and miR-555 were − 5.42 log (IQR − 3.25 to − 8.28, p < 0.0001), − 4.06 log (IQR − 0.34 to − 5.06, p = 0.023), and − 5.17 log (IQR − 2.40 to − 8.46, p < 0.0001), respectively.

Comparison of urinary miRNA levels between IgA nephropathy (IgAN) and control (CTL) groups in the validation cohort: (a) miR-16; (b) miR-26a; (c) miR-150; (d) miR-155; (e) miR-221; (f) miR-204; (g) miR-431; and (h) miR-555. Whisker-box plot, with boxes indicate median, 25th and 75th percentiles, whiskers indicate 5th and 95th percentiles. Data are compared by Kruskal Wallis test
Accuracy of diagnosis
The performance of urinary miRNA levels for the diagnosis of IgA nephropathy was explored by ROC curves (Fig. 3). In essence, the areas under curve (AUC) of the ROC curves of all 4 targets (miR-150, miR-204, miR-431, and miR-55) were statistically significant, with the AUC of miR-204 the highest (AUC = 0.976, p < 0.0001), and the diagnostic performance of combining additional miRNA targets was not further improved. For miR-204, an urinary level below 0.34 unit has a 100% specificity (and 90.9% sensitivity) in diagnosing IgA nephropathy, while the level above 1.70 unit has a 100% sensitivity (and 55.5% specificity) to exclude the diagnosis.

Receiver operating characteristic (ROC) curves indicating the performance of urinary levels of (a) miR-150; (b) miR-204; (c) miR-431; and (d) miR-555 for the diagnosis of IgA nephropathy. AUC, area under curve
Relation with clinical and pathological parameters
There were modest but statistically significant correlations between urinary miR-555 level and the duration of disease (Spearman’s r = − 0.590, p = 0.004) and baseline estimated GFR (r = 0.478, p = 0.024), but not with baseline proteinuria or any histological parameter. Urinary levels of miR-150, miR-204, miR-431, or other miRNA targets had no significant correlation with any baseline clinical or pathological parameter (details not shown).
The trend of renal function was observed for an average of 84.8 ± 30.2 months. None of the urinary miRNA targets correlated with the rate of estimated GFR decline or predicted the development of renal event (details not shown).
Discussion
In the present study, we identified 4 miRNA targets whose urinary levels are significantly different between IgA nephropathy and healthy controls, and urinary miR-204 level alone has the best diagnostic accuracy.
Several previous studies explored the alterations in urinary miRNA levels in IgA nephropathy [12, 13, 22]. For example, Wang et al. [22] reported that intra-renal and urinary levels of miR-146a and miR-155 were significantly elevated in IgA nephropathy, and the degree of upregulation correlates with the severity of histological damage. Urinary miR-29b, miR-29c and miR-93 levels correlated with the clinical disease severity of IgA nephropathy and with the down-stream signaling of transforming growth factor-beta (TGF-β) pathway [13], indicating that they may play important roles in the pathogenesis of renal fibrosis. In another study, urinary miR-200a, miR-200b and miR-429 levels were reduced in IgA nephropathy, and the degree of reduction correlated with the rate of renal function deterioration [12]. Similarly, Min et al. [23] reported a significant difference in urinary exosomal miRNA profiles between patients with IgAN and healthy controls, and miR-29c, miR-146a and miR-205 may serve as novel non-invasive biomarkers for IgAN, while Liang et al. [24] found that urinary miR-21 and miR-205 levels are prognostic markers for evaluating the tubulointerstitial damage of IgAN. However, it is important to note that these studies used a candidate gene approach and lacked a second validation cohort. Our present study used a hypothesis-free approach that screened for all possible miRNAs in the urinary sediment, and the results are further validated by an additional independent cohort. It is interesting to note that in our development cohort, urinary miR-146a, miR-155, miR-29b, miR-29c and miR-93 levels were also significantly different between IgAN and CTL groups, but the difference did not reach the pre-defined criteria for the second stage validation. In contrast, urinary miR-200a, miR-200b and miR-429 levels were similar between IgAN and CTL groups in our development cohort.
Our result must be distinguished from the study of Serino et al. [6], which used high-throughput miRNA profiling and identified 37 miRNAs that were differentially expressed in the peripheral blood mononuclear cells (PBMC) of patients with IgA nephropathy as compared to healthy persons. In that study, PBMC miR-148b is upregulated in IgA nephropathy; miR-148b targets the enzyme core 1, β1,3-galactosyltransferase-1, modulates IgA1 O-glycosylation as well as the levels of secreted galactose-deficient IgA1 [6]. Our present study focused on the miRNA levels in urinary sediment rather than PBMC, and the alteration in miRNA levels is expected to be different. In our development cohort, urinary miR-148b level was marginally reduced in the IgAN group (0.84 log as compared to the CTL group, p = 0.034), but the difference did not reach the pre-defined criteria for the second stage validation.
Since the primary objective of our study is to identify an “miRNA signature” in urine for the diagnosis of IgA nephropathy, we did not explore – and there may not be any – biological role of the miRNAs that we found. As a result, we excluded patients with crescentic changes in the kidney biopsy and those with IgA vasculitis, so that a risk stratification based on urinary miRNA level is not possible. Nonetheless, previous studies showed that miR-204 takes part in the regulation of epithelial-mesenchymal transition by targeting SP1 in the tubular epithelial cells after ischemia-reperfusion injury [25], and in the control of local inflammation by regulating interleukin-6 (IL-6) receptor expression [26]. It remains to be determined whether these molecular pathways contribute to the pathogenesis of IgA nephropathy. Since the clinical spectrum of IgAN varies from minor urinary abnormalities to rapidly progressive renal failure, it may also be useful to clusterize patients with similar clinical phenotypes in further studies so as to identify miRNA for risk stratification.
There are a number of inadequacies in our study. First, the sample size is small and all of the patients came from a single center and were ethnically Chinese. It remains to be determined whether our result could be extrapolated to other patient population. This consideration is particularly important in the context of IgA nephropathy because its prevalence and clinical behavior are highly variable in different countries [27].
Second, healthy subjects served as control in the present study, but the healthy controls we recruited may not be well-matched with the patients (for example, in terms of age, renal function, or proteinuria), and, because of the difference in the number of subject, we could not perform a match-paired analysis for detailed comparison. More importantly, it remains uncertain whether the observed alterations in urinary miRNA levels represent disease-specific changes for IgA nephropathy or non-specific alterations secondary to renal scarring. It is absolutely important to conduct further studies that compare urinary miRNA level between IgAN and other glomerulonephritis in order to exclude the potential identification of damage-related miRNAs.
We did not determine the cellular origin of the miRNAs that we found in the urinary sediment. Previous studies suggested that both renal tubular cells and local inflammatory cells contribute to the total RNA in urine [10, 28]. Since the primary objective of our study is to identify urinary miRNA for diagnosis in routine clinical practice, we believe the cellular origin of miRNA may not be immediately relevant. Recent studies actually showed that conventional urinary sediment consists of cellular debris and microvesicles, and the miRNA level of these two components may be different [15, 29]. Further studies are needed to determine the miRNA alterations in various specific urinary components, which may further refine the accuracy of this novel non-invasive diagnostic tool.
Conclusions
Urinary miR-150, miR-204, miR-431 and miR-555 levels are significantly different between IgAN and healthy controls; urinary miR-204 level alone has the best diagnostic accuracy. Our result suggests that urinary miRNA measurement could be developed as the diagnostic tool for specific glomerular diseases.
References
Donadio JV, Grande JP. IgA nephropathy. N Engl J Med. 2002;347:738–48.
Li PK, Ho KK, Szeto CC, Yu L, Lai FM. Prognostic indicators of IgA nephropathy in the Chinese--clinical and pathological perspectives. Nephrol Dial Transplant. 2002;17:64–9.
Szeto CC, Lai FM, To KF, Wong TY, Chow KM, Choi PC, Lui SF, Li PK. The natural history of immunoglobulin a nephropathy among patients with hematuria and minimal proteinuria. Am J Med. 2001;110:434–7.
Working Group of the International IgA Nephropathy Network and the Renal Pathology Society. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. 2009;76:546–56.
Bartel DP. MicroRNAs: genomics, biogenesis, mechanism and function. Cell. 2004;116:281–97.
Serino G, Sallustio F, Cox SN, Pesce F, Schena FP. Abnormal miR-148b expression promotes aberrant glycosylation of IgA1 in IgA nephropathy. J Am Soc Nephrol. 2012;23:814–24.
Fang Y, Yu X, Liu Y, Kriegel AJ, Heng Y, Xu X, Liang M, Ding X. miR-29c is downregulated in renal interstitial fibrosis in humans and rats and restored by HIF-α activation. Am J Physiol Renal Physiol. 2013;304:F1274–82.
Szeto CC, Chan RW, Lai KB, Szeto CY, Chow KM, Li PK, Lai FM. Messenger RNA expression of target genes in the urinary sediment of patients with chronic kidney diseases. Nephrol Dial Transplant. 2005;20:105–13.
Szeto CC, Kwan BC, Tam LS. Urinary mRNA in systemic lupus erythematosus. Adv Clin Chem. 2013;62:197–219.
Szeto CC. Urine miRNA in nephrotic syndrome. Clin Chim Acta. 2014;436:308–13.
Szeto CC, Li PK. MicroRNAs in IgA nephropathy. Nat Rev Nephrol. 2014;10:249–56.
Wang G, Kwan BC, Lai FM, Chow KM, Kam-Tao Li P, Szeto CC. Expression of microRNAs in the urinary sediment of patients with IgA nephropathy. Dis Markers. 2010;28:79–86.
Wang G, Kwan BC, Lai FM, Chow KM, Li PK, Szeto CC. Urinary miR-21, miR-29, and miR-93: novel biomarkers of fibrosis. Am J Nephrol. 2012;36:412–8.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N. Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of diet in renal disease study group. Ann Intern Med. 1999;130:461–70.
Wang G, Szeto CC. Methods of microRNA quantification in urinary sediment. Methods Mol Biol. 2013;1024:211–20.
NanoString Technologies, Inc. nCounter® miRNA expression assay user manual. Seattle, Washington, 2013.
Helsel DR. Less than obvious – statistical treatment of data below the detection limit. Environ Sci Technol. 1990;24:1766–74.
Wang G, Lai FM, Tam LS, Li EK, Lai KB, Chow KM, Li PK, Szeto CC. Messenger RNA expression of podocyte associated molecules in the urinary sediment of patients with lupus nephritis. J Rheumatol. 2007;34:2358–64.
Trimarchi H, Barratt J, Cattran DC, Cook HT, Coppo R, Haas M, Liu ZH, Roberts IS, Yuzawa Y, Zhang H, Feehally J. Oxford classification of IgA nephropathy 2016: an update from the IgA nephropathy classification working group. Kidney Int. 2017;91:1014–21.
Wang G, Kwan BCH, Lai FMM, Chow KM, Ng KCJ, Luk CWC, Li PKT, Szeto CC. Urinary sediment mRNA level of extracellular matrix molecules in adult nephrotic syndrome. Clin Chim Acta. 2016;456:157–62.
Wei PZ, Kwan BC, Chow KM, Cheng PM, Luk CC, Lai KB, Li PK, Szeto CC. Urinary mitochondrial DNA level in non-diabetic chronic kidney diseases. Clin Chim Acta. 2018;484:36–9.
Wang G, Kwan BC, Lai FM, Chow KM, Li PK, Szeto CC. Elevated levels of miR-146a and miR-155 in kidney biopsy and urine from patients with IgA nephropathy. Dis Markers. 2011;30:171–9.
Min QH, Chen XM, Zou YQ, Zhang J, Li J, Wang Y, Li SQ, Gao QF, Sun F, Liu J, Xu YM, Lin J, Huang LF, Huang B, Wang XZ. Differential expression of urinary exosomal microRNAs in IgA nephropathy. J Clin Lab Anal. 2018; in press.
Liang S, Cai GY, Duan ZY, Liu SW, Wu J, Lv Y, Hou K, Li ZX, Zhang XG, Chen XM. Urinary sediment miRNAs reflect tubulointerstitial damage and therapeutic response in IgA nephropathy. BMC Nephrol. 2017;18:63.
Chen SJ, Wu P, Sun LJ, Zhou B, Niu W, Liu S, Lin FJ, Jiang GR. miR-204 regulates epithelial-mesenchymal transition by targeting SP1 in the tubular epithelial cells after acute kidney injury induced by ischemia-reperfusion. Oncol Rep. 2017;37:1148–58.
Chen Y, Qiu J, Chen B, Lin Y, Chen Y, Xie G, Qiu J, Tong H, Jiang D. Long non-coding RNA NEAT1 plays an important role in sepsis-induced acute kidney injury by targeting miR-204 and modulating the NF-κB pathway. Int Immunopharmacol. 2018;59:252–60.
Rodrigues JC, Haas M, Reich HN. IgA nephropathy. Clin J Am Soc Nephrol. 2017;12:677–86.
Chan RW, Szeto CC. Advances in the clinical laboratory assessment of urinary sediment. Clin Chim Acta. 2004;340:67–78.
Wei PZ, Kwan BC, Chow KM, Cheng PM, Luk CC, Li PK, Szeto CC. Urinary mitochondrial DNA level is an indicator of intra-renal mitochondrial depletion and renal scarring in diabetic nephropathy. Nephrol Dial Transplant. 2018;33:784–8.
Acknowledgements
We thank Dr. Nelson Chau and Dr. Vivek Kaimal from Regulus Therapeutics Inc. for their contribution to the first part of this project, and Dr. Steve Neben from Regulus Therapeutics Inc. for his advice.
Funding
This work represents a collaborative project between Regulus Therapeutics Inc. and the Chinese University of Hong Kong (CUHK), and was also supported in part by the Hong Kong Society of Nephrology research grant and CUHK research accounts 6901031 and 7101215. The funders of this study do not have any role in study design, data collection, analysis, result interpretation, report writing, or the decision to submit the report for publication. The results presented in this paper have not been published previously in whole or part, except in abstract format.
Availability of data and materials
All study data are available from the corresponding author upon written request.
Author information
Authors and Affiliations
Contributions
CCS is responsible for data analysis and manuscript writing. GW is responsible for the laboratory work. JKCN, BCHK and KMC are responsible for patient recruitment and preliminary data analysis. CCWL and KBL are responsible for the coordination of the laboratory part of the study, preparation of laboratory specimens and assay optimization. FMML is responsible for the pathological assessment. PKTL is responsible for administrative matters and overall supervision. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This is an observational study approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong (approval number CRE-2017.0314). All study procedures were in compliance with the Declaration of Helsinki. All patients provided written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Internal correlation of urinary miRNA levels in the validation set. (DOCX 16 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Szeto, CC., Wang, G., Ng, J.KC. et al. Urinary miRNA profile for the diagnosis of IgA nephropathy. BMC Nephrol 20, 77 (2019). https://doi.org/10.1186/s12882-019-1267-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-019-1267-4